
The Impact of Electroconvulsive Therapy on Negative Symptoms in Schizophrenia and Their Association with Clinical Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Socio-Demographics and ECT Treatment Modalities
2.3. Clinical Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Participants
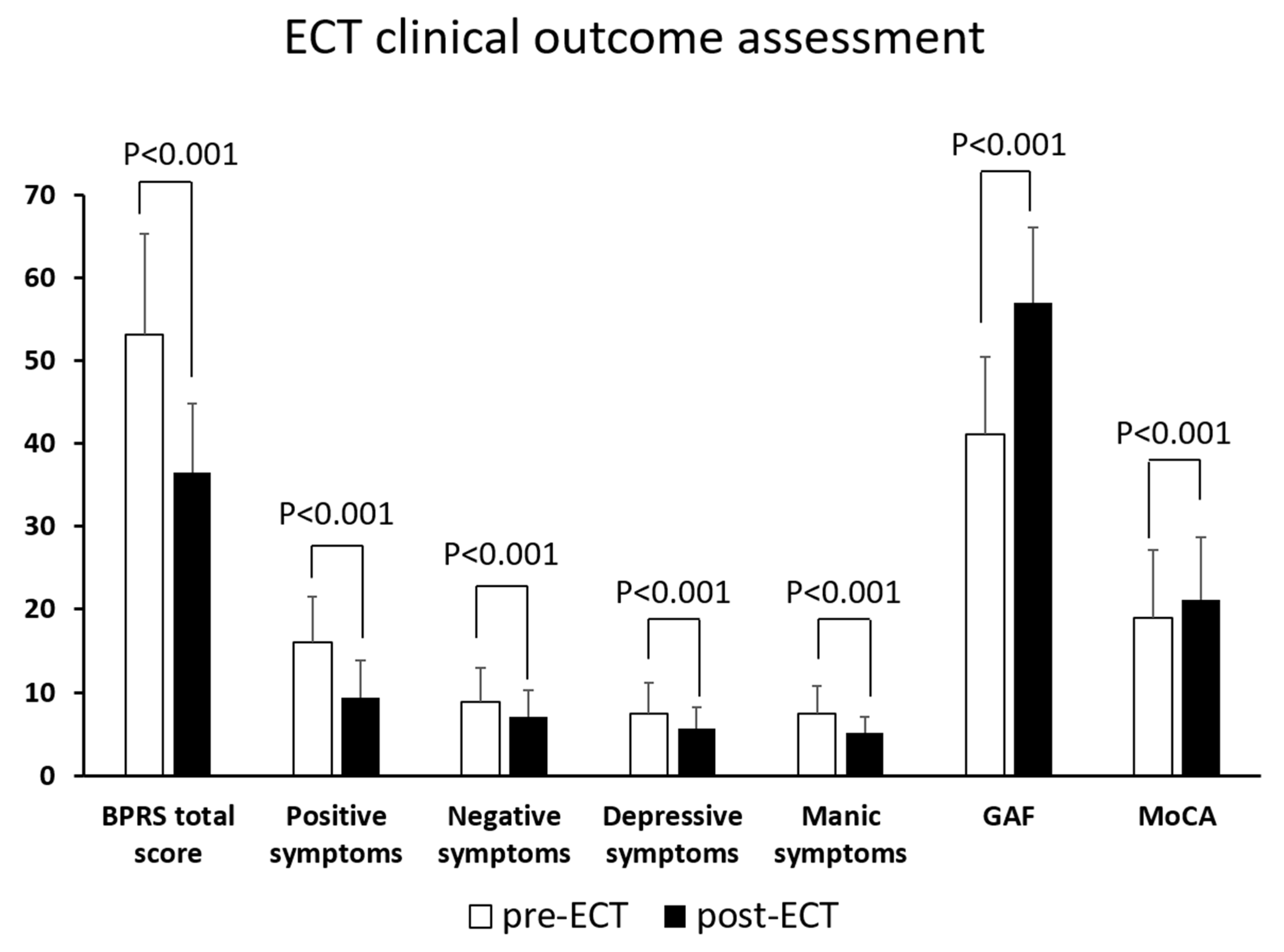
3.2. Clinical Outcomes
3.3. Associations between Symptom Improvement, Cognition and Functioning
3.4. Predictors of Negative Symptoms Improvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fenton, W.S.; McGlashan, T.H. Natural history of schizophrenia subtypes: I. Longitudinal study of paranoid, hebephrenic, and undifferentiated schizophrenia. Arch. Gen. Psychiatry 1991, 48, 969–977. [Google Scholar] [CrossRef]
- Fenton, W.S.; McGlashan, T.H. Natural history of schizophrenia subtypes: II. Positive and negative symptoms and long-term course. Arch. Gen. Psychiatry 1991, 48, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Siu, C.; Remington, G.; Fervaha, G.; Zipursky, R.B.; Foussias, G.; Agid, O. Does relapse contribute to treatment resistance? Antipsychotic response in first- vs. second-episode schizophrenia. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2019, 44, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.A.; Stroup, T.S.; McEvoy, J.P.; Swartz, M.S.; Rosenheck, R.A.; Perkins, D.O.; Keefe, R.S.; Davis, S.M.; Davis, C.E.; Lebowitz, B.D. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N. Engl. J. Med. 2005, 353, 1209–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phutane, V.H.; Thirthalli, J.; Kesavan, M.; Kumar, N.C.; Gangadhar, B.N. Why do we prescribe ECT to schizophrenia patients? Indian J. Psychiatry 2011, 53, 149–151. [Google Scholar] [PubMed]
- Tharyan, P.; Adams, C.E. Electroconvulsive therapy for schizophrenia. Cochrane Database Syst. Rev. 2005, CD000076. [Google Scholar] [CrossRef]
- Petrides, G.; Malur, C.; Braga, R.J.; Bailine, S.H.; Schooler, N.R.; Malhotra, A.K.; Kane, J.M.; Sanghani, S.; Goldberg, T.E.; John, M. Electroconvulsive therapy augmentation in clozapine-resistant schizophrenia: A prospective, randomized study. Am. J. Psychiatry 2015, 172, 52–58. [Google Scholar] [CrossRef]
- Wang, G.; Zheng, W.; Li, X.-B.; Wang, S.-B.; Cai, D.-B.; Yang, X.-H.; Ungvari, G.S.; Xiang, Y.-T.; Correll, C.U. ECT augmentation of clozapine for clozapine-resistant schizophrenia: A meta-analysis of randomized controlled trials. J. Psychiatr. Res. 2018, 105, 23–32. [Google Scholar] [CrossRef]
- Grover, S.; Hazari, N.; Kate, N. Combined use of clozapine and ECT: A review. Acta Neuropsychiatr. 2015, 27, 131–142. [Google Scholar] [CrossRef]
- American Psychiatric Association. The Practice of Electroconvulsive Therapy: Recommendations for Treatment, Training, and Privileging (A Task Force Report of the American Psychiatric Association); American Psychiatric Pub.: Washington DC, USA, 2008. [Google Scholar]
- Practice Guideline Electrovonvulsive Therapy. Available online: https://www.ams.edu.sg/policy-advocacy/guidelines-consensus-statements-for-healthcare-professionals (accessed on 12 November 2021).
- Sinclair, D.J.; Zhao, S.; Qi, F.; Nyakyoma, K.; Kwong, J.S.; Adams, C.E. Electroconvulsive therapy for treatment-resistant schizophrenia. Cochrane Database Syst. Rev. 2019, 3, CD011847. [Google Scholar]
- Tor, P.C.; Ying, J.; Ho, N.F.; Wang, M.; Martin, D.; Ang, C.P.; Tan, C.; Yap, L.S.; Lu, V.J.M.; Simpson, B.; et al. Effectiveness of Electroconvulsive Therapy and Associated Cognitive Change in Schizophrenia: A Naturalistic, Comparative Study of Treating Schizophrenia with Electroconvulsive Therapy. J. ECT 2017, 33, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Y.W.; Abdin, E.; Seow, E.; Subramaniam, M.; Liu, J.; Peh, C.X.; Tor, P.C. Clinical effectiveness and speed of response of electroconvulsive therapy in treatment-resistant schizophrenia. Psychiatry Clin. Neurosci. 2019, 73, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Tor, P.C.; Tan, X.W.; Martin, D.; Loo, C. Comparative outcomes in electroconvulsive therapy (ECT): A naturalistic comparison between outcomes in psychosis, mania, depression, psychotic depression and catatonia. Eur. Neuropsychopharmacol. 2021, 51, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Tor, P.C.; Gálvez, V.; Ang, A.; Fam, J.; Chan, H.N.; Tan, S.N.; Loo, C.K. Electroconvulsive practice in Singapore: A cross-sectional national survey. Singap. Med. J. 2019, 60, 590–595. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, B.; Fenton, W.S.; Carpenter, W.T., Jr.; Marder, S.R. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr. Bull. 2006, 32, 214–219. [Google Scholar] [CrossRef] [Green Version]
- Galderisi, S.; Mucci, A.; Buchanan, R.W.; Arango, C. Negative symptoms of schizophrenia: New developments and unanswered research questions. Lancet Psychiatry 2018, 5, 664–677. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Buchanan, R.W.; Ross, D.E.; Carpenter, W.T., Jr. A separate disease within the syndrome of schizophrenia. Arch Gen. Psychiatry 2001, 58, 165–171. [Google Scholar] [CrossRef]
- Milev, P.; Ho, B.C.; Arndt, S.; Andreasen, N.C. Predictive values of neurocognition and negative symptoms on functional outcome in schizophrenia: A longitudinal first-episode study with 7-year follow-up. Am. J. Psychiatry 2005, 162, 495–506. [Google Scholar] [CrossRef]
- Correll, C.U.; Schooler, N.R. Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [Green Version]
- Remington, G.; Foussias, G.; Fervaha, G.; Agid, O.; Takeuchi, H.; Lee, J.; Hahn, M. Treating Negative Symptoms in Schizophrenia: An Update. Curr. Treat. Options Psychiatry 2016, 3, 133–150. [Google Scholar] [CrossRef] [Green Version]
- Bansod, A.; Sonavane, S.S.; Shah, N.B.; De Sousa, A.A.; Andrade, C. A Randomized, Nonblind, Naturalistic Comparison of Efficacy and Cognitive Outcomes with Right Unilateral, Bifrontal, and Bitemporal Electroconvulsive Therapy in Schizophrenia. J. ECT 2018, 34, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Shen, J.; Liu, F.H.; Wong, H.K.; Yang, X.J.; Wu, Q.J.; Zhang, H.; Wang, H.N.; Tan, Q.R.; Zhang, Z.J. Effectiveness of Electroacupuncture and Electroconvulsive Therapy as Additional Treatment in Hospitalized Patients with Schizophrenia: A Retrospective Controlled Study. Front. Psychol. 2019, 10, 2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kho, K.H.; Blansjaar, B.A.; de Vries, S.; Babuskova, D.; Zwinderman, A.H.; Linszen, D.H. Electroconvulsive therapy for the treatment of clozapine nonresponders suffering from schizophrenia--an open label study. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ye, F.; Xiao, W.; Tang, X.; Sha, W.; Zhang, X.; Wang, J. Increased serum brain-derived neurotrophic factor levels following electroconvulsive therapy or antipsychotic treatment in patients with schizophrenia. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2016, 36, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Ricci, V.; Di Nicola, M.; Caltagirone, C.; Bria, P.; Angelucci, F. Brain-derived neurotrophic factor and electroconvulsive therapy in a schizophrenic patient with treatment-resistant paranoid-hallucinatory symptoms. J. ECT 2011, 27, e44–e46. [Google Scholar] [CrossRef]
- Tang, W.K.; Ungvari, G.S. Efficacy of electroconvulsive therapy combined with antipsychotic medication in treatment-resistant schizophrenia: A prospective, open trial. J. ECT 2002, 18, 90–94. [Google Scholar] [CrossRef]
- Usta Saglam, N.G.; Aksoy Poyraz, C. ECT augmentation of antipsychotics in severely ill schizophrenia: A naturalistic, observational study. Int. J. Psychiatry Clin. Pract. 2020, 24, 392–397. [Google Scholar] [CrossRef]
- Chanpattana, W.; Chakrabhand, M.L. Combined ECT and neuroleptic therapy in treatment-refractory schizophrenia: Prediction of outcome. Psychiatry Res. 2001, 105, 107–115. [Google Scholar] [CrossRef]
- Chanpattana, W.; Sackeim, H.A. Electroconvulsive therapy in treatment-resistant schizophrenia: Prediction of response and the nature of symptomatic improvement. J. ECT 2010, 26, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Masoudzadeh, A.; Khalilian, A.R. Comparative study of clozapine, electroshock and the combination of ECT with clozapine in treatment-resistant schizophrenic patients. Pak. J. Biol. Sci. PJBS 2007, 10, 4287–4290. [Google Scholar] [CrossRef] [Green Version]
- Petrides, G.; Malur, C.; Braga, R.J.; Bailine, S.H.; Schooler, N.R.; Malhotra, A.K.; Kane, J.M.; Sanghani, S.; Goldberg, T.E.; John, M.; et al. Electroconvulsive Therapy Augmentation in Clozapine-Resistant Schizophrenia: A Prospective, Randomized Study. Focus (Am. Psychiatr. Publ.) 2019, 17, 76–82. [Google Scholar] [CrossRef]
- Martin, D.M.; Gálvez, V.; Lauf, S.; Dong, V.; Baily, S.A.; Cardoner, N.; Chan, H.N.; Davidson, D.; Fam, J.; De Felice, N.; et al. The Clinical Alliance and Research in Electroconvulsive Therapy Network: An Australian Initiative for Improving Service Delivery of Electroconvulsive Therapy. J. ECT 2018, 34, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.W.; Tor, P.C.; Martin, D.; Loo, C. Association of Anaesthesia-ECT time interval with ECT clinical outcomes: A retrospective cohort study. J. Affect. Disord. 2021, 285, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Buckley, P.F.; Meltzer, H.Y. The brief psychiatric rating scale: Effect of scaling system on clinical response assessment. J. Clin. Psychopharmacol. 1994, 14, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Burlingame, G.; Seaman, S.; Johnson, J.; Whipple, J.; Richardson, E.J.; Rees, F.; Earnshaw, D.; Spencer, R.; Payne, M.; O’Neil, B.B. Sensitivity to change of the Brief Psychiatric Rating Scale-Extended (BPRS-E): An item and subscale analysis. Psychol. Serv. 2006, 3, 77–87. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Aas, I.H. Guidelines for rating Global Assessment of Functioning (GAF). Ann. Gen. Psychiatry 2011, 10, 2. [Google Scholar] [CrossRef]
- Arlinghaus, A.; Lombardi, D.A.; Willetts, J.L.; Folkard, S.; Christiani, D.C. A structural equation modeling approach to fatigue-related risk factors for occupational injury. Am. J. Epidemiol. 2012, 176, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Hooper, D.; Coughlan, J.P.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit; University Press of America: New York, NY, USA, 2008. [Google Scholar]
- Martin, D.M.; Gálvez, V.; Loo, C.K. Predicting Retrograde Autobiographical Memory Changes Following Electroconvulsive Therapy: Relationships between Individual, Treatment, and Early Clinical Factors. Int. J. Neuropsychopharmacol. 2015, 18, pyv067. [Google Scholar] [CrossRef] [Green Version]
- van Diermen, L.; Poljac, E.; Van der Mast, R.; Plasmans, K.; Van den Ameele, S.; Heijnen, W.; Birkenhäger, T.; Schrijvers, D.; Kamperman, A. Toward Targeted ECT: The Interdependence of Predictors of Treatment Response in Depression Further Explained. J. Clin. Psychiatry 2020, 82, 15104. [Google Scholar] [CrossRef]
- Streiner, D.L. Finding our way: An introduction to path analysis. Can. J. Psychiatry 2005, 50, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Abdin, E.; Chong, S.A.; Peh, C.X.; Vaingankar, J.A.; Chua, B.Y.; Verma, S.; Jeyagurunathan, A.; Shafie, S.; Subramaniam, M. The mediational role of physical activity, social contact and stroke on the association between age, education, employment and dementia in an Asian older adult population. BMC Psychiatry 2017, 17, 98. [Google Scholar] [CrossRef] [Green Version]
- Reichenheim, M.E.; Moraes, C.L.; Lopes, C.S.; Lobato, G. The role of intimate partner violence and other health-related social factors on postpartum common mental disorders: A survey-based structural equation modeling analysis. BMC Public Health 2014, 14, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Kim, J.H.; Youn, T.; Choi, J.G.; Jeong, S.H.; Jung, H.Y.; Kim, Y.S.; Chung, I.W. Combination of Electroconvulsive Therapy and Clozapine in Treatment-Resistant Schizophrenia. Psychiatry Investig. 2018, 15, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Kołodziej-Kowalska, E.; Pawełczyk, A.; Rabe-Jabłońska, J. Augmentation of antipsychotics with electroconvulsive therapy in treatment-resistant schizophrenia patients with dominant negative symptoms: A pilot study of effectiveness. Neuropsychobiology 2014, 70, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, T.; Kołodziej-Kowalska, E.; Pawełczyk, A.; Rabe-Jabłońska, J. Effectiveness and clinical predictors of response to combined ECT and antipsychotic therapy in patients with treatment-resistant schizophrenia and dominant negative symptoms. Psychiatry Res. 2014, 220, 175–180. [Google Scholar] [CrossRef]
- Lehnhardt, F.G.; Konkol, C.; Kuhn, J. Use of ECT in drug-refractory schizophrenia--a survey of the current literature. Fortschr. Neurol.-Psychiatr. 2012, 80, 501–511. [Google Scholar]
- Tan, X.W.; Seow, E.; Abdin, E.; Verma, S.; Sim, K.; Chong, S.A.; Subramaniam, M. Subjective quality of life among patients with schizophrenia spectrum disorder and patients with major depressive disorder. BMC Psychiatry 2019, 19, 267. [Google Scholar] [CrossRef] [Green Version]
- Lysaker, P.H.; Davis, L.W. Social function in schizophrenia and schizoaffective disorder: Associations with personality, symptoms and neurocognition. Health Qual. Life Outcomes 2004, 2, 15. [Google Scholar] [CrossRef] [Green Version]
- Lysaker, P.H.; Lancaster, R.S.; Nees, M.A.; Davis, L.W. Attributional style and symptoms as predictors of social function in schizophrenia. J. Rehabil. Res. Dev. 2004, 41, 225. [Google Scholar] [CrossRef]
- Norman, R.M.; Malla, A.K.; McLean, T.; Voruganti, L.P.N.; Cortese, L.; McIntosh, E.; Cheng, S.; Rickwood, A. The relationship of symptoms and level of functioning in schizophrenia to general wellbeing and the Quality of Life Scale. Acta Psychiatr. Scand. 2000, 102, 303–309. [Google Scholar] [CrossRef]
- Quek, Y.F.; Yang, Z.; Dauwels, J.; Lee, J. The Impact of Negative Symptoms and Neurocognition on Functioning in MDD and Schizophrenia. Front. Psychiatry 2021, 12, 648108. [Google Scholar] [CrossRef]
- Startup, M.; Jackson, M.C.; Bendix, S. The concurrent validity of the Global Assessment of Functioning (GAF). Br. J. Clin. Psychol. 2002, 41 Pt 4, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, K.; Ono, Y.; Baba, K.; Ikegami, N. The actual process of rating the global assessment of functioning scale. Compr. Psychiatry 2001, 42, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Hilsenroth, M.J.; Ackerman, S.J.; Blagys, M.D.; Baumann, B.D.; Baity, M.R.; Smith, S.R.; Price, J.L.; Smith, C.L.; Heindselman, T.L.; Mount, M.K.; et al. Reliability and validity of DSM-IV axis V. Am. J. Psychiatry 2000, 157, 1858–1863. [Google Scholar] [CrossRef] [PubMed]
- Söderberg, P.; Tungström, S.; Armelius, B.A. Reliability of global assessment of functioning ratings made by clinical psychiatric staff. Psychiatr. Serv. 2005, 56, 434–438. [Google Scholar]
- Vatnaland, T.; Vatnaland, J.; Friis, S.; Opjordsmoen, S. Are GAF scores reliable in routine clinical use? Acta Psychiatr. Scand. 2007, 115, 326–330. [Google Scholar] [CrossRef]
- Burgess, P.M.; Harris, M.G.; Coombs, T.; Pirkis, J.E. A systematic review of clinician-rated instruments to assess adults’ levels of functioning in specialised public sector mental health services. Aust. N. Z. J. Psychiatry 2017, 51, 338–354. [Google Scholar] [CrossRef]
- Burlingame, G.M.; Dunn, T.W.; Chen, S.; Lehman, A.; Axman, R.; Earnshaw, D.; Rees, F.M. Selection of outcome assessment instruments for inpatients with severe and persistent mental illness. Psychiatr. Serv. 2005, 56, 444–451. [Google Scholar] [CrossRef]
- Goldman, H.H.; Skodol, A.E.; Lave, T.R. Revising axis V for DSM-IV: A review of measures of social functioning. Am. J. Psychiatry 1992, 149, 1148–1156. [Google Scholar]
- Nieuwenstein, M.R.; Aleman, A.; de Haan, E.H. Relationship between symptom dimensions and neurocognitive functioning in schizophrenia: A meta-analysis of WCST and CPT studies. Wisconsin Card Sorting Test. Continuous Performance Test. J. Psychiatr. Res. 2001, 35, 119–125. [Google Scholar] [CrossRef]
- Bora, E.; Binnur Akdede, B.; Alptekin, K. Neurocognitive impairment in deficit and non-deficit schizophrenia: A meta-analysis. Psychol Med. 2017, 47, 2401–2413. [Google Scholar] [CrossRef]
- Curley, A.; Murphy, R.; Fleming, S.; Kelly, B.D. Age, psychiatry admission status and linear mental capacity for treatment decisions. Int. J. Law Psychiatry 2019, 66, 101469. [Google Scholar] [CrossRef] [PubMed]
- Grisso, T.; Appelbaum, P.S. The MacArthur Treatment Competence Study. III: Abilities of patients to consent to psychiatric and medical treatments. Law Hum. Behav. 1995, 19, 149–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tor, P.C.; Tan, F.J.S.; Martin, D.; Loo, C. Outcomes in patients with and without capacity in electroconvulsive therapy. J. Affect Disord 2020, 266, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lan, T.H.; Wu, B.J.; Chen, H.K.; Liao, H.Y.; Lee, S.M.; Sun, H.J. Validation of Chinese version of the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR) in patients with schizophrenia spectrum disorders. Psychiatry Res. 2013, 210, 634–640. [Google Scholar] [CrossRef]
- Moser, D.J.; Schultz, S.K.; Arndt, S.; Benjamin, M.L.; Fleming, F.W.; Brems, C.S.; Paulsen, J.S.; Appelbaum, P.S.; Andreasen, N.C. Capacity to provide informed consent for participation in schizophrenia and HIV research. Am. J. Psychiatry 2002, 159, 1201–1207. [Google Scholar] [CrossRef]
- Stroup, S.; Appelbaum, P.; Swartz, M.; Patel, M.; Davis, S.; Jeste, D.; Kim, S.; Keefe, R.; Manschreck, T.; McEvoy, J.; et al. Decision-making capacity for research participation among individuals in the CATIE schizophrenia trial. Schizophr. Res. 2005, 80, 1–8. [Google Scholar] [CrossRef]
- Gray, J.D.; McEwen, B.S. Lithium’s role in neural plasticity and its implications for mood disorders. Acta Psychiatr. Scand. 2013, 128, 347–361. [Google Scholar] [CrossRef]
- Roy, U.; Mukherjee, B.P. Correlation of lithium effect on electroshock-induced seizure in rats with its concentration in brain and plasma. Arch. Int. Pharmacodyn. Ther. 1982, 255, 81–88. [Google Scholar]
- Schmidt, J. Lithium suppresses seizure susceptibility in pentylenetetrazol-kindled rats. Biomed. Biochim. Acta 1986, 45, 1167–1172. [Google Scholar] [PubMed]
- Patel, R.S.; Bachu, A.; Youssef, N.A. Combination of lithium and electroconvulsive therapy (ECT) is associated with higher odds of delirium and cognitive problems in a large national sample across the United States. Brain Stimul. 2020, 13, 15–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total Sample (n = 340) | Negative Symptoms Improvement (196, 57.6%) | Negative Symptoms No Change (53, 15.5%) | Negative Symptoms Deterioration (91, 26.7%) | ||||
|---|---|---|---|---|---|---|---|---|
| Age (years, mean ± SD) | 40.9 ± 14.5 | 39.8 ± 14 | 42.3 ± 14.5 | 42.6 ± 15.3 | ||||
| Number of ECT sessions (mean ± SD) | 7.2 ± 2.4 | 7.3 ± 2.4 | 6.9 ± 1.9 | 7.4 ± 2.6 | ||||
| Gender (N, %) | Female | 174 | 96 | 55.2% | 31 | 17.8% | 47 | 27.0% |
| Male | 166 | 100 | 60.2% | 22 | 13.3% | 44 | 26.5% | |
| Admission status # (N, %) | Voluntary | 156 | 90 | 57.7% | 26 | 16.7% | 40 | 25.6% |
| Involuntary | 183 | 105 | 57.4% | 27 | 14.8% | 51 | 27.9% | |
| Consent # (N, %) | Own Consent | 55 | 39 | 70.9% | 9 | 16.4% | 7 | 12.7% |
| Consent by others | 281 | 154 | 54.8% | 44 | 15.7% | 83 | 29.5% | |
| No of previous episodes # (N, %) | >3 | 230 | 130 | 56.5% | 33 | 14.3% | 67 | 29.1% |
| 1–3 | 98 | 57 | 58.2% | 20 | 20.4% | 21 | 21.4% | |
| 0 | 11 | 8 | 72.7% | 0 | 0.0% | 3 | 27.3% | |
| Antidepressant # (N, %) | YES | 99 | 60 | 60.6% | 18 | 18.2% | 21 | 21.2% |
| NO | 239 | 134 | 56.1% | 35 | 14.6% | 70 | 29.3% | |
| Antipsychotics other than clozapine # (N, %) | YES | 309 | 171 | 55.3% | 50 | 16.2% | 88 | 28.5% |
| NO | 28 | 23 | 82.1% | 3 | 10.7% | 2 | 7.1% | |
| Clozapine # (N, %) | YES | 108 | 70 | 64.8% | 10 | 9.3% | 28 | 25.9% |
| NO | 225 | 122 | 54.2% | 41 | 18.2% | 62 | 27.6% | |
| Lithium # (N, %) | YES | 21 | 17 | 81.0% | 2 | 9.5% | 2 | 9.5% |
| NO | 317 | 177 | 55.8% | 51 | 16.1% | 89 | 28.1% | |
| Benzodiazepines # (N, %) | YES | 190 | 109 | 57.4% | 24 | 12.6% | 57 | 30.0% |
| NO | 148 | 85 | 57.4% | 29 | 19.6% | 34 | 23.0% | |
| Anticonvulsant # (N, %) | YES | 79 | 45 | 57.0% | 13 | 16.5% | 21 | 26.6% |
| NO | 258 | 149 | 57.8% | 39 | 15.1% | 70 | 27.1% | |
| Failed Antipsychotics # (N, %) | ≥3 | 220 | 132 | 60.0% | 29 | 13.2% | 59 | 26.8% |
| 1–2 | 102 | 55 | 53.9% | 19 | 18.6% | 28 | 27.5% | |
| 0 | 14 | 6 | 42.9% | 4 | 28.6% | 4 | 28.6% | |
| ECT type # (N, %) | Bifrontal | 274 | 163 | 59.5% | 37 | 13.5% | 74 | 27.0% |
| Bitemporal | 48 | 25 | 52.1% | 9 | 18.8% | 14 | 29.2% | |
| Right unilateral | 17 | 8 | 47.1% | 6 | 35.3% | 3 | 17.6% | |
| r | se | p Value | ||
|---|---|---|---|---|
| From: | to Change of GAF | |||
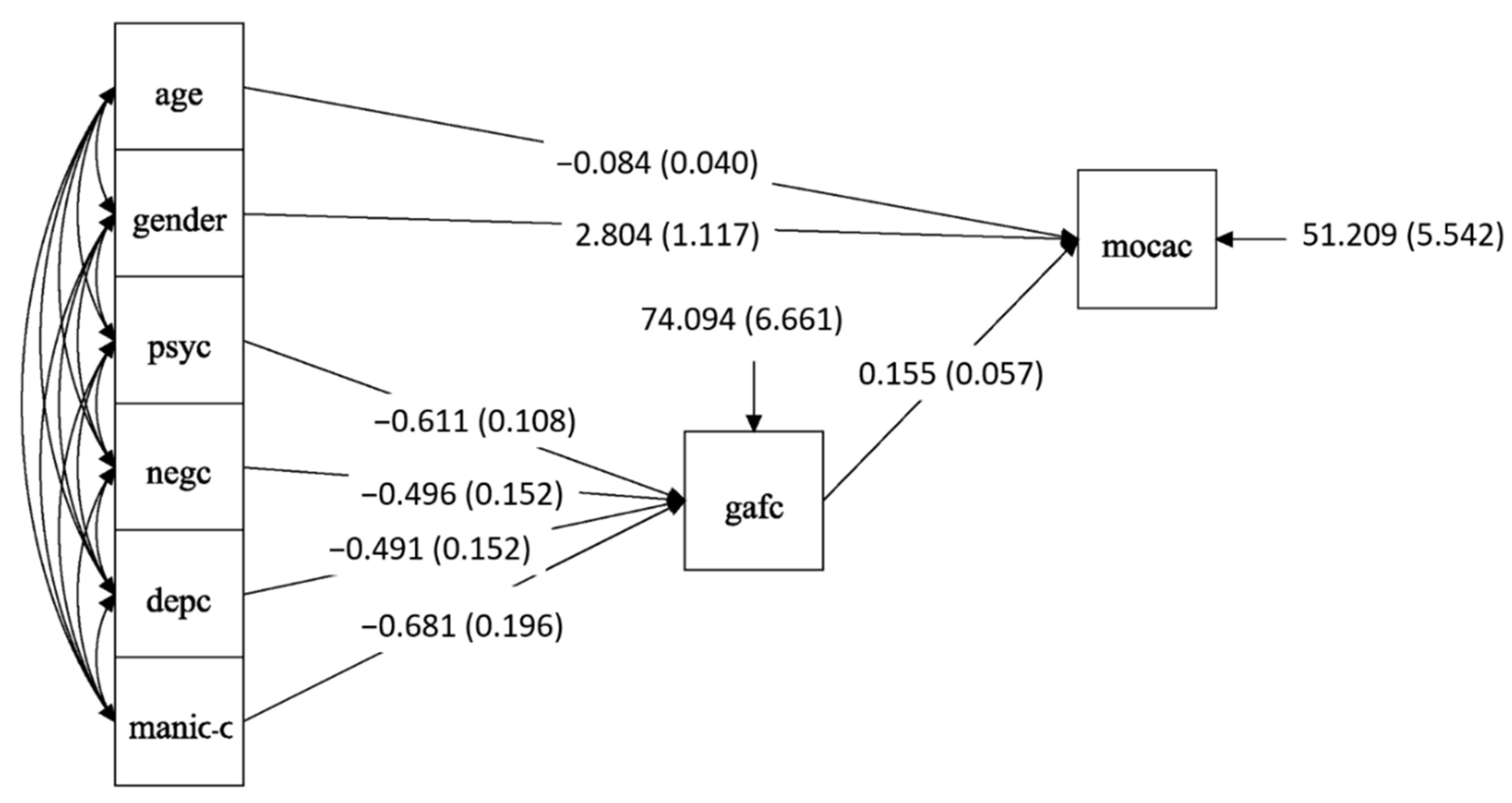
| Change of positive symptoms | direct effect | −0.611 | 0.108 | <0.001 ** |
| Change of negative symptoms | direct effect | −0.496 | 0.152 | 0.001 ** |
| Change of depressive symptoms | direct effect | −0.491 | 0.152 | 0.001 ** |
| Change of manic symptoms | direct effect | −0.681 | 0.196 | 0.001 ** |
| From: | to Change of MoCA | |||
| Age | direct effect | −0.084 | 0.040 | 0.034 * |
| Female gender (vs. male) | direct effect | 2.804 | 1.117 | 0.012 * |
| Change of GAF | direct effect | 0.155 | 0.057 | 0.007 ** |
| Change of positive symptoms | indirect effect | −0.095 | 0.038 | 0.014 * |
| Change of negative symptoms | indirect effect | −0.077 | 0.037 | 0.035 * |
| Change of depressive symptoms | indirect effect | −0.076 | 0.036 | 0.034 * |
| Change of manic symptoms | indirect effect | −0.106 | 0.050 | 0.035 * |
| Model fit: χ2, p = 0.278; RMSEA = 0.03; CFI = 0.985; SRMR = 0.045 | ||||
| r | se | p Value | ||
|---|---|---|---|---|
| From: | To: Own consent | |||
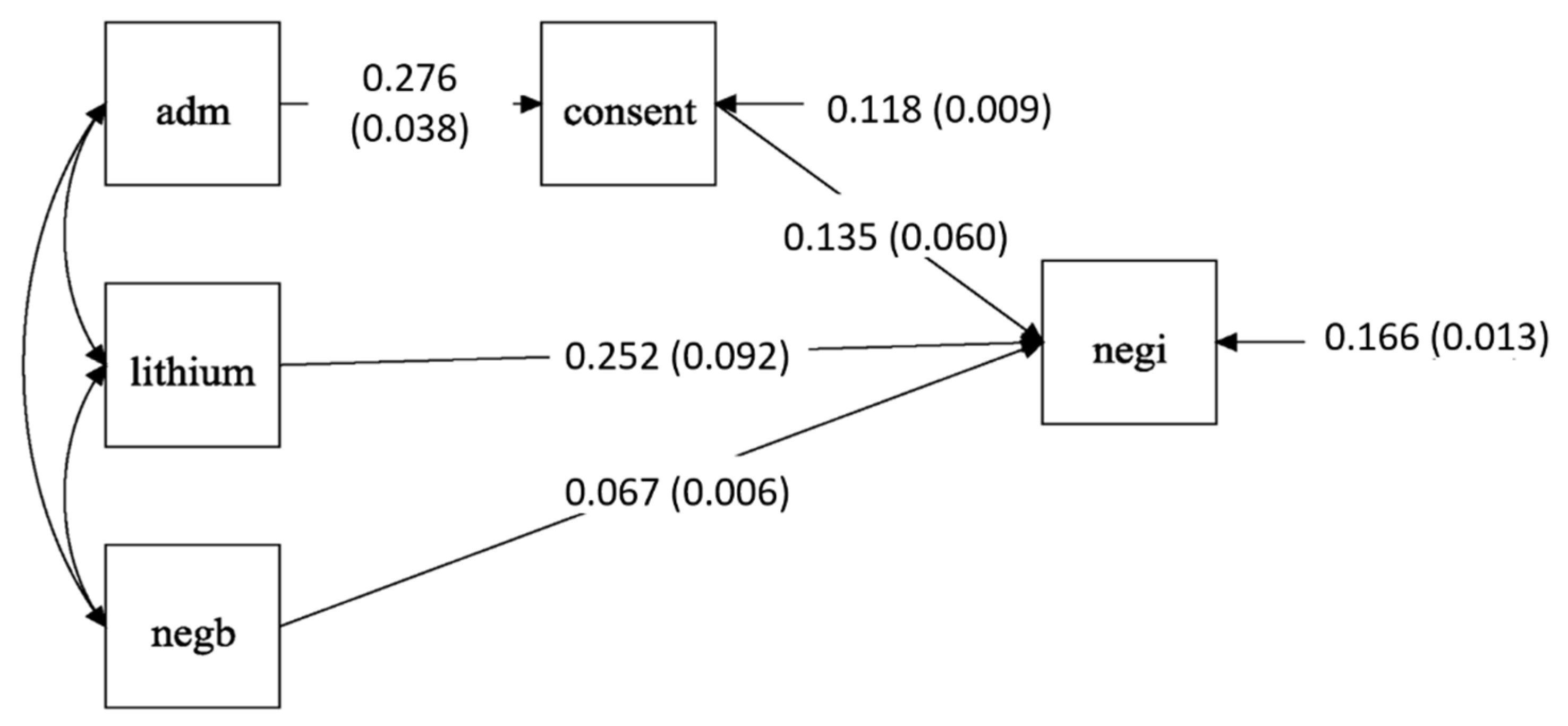
| Voluntary admission status (vs. involuntary) | direct effect | 0.276 | 0.038 | <0.001 ** |
| From: | To: Negative symptoms improvement | |||
| Own consent (vs. consent by others) | direct effect | 0.135 | 0.06 | 0.025 * |
| With lithium (vs. without lithium) | direct effect | 0.252 | 0.152 | 0.006 ** |
| Baseline negative symptoms score | direct effect | 0.067 | 0.006 | <0.001 ** |
| Voluntary admission status (vs. involuntary) | indirect effect | 0.037 | 0.017 | 0.032 * |
| Model fit: χ2, p = 0.183; RMSEA = 0.043; CFI = 0.990; SRMR = 0.027 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, X.; Martin, D.; Lee, J.; Tor, P.C. The Impact of Electroconvulsive Therapy on Negative Symptoms in Schizophrenia and Their Association with Clinical Outcomes. Brain Sci. 2022, 12, 545. https://doi.org/10.3390/brainsci12050545
Tan X, Martin D, Lee J, Tor PC. The Impact of Electroconvulsive Therapy on Negative Symptoms in Schizophrenia and Their Association with Clinical Outcomes. Brain Sciences. 2022; 12(5):545. https://doi.org/10.3390/brainsci12050545
Chicago/Turabian StyleTan, Xiaowei, Donel Martin, Jimmy Lee, and Phern Chern Tor. 2022. "The Impact of Electroconvulsive Therapy on Negative Symptoms in Schizophrenia and Their Association with Clinical Outcomes" Brain Sciences 12, no. 5: 545. https://doi.org/10.3390/brainsci12050545
APA StyleTan, X., Martin, D., Lee, J., & Tor, P. C. (2022). The Impact of Electroconvulsive Therapy on Negative Symptoms in Schizophrenia and Their Association with Clinical Outcomes. Brain Sciences, 12(5), 545. https://doi.org/10.3390/brainsci12050545