
Optimal Intervention Timing for Robotic-Assisted Gait Training in Hemiplegic Stroke


_H._You.png)
Abstract
:1. Introduction
2. Materials and Methods
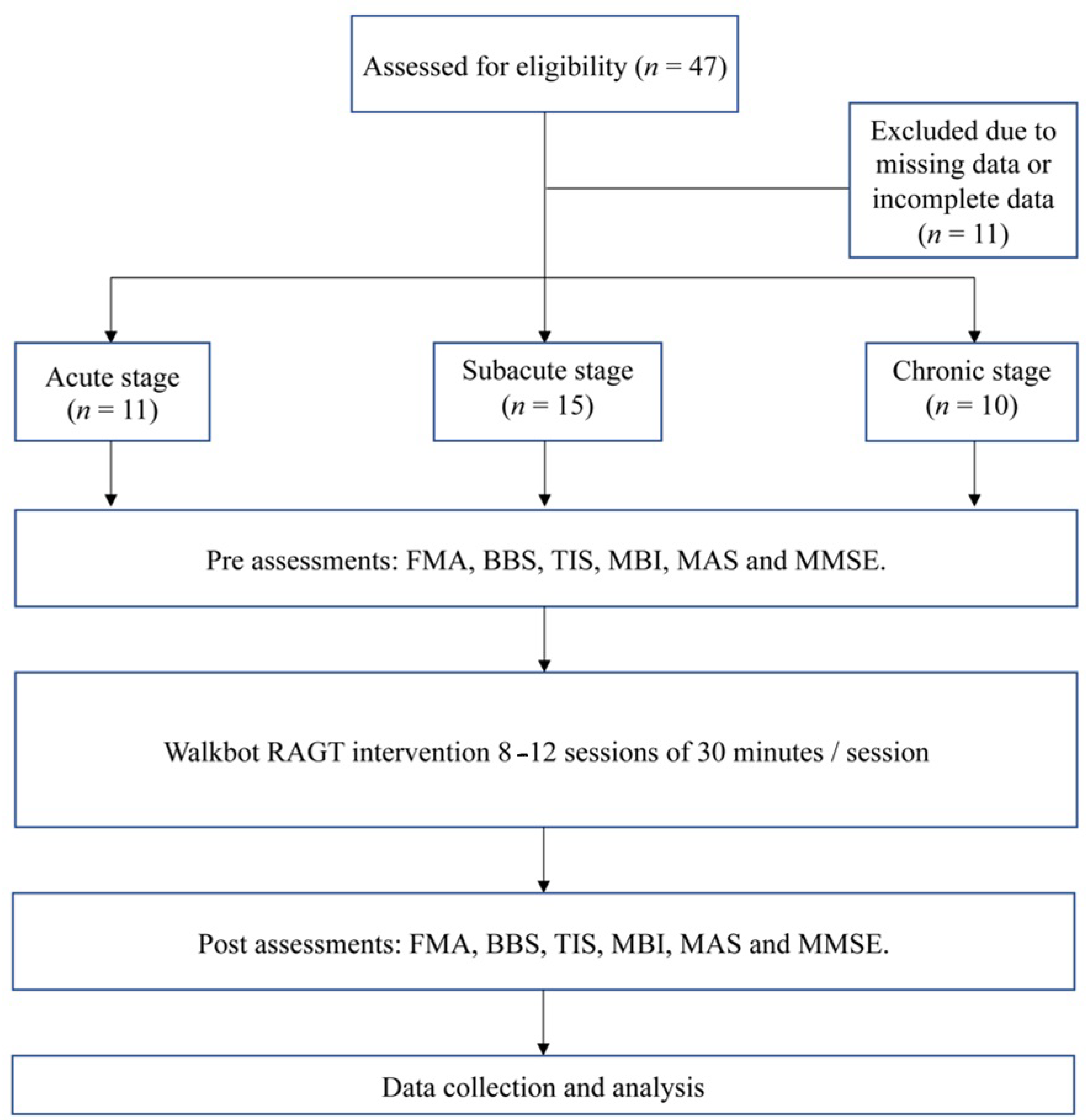
2.1. Participants
2.2. Study Design
2.2.1. Sensorimotor Function Assessment
2.2.2. Balance Measurement
2.2.3. Trunk Coordination
2.2.4. ADLs
2.2.5. Muscle Tone Assessment
2.2.6. Cognitive Function Assessment
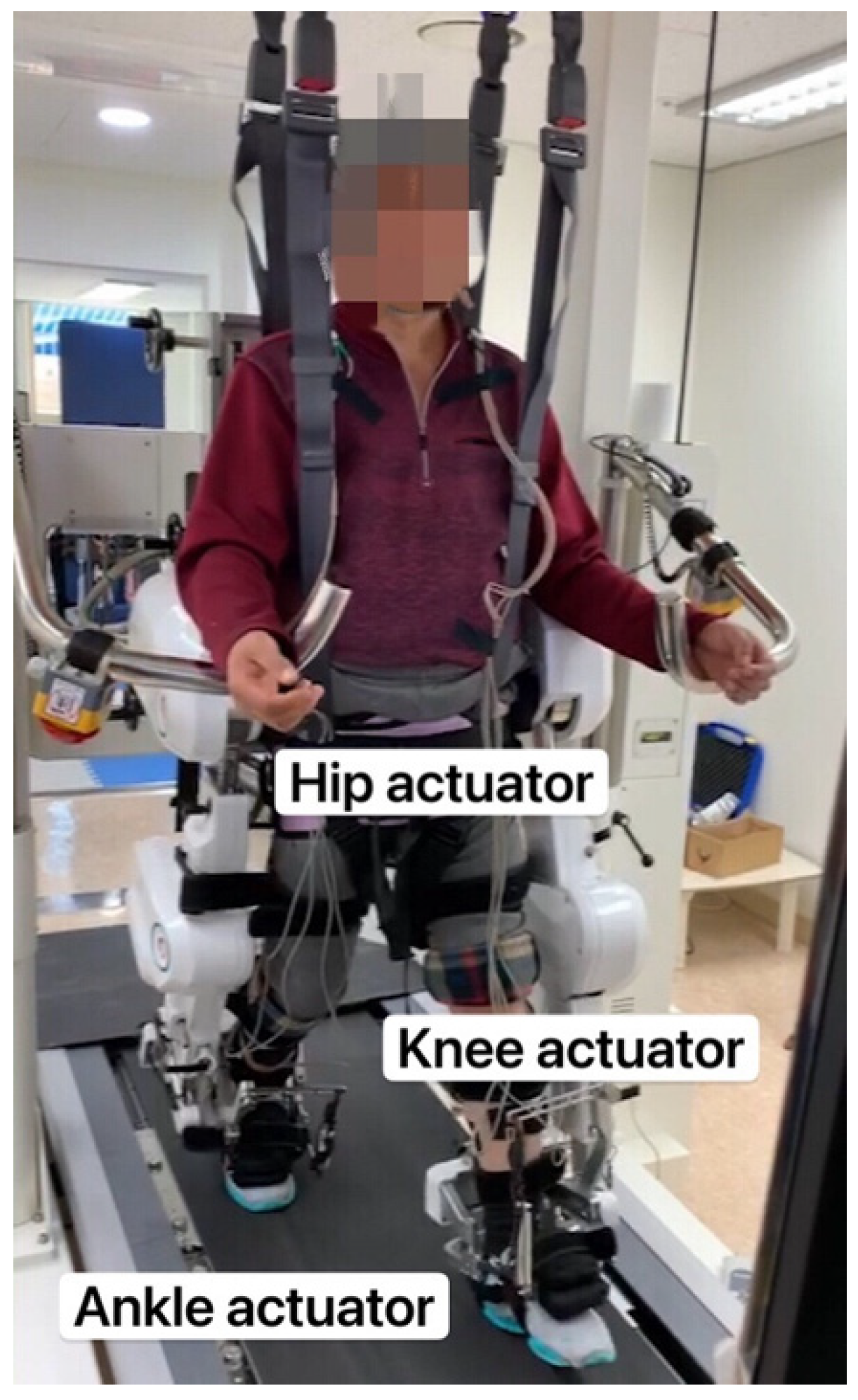
2.3. Intervention
2.4. Statistical Analyses
3. Results
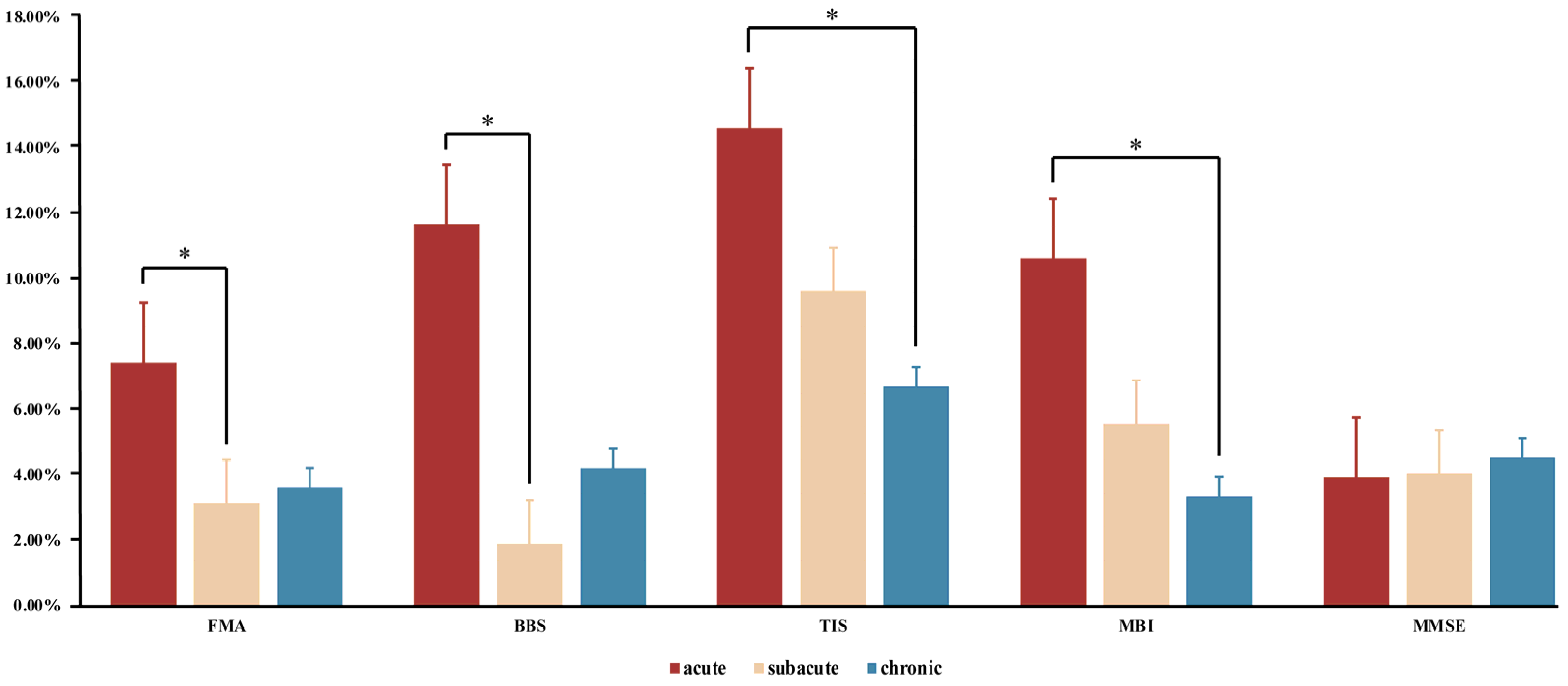
3.1. Sensorimotor Function
3.2. Balance Measurement
3.3. Trunk Coordination
3.4. ADLs
3.5. Muscle Tone Assessment
3.6. Cognitive Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, W.H.; Kim, M.S.; Huh, J.P.; Lee, P.K.; Kim, Y.-H. Effects of robot-assisted gait training on cardiopulmonary fitness in subacute stroke patients: A randomized controlled study. Neurorehabil. Neural Repair 2012, 26, 318–324. [Google Scholar] [CrossRef]
- Park, C.; Oh-Park, M.; Dohle, C.; Bialek, A.; Friel, K.; Edwards, D.; Krebs, H.I.; You, J.S.H. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation 2020, 46, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Yokota, C.; Yamamoto, Y.; Kamada, M.; Nakai, M.; Nishimura, K.; Ando, D.; Sato, T.; Koga, M.; Ihara, M.; Toyoda, K. Acute stroke rehabilitation for gait training with cyborg type robot Hybrid Assistive Limb: A pilot study. J. Neurol. Sci. 2019, 404, 11–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.-E.; Yoo, J.S.; Kim, K.E.; Cho, S.T.; Jang, W.S.; Cho, K.H.; Lee, W.-H. Systematic review of appropriate robotic intervention for gait function in subacute stroke patients. BioMed Res. Int. 2018, 2018, 4085298. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, H.J.; Hwang, S.W.; Pyo, H.; Yang, S.P.; Lim, M.-H.; Park, G.L.; Kim, E.J. Clinical characteristics of proper robot-assisted gait training group in non-ambulatory subacute stroke patients. Ann. Rehabil. Med. 2016, 40, 183–189. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.; Sajin, A.; Fisher, I.; Neeb, M.; Shochina, M.; Katz-Leurer, M.; Meiner, Z. The effectiveness of locomotor therapy using robotic-assisted gait training in subacute stroke patients: A randomized controlled trial. PM&R 2009, 1, 516–523. [Google Scholar] [CrossRef]
- Bang, D.-H.; Shin, W.-S. Effects of robot-assisted gait training on spatiotemporal gait parameters and balance in patients with chronic stroke: A randomized controlled pilot trial. NeuroRehabilitation 2016, 38, 343–349. [Google Scholar] [CrossRef]
- Cho, D.Y.; Park, S.-W.; Lee, M.J.; Park, D.S.; Kim, E.J. Effects of robot-assisted gait training on the balance and gait of chronic stroke patients: Focus on dependent ambulators. J. Phys. Ther. Sci. 2015, 27, 3053–3057. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, G.; Shin, J.-H.; You, J.H. Neuroplastic effects of end-effector robotic gait training for hemiparetic stroke: A randomised controlled trial. Sci. Rep. 2020, 10, 12461. [Google Scholar] [CrossRef]
- Kim, H.Y.; You, J.S.H. A review of robot-assisted gait training in stroke patients. Brain Neurorehabil. 2017, 10, e9. [Google Scholar] [CrossRef] [Green Version]
- Taveggia, G.; Borboni, A.; Mulé, C.; Villafañe, J.H.; Negrini, S. Conflicting results of robot-assisted versus usual gait training during postacute rehabilitation of stroke patients: A randomized clinical trial. Int. J. Rehabil. Res. Int. Z. Rehabil. Rev. Int. Rech. Readapt. 2016, 39, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Nunen, M.P.; Gerrits, K.H.; Konijnenbelt, M.; Janssen, T.W.; de Haan, A. Recovery of walking ability using a robotic device in subacute stroke patients: A randomized controlled study. Disabil. Rehabil. Assist. Technol. 2015, 10, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, CD006185. [Google Scholar] [CrossRef] [PubMed]
- Biernaskie, J.; Chernenko, G.; Corbett, D. Efficacy of rehabilitative experience declines with time after focal ischemic brain injury. J. Neurosci. 2004, 24, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurol. Res. Pract. 2020, 2, 17. [Google Scholar] [CrossRef]
- See, J.; Dodakian, L.; Chou, C.; Chan, V.; McKenzie, A.; Reinkensmeyer, D.J.; Cramer, S.C. A standardized approach to the Fugl-Meyer assessment and its implications for clinical trials. Neurorehabil. Neural Repair 2013, 27, 732–741. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale has high intra-and inter-rater reliability but absolute reliability varies across the scale: A systematic review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Leung, S.O.; Chan, C.C.; Shah, S. Development of a Chinese version of the Modified Barthel Index—validity and reliability. Clin. Rehabil. 2007, 21, 912–922. [Google Scholar] [CrossRef]
- Verheyden, G.; Kersten, P. Investigating the internal validity of the Trunk Impairment Scale (TIS) using Rasch analysis: The TIS 2.0. Disabil. Rehabil. 2010, 32, 2127–2137. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, C.P. Interrater reliability of a modified Ashworth scale of muscle spasticity. In Classic Papers in Orthopaedics; Springer: Berlin/Heidelberg, Germany, 2014; pp. 415–417. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; i Figuls, M.R.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Cosp, X.B.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015, 2015, CD010783. [Google Scholar] [CrossRef]
- Amanzonwe, R.; Kossi, R.; Tedesco Triccas, L.; Codjo, L.; Feys, P.; Hansen, D.; BIOMED-REVAL-Rehabilitation Research Centre, Hasselt University, Belgium. The type and dosage of exercise therapy to facilitate the recovery from stroke for balance, walking and quality of life: A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J. 2021, 42, ehab724.2064. [Google Scholar] [CrossRef]
- Hwang, J.; Shin, Y.; Park, J.-H.; Cha, Y.J.; You, J.S.H. Effects of Walkbot gait training on kinematics, kinetics, and clinical gait function in paraplegia and quadriplegia. NeuroRehabilitation 2018, 42, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Manganotti, P.; Patuzzo, S.; Cortese, F.; Palermo, A.; Smania, N.; Fiaschi, A. Motor disinhibition in affected and unaffected hemisphere in the early period of recovery after stroke. Clin. Neurophysiol. 2002, 113, 936–943. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Yang, L.; Park, I.J.; Kim, E.J.; Park, M.S.; You, S.H.; Kim, Y.-H.; Ko, H.-Y.; Shin, Y.-I. Effects of innovative WALKBOT robotic-assisted locomotor training on balance and gait recovery in hemiparetic stroke: A prospective, randomized, experimenter blinded case control study with a four-week follow-up. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Shin, Y.-I.; You, J.S.H.; Park, M.S. Comparative effects of robotic-assisted gait training combined with conventional physical therapy on paretic hip joint stiffness and kinematics between subacute and chronic hemiparetic stroke. NeuroRehabilitation 2018, 42, 181–190. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Oh, W.; Park, C.; Oh, S.; You, S.J.H. Stage 2: Who Are the Best Candidates for Robotic Gait Training Rehabilitation in Hemiparetic Stroke? J. Clin. Med. 2021, 10, 5715. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Oh-Park, M.; Bialek, A.; Friel, K.; Edwards, D.; You, J.S.H. Abnormal synergistic gait mitigation in acute stroke using an innovative ankle–knee–hip interlimb humanoid robot: A preliminary randomized controlled trial. Sci. Rep. 2021, 11, 22823. [Google Scholar] [CrossRef]
- Shin, J.; Yang, S.; Park, C.; Lee, Y.; You, S.J.H. Comparative effects of passive and active mode robot-assisted gait training on brain and muscular activities in sub-acute and chronic stroke. NeuroRehabilitation, 2022; 1–13, pre-press. [Google Scholar] [CrossRef]
- Boyd, L.A.; Winstein, C.J. Explicit information interferes with implicit motor learning of both continuous and discrete movement tasks after stroke. J. Neurol. Phys. Ther. 2006, 30, 46–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, M.S.; Thoroughman, K.A. Motor adaptation to single force pulses: Sensitive to direction but insensitive to within-movement pulse placement and magnitude. J. Neurophysiol. 2006, 96, 710–720. [Google Scholar] [CrossRef] [Green Version]
- Mackay, C.P.; Brauer, S.G.; Schaumberg, M.A.; Kuys, S.S.; Leow, L.-A. The acute effects of aerobic exercise on sensorimotor adaptation in chronic stroke. Restor. Neurol. Neurosci. 2021, 39, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Cunha, C.; Brambilla, R.; Thomas, K.L. A simple role for BDNF in learning and memory? Front. Mol. Neurosci. 2010, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, D.; Drummond, J.; Handberg, E.; Ewell, S.; Pozzo-Miller, L. Multiple approaches to investigate the transport and activity-dependent release of BDNF and their application in neurogenetic disorders. Neural Plast. 2012, 2012, 203734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leßmann, V.; Brigadski, T. Mechanisms, locations, and kinetics of synaptic BDNF secretion: An update. Neurosci. Res. 2009, 65, 11–22. [Google Scholar] [CrossRef]
- Chung, B.P.H. Effectiveness of robotic-assisted gait training in stroke rehabilitation: A retrospective matched control study. Hong Kong Physiother. J. 2017, 36, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Liepert, J.; Bauder, H.; Miltner, W.H.; Taub, E.; Weiller, C. Treatment-induced cortical reorganization after stroke in humans. Stroke 2000, 31, 1210–1216. [Google Scholar] [CrossRef] [Green Version]
- Yoon, B.H.; Park, C.; You, J.H. Minimal Contact Robotic Stroke Rehabilitation on Risk of COVID-19, Work Efficiency and Sensorimotor Function. Healthcare 2022, 10, 691. [Google Scholar] [CrossRef]
- Kim, H.Y.; Shin, J.-H.; Yang, S.P.; Shin, M.A.; Lee, S.H. Robot-assisted gait training for balance and lower extremity function in patients with infratentorial stroke: A single-blinded randomized controlled trial. J. Neuroeng. Rehabil. 2019, 16, 99. [Google Scholar] [CrossRef]
- Srivastava, S.; Kao, P.-C.; Kim, S.H.; Stegall, P.; Zanotto, D.; Higginson, J.S.; Agrawal, S.K.; Scholz, J.P. Assist-as-needed robot-aided gait training improves walking function in individuals following stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 23, 956–963. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Reitano, S.; Leo, A.; De Luca, R.; Melegari, C.; Bramanti, P. Can robot-assisted movement training (Lokomat) improve functional recovery and psychological well-being in chronic stroke? Promising findings from a case study. Funct. Neurol. 2014, 29, 139. [Google Scholar]
- Dundar, U.; Toktas, H.; Solak, O.; Ulasli, A.; Eroglu, S. A comparative study of conventional physiotherapy versus robotic training combined with physiotherapy in patients with stroke. Top. Stroke Rehabil. 2014, 21, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdette, J.H.; Laurienti, P.J.; Espeland, M.A.; Morgan, A.R.; Telesford, Q.; Vechlekar, C.D.; Hayaska, S.; Jennings, J.J.; Katula, J.A.; Kraft, R.A. Using network science to evaluate exercise-associated brain changes in older adults. Front. Aging Neurosci. 2010, 2, 23. [Google Scholar] [CrossRef] [Green Version]
- Pallesen, H.; Bjerk, M.; Pedersen, A.R.; Nielsen, J.F.; Evald, L. The effects of high-intensity aerobic exercise on cognitive performance after stroke: A pilot randomised controlled trial. J. Cent. Nerv. Syst. Dis. 2019, 11, 1179573519843493. [Google Scholar] [CrossRef] [Green Version]
- Wahl, A.-S.; Schwab, M.E. Finding an optimal rehabilitation paradigm after stroke: Enhancing fiber growth and training of the brain at the right moment. Front. Hum. Neurosci. 2014, 8, 381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, I.J.; Park, J.-H.; Seong, H.Y.; You, J.S.H.; Kim, S.J.; Min, J.H.; Ko, H.Y.; Shin, Y.-I. Comparative effects of different assistance force during robot-assisted gait training on locomotor functions in patients with subacute stroke: An assessor-blind, randomized controlled trial. Am. J. Phys. Med. Rehabil. 2019, 98, 58–64. [Google Scholar] [CrossRef]
- Chollet, F.; Tardy, J.; Albucher, J.-F.; Thalamas, C.; Berard, E.; Lamy, C.; Bejot, Y.; Deltour, S.; Jaillard, A.; Niclot, P. Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): A randomised placebo-controlled trial. Lancet Neurol. 2011, 10, 123–130. [Google Scholar] [CrossRef]
- Cassidy, J.M.; Cramer, S.C. Spontaneous and therapeutic-induced mechanisms of functional recovery after stroke. Transl. Stroke Res. 2017, 8, 33–46. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Acute Stage Group (n = 11) | Subacute Stage Group (n = 15) | Chronic Stage Group (n = 10) | p-Value * |
|---|---|---|---|---|
| Age (years) a | 63.18 ± 12.61 | 68.33 ± 11.29 | 68.43 ± 9.43 | 0.55 |
| Sex (male/female) | 5/5 | 10/4 | 3/7 | 0.45 |
| Height (cm) a | 164.18 ± 10.63 | 162.13 ± 7.46 | 168.00 ± 9.75 | 0.49 |
| Weight (kg) a | 65.14 ± 8.63 | 61.29 ± 7.70 | 65.50 ± 13.61 | 0.21 |
| Hemiparetic side (left/right) | 3/7 | 8/7 | 7/3 | 0.52 |
| FAC a | 2.82 ± 0.57 | 3.07 ± 0.57 | 3.10 ± 0.54 | 0.38 |
| FMA a pre-baseline | 30.55 ± 20.93 | 13.13 ± 10.19 | 19.40 ± 2.01 | 0.01 * |
| Type of stroke (Ischemic/Hemorrhagic) | 7/3 | 6/9 | 4/6 | 0.71 |
| FMA | BBS | TIS | MBI | MAS | MMSE | ||
|---|---|---|---|---|---|---|---|
| Acute stage group | Pre-test | 30.55 ± 20.93 | 7.45 ± 5.58 | 5.27 ± 5.63 | 36.01 ± 13.34 | 0.27 ± 0.44 | 24.73 ± 4.22 |
| Post-test | 38.00 ± 21.99 | 14.00 ± 11.65 | 8.64 ± 6.08 | 47.55 ± 15.10 | 0.27 ± 0.62 | 25.91 ± 3.53 | |
| Mean change | 7.45 ± 5.58 | 6.55 ± 7.98 | 3.36 ± 1.67 | 10.64 ± 7.88 | 0.00 ± 0.43 | 1.18 ± 1.64 | |
| p-value | 0.01 † | 0.03 † | 0.01 † | 0.01 † | 1.00 | 0.04 † | |
| Subacute stage group | Pre-test | 13.13 ± 10.19 | 4.07 ± 2.41 | 3.07 ± 1.84 | 22.40 ± 10.98 | 0.73 ± 0.85 | 15.2 ± 10.02 |
| Post-test | 16.33 ± 10.34 | 5.13 ± 2.83 | 5.27 ± 2.46 | 28.00 ± 10.56 | 0.73 ± 0.85 | 16.33 ± 9.43 | |
| Mean change | 3.2 ± 1.05 | 1.07 ± 0.77 | 2.20 ± 1.56 | 5.60 ± 3.86 | 0.00 ± 0.00 | 1.13 ± 1.75 | |
| p-value | 0.01 † | 0.01 † | 0.01 † | 0.01 † | 0.01 † | 0.03 † | |
| Chronic stage group | Pre-test | 19.40 ± 2.01 | 7.30 ± 13.36 | 1.90 ± 3.59 | 26.30 ± 21.68 | 1.60 ± 1.50 | 13.90 ± 9.64 |
| Post-test | 23.00 ± 22.61 | 9.80 ± 13.87 | 3.40 ± 4.27 | 29.40 ± 22.71 | 1.40 ± 1.43 | 15.40 ± 9.24 | |
| Mean change | 3.60 ± 3.47 | 2.50 ± 3.38 | 1.50 ± 1.11 | 3.10 ± 4.83 | −0.20 ± 0.60 | 1.50 ± 2.01 | |
| p-value | 0.01 † | 0.02 † | 0.01 † | 0.09 | 0.34 | 0.05 | |
| ANOVA p-value | 0.02 ∞ | 0.03 * | 0.03 * | 0.02 * | 0.44 | 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, L.; Yoon, B.H.; Park, C.; You, J.H. Optimal Intervention Timing for Robotic-Assisted Gait Training in Hemiplegic Stroke. Brain Sci. 2022, 12, 1058. https://doi.org/10.3390/brainsci12081058
Xie L, Yoon BH, Park C, You JH. Optimal Intervention Timing for Robotic-Assisted Gait Training in Hemiplegic Stroke. Brain Sciences. 2022; 12(8):1058. https://doi.org/10.3390/brainsci12081058
Chicago/Turabian StyleXie, Lingchao, Bu Hyun Yoon, Chanhee Park, and Joshua (Sung) H. You. 2022. "Optimal Intervention Timing for Robotic-Assisted Gait Training in Hemiplegic Stroke" Brain Sciences 12, no. 8: 1058. https://doi.org/10.3390/brainsci12081058
APA StyleXie, L., Yoon, B. H., Park, C., & You, J. H. (2022). Optimal Intervention Timing for Robotic-Assisted Gait Training in Hemiplegic Stroke. Brain Sciences, 12(8), 1058. https://doi.org/10.3390/brainsci12081058