
The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review



 , ,
, ,
Abstract
:1. Introduction
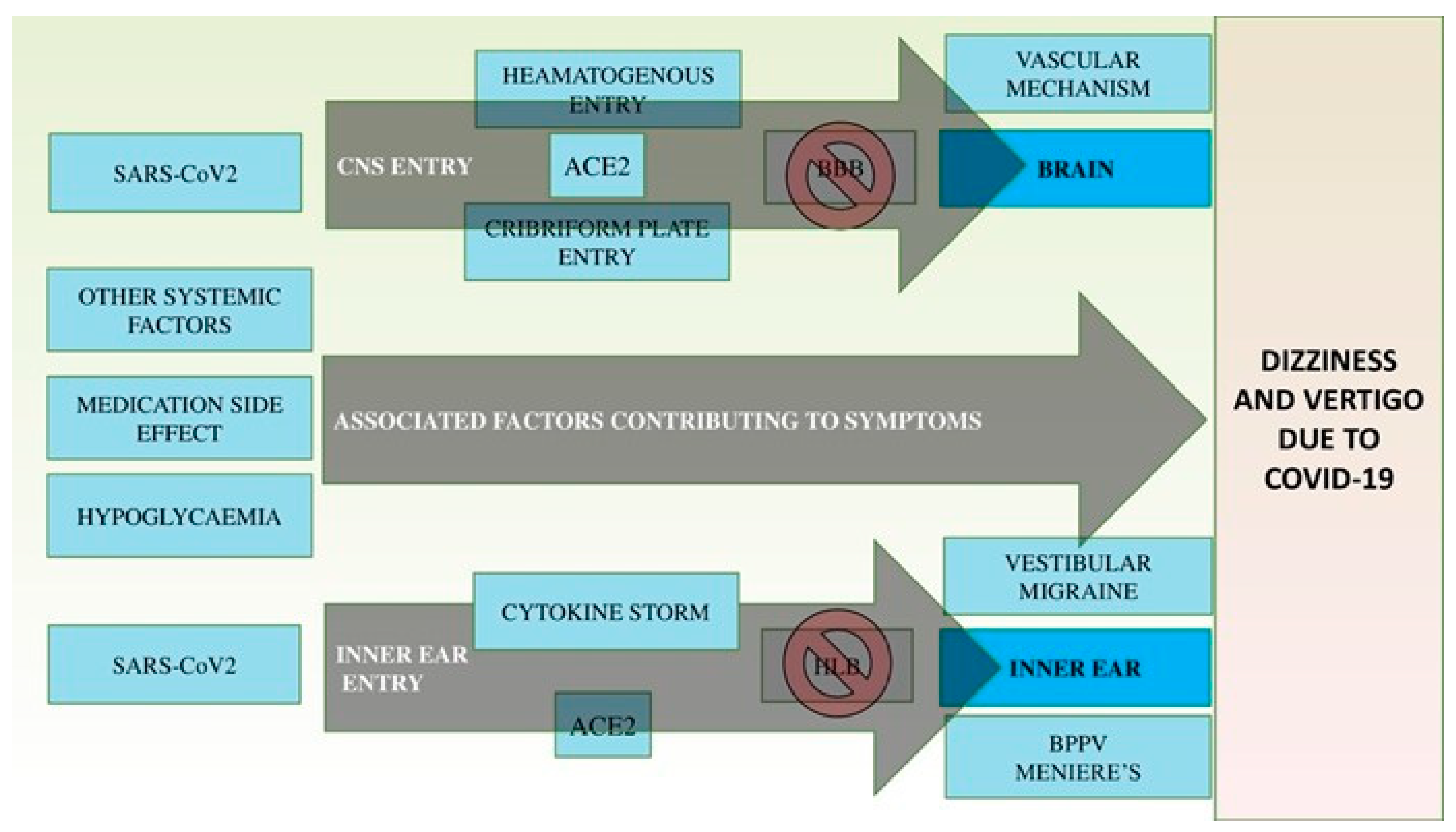
1.1. The Neurotropism of COVID-19 Disease
1.2. Vertigo and Dizziness as Part of COVID-19 Manifestations
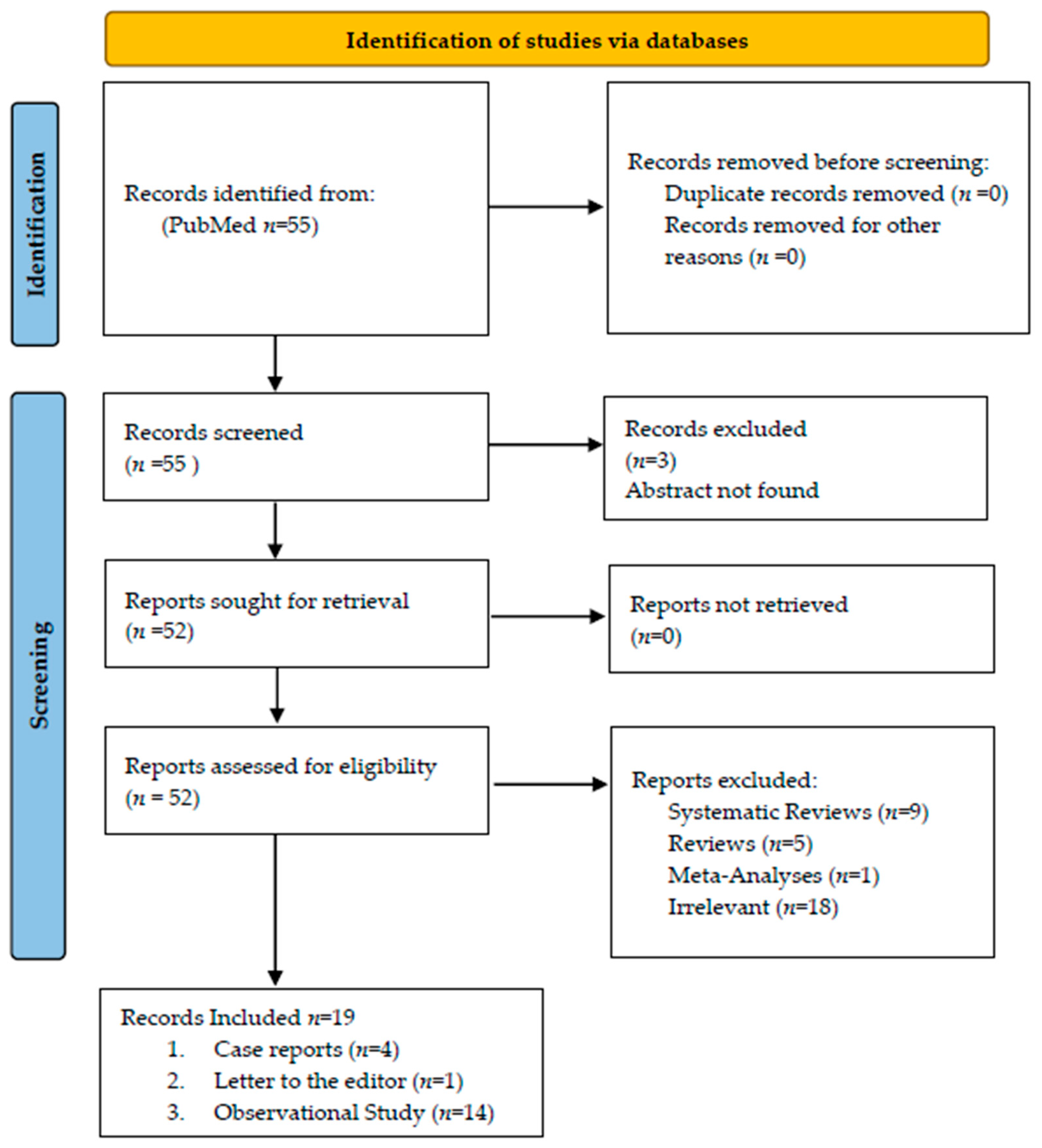
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACE-2 | Angiotensin-converting enzyme 2 |
| BBB | Blood–Brain Barrier |
| BPPV | Benign Paroxysmal Positional Vertigo |
| CNS | Central Nervous System |
| COVID-19 | 2019 novel coronavirus |
| CR | Case Report |
| CS | Case Series |
| CSF | Cerebral Spinal Fluid |
| cVEMP | Cervical Vestibular Evoked Myogenic Potential |
| ICU | Intensive Care Unit |
| LtE | Letter to the Editor |
| MERS-Cov | Middle East respiratory syndrome–related coronavirus |
| OS | Observational study |
| PTA | Pure Tone Audiometry |
| PCR | Polymerase Chain Reaction |
| SARS-CoV | Severe acute respiratory syndrome coronavirus |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus-2 |
| TNF | Tumor Necrosis Factor |
| WHO | World Health Organization |
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. Atenei Parm. 2020, 91, 157–160. [Google Scholar]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report-36. Updated 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 25 February 2020).
- Yin, R.; Feng, W.; Wang, T.; Chen, G.; Wu, T.; Chen, D.; Lv, T.; Xiang, D. Concomitant neurological symptoms observed in a patient diagnosed with coronavirus disease 2019. J. Med. Virol. 2020, 92, 1782–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Tawfiq, J.A.; Zumla, A.; Memish, Z.A. Coronaviruses: Severe acute respiratory syndrome coronavirus and Middle East respiratory syndrome coronavirus in travelers. Curr. Opin. Infect. Dis. 2014, 27, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Filatov, A.; Sharma, P.; Hindi, F.; Espinosa, P.S. Neurological complications of coronavirus disease (COVID-19) Encephalopathy. Cureus 2020, 12, e7352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARSCoV2 may be at least partially responsible for the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, M.; Okano, H.; Ogawa, K. Inflammatory and immune responses in the cochlea: Potential therapeutic targets for sensorineural hearing loss. Front. Pharmacol. 2014, 5, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host-Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Schett, G.; Sticherling, M.; Neurath, M.F. COVID-19: Risk for cytokine targeting in chronic inflammatory diseases? Nat. Rev. Immunol. 2020, 20, 271–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Hoiland, R.L.; Stukas, S.; Wellington, C.L.; Sekhon, M.S. Confronting the controversy: Interleukin-6 and the COVID-19 cytokine storm syndrome. Eur. Respir. J. 2020, 56, 2003006. [Google Scholar] [CrossRef]
- de Sousa, A.K.; Magalhães, D.A.; Ferreira, J.; Barbosa, A. SARS-CoV-2-mediated encephalitis: Role of AT2R receptors in the blood-brain barrier. Med. Hypotheses 2020, 144, 110213. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Kulasegarah, J. Dizziness and COVID-19. Ear Nose Throat J. 2021, 100, 29–30. [Google Scholar] [CrossRef] [PubMed]
- Bisdorff, A.; Von Brevern, M.; Lempert, T.; Newman-Toker, D.E. Classification of vestibular symptoms: Towards an international classification of vestibular disorders. J. Vestib. Res. 2009, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, M.B.; Basu, S.; Sherwin, E.; Cohen, J.S. Triple threat: New presentation with diabetic ketoacidosis, COVID-19, and cardiac arrhythmias. Am J Emerg Med. 2021, 49, 437.e5–437.e8. [Google Scholar] [CrossRef]
- Whittaker, A.; Anson, M.; Harky, A. Neurological Manifestations of COVID-19: A systematic review and current update. Acta Neurol. Scand. 2020, 142, 14–22. [Google Scholar] [CrossRef]
- Cha, Y.H. Migraine-associated vertigo: Diagnosis and treatment. Semin. Neurol. 2010, 30, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Frejo, L.; Gallego-Martinez, A.; Requena, T.; Martin-Sanz, E.; Amor-Dorado, J.C.; Soto-Varela, A.; Santos-Perez, S.; Espinosa-Sanchez, J.M.; Batuecas-Caletrio, A.; Aran, I.; et al. Proinflammatory cytokines and response to molds in mononuclear cells of patients with Meniere disease. Sci. Rep. 2018, 8, 5974. [Google Scholar] [CrossRef]
- Qian, S.X.; Gu, J.X.; Guan, Q.B.; Zhang, X.L.; Wang, Y.P. Serum oxidative stress, inflammatory response and platelet activation in patients with vascular vertigo. J. Biol. Regul. Homeost. Agents 2019, 33, 499–504. [Google Scholar] [PubMed]
- Tsai, K.L.; Wang, C.T.; Kuo, C.H.; Cheng, Y.Y.; Ma, H.I.; Hung, C.H.; Tsai, Y.J.; Kao, C.L. The potential role of epigenetic modulations in BPPV maneuver exercises. Oncotarget 2016, 7, 35522–35534. [Google Scholar] [CrossRef] [Green Version]
- Trigo, J.; García-Azorín, D.; Sierra-Mencía, Á.; Tamayo-Velasco, A.; Martínez-Paz, P.; Tamayo, E.; Luis Guerrero, A.; Gonzalo-Benito, H. Cytokine and interleukin profile in patients with headache and COVID-19: A pilot, CASE-control, study on 104 patients. J. Headache Pain 2021, 22, 51. [Google Scholar] [CrossRef]
- Spiezia, L.; Boscolo, A.; Correale, C.; Sella, N.; Pesenti, E.; Beghetto, L.; Campello, E.; Poletto, F.; Cerruti, L.; Cola, M.; et al. Different Hypercoagulable Profiles in Patients with COVID-19 Admitted to the Internal Medicine Ward and the Intensive Care Unit. Thromb. Haemost. 2020, 120, 1474–1477. [Google Scholar] [CrossRef]
- Ciorba, A.; Corazzi, V.; Skarżyński, P.H.; Skarżyńska, M.B.; Bianchini, C.; Pelucchi, S.; Hatzopoulos, S. Don’t forget ototoxicity during the SARS-CoV-2 (COVID-19) pandemic! Int. J. Immunopathol. Pharmacol. 2020, 34, 2058738420941754. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Aldè, M.; Barozzi, S.; Di Berardino, F.; Zuccotti, G.; Consonni, D.; Ambrosetti, U.; Socci, M.; Bertoli, S.; Battezzati, A.; Foppiani, A.; et al. Prevalence of symptoms in 1512 COVID-19 patients: Have dizziness and vertigo been underestimated thus far? Intern. Emerg. Med. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Gallus, R.; Melis, A.; Rizzo, D.; Piras, A.; De Luca, L.M.; Tramaloni, P.; Serra, A.; Longoni, E.; Soro, G.M.; Bussu, F. Audiovestibular symptoms and sequelae in COVID-19 patients. J. Vestib. Res. 2021, 31, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zheng, Z.; Zhang, C.; Zhang, X.; Wu, H.; Wang, J.; Wang, S.; Zheng, C. Clinical characteristics of 145 patients with corona virus disease 2019 (COVID-19) in Taizhou, Zhejiang, China. Infection 2020, 48, 543–551. [Google Scholar] [CrossRef]
- Cui, C.; Yao, Q.; Zhang, D.; Zhao, Y.; Zhang, K.; Nisenbaum, E.; Cao, P.; Zhao, K.; Huang, X.; Leng, D.; et al. Approaching Otolaryngology Patients During the COVID-19 Pandemic. Otolaryngol. Head Neck Surg. 2020, 163, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Han, W.; Quan, B.; Guo, Y.; Zhang, J.; Lu, Y.; Feng, G.; Wu, Q.; Fang, F.; Cheng, L.; Jiao, N.; et al. The course of clinical diagnosis and treatment of a case infected with coronavirus disease 2019. J. Med. Virol. 2020, 92, 461–463. [Google Scholar] [CrossRef]
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Karadaş, Ö.; Öztürk, B.; Sonkaya, A.R. A prospective clinical study of detailed neurological manifestations in patients with COVID-19. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 1991–1995. [Google Scholar] [CrossRef]
- Karimi-Galougahi, M.; Naeini, A.S.; Raad, N.; Mikaniki, N.; Ghorbani, J. Vertigo and hearing loss during the COVID-19 pandemic—Is there an association? Acta Otorhinolaryngol. Ital. 2020, 40, 463–465. [Google Scholar] [CrossRef]
- Kong, Z.; Wang, J.; Li, T.; Zhang, Z.; Jian, J. 2019 novel coronavirus pneumonia with onset of dizziness: A case report. Ann. Transl. Med. 2020, 8, 506. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Place, S.; Van Laethem, Y.; Cabaraux, P.; Mat, Q.; Huet, K.; Plzak, J.; Horoi, M.; Hans, S.; et al. Clinical and epidemiological characteristics of 1420 European patients with mild-to-moderate coronavirus disease 2019. J. Intern. Med. 2020, 288, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Lo, I.L.; Lio, C.F.; Cheong, H.H.; Lei, C.I.; Cheong, T.H.; Zhong, X.; Tian, Y.; Sin, N.N. Evaluation of SARS-CoV-2 RNA shedding in clinical specimens and clinical characteristics of 10 patients with COVID-19 in Macau. Int. J. Biol. Sci. 2020, 16, 1698–1707. [Google Scholar] [CrossRef] [Green Version]
- Malayala, S.V.; Raza, A. A Case of COVID-19-Induced Vestibular Neuritis. Cureus 2020, 12, e8918. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Mi, B.; Chen, L.; Xiong, Y.; Xue, H.; Zhou, W.; Liu, G. Characteristics and Early Prognosis of COVID-19 Infection in Fracture Patients. J. Bone Joint Surg. Am. 2020, 102, 750–758. [Google Scholar] [CrossRef]
- Sia, J. Dizziness can be an early sole clinical manifestation for COVID-19 infection: A case report. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1354–1356. [Google Scholar] [CrossRef]
- Vacchiano, V.; Riguzzi, P.; Volpi, L.; Tappatà, M.; Avoni, P.; Rizzo, G.; Guerra, L.; Zaccaroni, S.; Cortelli, P.; Michelucci, R.; et al. Early neurological manifestations of hospitalized COVID-19 patients. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 2029–2203. [Google Scholar] [CrossRef]
- Viola, P.; Ralli, M.; Pisani, D.; Malanga, D.; Sculco, D.; Messina, L.; Laria, C.; Aragona, T.; Leopardi, G.; Ursini, F.; et al. Tinnitus and equilibrium disorders in COVID-19 patients: Preliminary results. Eur. Arch. Otorhinolaryngol. 2021, 278, 3725–3730. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases with Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Maslovara, S.; Košec, A. Post-COVID-19 Benign Paroxysmal Positional Vertigo. Case Rep. Med. 2021, 2021, 9967555. [Google Scholar] [CrossRef]
- Ousseiran, Z.H.; Fares, Y.; Chamoun, W.T. Neurological manifestations of COVID-19: A systematic review and detailed comprehension. Int. J. Neurosci. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Abdullahi, A.; Candan, S.; Abba, M.; Bello, A.H.; AlShehri, M.A.; Victor, E.A.; Umar, N.A.; Kundakci, B. Neurological and musculoskeletal features of COVID-19: A systematic review and meta-analysis. Front. Neurol. 2020, 11, 687. [Google Scholar] [CrossRef] [PubMed]
- Abenza-Abildúa, M.J.; Ramírez-Prieto, M.T.; Moreno-Zabaleta, R.; Arenas-Valls, N.; Salvador-Maya, M.; Algarra-Lucas, C.; Moreno-Arrones, B.R.; Sánchez-Cordón, B.; de Luna, J.O.-R.; Jimeno-Montero, C.; et al. Neurological complications in critical patients with COVID-19. Neurología 2020, 35, 621–627. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Study Type | Sample Size | Dizziness | Vertigo | Other |
|---|---|---|---|---|---|
| Alde et al., 2021 [24] | OS | 1512 | - |
12% (30/251) |
Lightheadedness 43.8% (110/251) Disequilibrium 27.9% (70/251) Presyncope 16.3% (41/251) |
| Gallus et al., 2021 [25] | OS | 48 |
3%
(4/48) |
2%
(1/48) Spinning Vertigo |
Tinnitus 4,2% (2/48)
Dynamic imbalance 2% (1/48) Static imbalance 6% (3/48) |
| Chen et al., 2020 [26] | OS | 145 | 20% (29/145) | - | - |
| Cui et al., 2020 [27] | OS | 20 | 20%(5/20) | - | - |
| Han et al., 2020 [28] | CR | 1 | - | √ | - |
| Hu et al., 2020 [29] | OS | 24 | 0.03% (1/28) | - | - |
| Karadas et al., 2020 [30] | OS | 239 |
6.7% (16/239) | - |
Tinnitus 2.1% (5/239) Neurological findings 34% (83/239) |
| Karimi-Galougahi et al., 2020 [31] | LtE | 6 | - | 33% (1/3) | Tinnitus (3/3) Unilateral hearing loss (3/3) |
| Kong et al. 2020 [32] | CR | 1 Electronystagmography, Pure Tone Audiometry, Brain MRI performed. Symptomatic Treatment given | √ | - | - |
| Lechien et al., 2020 [33] | OS | 1420 | - |
0.004%
(6/1420) Rotatory Vertigo | Tinnitus 0.003% (5/1420) |
| Lo et al., 2020 [34] | OS | 10 | 20% (2/10) | - | - |
| Malayala et al., 2020 [35] | CR | 1 patient Suspected COVID-19-induced acute vestibular neuritis. CT brain performed Symptomatic Treatment given Vestibular Rehabilitation performed | - | √ | - |
| Mao et al., 2020 [36] | OS | 214 |
16.8% (36/214) | - | - |
| Mi et al., 2020 [37] | OS | 10 | 3% (3/10) | - | - |
| Sia et al., 2020 [38] | CR | 1 | Sudden onset | - | - |
| Vacchiano et al., 2020 [39] | OS | 133 | 10%(11/133) | - | - |
| Viola et al., 2020 [40] | OS | 185 | 94.1% (32/34) | 5.9% (2/34) acute vertigo attacks | Equilibrium disorders 18.4% (34/185) Tinnitus 23.2% (43/185) Combination 7.65% 14/185 (tinnitus and equilibrium disorder) |
| Wang et al., 2020 [41] | OS | 69 | 5/69 (7%) | - | - |
| Wang et al., 2020 [42] | OS | 138 | 13/138 (9.4%) | - | - |
| Maslovara et al., 2021 [43] | CR | 2 | - | BPPV | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korres, G.; Kitsos, D.K.; Kaski, D.; Tsogka, A.; Giannopoulos, S.; Giannopapas, V.; Sideris, G.; Tyrellis, G.; Voumvourakis, K. The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review. Brain Sci. 2022, 12, 948. https://doi.org/10.3390/brainsci12070948
Korres G, Kitsos DK, Kaski D, Tsogka A, Giannopoulos S, Giannopapas V, Sideris G, Tyrellis G, Voumvourakis K. The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review. Brain Sciences. 2022; 12(7):948. https://doi.org/10.3390/brainsci12070948
Chicago/Turabian StyleKorres, George, Dimitrios K. Kitsos, Diego Kaski, Anthi Tsogka, Sotirios Giannopoulos, Vasileios Giannopapas, Giorgos Sideris, Giorgos Tyrellis, and Konstantine Voumvourakis. 2022. "The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review" Brain Sciences 12, no. 7: 948. https://doi.org/10.3390/brainsci12070948
APA StyleKorres, G., Kitsos, D. K., Kaski, D., Tsogka, A., Giannopoulos, S., Giannopapas, V., Sideris, G., Tyrellis, G., & Voumvourakis, K. (2022). The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review. Brain Sciences, 12(7), 948. https://doi.org/10.3390/brainsci12070948