
Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options

 , , ,
, , ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Non-RT Therapeutic Options for Recurrent GBM
3. Re-Irradiation
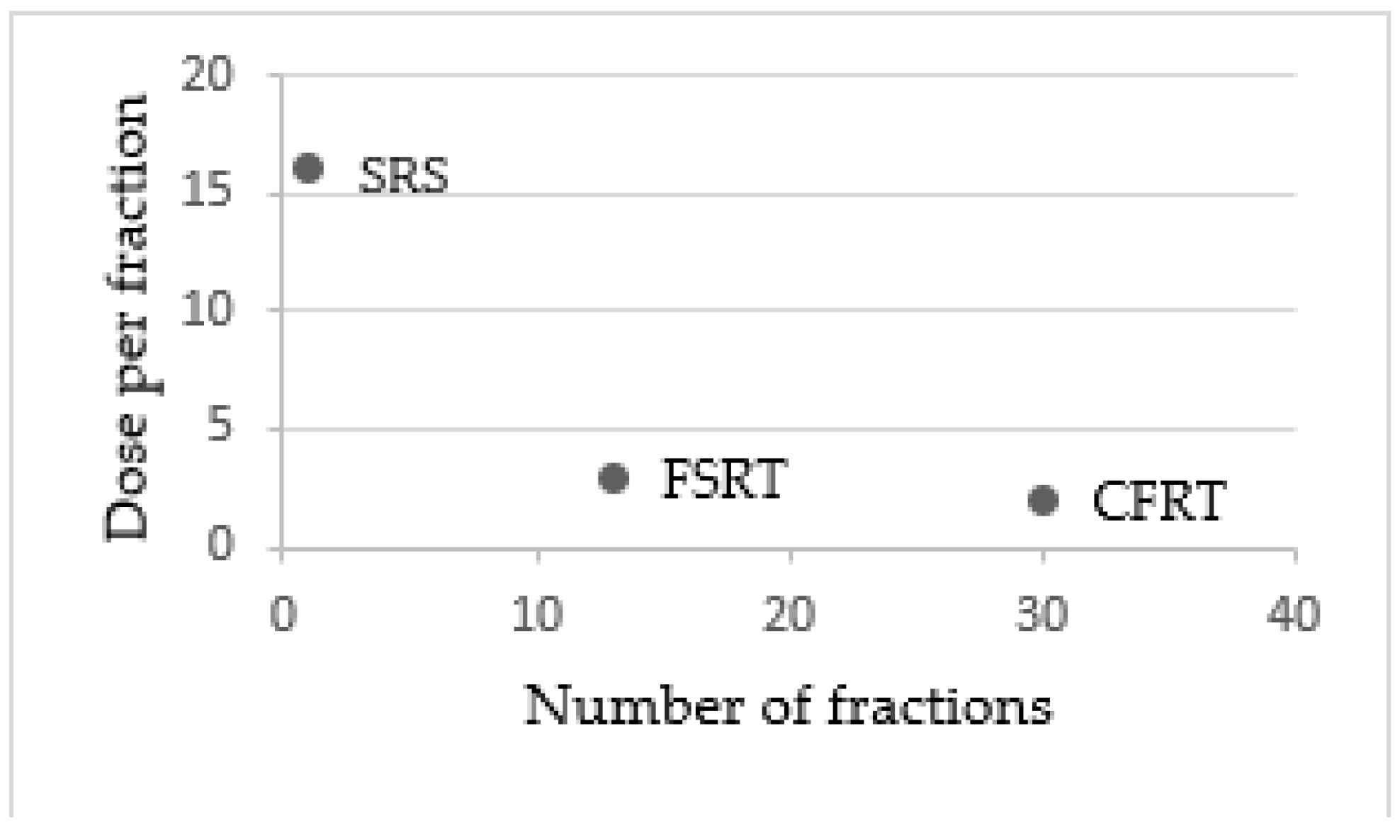
3.1. Stereotactic Techniques, Altered Fractionation and Brachytherapy Treatments
3.2. Safety and Tolerance of Reirradiation
3.3. Charged Particle Therapy
4. Predictive Factor of Response to Re-Irradiation and Combination with Systemic Therapies
4.1. Role of IDH1 and MGMT
4.2. Radiosensitizers
5. The Role of Radiomics and PET/MRI Advanced Imaging in the Management of Relapsing GBM
5.1. Radiomics
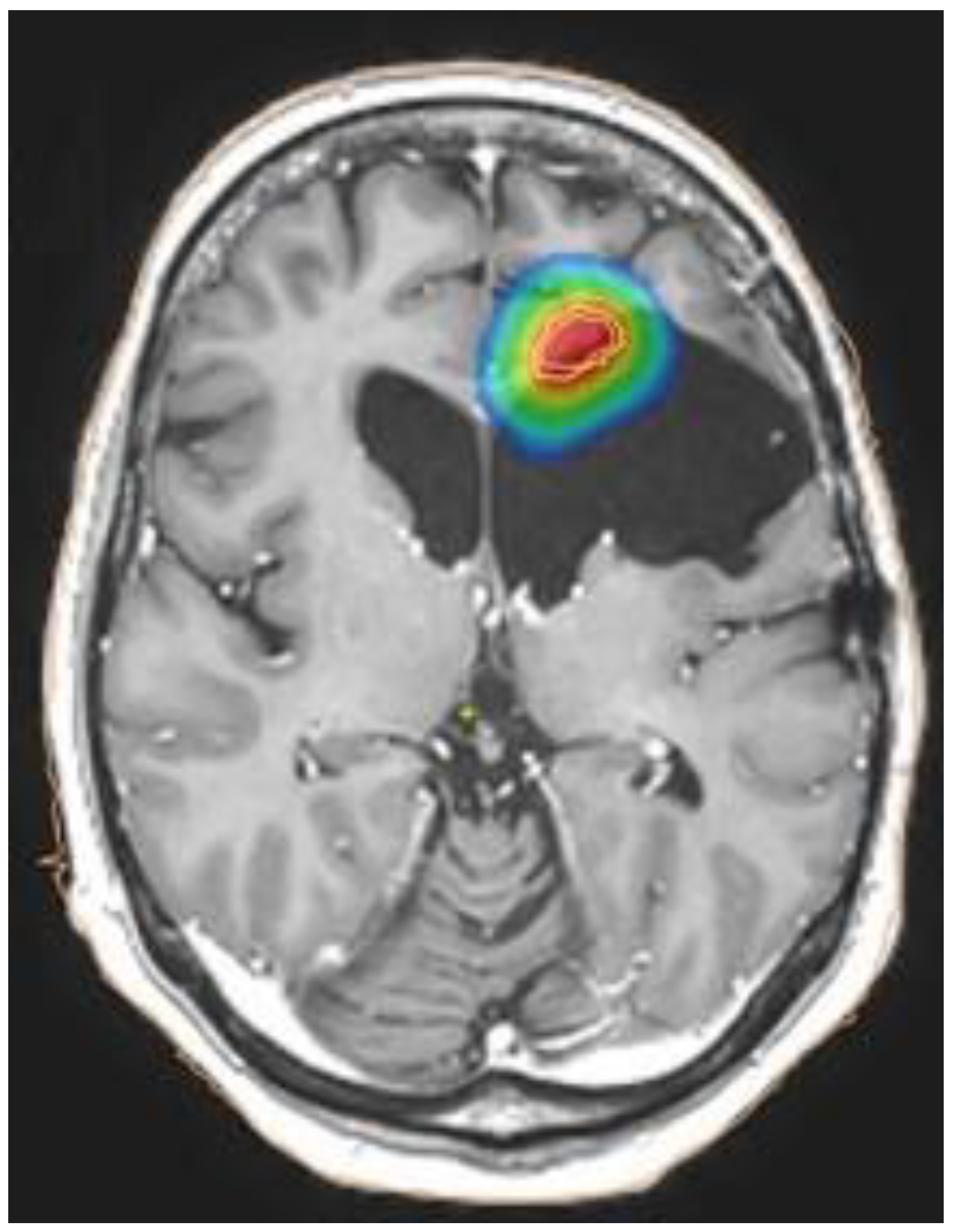
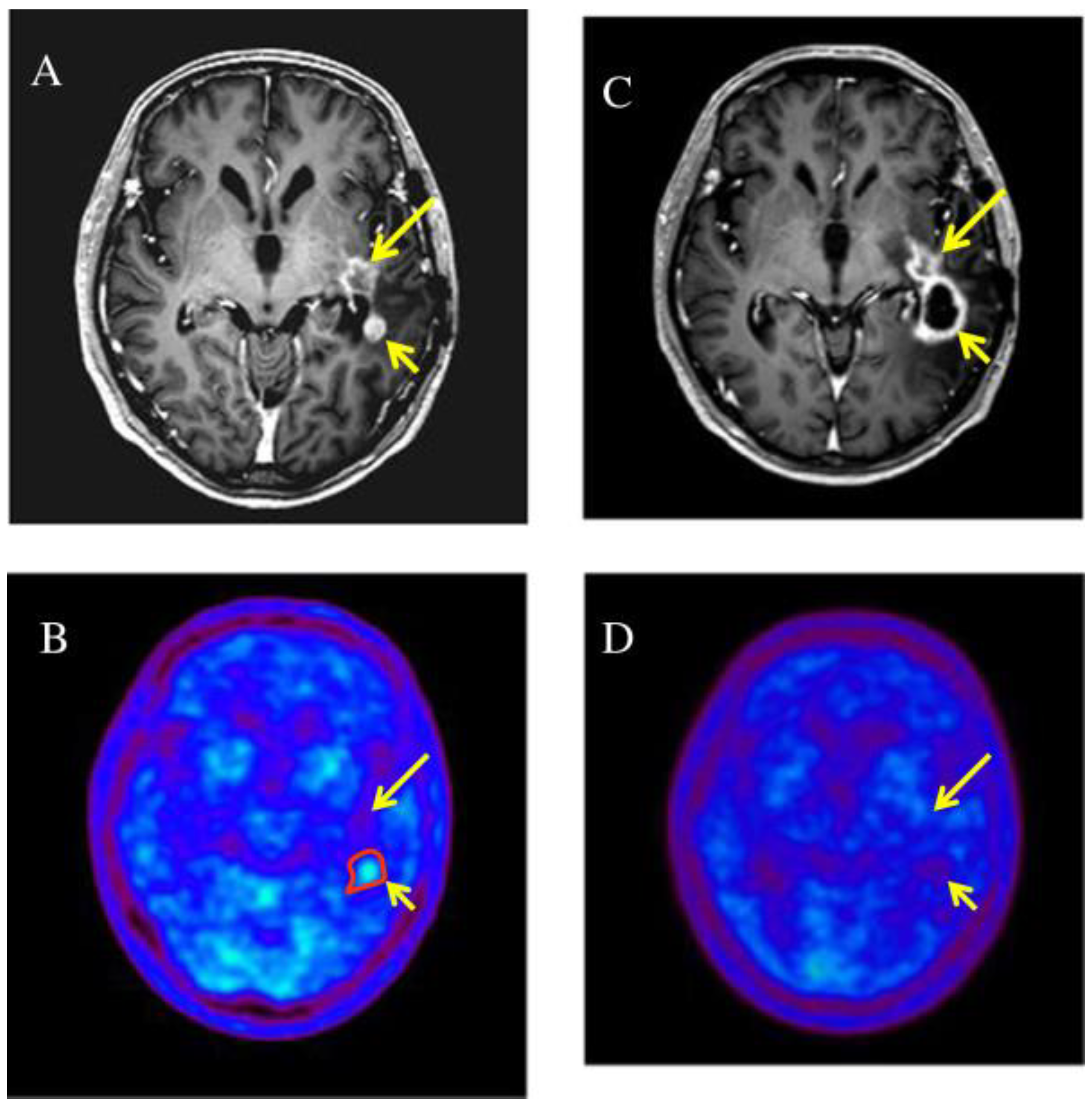
5.2. The Use of PET/MRI
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Farah, P.; Ondracek, A.; Chen, Y.; Wolinsky, Y.; Stroup, N.E.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro-Oncology 2013, 15 (Suppl. 2), ii1–ii56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshy, M.; Villano, J.L.; Dolecek, T.A.; Howard, A.; Mahmood, U.; Chmura, S.J.; Weichselbaum, R.R.; McCarthy, B.J. Improved survival time trends for glioblastoma using the SEER 17 population-based registries. J. Neuro-Oncol. 2012, 107, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Manrique-Guzmán, S.; Herrada-Pineda, T.; Revilla-Pacheco, F. Surgical Management of Glioblastoma; De Vleeschouwer, S., Ed.; Codon Publications: Brisbane, Australia, 2017; Chapter 12. [Google Scholar]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups, National Cancer Institute of Canada Clinical Trials Group Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Kim, B.S.; Seol, H.J.; Nam, D.H.; Park, C.K.; Kim, I.H.; Kim, T.M.; Kim, J.H.; Cho, Y.H.; Yoon, S.M.; Chang, J.H.; et al. Concurrent Chemoradiotherapy with Temozolomide Followed by Adjuvant Temozolomide for Newly Diagnosed Glioblastoma Patients: A Retrospective Multicenter Observation Study in Korea. Cancer Res. Treat. 2017, 49, 193–203. [Google Scholar] [CrossRef]
- Wallner, K.E.; Galicich, J.H.; Krol, G.; Arbit, E.; Malkin, M.G. Patterns of failure following treatment for glioblastoma multiforme and anaplastic astrocytoma. Int. J. Radiat. Oncol. Biol. Phys. 1989, 16, 1405–1409. [Google Scholar] [CrossRef]
- Nava, F.; Tramacere, I.; Fittipaldo, A.; Bruzzone, M.G.; Dimeco, F.; Fariselli, L.; Finocchiaro, G.; Pollo, B.; Salmaggi, A.; Silvani, A.; et al. Survival effect of first- and second-line treatments for patients with primary glioblastoma: A cohort study from a prospective registry, 1997–2010. Neuro-Oncology 2014, 16, 719–727. [Google Scholar] [CrossRef] [Green Version]
- Minniti, G.; Niyazi, M.; Alongi, F.; Navarria, P.; Belka, C. Current status and recent advances in reirradiation of glioblastoma. Radiat. Oncol. 2021, 16, 36. [Google Scholar] [CrossRef]
- Reardon, D.A.; Desjardins, A.; Peters, K.; Gururangan, S.; Sampson, J.; Rich, J.N.; McLendon, R.; Herndon, J.E.; 2nd Marcello, J.; Threatt, S.; et al. Phase II study of metronomic chemotherapy with bevacizumab for recurrent glioblastoma after progression on bevacizumab therapy. J. Neuro-Oncol. 2011, 103, 371–379. [Google Scholar] [CrossRef] [Green Version]
- Diaz, R.J.; Ali, S.; Qadir, M.G.; De La Fuente, M.I.; Ivan, M.E.; Komotar, R.J. The role of bevacizumab in the treatment of glioblastoma. J. Neurooncol. 2017, 133, 455–467. [Google Scholar] [CrossRef]
- Martínez-Garcia, M.; Álvarez-Linera, J.; Carrato, C.; Ley, L.; Luque, R.; Maldonado, X.; Martínez-Aguillo, M.; Navarro, L.M.; Vaz-Salgado, M.A.; Gil-Gil, M. SEOM clinical guidelines for diagnosis and treatment of glioblastoma (2017). Clin. Transl. Oncol. 2018, 20, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, G.; De Salvo, G.L.; Brandes, A.A.; Eoli, M.; Rudà, R.; Faedi, M.; Lolli, I.; Pace, A.; Daniele, B.; Pasqualetti, F.; et al. Regorafenibcompared with lomustine in patients with relapsed glioblastoma (REGOMA): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol. 2019, 20, 110–119. [Google Scholar] [CrossRef]
- Kong, D.S.; Lee, J.I.; Park, K.; Kim, J.H.; Lim, D.H.; Nam, D.H. Efficacy of stereotactic radiosurgery as a salvage treatment for recurrent malignant gliomas. Cancer 2008, 112, 2046–2051. [Google Scholar] [CrossRef] [PubMed]
- Skeie, B.S.; Enger, P.Ø.; Brøgger, J.; Ganz, J.C.; Thorsen, F.; Heggdal, J.I.; Pedersen, P.H. γ knife surgery versus reoperation for recurrent glioblastoma multiforme. World Neurosurg. 2012, 78, 658–669. [Google Scholar] [CrossRef] [PubMed]
- Liao, G.; Zhao, Z.; Yang, H.; Li, X. Efficacy and Safety of Hypofractionated Radiotherapy for the Treatment of Newly Diagnosed Glioblastoma Multiforme: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 1017. [Google Scholar] [CrossRef] [PubMed]
- Yu, V.Y.; Nguyen, D.; O’Connor, D.; Ruan, D.; Kaprealian, T.; Chin, R.; Sheng, K. Treating Glioblastoma Multiforme (GBM) with super hyperfractionated radiation therapy: Implication of temporal dose fractionation optimization including cancer stem cell dynamics. PLoS ONE 2021, 16, e0245676. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, F.; Soon, Y.Y.; Leong, Y.H.; Koh, W.Y.; Vellayappan, B. Re-irradiation for recurrent glioblastoma (GBM): A systematic review and meta-analysis. J. Neuro-Oncol. 2019, 142, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Mayer, R.; Sminia, P. Reirradiation tolerance of the human brain. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1350–1360. [Google Scholar] [CrossRef] [PubMed]
- Scoccianti, S.; Francolini, G.; Carta, G.A.; Greto, D.; Detti, B.; Simontacchi, G.; Visani, L.; Baki, M.; Poggesi, L.; Bonomo, P.; et al. Re-irradiationassalvage treatment in recurrent glioblastoma: A comprehensive literature review to providepracticalanswers to frequentlyaskedquestions. Oncol./Hematol. 2018, 126, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.; Yorke, E.; Merchant, T.E. Radiation associated brainstem injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), S36–S41. [Google Scholar] [CrossRef] [Green Version]
- Cho, K.H.; Hall, W.A.; Gerbi, B.J.; Higgins, P.D.; McGuire, W.A.; Clark, H.B. Single dose versus fractionated stereotactic radiotherapy for recurrent high-grade gliomas. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 1133–1141. [Google Scholar] [CrossRef]
- Kim, B.; Soisson, E.; Duma, C.; Chen, P.; Hafer, R.; Cox, C.; Cubellis, J.; Minion, A.; Plunkett, M.; Mackintosh, R. Treatment of recurrent high-grade gliomas with hypofractionated stereotactic image-guided helical tomotherapy. Clin. Neurol. Neurosurg. 2011, 113, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlaeger, F.S.; Dumke, R.; Schymalla, M.; Hauswald, H.; Carl, B.; Stein, M.; Keber, U.; Jensen, A.; Engenhart-Cabillic, R.; Eberle, F. Comparison of carbon ion and photon reirradiation for recurrent glioblastoma. Strahlenther. Onkol. Organ. Der Dtsch. 2021. advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Combs, S.E.; Zipp, L.; Rieken, S.; Habermehl, D.; Brons, S.; Winter, M.; Haberer, T.; Debus, J.; Weber, K.J. In vitro evaluation of photon and carbon ion radiotherapy in combination with chemotherapy in glioblastoma cells. Radiat. Oncol. 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combs, S.E.; Burkholder, I.; Edler, L.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomised phase I/II study to evaluate carbon ion radiotherapy versus fractionated stereotactic radiotherapy in patients with recurrent or progressive gliomas: The CINDERELLA trial. BMC Cancer 2010, 10, 533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galle, J.O.; McDonald, M.W.; Simoneaux, V.; Buchsbaum, J.C. Reirradiation with Proton Therapy for Recurrent Gliomas. Int. J. Part Ther. 2015, 2, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Gulidov, I.; Gordon, K.; Semenov, A.; Gogolin, D.; Lepilina, O.; Golovanova, O.; Dujenko, S.; Medvedeva, K.; Koryakin, S.; Ivanov, S.; et al. Proton re-irradiation of unresectable recurrent brain gliomas: Clinical outcomes and toxicity. J. BU ON Off. J. Balk. Union Oncol. 2021, 26, 970–976. [Google Scholar]
- Saeed, A.M.; Khairnar, R.; Sharma, A.M.; Larson, G.L.; Tsai, H.K.; Wang, C.J.; Halasz, L.M.; Chinnaiyan, P.; Vargas, C.E.; Mishra, M.V. Clinical Outcomes in Patients with Recurrent Glioblastoma Treated with Proton Beam Therapy Reirradiation: Analysis of the Multi-Institutional Proton Collaborative Group Registry. Adv. Radiat. Oncol. 2020, 5, 978–983. [Google Scholar] [CrossRef]
- Scartoni, D.; Amelio, D.; Palumbo, P.; Giacomelli, I.; Amichetti, M. Proton therapy re-irradiation preserves health-related quality of life in large recurrent glioblastoma. J. Cancer Res. Clin. Oncol. 2020, 146, 1615–1622. [Google Scholar] [CrossRef]
- Milazzotto, R.; Liardo, R.; Privitera, G.; Raffaele, L.; Salamone, V.; Arena, F.; Spatola, C. Proton beam radiotherapy of locally advanced or recurrent conjunctival squamous cell carcinoma: Experience of the CATANA Centre. J. Radiother. Pract. 2020, 21, 97–104. [Google Scholar] [CrossRef]
- Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; Basile, A.; Foti, P.V.; Palmucci, S.; Cirrone, G.A.P.; Cuttone, G.; et al. Radiotherapy of Conjunctival Melanoma: Role and Challenges of Brachytherapy, Photon-Beam and Protontherapy. Appl. Sci. 2020, 10, 9071. [Google Scholar] [CrossRef]
- Parsons, D.W.; Jones, S.; Zhang, X.; Lin, J.C.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Siu, I.M.; Gallia, G.L.; et al. An integrated genomic analysis of human glioblastoma multiforme. Science 2008, 321, 1807–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, A.N.; Lai, A.; Li, S.; Pope, W.B.; Teixeira, S.; Harris, R.J.; Woodworth, D.C.; Nghiemphu, P.L.; Cloughesy, T.F.; Ellingson, B.M. Increased sensitivity to radiochemotherapy in IDH1 mutant glioblastoma as demonstrated by serial quantitative MR volumetry. Neuro-Oncology 2014, 16, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Lin, Y.; Xu, W.; Jiang, W.; Zha, Z.; Wang, P.; Yu, W.; Li, Z.; Gong, L.; Peng, Y.; et al. Glioma-derived mutations in IDH1 dominantly inhibit IDH1 catalytic activity and induce HIF-1alpha. Science 2009, 324, 261–265. [Google Scholar] [CrossRef] [Green Version]
- Dang, L.; White, D.W.; Gross, S.; Bennett, B.D.; Bittinger, M.A.; Driggers, E.M.; Fantin, V.R.; Jang, H.G.; Jin, S.; Keenan, M.C.; et al. Cancer-associated IDH1 mutations produce 2-hydroxyglutarate. Nature 2009, 462, 739–744. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Chou, A.P.; Chen, W.; Chen, R.; Deng, Y.; Phillips, H.S.; Selfridge, J.; Zurayk, M.; Lou, J.J.; Everson, R.G.; et al. Overexpression of isocitrate dehydrogenase mutant proteins renders glioma cells more sensitive to radiation. Neuro-Oncology 2013, 15, 57–68. [Google Scholar] [CrossRef]
- Yu, W.; Zhang, L.; Wei, Q.; Shao, A. O6-Methylguanine-DNA Methyltransferase (MGMT): Challenges and New Opportunities in Glioma Chemotherapy. Front. Oncol. 2020, 9, 1547. [Google Scholar] [CrossRef] [Green Version]
- Brandes, A.A.; Tosoni, A.; Franceschi, E.; Sotti, G.; Frezza, G.; Amistà, P.; Morandi, L.; Spagnolli, F.; Ermani, M. Recurrence pattern after temozolomide concomitant with and adjuvant to radiotherapy in newly diagnosed patients with glioblastoma: Correlation With MGMT promoter methylation status. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 1275–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.P.; Schlegel, U.; Sabel, M.; Hau, P.; Kortmann, R.D.; Krex, D.; Grauer, O.; et al. Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA-09): A randomised, open-label, phase 3 trial. Lancet 2019, 393, 678–688. [Google Scholar] [CrossRef]
- Ali, M.Y.; Oliva, C.R.; Noman, A.; Allen, B.G.; Goswami, P.C.; Zakharia, Y.; Monga, V.; Spitz, D.R.; Buatti, J.M.; Griguer, C.E. Radioresistance in Glioblastoma and the Development of Radiosensitizers. Cancers 2020, 12, 2511. [Google Scholar] [CrossRef]
- Sigmond, J.; Honeywell, R.J.; Postma, T.J.; Dirven, C.M.; de Lange, S.M.; van der Born, K.; Laan, A.C.; Baayen, J.C.; Van Groeningen, C.J.; Bergman, A.M.; et al. Gemcitabine uptake in glioblastoma multiforme: Potential as a radiosensitizer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2009, 20, 182–187. [Google Scholar] [CrossRef]
- Metro, G.; Fabi, A.; Mirri, M.A.; Vidiri, A.; Pace, A.; Carosi, M.; Russillo, M.; Maschio, M.; Giannarelli, D.; Pellegrini, D.; et al. Phase II study of fixed dose rate gemcitabineasradiosensitizer for newlydiagnosed glioblastoma multiforme. Cancer Chemother. Pharmacol. 2010, 65, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Palanichamy, K.; Chakravarti, A. Combining drugs and radiotherapy: From the bench to the bedside. Curr. Opin. Neurol. 2009, 22, 625–632. [Google Scholar] [CrossRef] [Green Version]
- Setua, S.; Ouberai, M.; Piccirillo, S.G.; Watts, C.; Welland, M. Cisplatin-tethered gold nanospheres for multimodal chemo-radiotherapy of glioblastoma. Nanoscale 2014, 6, 10865–10873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulton, B.; Short, S.C.; James, A.; Nowicki, S.; McBain, C.; Jefferies, S.; Kelly, C.; Stobo, J.; Morris, A.; Williamson, A.; et al. PARADIGM-2: Two parallel phase I studies of olaparib and radiotherapy or olaparib and radiotherapy plus temozolomide in patients with newly diagnosed glioblastoma, with treatment stratified by MGMT status. Clin. Transl. Radiat. Oncol. 2017, 8, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Sim, H.W.; McDonald, K.L.; Lwin, Z.; Barnes, E.H.; Rosenthal, M.; Foote, M.C.; Koh, E.S.; Back, M.; Wheeler, H.; Sulman, E.P.; et al. A randomized phase II trial of veliparib, radiotherapy, and temozolomide in patients with unmethylated MGMT glioblastoma: The VERTU study. Neuro-Oncology 2021, 23, 1736–1749. [Google Scholar] [CrossRef]
- Barbagallo, G.; Certo, F.; Di Gregorio, S.; Maione, M.; Garozzo, M.; Peschillo, S.; Altieri, R. Recurrent high-grade glioma surgery: A multimodal intraoperative protocol to safely increase extent of tumor resection and analysis of its impact on patient outcome. Neurosurg. Focus 2021, 50, E20. [Google Scholar] [CrossRef] [PubMed]
- Altieri, R.; Barbagallo, D.; Certo, F.; Broggi, G.; Ragusa, M.; Di Pietro, C.; Caltabiano, R.; Magro, G.; Peschillo, S.; Purrello, M.; et al. Peritumoral Microenvironment in High-Grade Gliomas: From FLAIRectomy to Microglia-Glioma Cross-Talk. Brain Sci. 2021, 11, 200. [Google Scholar] [CrossRef]
- Certo, F.; Altieri, R.; Maione, M.; Schonauer, C.; Sortino, G.; Fiumanò, G.; Tirrò, E.; Massimino, M.; Broggi, G.; Vigneri, P.; et al. FLAIRectomy in Supramarginal Resection of Glioblastoma Correlates With Clinical Outcome and Survival Analysis: A Prospective, Single Institution, Case Series. Oper. Neurosurg. 2021, 20, 151–163. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.; Deist, T.M.; Peerlings, J.; de Jong, E.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Spatola, C.; Milazzotto, R.; Tocco, A.; Raffaele, L.; La Monaca, V.; Salamone, V.; Privitera, G. Metachronous NSCLC in previously irradiated patients: Is re-irradiation with SBRT a good option as definitive treatment? J. Radiother. Pract. 2020, 19, 215–218. [Google Scholar] [CrossRef]
- Russo, G.; Stefano, A.; Alongi, P.; Comelli, A.; Catalfamo, B.; Mantarro, C.; Longo, C.; Altieri, R.; Certo, F.; Cosentino, S.; et al. Feasibility on the Use of Radiomics Features of 11[C]-MET PET/CT in Central Nervous System Tumours: Preliminary Results on Potential Grading Discrimination Using a Machine Learning Model. Curr. Oncol. 2021, 28, 5318–5331. [Google Scholar] [CrossRef]
- Baine, M.; Burr, J.; Du, Q.; Zhang, C.; Liang, X.; Krajewski, L.; Zima, L.; Rux, G.; Zhang, C.; Zheng, D. The potential use of radiomics with pre-radiation therapy mr imaging in predicting risk of pseudoprogression in glioblastoma patients. J. Imaging 2021, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Grosu, A.L.; Weber, W.A.; Franz, M.; Stärk, S.; Piert, M.; Thamm, R.; Gumprecht, H.; Schwaiger, M.; Molls, M.; Nieder, C. Reirradiation of recurrent high-grade gliomas using amino acid PET (SPECT)/CT/MRI image fusion to determine gross tumor volume for stereotactic fractionated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 511–519. [Google Scholar] [CrossRef] [PubMed]
- García-Cabezas, S.; Rivin Del Campo, E.; Solivera-Vela, J.; Palacios-Eito, A. Re-irradiation for high-grade gliomas: Has anything changed? World J. Clin. Oncol. 2021, 12, 767–786. [Google Scholar] [CrossRef] [PubMed]
- Oehlke, O.; Mix, M.; Graf, E.; Schimek-Jasch, T.; Nestle, U.; Götz, I.; Schneider-Fuchs, S.; Weyerbrock, A.; Mader, I.; Baumert, B.G.; et al. Amino-acid PET versus MRI guided re-irradiation in patients with recurrent glioblastoma multiforme (GLIAA)—Protocol of a randomized phase II trial (NOA 10/ARO 2013-1). BMC Cancer 2016, 16, 769. [Google Scholar] [CrossRef] [Green Version]
- Miwa, K.; Matsuo, M.; Ogawa, S.; Shinoda, J.; Yokoyama, K.; Yamada, J.; Yano, H.; Iwama, T. Re-irradiation of recurrent glioblastoma multiforme using 11C-methionine PET/CT/MRI image fusion for hypofractionated stereotactic radiotherapy by intensity modulated radiation therapy. Radiat. Oncol. 2014, 9, 181. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, D.F.; Unterrainer, M.; Corradini, S.; Rottler, M.; Förster, S.; la Fougère, C.; Siepmann, T.; Schwaiger, M.; Bartenstein, P.; Belka, C.; et al. Report of first recurrent glioma patients examined with PET-MRI prior to re-irradiation. PLoS ONE 2019, 14, e0216111. [Google Scholar] [CrossRef]
- Debus, C.; Waltenberger, M.; Floca, R.; Afshar-Oromieh, A.; Bougatf, N.; Adeberg, S.; Heiland, S.; Bendszus, M.; Wick, W.; Rieken, S.; et al. Impact of 18F-FET PET on Target Volume Definition and Tumor Progression of Recurrent High-Grade Glioma Treated with Carbon-Ion Radiotherapy. Sci. Rep. 2018, 8, 7201. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Technique | Schedules | OS | PFS |
|---|---|---|---|---|
| Lautenschlaeger F.S. et al. [24] | Carbon Ionsradiotherapy (CIRT) | 45 Gy, median fraction size 3 Gy per fx | 8.0 months | 5.5 months |
| Fractionated stereotactic radiotherapy with photons (FSRT) | 39 Gy, median fraction size 3 Gy per fx | 6.5 months | 3.9 months | |
| Saeed A.M. et al. [25] | Proton beam therapy (PBRT) | 46.2 Gy (range, 25–60 Gy), median fraction size 2.2 per fx | 14.2 months | 13.9 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Greco, M.C.; Milazzotto, R.; Liardo, R.L.E.; Acquaviva, G.; La Rocca, M.; Altieri, R.; Certo, F.; Barbagallo, G.M.; Basile, A.; Foti, P.V.; et al. Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options. Brain Sci. 2022, 12, 416. https://doi.org/10.3390/brainsci12040416
Lo Greco MC, Milazzotto R, Liardo RLE, Acquaviva G, La Rocca M, Altieri R, Certo F, Barbagallo GM, Basile A, Foti PV, et al. Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options. Brain Sciences. 2022; 12(4):416. https://doi.org/10.3390/brainsci12040416
Chicago/Turabian StyleLo Greco, Maria Chiara, Roberto Milazzotto, Rocco Luca Emanuele Liardo, Grazia Acquaviva, Madalina La Rocca, Roberto Altieri, Francesco Certo, Giuseppe Maria Barbagallo, Antonio Basile, Pietro Valerio Foti, and et al. 2022. "Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options" Brain Sciences 12, no. 4: 416. https://doi.org/10.3390/brainsci12040416
APA StyleLo Greco, M. C., Milazzotto, R., Liardo, R. L. E., Acquaviva, G., La Rocca, M., Altieri, R., Certo, F., Barbagallo, G. M., Basile, A., Foti, P. V., Palmucci, S., Pergolizzi, S., Pontoriero, A., & Spatola, C. (2022). Relapsing High—Grade Glioma from Peritumoral Zone: Critical Review of Radiotherapy Treatment Options. Brain Sciences, 12(4), 416. https://doi.org/10.3390/brainsci12040416