Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
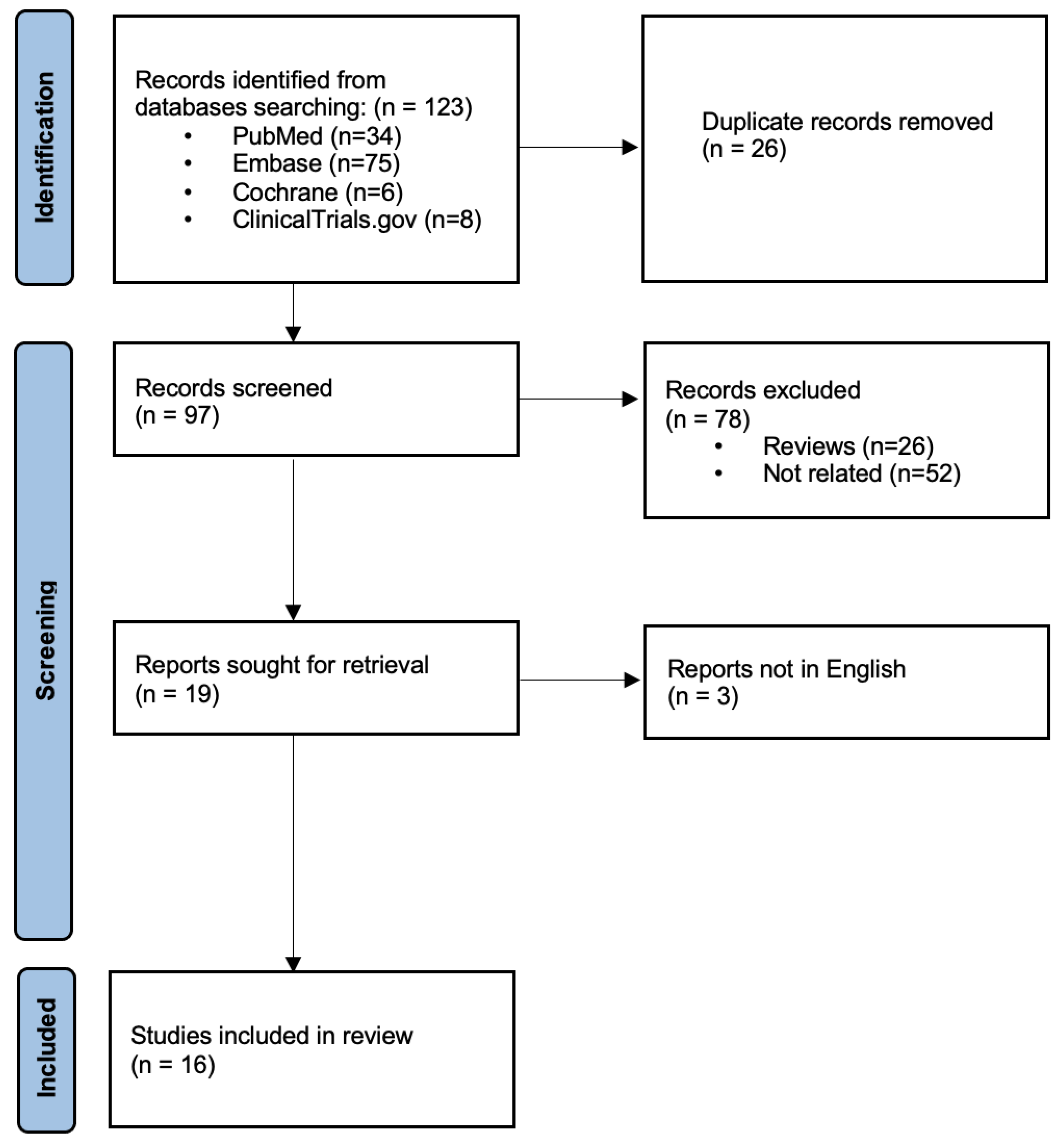
2. Materials and Methods
3. Results
3.1. Pre-Clinical Studies
3.2. Clinical Studies
3.2.1. Anti-Seizure Effects of Perampanel
3.2.2. Antitumor Effects of Perampanel
3.2.3. Tolerability and Safety of Perampanel
4. Discussion
4.1. Pre-Clinical Evidence
4.2. Clinical Evidence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Breemen, M.S.; Wilms, E.B.; Vecht, C.J. Epilepsy in Patients with Brain Tumours: Epidemiology, Mechanisms, and Management. Lancet Neurol. 2007, 6, 421–430. [Google Scholar] [CrossRef]
- Perucca, E. Optimizing Antiepileptic Drug Treatment in Tumoral Epilepsy. Epilepsia 2013, 54, 97–104. [Google Scholar] [CrossRef]
- Chen, D.Y.; Chen, C.C.; Crawford, J.R.; Wang, S.G. Tumor-Related Epilepsy: Epidemiology, Pathogenesis and Management. J. Neuro-Oncol. 2018, 139, 13–21. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of Radiotherapy with Concomitant and Adjuvant Temozolomide versus Radiotherapy Alone on Survival in Glioblastoma in a Randomised Phase III Study: 5-Year Analysis of the EORTC-NCIC Trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, H.S.; Morishita, W.; Geraghty, A.C.; Silverbush, D.; Gillespie, S.M.; Arzt, M.; Tam, L.T.; Espenel, C.; Ponnuswami, A.; Ni, L.; et al. Electrical and Synaptic Integration of Glioma into Neural Circuits. Nature 2019, 573, 539–545. [Google Scholar] [CrossRef]
- Takano, T.; Lin, J.H.C.; Arcuino, G.; Gao, Q.; Yang, J.; Nedergaard, M. Glutamate Release Promotes Growth of Malignant Gliomas. Nat. Med. 2001, 7, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, S.K.; Venneti, S. Glutamine Metabolism in Brain Tumors. Cancers 2019, 11, 1628. [Google Scholar] [CrossRef] [PubMed]
- Wirsching, H.G.; Weller, M. Does Neuronal Activity Promote Glioma Progression? Trends Cancer 2020, 6, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Ye, X.; Chamberlain, M.; Mikkelsen, T.; Batchelor, T.; Desideri, S.; Piantadosi, S.; Fisher, J.; Fine, H.A. Talampanel with Standard Radiation and Temozolomide in Patients with Newly Diagnosed Glioblastoma: A Multicenter Phase II Trial. J. Clin. Oncol. 2009, 27, 4155–4161. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, F.M.; Kreisl, T.N.; Kim, L.; Duic, J.P.; Butman, J.A.; Albert, P.S.; Fine, H.A. Phase 2 Trial of Talampanel, a Glutamate Receptor Inhibitor, for Adults with Recurrent Malignant Gliomas. Cancer 2010, 116, 1776–1782. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Trinka, E.; Lattanzi, S.; Carpenter, K.; Corradetti, T.; Nucera, B.; Rinaldi, F.; Shankar, R.; Brigo, F. Exploring the Evidence for Broad-Spectrum Effectiveness of Perampanel: A Systematic Review of Clinical Data in Generalised Seizures. CNS Drugs 2021, 35, 821–837. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, b2535. [Google Scholar] [CrossRef]
- Cunningham, M. Targeting Elevated Glutamate in Brain Tumour Related Epilepsy. Epilepsia 2016, 57 (Suppl. S2), 226. [Google Scholar] [CrossRef]
- Lange, F.; Weßlau, K.; Porath, K.; Hörnschemeyer, J.; Bergner, C.; Krause, B.J.; Mullins, C.S.; Linnebacher, M.; Köhling, R.; Kirschstein, T. AMPA Receptor Antagonist Perampanel Affects Glioblastoma Cell Growth and Glutamate Release In Vitro. PLoS ONE 2019, 14, e0211644. [Google Scholar] [CrossRef]
- Tönjes, M.; Barbus, S.; Park, Y.J.; Wang, W.; Schlotter, M.; Lindroth, A.M.; Pleier, S.V.; Bai, A.H.C.; Karra, D.; Piro, R.M.; et al. BCAT1 Promotes Cell Proliferation through Amino Acid Catabolism in Gliomas Carrying Wild-Type IDH1. Nat. Med. 2013, 19, 901. [Google Scholar] [CrossRef] [PubMed]
- GLUL. Glutamate-Ammonia Ligase [Homo Sapiens (Human)]. Available online: https://www.ncbi.nlm.nih.gov/gene/2752 (accessed on 16 December 2022).
- Lai, M.C.; Tzeng, R.C.; Huang, C.W.; Wu, S.N. The Novel Direct Modulatory Effects of Perampanel, an Antagonist of AMPA Receptors, on Voltage-Gated Sodium and M-Type Potassium Currents. Biomolecules 2019, 9, 638. [Google Scholar] [CrossRef]
- Salmaggi, A.; Corno, C.; Maschio, M.; Donzelli, S.; D’urso, A.; Perego, P.; Ciusani, E. Synergistic Effect of Perampanel and Temozolomide in Human Glioma Cell Lines. J. Pers. Med. 2021, 11, 390. [Google Scholar] [CrossRef]
- Tatsuoka, J.; Sano, E.; Hanashima, Y.; Yagi, C.; Yamamuro, S.; Sumi, K.; Hara, H.; Takada, K.; Kanemaru, K.; Komine-Aizawa, S.; et al. Anti-tumor Effects of Perampanel in Malignant Glioma Cells. Oncol. Lett. 2022, 24, 421. [Google Scholar] [CrossRef]
- Yagi, C.; Tatsuoka, J.; Sano, E.; Hanashima, Y.; Ozawa, Y.; Yoshimura, S.; Yamamuro, S.; Sumi, K.; Hara, H.; Katayama, Y.; et al. Anti-tumor effects of anti-epileptic drugs in malignant glioma cells. Oncol. Rep. 2022, 48, 216. [Google Scholar] [CrossRef] [PubMed]
- Mayer, J.; Kirschstein, T.; Resch, T.; Porath, K.; Krause, B.J.; Köhling, R.; Lange, F. Perampanel Attenuates Epileptiform Phenotype in C6 Glioma. Neurosci. Lett. 2020, 715, 134629. [Google Scholar] [CrossRef] [PubMed]
- Lange, F.; Hartung, J.; Liebelt, C.; Boisserée, J.; Resch, T.; Porath, K.; Hörnschemeyer, J.; Reichart, G.; Sellmann, T.; Neubert, V.; et al. Perampanel Add-on to Standard Radiochemotherapy in Vivo Promotes Neuroprotection in a Rodent F98 Glioma Model. Front. Neurosci. 2020, 14, 598266. [Google Scholar] [CrossRef]
- Vecht, C.; Duran-Peña, A.; Houillier, C.; Durand, T.; Capelle, L.; Huberfeld, G. Seizure Response to Perampanel in Drug-Resistant Epilepsy with Gliomas: Early Observations. J. Neurooncol. 2017, 133, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Izumoto, S.; Miyauchi, M.; Tasaki, T.; Okuda, T.; Nakagawa, N.; Nakano, N.; Kato, A.; Fujita, M. Seizures and Tumor Progression in Glioma Patients with Uncontrollable Epilepsy Treated with Perampanel. Anticancer Res. 2018, 38, 4361–4366. [Google Scholar] [CrossRef]
- Dunn-Pirio, A.M.; Woodring, S.; Lipp, E.; Herndon, J.E.; Healy, P.; Weant, M.; Randazzo, D.; Desjardins, A.; Friedman, H.S.; Peters, K.B. Adjunctive Perampanel for Glioma-Associated Epilepsy. Epilepsy Behav. Case Rep. 2018, 10, 114–117. [Google Scholar] [CrossRef]
- Chonan, M.; Saito, R.; Kanamori, M.; Osawa, S.I.; Watanabe, M.; Suzuki, H.; Nakasato, N.; Tominaga, T. Experience of Low Dose Perampanel to Add-on in Glioma Patients with Levetiracetam-Uncontrollable Epilepsy. Neurol. Med. Chir. 2020, 60, 37–44. [Google Scholar] [CrossRef]
- Maschio, M.; Pauletto, G.; Zarabla, A.; Maialetti, A.; Lus, T.; Villani, V.; Fabi, A.; Koudriavtseva, T.; Giannarelli, D. Perampanel in Patients with Brain Tumor-Related Epilepsy in Real-Life Clinical Practice: A Retrospective Analysis. Int. J. Neurosci. 2019, 129, 593–597. [Google Scholar] [CrossRef]
- Maschio, M.; Zarabla, A.; Maialetti, A.; Giannarelli, D.; Koudriavtseva, T.; Villani, V.; Zannino, S. Perampanel in Brain Tumor-Related Epilepsy: Observational Pilot Study. Brain Behav. 2020, 10, e01612. [Google Scholar] [CrossRef]
- Coppola, A.; Zarabla, A.; Maialetti, A.; Villani, V.; Koudriavtseva, T.; Russo, E.; Nozzolillo, A.; Sueri, C.; Belcastro, V.; Balestrini, S.; et al. Perampanel Confirms to Be Effective and Well-Tolerated as an Add-On Treatment in Patients With Brain Tumor-Related Epilepsy (PERADET Study). Front. Neurol. 2020, 11, 592. [Google Scholar] [CrossRef]
- Heugenhauser, J.; Iglseder, S.; Muigg, A.; Kerschbaumer, J.; Stockhammer, G.; Nowosielski, M.; Unterberger, I. Perampanel in Brain Tumor and SMART-Syndrome Related Epilepsy—A Single Institutional Experience. J. Neurol. Sci. 2021, 423, 117386. [Google Scholar] [CrossRef] [PubMed]
- Fycompa. (Perampanel) [Package Insert]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/202834s011lbl.pdf (accessed on 16 December 2022).
- Ishiuchi, S.; Tsuzuki, K.; Yoshida, Y.; Yamada, N.; Hagimura, N.; Okado, H.; Miwa, A.; Kurihara, H.; Nakazato, Y.; Sasaki, T.; et al. Blockage of Ca(2+)-Permeable AMPA Receptors Suppresses Migration and Induces Apoptosis in Human Glioblastoma Cells. Nat. Med. 2002, 8, 971–978. [Google Scholar] [CrossRef]
- Seker, F.; Cingoz, A.; Sur-Erdem, İ.; Erguder, N.; Erkent, A.; Uyulur, F.; Selvan, M.E.; Gümüş, Z.H.; Gönen, M.; Bayraktar, H.; et al. Identification of SERPINE1 as a Regulator of Glioblastoma Cell Dispersal with Transcriptome Profiling. Cancers 2019, 11, 1651. [Google Scholar] [CrossRef]
- Schrey, M.; Codina, C.; Kraft, R.; Beetz, C.; Kalff, R.; Wölfl, S.; Patt, S. Molecular Characterization of Voltage-Gated Sodium Channels in Human Gliomas. Neuroreport 2002, 13, 2493–2498. [Google Scholar] [CrossRef]
- Joshi, A.D.; Parsons, D.W.; Velculescu, V.E.; Riggins, G.J. Sodium Ion Channel Mutations in Glioblastoma Patients Correlate with Shorter Survival. Mol. Cancer 2011, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, G.D.; Eljamel, S. Impact of Particular Antiepileptic Drugs on the Survival of Patients with Glioblastoma Multiforme. J. Neurosurg. 2013, 118, 859–865. [Google Scholar] [CrossRef]
- Ishiuchi, S.; Yoshida, Y.; Sugawara, K.; Aihara, M.; Ohtani, T.; Watanabe, T.; Saito, N.; Tsuzuki, K.; Okado, H.; Miwa, A.; et al. Ca2+-Permeable AMPA Receptors Regulate Growth of Human Glioblastoma via Akt Activation. J. Neurosci. 2007, 27, 7987–8001. [Google Scholar] [CrossRef]
- Wang, X.Y.; Li, Y.L.; Wang, H.Y.; Zhu, M.; Guo, D.; Wang, G.L.; Gao, Y.T.; Yang, Z.; Li, T.; Yang, C.Y.; et al. Propofol Inhibits Invasion and Proliferation of C6 Glioma Cells by Regulating the Ca2+ Permeable AMPA Receptor-System Xc- Pathway. Toxicol. Vitr. 2017, 44, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Rösche, J.; Piek, J.; Hildebrandt, G.; Grossmann, A.; Kirschstein, T.; Benecke, R. Perampanel in the Treatment of a Patient with Glioblastoma Multiforme without IDH1 Mutation and without MGMT Promotor Methylation. Fortschr. Neurol. Psychiatr. 2015, 83, 286–289. [Google Scholar] [CrossRef]
- Feyissa, A.M.; Worrell, G.A.; Tatum, W.O.; Chaichana, K.L.; Jentoft, M.E.; Guerrero Cazares, H.; Ertekin-Taner, N.; Rosenfeld, S.S.; ReFaey, K.; Quinones-Hinojosa, A. Potential Influence of IDH1 Mutation and MGMT Gene Promoter Methylation on Glioma-Related Preoperative Seizures and Postoperative Seizure Control. Seizure 2019, 69, 283–289. [Google Scholar] [CrossRef]
- Chen, H.; Judkins, J.; Thomas, C.; Wu, M.; Khoury, L.; Benjamin, C.G.; Pacione, D.; Golfinos, J.G.; Kumthekar, P.; Ghamsari, F.; et al. Mutant IDH1 and Seizures in Patients with Glioma. Neurology 2017, 88, 1805. [Google Scholar] [CrossRef] [Green Version]
- van der Meer, P.B.; Dirven, L.; Fiocco, M.; Vos, M.J.; Kouwenhoven, M.C.M.; van den Bent, M.J.; Taphoorn, M.J.B.; Koekkoek, J.A.F. First-line antiepileptic drug treatment in glioma patients with epilepsy: Levetiracetam vs valproic acid. Epilepsia 2021, 62, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, P.B.; Taphoorn, M.J.B.; Koekkoek, J.A.F. Management of epilepsy in brain tumor patients. Curr. Opin. Oncol. 2022, 34, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Vecht, C.J.; Wagner, G.L.; Wilms, E.B. Interactions between antiepileptic and chemotherapeutic drugs. Lancet Neurol. 2003, 2, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Post, D.S.; van der Veer, A.; Schijns, O.E.M.G.; Klinkenberg, S.; Rijkers, K.; Wagner, G.L.; van Kranen-Mastenbroek, V.H.J.M.; Willems, P.C.P.H.; Verhezen, P.W.M.; Beckers, E.A.M.; et al. Assessment of need for hemostatic evaluation in patients taking valproic acid: A retrospective cross-sectional study. PLoS ONE 2022, 17, e0264351. [Google Scholar] [CrossRef] [PubMed]
- Perampanel. Highlights of Prescribing Information. Available online: https://www.fycompa.com/-/media/Files/Fycompa/Fycompa_Prescribing_Information.pdf. (accessed on 9 February 2023).
- Majid, O.; Laurenza, A.; Ferry, J.; Hussein, Z. Impact of perampanel on pharmacokinetics of concomitant antiepileptics in patients with partial-onset seizures: Pooled analysis of clinical trials. Br. J. Clin. Pharmacol. 2016, 82, 422–430. [Google Scholar] [CrossRef]
- Effect of Perampanel on Peritumoral Hyperexcitability in HGG—Full Text View—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04497142?term=perampanel&age=12&draw=2&rank=5 (accessed on 16 December 2022).
- Perampanel for the Reduction of Seizure Frequency in Patients With High-Grade Glioma and Focal Epilepsy—Full Text View—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04650204?term=perampanel&age=12&draw=4&rank=23 (accessed on 16 December 2022).



{kind=link}
{kind=link}
| Study (Year) | Study Design | Main Findings |
|---|---|---|
| Cunningham (2016) | Ex vivo | PER blocked inter-ictal discharges in ex vivo human peritumoral brain slices |
| Lange et al. (2019) | In vitro | PER showed systematic inhibitory effects on cell proliferation in patient-derived low-passage cell lines of glioblastoma. Metastasis cells were more resistant to PER. Glucose uptake was attenuated in all glioblastoma cells after exposure to PER, whereas apoptosis was not induced |
| Lai et al. (2019) | In vitro | PER suppressed voltage-gated Na+ currents in U87 glioma cells |
| Mayer et al. (2019) | In vitro, in vivo | PER reduced glucose uptake in vitro without affecting extracellular glutamate levels. PER prevented recurrent epileptiform discharges in brain slices from rats bearing C6 glioma. PER did not reduce tumor size |
| Lange et al. (2020) | In vivo | PER showed anticonvulsant properties in rodent F98 glioma model. PER as an add-on treatment to radiochemotherapy had no effect on tumor progression, but preserved the glutamatergic network activity on healthy peritumoral tissue |
| Salmaggi et al. (2021) | In vitro | PER showed antitumor activity in glioblastoma cell lines U87, U138, A172 and the grade III astrocytoma cell line SW1783, via a pro-apoptotic effect. The combination of PER and temozolomide had a significant synergistic effect |
| Tatsuoka et al. (2022) | In vitro | PER showed inhibitory effects on cell viability in a dose-dependent manner on malignant glioma cell lines A-172, AM-38, T98G, U-138MG, U-251MG and YH-13, via a pro-apoptotic effect |
| Yagi et al. (2022) | In vitro | Inhibitory effect on cell proliferation of PER confirmed on A-172, AM-38, T98G, U-138MG, U-251MG and YH-13 cell lines. PER and temozolomide showed synergistic effect on T98G and U-251MG lines. PER suppressed migration of T98G and U-251MG cells. |
| Study (Year) | Study Design | Number of Participants | Main Efficacy Findings |
|---|---|---|---|
| Vecht et al. (2017) | Prospective study | 12 | Objective seizure response in 9 out of 12 patients (75%): 50% seizure reduction in 3 patients and seizure-freedom in 6 patients |
| Izumoto et al. (2018) | Case series | 12 | Seizure frequency reduction ≥50% in 12/12 patients, with six patients (60%) seizure free |
| Dunn-Pirio et al. (2018) | Prospective study | 8 | Self-reported seizure reduction in 6 out of 8 patients; percent seizure reduction not available as baseline seizure frequencies were not collected. No participants reached seizure freedom |
| Maschio et al. (2019) | Retrospective study | 11 | After 12 months of PER add-on therapy, 5 patients were seizure-free, 4 had ≥50% seizure frequency reduction, and seizure frequency was unchanged in 2 patients. The responder rate was 81.8%. The final median dose of PER was 7.3 mg/day |
| Chonan et al. (2020) | Retrospective study | 18 | All patients were receiving LEV monotherapy. Seventeen of 18 patients achieved seizure freedom with 2–4 mg of PER. The median time to achieve seizure freedom after PER add-on was 11 days (range 0–2 months) |
| Maschio et al. (2020) | Prospective study | 26 | After 6 months of follow-up, 8 patients were seizure-free, 15 had ≥50% seizure reduction, and 3 remained stable. Five patients dropped out. No significant differences was found in seizure control in patients with/without IDH1 mutation and MGMT methylation |
| Coppola et al. (2020) | Prospective study | 36 | After 12 months of follow-up, 21 patients were available for evaluation, with a responder rate of 90.4% and 33.3% of patients being seizure-free |
| Heugenhauser et al. (2021) | Case series | 5 | The responder rate was 40%, with 2 patients experiencing a ≥50% reduction in seizure frequency after add-on treatment with PER. One patient was seizure-free after 1 year |
| Study (Year) | Patients with Adverse Effects (%) | Adverse Effects (% of Patients) | Discontinuation of PER Due to Adverse Effects (% of Patients) |
|---|---|---|---|
| Vecht et al. (2017) | 6 (50) | Dizziness (33), drowsiness (17) | 1 (8) |
| Izumoto et al. (2018) | 2 (17) | Dizziness (17) | 1 (8) |
| Dunn-Pirio et al. (2018) | NR | Fatigue (63), dizziness (25), confusion (13), nausea (13), somnolence (13), insomnia (NR), anxiety (NR) | 1 (13) |
| Maschio et al. (2019) | 2 (18) | Anxiety (9), agitation (9) | 0 (0) |
| Chonan et al. (2020) | 2 (11) | Irritability (11) | 0 (0) |
| Maschio et al. (2020) | 4 (15) | Vertigo (7.5), aggressiveness (7.5) | 2 (8) |
| Coppola et al. (2020) | 11 (31) | Anxiety (6), aggressiveness (6), dizziness (14), fatigue (6) | 3 (27) |
| Heugenhauser et al. (2021) | 2 (40) | Fatigue (20), aggressiveness (20) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabaee Damavandi, P.; Pasini, F.; Fanella, G.; Cereda, G.S.; Mainini, G.; DiFrancesco, J.C.; Trinka, E.; Lattanzi, S. Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review. Brain Sci. 2023, 13, 326. https://doi.org/10.3390/brainsci13020326
Tabaee Damavandi P, Pasini F, Fanella G, Cereda GS, Mainini G, DiFrancesco JC, Trinka E, Lattanzi S. Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review. Brain Sciences. 2023; 13(2):326. https://doi.org/10.3390/brainsci13020326
Chicago/Turabian StyleTabaee Damavandi, Payam, Francesco Pasini, Gaia Fanella, Giulia Sofia Cereda, Gabriele Mainini, Jacopo C. DiFrancesco, Eugen Trinka, and Simona Lattanzi. 2023. "Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review" Brain Sciences 13, no. 2: 326. https://doi.org/10.3390/brainsci13020326
APA StyleTabaee Damavandi, P., Pasini, F., Fanella, G., Cereda, G. S., Mainini, G., DiFrancesco, J. C., Trinka, E., & Lattanzi, S. (2023). Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review. Brain Sciences, 13(2), 326. https://doi.org/10.3390/brainsci13020326