
A Cross-Sectional Comparison of Arterial Stiffness and Cognitive Performances in Physically Active Late Pre- and Early Post-Menopausal Females

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Blood Samples
2.4. Vascular Assessment
2.5. Neuropsychological Assessment
2.6. Maximal Cardiopulmonary Exercise
2.7. Menopausal Symptoms
2.8. Statistics
3. Results
3.1. Participant Characteristics
3.2. Cardiovascular Assessment
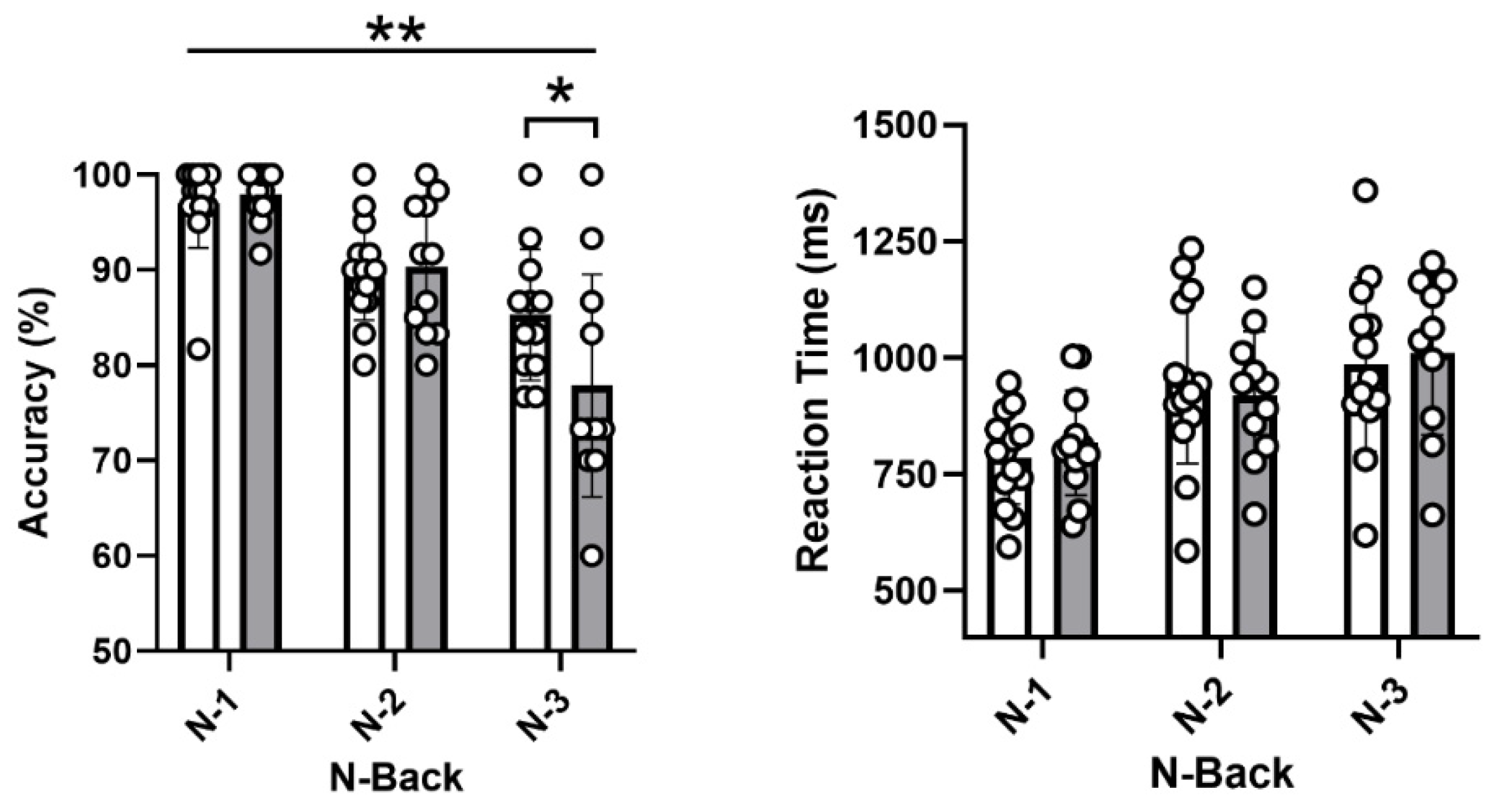
3.3. Neuropsychological Assessment
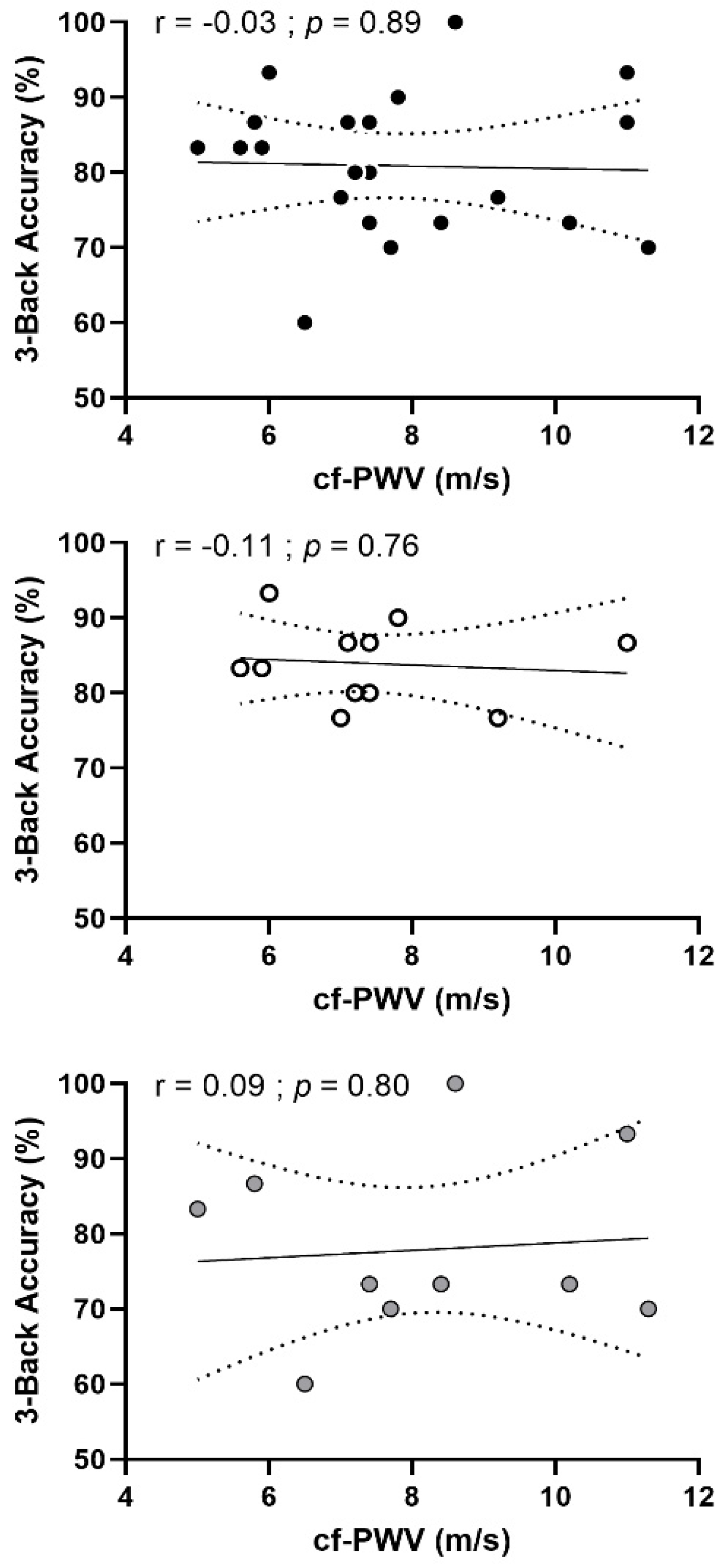
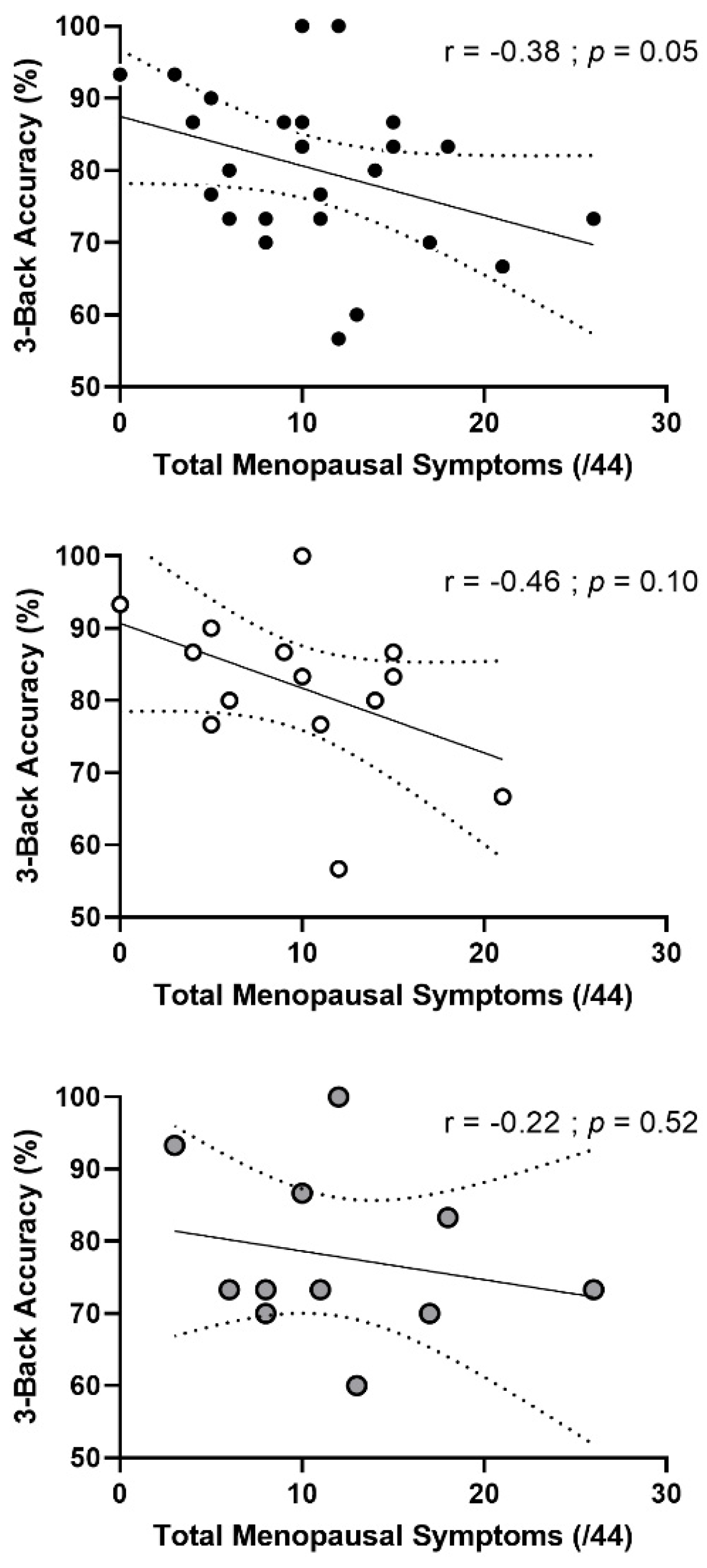
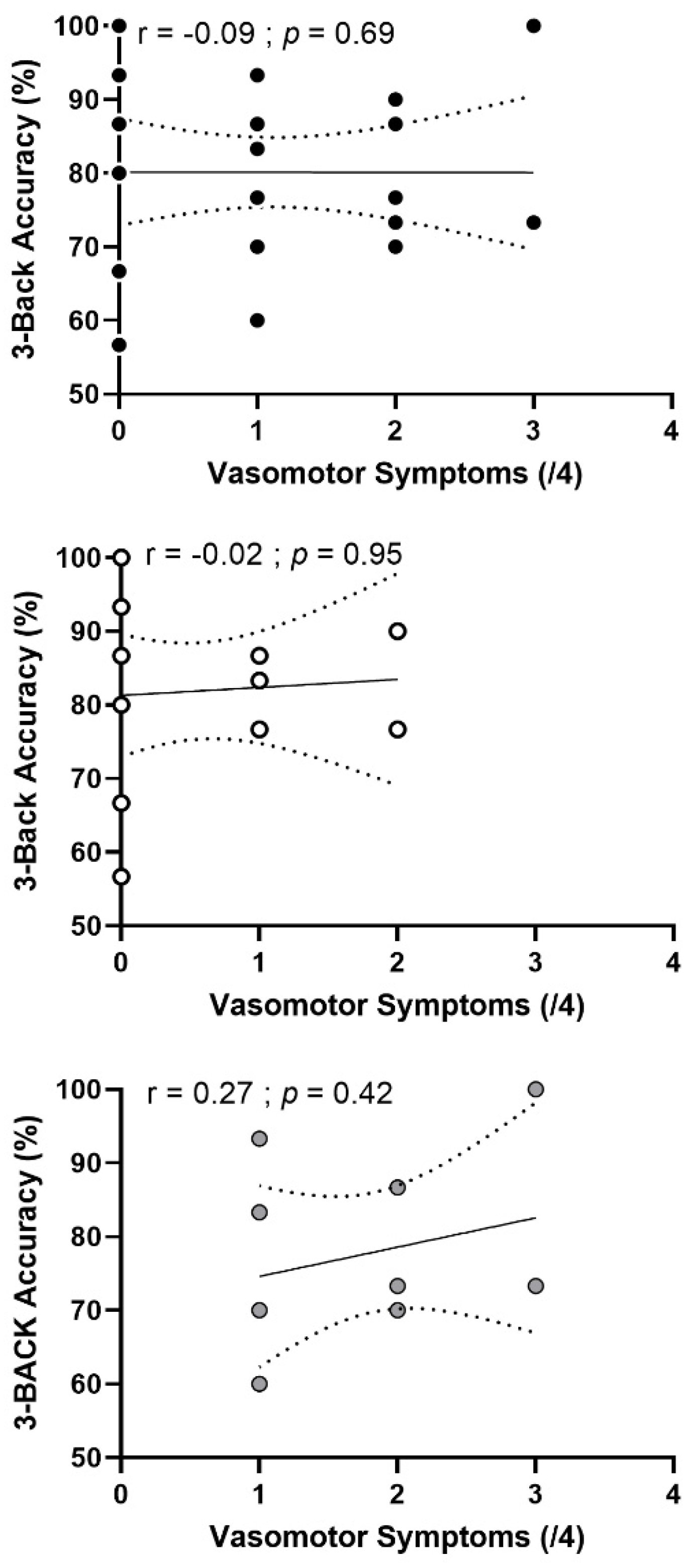
3.4. Correlation Analyses
3.5. Moderation Analysis
4. Discussion
4.1. Menopause, Physical Activity and Arterial Stiffness
4.2. Menopause, Arterial Stiffness and Executive Function
4.3. Menopause and Episodic Memory
4.4. Menopausal Symptoms and Cognitive Performance
4.5. Limits and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Roos, A.; van der Grond, J.; Mitchell, G.; Westenberg, J. Magnetic Resonance Imaging of Cardiovascular Function and the Brain: Is Dementia a Cardiovascular-Driven Disease? Circulation 2017, 135, 2178–2195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rensma, S.P.; Stehouwer, C.D.A.; Van Boxtel, M.P.J.; Houben, A.J.H.M.; Berendschot, T.T.J.M.; Jansen, J.F.A.; Schalkwijk, C.G.; Verhey, F.R.J.; Kroon, A.A.; Henry, R.M.A.; et al. Associations of Arterial Stiffness with Cognitive Performance, and the Role of Microvascular Dysfunction: The Maastricht Study. Hypertension 2020, 75, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Thorin-Trescases, N.; de Montgolfier, O.; Pinçon, A.; Raignault, A.; Caland, L.; Labbé, P.; Thorin, E. Impact of Pulse Pressure on Cerebrovascular Events Leading to Age-Related Cognitive Decline. Am. J. Physiol.-Heart Circ. Physiol. 2018, 314, H1214–H1224. [Google Scholar] [CrossRef]
- Tomoto, T.; Liu, J.; Tseng, B.Y.; Pasha, E.P.; Cardim, D.; Tarumi, T.; Hynan, L.S.; Munro Cullum, C.; Zhang, R. One-Year Aerobic Exercise Reduced Carotid Arterial Stiffness and Increased Cerebral Blood Flow in Amnestic Mild Cognitive Impairment. J. Alzheimers Dis. JAD 2021, 80, 841–853. [Google Scholar] [CrossRef]
- Alvarez-Bueno, C.; Cunha, P.G.; Martinez-Vizcaino, V.; Pozuelo-Carrascosa, D.P.; Visier-Alfonso, M.E.; Jimenez-Lopez, E.; Cavero-Redondo, I. Arterial Stiffness and Cognition Among Adults: A Systematic Review and Meta-Analysis of Observational and Longitudinal Studies. J. Am. Heart Assoc. 2020, 9, e014621. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert Consensus Document on Arterial Stiffness: Methodological Issues and Clinical Applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pertesi, S.; Coughlan, G.; Puthusseryppady, V.; Morris, E.; Hornberger, M. Menopause, Cognition and Dementia—A Review. Post Reprod. Health 2019, 25, 200–206. [Google Scholar] [CrossRef]
- Samargandy, S.; Matthews, K.A.; Brooks, M.M.; Barinas-Mitchell, E.; Magnani, J.W.; Janssen, I.; Hollenberg, S.M.; El Khoudary, S.R. Arterial Stiffness Accelerates Within 1 Year of the Final Menstrual Period: The SWAN Heart Study. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1001–1008. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A.; et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e506–e532. [Google Scholar] [CrossRef]
- Volgman, A.S.; Bairey Merz, C.N.; Aggarwal, N.T.; Bittner, V.; Bunch, T.J.; Gorelick, P.B.; Maki, P.; Patel, H.N.; Poppas, A.; Ruskin, J.; et al. Sex Differences in Cardiovascular Disease and Cognitive Impairment: Another Health Disparity for Women? J. Am. Heart Assoc. 2019, 8, e013154. [Google Scholar] [CrossRef]
- Thurston, R.C.; Aslanidou Vlachos, H.E.; Derby, C.A.; Jackson, E.A.; Brooks, M.M.; Matthews, K.A.; Harlow, S.; Joffe, H.; El Khoudary, S.R. Menopausal Vasomotor Symptoms and Risk of Incident Cardiovascular Disease Events in SWAN. J. Am. Heart Assoc. 2021, 10, e017416. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Kaur, M. Is Cognitive Performance of Women Sensitive to the Severity of Menopausal Symptoms? Menopause 2022, 29, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Epperson, C.N.; Sammel, M.D.; Freeman, E.W. Menopause Effects on Verbal Memory: Findings from a Longitudinal Community Cohort. J. Clin. Endocrinol. Metab. 2013, 98, 3829–3838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luetters, C.; Huang, M.-H.; Seeman, T.; Buckwalter, G.; Meyer, P.M.; Avis, N.E.; Sternfeld, B.; Johnston, J.M.; Greendale, G.A. Menopause Transition Stage and Endogenous Estradiol and Follicle-Stimulating Hormone Levels Are Not Related to Cognitive Performance: Cross-Sectional Results from the Study of Women’s Health across the Nation (SWAN). J. Womens Health 2007, 16, 331–344. [Google Scholar] [CrossRef]
- Brinton, R.D. Estrogen-Induced Plasticity from Cells to Circuits: Predictions for Cognitive Function. Trends Pharmacol. Sci. 2009, 30, 212–222. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Lyu, P.; Ren, Y.; An, J.; Dong, Y. Arterial Stiffness and Cognitive Impairment. J. Neurol. Sci. 2017, 380, 1–10. [Google Scholar] [CrossRef]
- Tanaka, H. Antiaging Effects of Aerobic Exercise on Systemic Arteries. Hypertension 2019, 74, 237–242. [Google Scholar] [CrossRef]
- Loaiza-Betancur, A.F.; Chulvi-Medrano, I.; Díaz-López, V.A.; Gómez-Tomás, C. The Effect of Exercise Training on Blood Pressure in Menopause and Postmenopausal Women: A Systematic Review of Randomized Controlled Trials. Maturitas 2021, 149, 40–55. [Google Scholar] [CrossRef]
- Xi, H.; He, Y.; Niu, Y.; Sui, X.; Zhang, J.; Zhu, R.; Xu, H.; Zhang, S.; Li, Y.; Yuan, Y.; et al. Effect of Combined Aerobic and Resistance Exercise on Blood Pressure in Postmenopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Exp. Gerontol. 2021, 155, 111560. [Google Scholar] [CrossRef]
- Yau, S.Y.; Li, A.; Sun, X.; Fontaine, C.J.; Christie, B.R.; So, K.-F. Potential Biomarkers for Physical Exercise-Induced Brain Health. In Role of Biomarkers in Medicine; Wang, M., Witzmann, F.A., Eds.; InTech: Rijeka, Croatia, 2016; ISBN 978-953-51-2505-1. [Google Scholar]
- DuPont, J.J.; Kenney, R.M.; Patel, A.R.; Jaffe, I.Z. Sex Differences in Mechanisms of Arterial Stiffness. Br. J. Pharmacol. 2019, 176, 4208–4225. [Google Scholar] [CrossRef]
- Debray, A.; Enea, C.; Ravanelli, N.; Chaseling, G.K.; Gravel, H.; Bosquet, L.; Bherer, L.; Gagnon, D. Comparison of Blood Pressure and Vascular Health in Physically Active Late Pre- and Early Postmenopausal Females. Med. Sci. Sports Exerc. 2022, 54, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement from the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Kane, M.J.; Conway, A.R.A.; Miura, T.K.; Colflesh, G.J.H. Working Memory, Attention Control, and the N-Back Task: A Question of Construct Validity. J. Exp. Psychol. Learn. Mem. Cogn. 2007, 33, 615–622. [Google Scholar] [CrossRef] [Green Version]
- Wylie, G.; Allport, A. Task Switching and the Measurement of “Switch Costs”. Psychol. Res. 2000, 63, 212–233. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, B.N.; Ryan, J.J. Prorating Wechsler Adult Intelligence Scale-III Summary Scores. J. Clin. Psychol. 2000, 56, 807–811. [Google Scholar] [CrossRef]
- Ryan, J.J.; Sattler, J.M.; Lopez, S.J. Age Effects on Wechsler Adult Intelligence Scale-III Subtests. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2000, 15, 311–317. [Google Scholar] [CrossRef]
- Stallings, G.; Boake, C.; Sherer, M. Comparison of the California Verbal Learning Test and the Rey Auditory Verbal Learning Test in Head-Injured Patients. J. Clin. Exp. Neuropsychol. 1995, 17, 706–712. [Google Scholar] [CrossRef]
- Bohnen, N.; Twijnstra, A.; Jolles, J. Performance in the Stroop Color Word Test in Relationship to the Persistence of Symptoms Following Mild Head Injury. Acta Neurol. Scand. 1992, 85, 116–121. [Google Scholar] [CrossRef]
- Aadland, E.; Solbraa, A.K.; Resaland, G.K.; Steene-Johannessen, J.; Edvardsen, E.; Hansen, B.H.; Anderssen, S.A. Reference Values for and Cross-Validation of Time to Exhaustion on a Modified Balke Protocol in Norwegian Men and Women. Scand. J. Med. Sci. Sports 2017, 27, 1248–1257. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, K.; Ruebig, A.; Potthoff, P.; Schneider, H.P.G.; Strelow, F.; Heinemann, L.A.J.; Do, M.T. The Menopause Rating Scale (MRS) Scale: A Methodological Review. Health Qual. Life Outcomes 2004, 2, 45. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.; Jiang, S.; Geng, L.; Li, C.; Tao, M. Correlation between Menopausal Symptoms and Everyday Cognition in Chinese (Peri)Menopausal Women. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2021, 37, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; DeSouza, C.A.; Seals, D.R. Absence of Age-Related Increase in Central Arterial Stiffness in Physically Active Women. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 127–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casey, D.P.; Pierce, G.L.; Howe, K.S.; Mering, M.C.; Braith, R.W. Effect of Resistance Training on Arterial Wave Reflection and Brachial Artery Reactivity in Normotensive Postmenopausal Women. Eur. J. Appl. Physiol. 2007, 100, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Moreau, K. Regular Exercise, Hormone Replacement Therapy and the Age-Related Decline in Carotid Arterial Compliance in Healthy Women. Cardiovasc. Res. 2003, 57, 861–868. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Son, W.-M.; Chernykh, O.; Park, S.-Y. The Effects of Stair Climbing on Arterial Stiffness, Blood Pressure, and Leg Strength in Postmenopausal Women with Stage 2 Hypertension. Menopause 2018, 25, 731–737. [Google Scholar] [CrossRef]
- Stamatelopoulos, K.; Tsoltos, N.; Armeni, E.; Paschou, S.A.; Augoulea, A.; Kaparos, G.; Rizos, D.; Karagouni, I.; Delialis, D.; Ioannou, S.; et al. Physical Activity Is Associated with Lower Arterial Stiffness in Normal-Weight Postmenopausal Women. J. Clin. Hypertens. Greenwich Conn. 2020, 22, 1682–1690. [Google Scholar] [CrossRef]
- Inaraja, V.; Thuissard, I.; Andreu-Vazquez, C.; Jodar, E. Lipid Profile Changes during the Menopausal Transition. Menopause 2020, 27, 780–787. [Google Scholar] [CrossRef]
- Hou, Q.; Li, S.; Gao, Y.; Tian, H. Relations of Lipid Parameters, Other Variables with Carotid Intima-Media Thickness and Plaque in the General Chinese Adults: An Observational Study. Lipids Health Dis. 2018, 17, 107. [Google Scholar] [CrossRef] [Green Version]
- Singer, J.; Trollor, J.N.; Crawford, J.; O’Rourke, M.F.; Baune, B.T.; Brodaty, H.; Samaras, K.; Kochan, N.A.; Campbell, L.; Sachdev, P.S.; et al. The Association between Pulse Wave Velocity and Cognitive Function: The Sydney Memory and Ageing Study. PLoS ONE 2013, 8, e61855. [Google Scholar] [CrossRef] [Green Version]
- Duff, S.J.; Hampson, E. A Beneficial Effect of Estrogen on Working Memory in Postmenopausal Women Taking Hormone Replacement Therapy. Horm. Behav. 2000, 38, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Keenan, P.A.; Ezzat, W.H.; Ginsburg, K.; Moore, G.J. Prefrontal Cortex as the Site of Estrogen’s Effect on Cognition. Psychoneuroendocrinology 2001, 26, 577–590. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Beskou-Kontou, T.; Theodoridis, I.; Skalkidou, A.; Petridou, E.T. Surgical Menopause in Association with Cognitive Function and Risk of Dementia: A Systematic Review and Meta-Analysis. Psychoneuroendocrinology 2019, 106, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Dumas, J.A.; Kutz, A.M.; Naylor, M.R.; Johnson, J.V.; Newhouse, P.A. Increased Memory Load-Related Frontal Activation after Estradiol Treatment in Postmenopausal Women. Horm. Behav. 2010, 58, 929–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greendale, G.A.; Wight, R.G.; Huang, M.H.; Avis, N.; Gold, E.B.; Joffe, H.; Seeman, T.; Vuge, M.; Karlamangla, A.S. Menopause-Associated Symptoms and Cognitive Performance: Results from the Study of Women’s Health Across the Nation. Am. J. Epidemiol. 2010, 171, 1214–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, D.; Correia, R.; Nieto, A.; Machado, A.; Molina, Y.; Barroso, J. Cognitive Decline before the Age of 50 Can Be Detected with Sensitive Cognitive Measures. Psicothema 2015, 27, 216–222. [Google Scholar] [CrossRef]
- Henderson, V.W. Cognitive Changes after Menopause: Influence of Estrogen. Clin. Obstet. Gynecol. 2008, 51, 618–626. [Google Scholar] [CrossRef]
- Maki, P.M.; Gast, M.J.; Vieweg, A.J.; Burriss, S.W.; Yaffe, K. Hormone Therapy in Menopausal Women with Cognitive Complaints: A Randomized, Double-Blind Trial. Neurology 2007, 69, 1322–1330. [Google Scholar] [CrossRef]
- Soares, C.N. Vasomotor Symptoms, Cognition, and Breast Cancer: Another Important Piece of the Puzzle. Menopause 2020, 27, 1202–1204. [Google Scholar] [CrossRef]
- Avis, N.E.; Crawford, S.L.; Greendale, G.; Bromberger, J.T.; Everson-Rose, S.A.; Gold, E.B.; Hess, R.; Joffe, H.; Kravitz, H.M.; Tepper, P.G.; et al. Duration of Menopausal Vasomotor Symptoms over the Menopause Transition. JAMA Intern. Med. 2015, 175, 531–539. [Google Scholar] [CrossRef]
- Dibonaventura, M.D.; Chandran, A.; Hsu, M.-A.; Bushmakin, A. Burden of Vasomotor Symptoms in France, Germany, Italy, Spain, and the United Kingdom. Int. J. Womens Health 2013, 5, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, S.D.; Lampe, J.W.; Qu, C.; Gundersen, G.; Fuller, S.; Copeland, W.K.; Newton, K.M. Self-Reported Menopausal Symptoms in a Racially Diverse Population and Soy Food Consumption. Maturitas 2013, 75, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Muka, T.; Oliver-Williams, C.; Kunutsor, S.; Laven, J.S.E.; Fauser, B.C.J.M.; Chowdhury, R.; Kavousi, M.; Franco, O.H. Association of Age at Onset of Menopause and Time Since Onset of Menopause with Cardiovascular Outcomes, Intermediate Vascular Traits, and All-Cause Mortality: A Systematic Review and Meta-Analysis. JAMA Cardiol. 2016, 1, 767–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regestein, Q.; Friebely, J.; Schiff, I. How Self-Reported Hot Flashes May Relate to Affect, Cognitive Performance and Sleep. Maturitas 2015, 81, 449–455. [Google Scholar] [CrossRef]
- Weber, M.; Mapstone, M. Memory Complaints and Memory Performance in the Menopausal Transition. Menopause 2009, 16, 694–700. [Google Scholar] [CrossRef]
- Bailey, T.G.; Cable, N.T.; Aziz, N.; Dobson, R.; Sprung, V.S.; Low, D.A.; Jones, H. Exercise Training Reduces the Frequency of Menopausal Hot Flushes by Improving Thermoregulatory Control. Menopause 2016, 23, 708–718. [Google Scholar] [CrossRef]
- Elavsky, S.; McAuley, E. Physical Activity and Mental Health Outcomes during Menopause: A Randomized Controlled Trial. Ann. Behav. Med. Publ. Soc. Behav. Med. 2007, 33, 132–142. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Menopause (n = 16) | Post-Menopause (n = 14) | p Value | Cohen’s d | |
|---|---|---|---|---|
| Age (years) | 48 ± 2 | 53 ± 2 | <0.01 | >0.8 |
| Education (years) | 19 ± 3 | 19 ± 3 | 0.51 | <0.2 |
| BMI (kg/m2) | 23.8 ± 3.5 | 22.2 ± 2.8 | 0.19 | <0.2 |
| Fat mass (%) | 29.1 ± 5.5 | 28.4 ± 7.1 | 0.74 | <0.2 |
| Body mass (kg) | 63.5 ± 9.7 | 59.9 ± 8.8 | 0.52 | <0.2 |
| Total cholesterol (mmol/L) | 4.8 ± 0.7 | 6.2 ± 1.6 | <0.01 | 0.8 |
| LDL (mmol/L) | 2.5 ± 0.6 | 3.5 ± 1.3 | 0.01 | 1.0 |
| HDL (mmol/L) | 1.9 ± 0.3 | 2.3 ± 0.4 | 0.02 | 0.9 |
| Triglycerides (mmol/L) | 0.9 ± 0.3 | 0.8 ± 0.3 | 0.64 | <0.2 |
| Total Cholesterol/HDL | 2.6 ± 0.5 | 2.7 ± 0.5 | 0.40 | 0.3 |
| LDL/HDL | 1.3 ± 0.5 | 1.5 ± 0.4 | 0.26 | 0.4 |
| Estradiols (pmol/L) | 267.0 ± 179.1 | <36.7 | <0.01 | <0.2 |
| MVPA (min/week) | 490 ± 214 | 550 ± 303 | 0.87 | 0.2 |
| VO2max (mL/min/kg) | 35.8 ± 6.0 | 34.0 ± 6.1 | 0.18 | <0.2 |
| Neuropsychological Tests | Pre-Menopause (n = 16) | Post-Menopause (n = 14) | p Value | Eta Squared ŋ2 |
|---|---|---|---|---|
| MoCA (/30) | 29 ± 1 | 28 ± 1 | 0.26 | 0.05 |
| DSST (/133) | 88 ± 14 | 84 ± 12 | 0.51 | 0.02 |
| TMT A (s) | 27.2 ± 8.5 | 29.6 ± 8.6 | 0.06 | 0.12 |
| TMT B (s) | 51.5 ± 11.7 | 56.0 ± 14.6 | 0.40 | 0.03 |
| TMT (B-A)/A | 0.97 ± 0.46 | 0.98 ± 0.52 | 0.52 | 0.02 |
| EMPAN forward (/8) | 5.5 ± 0.7 | 5.4 ± 1.2 | 0.26 | 0.05 |
| EMPAN backward (/7) | 4.2 ± 1.3 | 3.9 ± 1.3 | 0.07 | 0.11 |
| Stroop test—Accuracy (%) | ||||
| Naming | 99.0 ± 1.5 | 98.3 ± 2.4 | 0.87 | <0.01 |
| Inhibition | 99.2 ± 1.0 | 98.4 ± 1.9 | 0.72 | <0.01 |
| Switching | 92.0 ± 6.4 | 87.6 ± 12.2 | 0.88 | <0.01 |
| Stroop test—Reaction Time (ms) | ||||
| Naming (N) | 727 ± 113 | 766 ± 160 | 0.33 | 0.04 |
| Inhibition (I) | 783 ± 72 | 863 ± 158 | 0.54 | 0.01 |
| Switching (S) | 1092 ± 182 | 1263 ± 289 | 0.58 | 0.01 |
| Stroop (I-N)/N | 0.10 ± 0.16 | 0.15 ± 0.21 | 0.60 | 0.01 |
| Stroop (S-I)/I | 0.40 ± 0.22 | 0.48 ± 0.27 | 0.95 | <0.01 |
| N-Back test—Accuracy (%) | ||||
| 1-Back | 96.8 ± 4.6 | 96.1 ± 5.7 | 0.98 | <0.01 |
| 2-Back | 89.9 ± 5.2 | 90.3 ± 6.7 | 0.84 | <0.01 |
| 3-Back | 83.9 ± 8.0 | 77.9 ± 11.1 | 0.02 | 0.36 |
| N-Back—Reaction Time (ms) | ||||
| 1-Back | 780 ± 98 | 800 ± 95 | 0.80 | <0.01 |
| 2-Back | 951 ± 179 | 918 ± 133 | 0.46 | 0.03 |
| 3-Back | 1047 ± 259 | 1055 ± 214 | 0.46 | <0.01 |
| N-Back (2-1)/1 | 0.23 ± 0.26 | 0.15 ± 0.10 | 0.60 | 0.01 |
| N-Back (3-2)/2 | 0.10 ± 0.13 | 0.15 ± 0.16 | 0.95 | <0.01 |
| RAVLT | ||||
| Rey 1–5 total words (/75) | 58 ± 8 | 55 ± 8 | 0.61 | 0.09 |
| Immediate recall (/15) | 13 ± 2 | 12 ± 2 | 0.73 | <0.01 |
| Delayed recall (/15) | 13 ± 1 | 12 ± 2 | 0.61 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Debray, A.; Bherer, L.; Gagnon, C.; Bosquet, L.; Hay, E.; Bartlett, A.-A.; Gagnon, D.; Enea, C. A Cross-Sectional Comparison of Arterial Stiffness and Cognitive Performances in Physically Active Late Pre- and Early Post-Menopausal Females. Brain Sci. 2022, 12, 901. https://doi.org/10.3390/brainsci12070901
Debray A, Bherer L, Gagnon C, Bosquet L, Hay E, Bartlett A-A, Gagnon D, Enea C. A Cross-Sectional Comparison of Arterial Stiffness and Cognitive Performances in Physically Active Late Pre- and Early Post-Menopausal Females. Brain Sciences. 2022; 12(7):901. https://doi.org/10.3390/brainsci12070901
Chicago/Turabian StyleDebray, Amélie, Louis Bherer, Christine Gagnon, Laurent Bosquet, Eva Hay, Audrey-Ann Bartlett, Daniel Gagnon, and Carina Enea. 2022. "A Cross-Sectional Comparison of Arterial Stiffness and Cognitive Performances in Physically Active Late Pre- and Early Post-Menopausal Females" Brain Sciences 12, no. 7: 901. https://doi.org/10.3390/brainsci12070901
APA StyleDebray, A., Bherer, L., Gagnon, C., Bosquet, L., Hay, E., Bartlett, A. -A., Gagnon, D., & Enea, C. (2022). A Cross-Sectional Comparison of Arterial Stiffness and Cognitive Performances in Physically Active Late Pre- and Early Post-Menopausal Females. Brain Sciences, 12(7), 901. https://doi.org/10.3390/brainsci12070901