
Cerebrolysin in Patients with TBI: Systematic Review and Meta-Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
- Human studies
- Adult patients (>18 y)
- Diagnosis of mild, moderate, or severe TBI (head trauma, brain trauma)
- Animal studies, in vitro studies, reviews, systematic reviews, editorials, individual case reports, and opinion, editorial, or perspectives articles
- Pediatric patients (<18 y)
- Pregnant patients
- Multiorgan failure
- Studies in language other than English
2.1.1. Data Abstraction
2.1.2. Outcomes
2.1.3. Data Synthesis and Statistical Analysis
3. Results
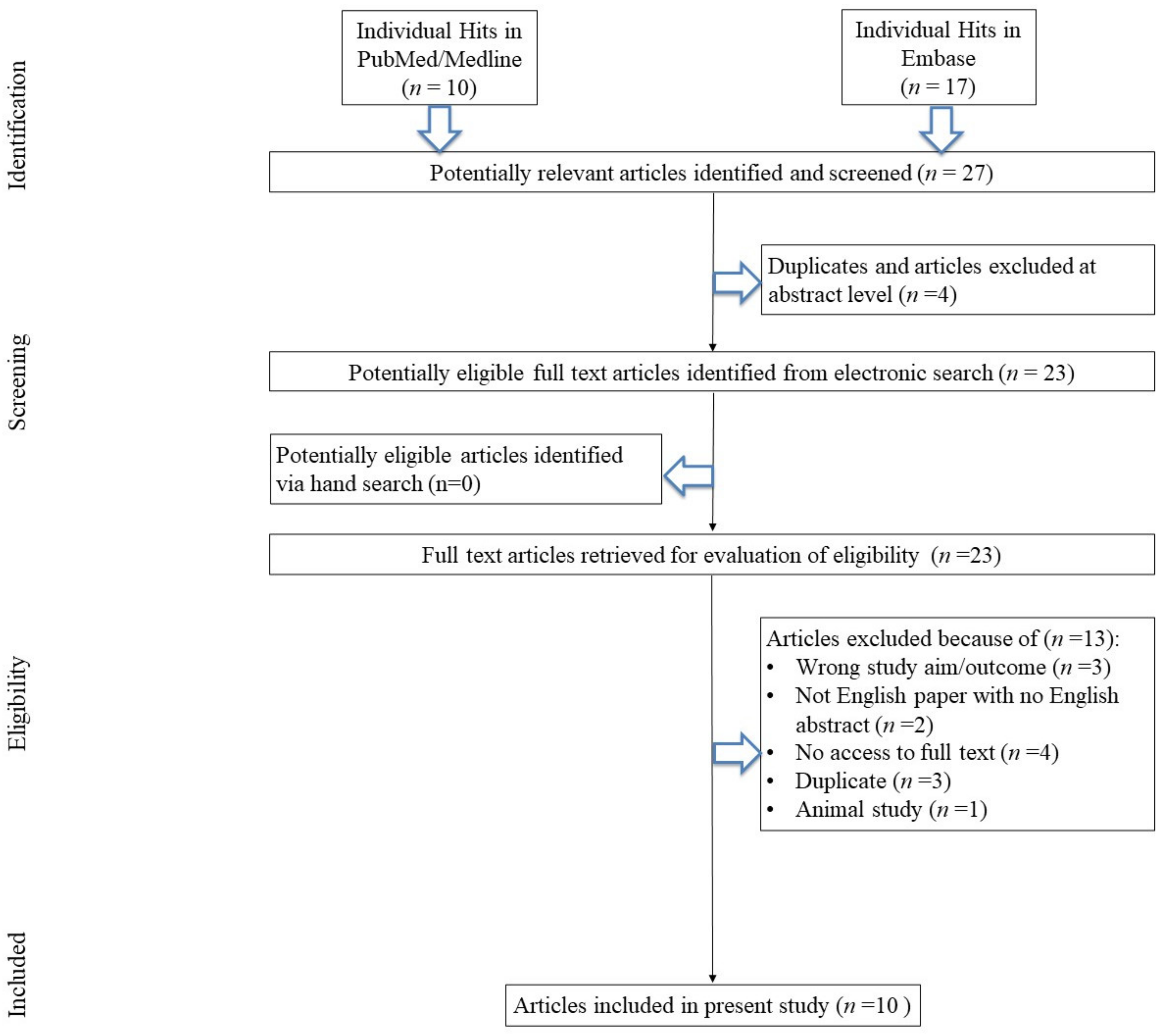
3.1. Search Results
3.2. Study, Patients, and Treatment Characteristics
3.3. Effects on GCS Score at Endpoint
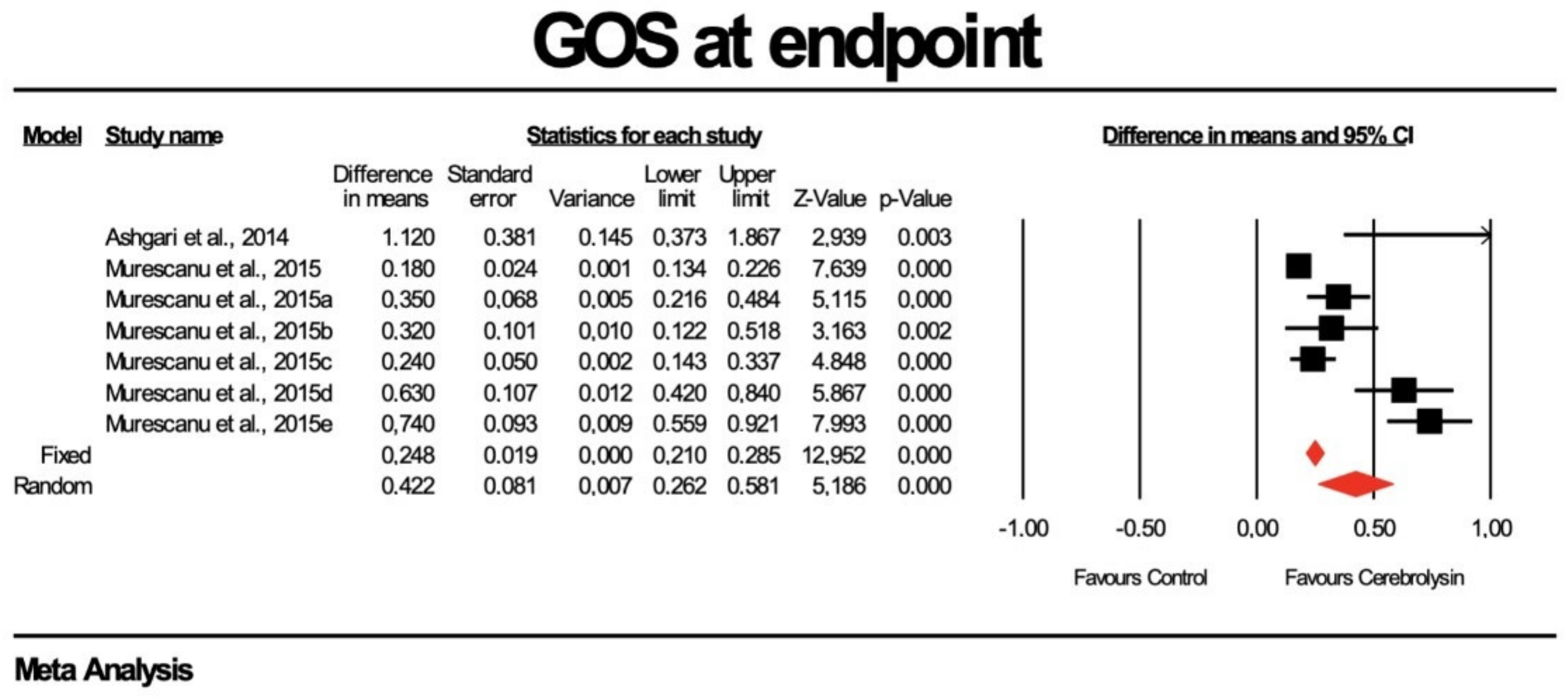
3.4. Effects on GOS Score at Endpoint
3.5. Effects on Hospital LOS
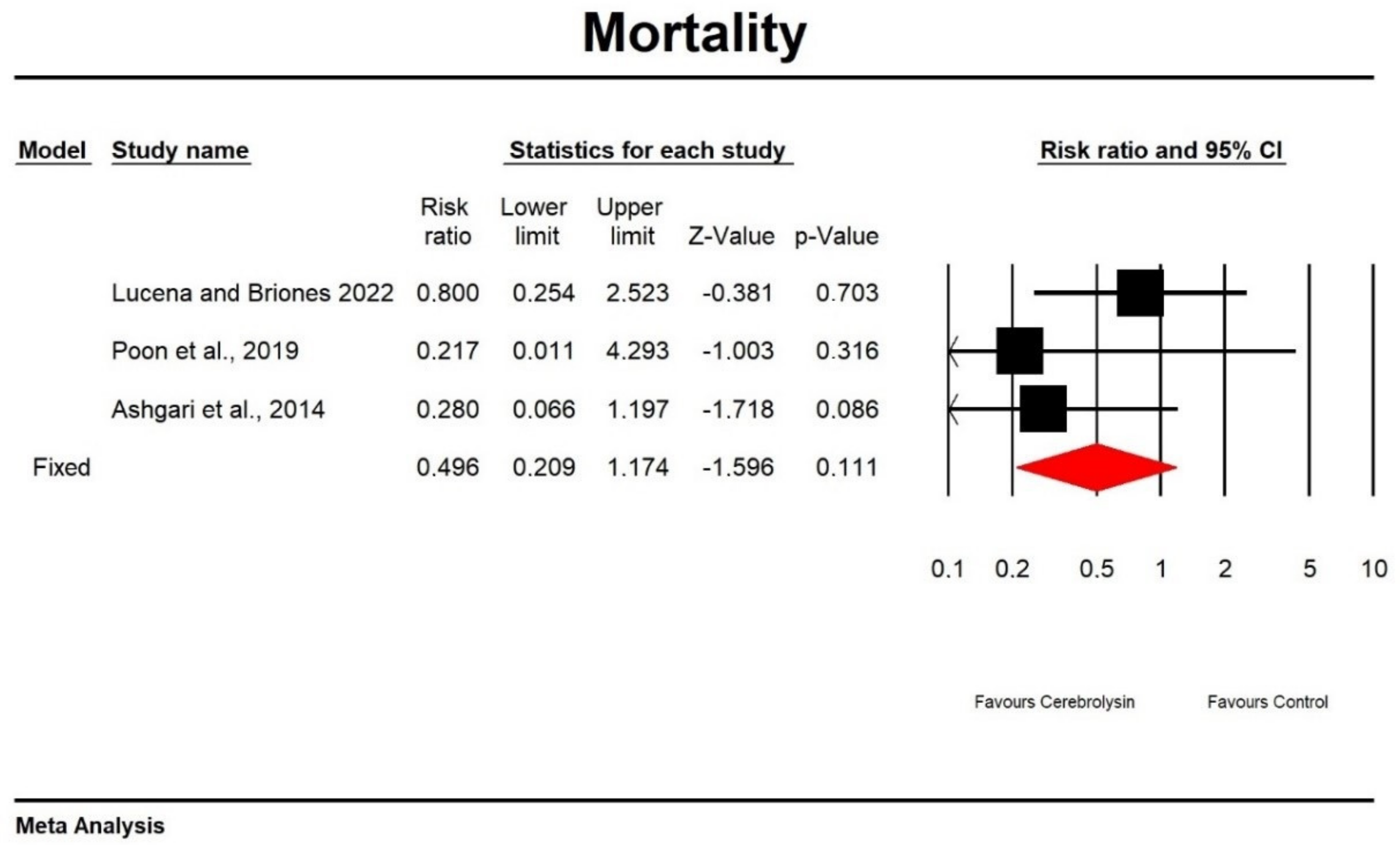
3.6. Effects on Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, J.-Y.; Gao, G.-Y.; Feng, J.-F.; Mao, Q.; Chen, L.-G.; Yang, X.-F.; Liu, J.-F.; Wang, Y.-H.; Qiu, B.-H.; Huang, X.-J. Traumatic brain injury in China. Lancet Neurol. 2019, 18, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Majdan, M.; Plancikova, D.; Brazinova, A.; Rusnak, M.; Nieboer, D.; Feigin, V.; Maas, A. Epidemiology of traumatic brain injuries in Europe: A cross-sectional analysis. Lancet Public Health 2016, 1, e76–e83. [Google Scholar] [CrossRef] [PubMed]
- Carney, N.; Totten, A.M.; O-Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2016, 1, 1–10. [Google Scholar] [CrossRef]
- Gerber, L.M.; Chiu, Y.; Carney, N.; Hartl, R.; Ghajar, J. Marked reduction in mortality in patients with severe traumatic brain injury. J. Neurosurg. 2013, 119, 1583–1590. [Google Scholar] [CrossRef] [Green Version]
- Hawryluk, G.W.J.; Aguilera, S.; Buki, A.; Bulger, E.; Citero, G.; Cooper, D.J.; Arrastia, R.D.; Diringer, M.; Figaji, A.; Gao, G.; et al. A management algorithm for patients with intracranial pressure monitoring: The Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2019, 45, 1783–1794. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Chopp, M.; Meng, Y.; Zhang, Z.G.; Doppler, E.; Mahmood, A.; Xiong, Y. Improvement in functional recovery with administration of Cerebrolysin after experimental closed head injury. J. Neurosurg. 2013, 118, 1343–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Chopp, M.; Meng, Y.; Zhang, Z.G.; Doppler, E.; Winter, S.; Schallert, T.; Mahmood, A.; Xiong, Y. Cerebrolysin improves cognitive performance in rats after mild traumatic brain injury. J. Neurosurg. 2015, 122, 843–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shmakova, A.A.; Androsova, L.W. Investigating the effect of central nervous system drugs on leukocyte elastase activity in vitro. Eur. Neuropsychopharmacol. 2018, 28, 13–14. [Google Scholar] [CrossRef]
- Fiani, B.; Covarrubias, C.; Wong, A.; Doan, T.; Reardon, T.; Nikolaidis, D.; Sarno, E. Cerebrolysin for stroke, neurodegeneration, and traumatic brain injury: Review of the literature and outcomes. Neurol. Sci. 2021, 42, 1345–1353. [Google Scholar] [CrossRef]
- Chen, S.-D.; Yang, J.-L.; Hwang, W.-C.; Yang, D.-I. Emerging roles of sonic hedgehog in adult neurological diseases: Neurogenesis and beyond. Int. J. Mol. Sci. 2018, 19, 2423. [Google Scholar] [CrossRef] [Green Version]
- Lai, K.; Kaspar, B.K.; Gage, F.H.; Schaffer, D.V. Sonic hedgehog regulates adult neural progenitor proliferation in vitro and in vivo. Nat. Neurosci. 2003, 6, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Masliah, E.; Diez-Tejedor, E. The pharmacology of neurotrophic treatment with Cerebrolysin: Brain protection and repair to counteract pathologies of acute and chronic neurological disorders. Drugs Today 2012, 48, 3–24. [Google Scholar]
- Zhang, Y.; Chopp, M. Cerebrolysin reduces astrogliosis and axonal injury and enhances neurogenesis in rats after closed head injury. Neurorehabil. Neural Repair 2019, 33, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.K.C.; Zhu, X.L.; Poon, W.S. Beneficial effect of cerebrolysin on moderate and severe head injury patients: Result of a cohort study. In Intracranial Pressure and Brain Monitoring XII; Springer: Vienna, Austria, 2005; Volume 95. [Google Scholar] [CrossRef]
- Muresanu, D.F.; Florian, S.; Homberg, V.; Matula, C.; Von Steinbuchel, N.; Vos, P.E.; Wild, K.; Birle, C.; Muresanu, I.; Slavoaca, D.; et al. Efficacy and safety of cerebrolysin in neurorecovery after moderate-severe traumatic brain injury: Results from the CAPTAIN II trial. Neurol. Sci. 2020, 41, 1171–1181. [Google Scholar] [CrossRef]
- Sharma, H.S.; Zimmermann-Meinzingen, S.; Johanson, C.E. Cerebrolysin reduces blood-cerebrospinal fluid barrier permeability change, brain pathology, and functional deficits following traumatic brain injury in the rat. Ann. N. Y. Acad. Sci. 2010, 1199, 125–137. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Chneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R.A. Nonparametric “Trim and Fill” Method of Accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar] [CrossRef]
- Khalili, H.; Niakan, A.; Ghaffarpasand, F. Effects of cerebrolysin on functional recovery in patients with severe disability after traumatic brain injury: A historical cohort study. Clin. Neurol. Neurosurg. 2017, 152, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Asghari, M.; Meshkini, A.; Salehpoor, F.; Aghazadek, J.; Shakeri, M.; Shokohi, G.; Ebrahimi, N.; Bazazi, A.M.; Pourhajshokr, N. Investigation of the effect of cerebrolysin on patients with head trauma and diffuse axonal injury. Int. J. Curr. Res. Acad. Rev. 2014, 2, 1–8. [Google Scholar]
- Muresanu, D.F.; Ciurea, A.V.; Gorgan, R.M.; Gheoghita, E.; Florian, S.; Stan, H.; Blaga, A.; Ianovici, N.; Iencean, S.M.; Turliuc, D.; et al. A retrospective, multi-center cohort study evaluating the severity-related effects of cerebrolysin treatment on clinical outcomes in traumatic brain injury. CNS Neurol. Disord. Drug Targets 2015, 14, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvarez, X.A.; Sampedro, C.; Figueroa, J.; Tellado, I.; Gonzalez, A.; Garcia-Fantini, M.; Cacabelos, R.; Muresanu, D.; Moessler, H. Reductions in qEEG slowing over 1 year and after treatment with Cerebrolysin in patients with moderate–severe traumatic brain injury. J. Neural Transm. 2008, 115, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, X.A.; Sampedro, C.; Perez, P.; Laredo, M.; Couceiro, V.; Hernandez, A.; Figueroa, J.; Varela, M.; Dulce, A.; Dprzp, L.; et al. Positive effects of Cerebrolysin on electroencephalogram slowing, cognition and clinical outcome in patients with postacute traumatic brain injury: An exploratory study. Int. Clin. Psychopharmacol. 2003, 18, 271–278. [Google Scholar] [CrossRef]
- Chen, C.C.; Wei, S.-T.; Tsaia, S.-C.; Chen, X.-X.; Cho, D.-Y. Cerebrolysin enhances cognitive recovery of mild traumatic brain injury patients: Double-blind, placebo-controlled, randomized study. Br. J. Neurosurg. 2013, 27, 803–807. [Google Scholar] [CrossRef]
- Lucena, L.L.; Briones, M.V.A. Effect of Cerebrolysin in severe traumatic brain injury: A multi-center, retrospective cohort study. Clin. Neurol. Neurosurg. 2022, 216, 107216. [Google Scholar] [CrossRef] [PubMed]
- Poon, W.; Matula, C.; Vos, P.E.; Muresanu, D.F.; Steinbuchel, N.; Wild, K.; Homberg, V.; Wang, E.; Lee, T.M.C.; Strilciuc, S.; et al. Safety and efficacy of Cerebrolysin in acute brain injury and neurorecovery: CAPTAIN I—A randomized, placebo-controlled, double-blind, Asian-Pacific trial. Neurol. Sci. 2020, 41, 281–293. [Google Scholar] [CrossRef]
- Ghaffarpasand, F.; Torabi, S.; Rasti, A.; Niakanm, M.H.; Aghakablou, A.; Pakzad, F.; Beheshtian, M.S.; Tabrizi, R. Effects of cerebrolysin on functional outcome of patients with traumatic brain injury: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2018, 15, 127–135. [Google Scholar] [CrossRef] [Green Version]
- El Sayed, I.; Zaki, A.; Fayed, A.M.; Shehat, G.M.; Abdelmonem, S. A meta-analysis of the effect of different neuroprotective drugs in management of patients with traumatic brain injury. Neurosurg. Rev. 2018, 41, 427–438. [Google Scholar] [CrossRef]
- Shin, D.-S.; Hwang, S.-C. Serial Brain CT Scans in Severe Head Injury without Intracranial Pressure Monitoring. KJNT 2014, 10, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Brazinova, A.; Rehorcikova, V.; Taylor, M.S.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.; van Veen, E.; Yang, C.; Huijben, J.A.; Lingsma, H.F.; Gao, G.; Jiang, J. Comparison of care system and treatment approaches for patients with traumatic brain injury in China versus Europe: A CENTER-TBI survey study. J. Neurotrauma 2020, 37, 1806–1817. [Google Scholar] [CrossRef]
- Muresanu, D.; Birle, C.; Muresanu, I.; Costin, C.; Vester, J.; Rafila, A. Neuroprotection in TBI. In Neurotrauma: A Comprehensive Textbook on Traumatic Brain Injury and Spinal Cord Injury; Wang, K.K.W., Ed.; Oxford University Press: New York, NY, USA, 2018; pp. 333–346. [Google Scholar]
- Sharma, H.S.; Muresanu, D.F.; Sahib, S.; Tian, Z.R.; Lafuente, J.V.; Buzoianu, A.D.; Castellani, R.J.; Nozari, A.; Li, C.; Zhang, Z.; et al. Cerebrolysin restores balance between excitatory and inhibitory amino acids in brain following concussive head injury. Superior neuroprotective effects of TiO2 nanowired drug delivery. Prog. Brain Res. 2021, 266, 211–267. [Google Scholar] [CrossRef] [PubMed]
- Wheaton, P.; Mathias, J.L.; Vink, R. Impact of pharmacological treatments on cognitive and behavioral outcome in the postacute stages of adult traumatic brain injury: A meta-analysis. J. Clin. Psychopharmacol. 2011, 31, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Vester, J.C.; Buzoianu, A.D.; Florian, S.I.; Homberg, V.; Kim, S.-H.; Lee, T.M.C.; Matula, C.; Poon, W.S.; Steinbuchel, N. Cerebrolysin after moderate to severe traumatic brain injury: Prospective meta-analysis of the CAPTAIN trial series. Neurol. Sci. 2021, 42, 4531–4541. [Google Scholar] [CrossRef] [PubMed]
- Bayley, M.; Ponsford, J.; Jeffay, E.; Ponsford, J.; Harnett, A.; Janzen, S.; Patsakos, E.; Douglas, J.; Kennedy, M.; Kua, A.; et al. INCOG 2.0 Guidelines for Cognitive Rehabilitation Following Traumatic Brain Injury, Part III: Executive Functions. J. Head Trauma Rehabil. 2023, 38, 52–64. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Strings with Medical Subject Headings |
|---|---|
| Pub Med./Cinahl/Web Of Science | (traumatic brain injury OR brain injuries, traumatic OR brain lesion, traumatic OR brain system trauma OR brain trauma OR cerebral trauma OR cerebrovascular trauma OR encephalopathy, traumatic OR mild traumatic brain injury OR organic cerebral trauma OR posttraumatic encephalopathy OR traumatic brain injuries OR traumatic brain injury OR traumatic brain lesion OR traumatic cerebral lesion OR traumatic encephalopathy) AND (cerebrolysin OR cerebrolysin OR cerebrolysine) AND (glasgow outcome scale OR rankin scale OR mini mental state examination OR mortality OR barthel index OR barthel adl index OR barthel index) |
| Embase | (‘traumatic brain injury’/exp OR ‘brain injuries, traumatic’ OR ‘brain lesion, traumatic’ OR ‘brain system trauma’ OR ‘brain trauma’ OR ‘cerebral trauma’ OR ‘cerebrovascular trauma’ OR ‘encephalopathy, traumatic’ OR ‘mild traumatic brain injury’ OR ‘organic cerebral trauma’ OR ‘posttraumatic encephalopathy’ OR ‘traumatic brain injuries’ OR ‘traumatic brain injury’ OR ‘traumatic brain lesion’ OR ‘traumatic cerebral lesion’ OR ‘traumatic encephalopathy’) AND (‘cerebrolysin’/exp OR ‘cerebrolysin’ OR ‘cerebrolysine’) AND (‘glasgow outcome scale’/exp OR ‘rankin scale’/exp OR ‘mini mental state examination’/exp OR ‘mortality’/exp OR ‘barthel index’/exp OR ‘barthel adl index’ OR ‘barthel index’) |
| Study Characteristics | Intervention | Comparator | Sample Characteristics | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Country | Sponsorship | Blinding (Y/N) | Trial Duration (Days) | N Total Analyzed | Cerebrolysin Mean Dose/Day (mL); Duration | PBO or Other Intervention | Age (Mean) | N Male | % Male | Seizure (Y/N) |
| Alvarez et al., 2008 [23] | Spain | industry | N | 30 days | 59 | 30 mL/day, 20 infusions over 4 weeks | NA | 30.4 | 40 | 68 | ND |
| Alvarez et al., 2003 [24] | Spain | industry | N | 30 days | 20 | 30 mL/day, 20 infusions over 4 weeks | Y | 30.1 | 15 | 75 | 4 |
| Chen et al., 2012 [25] | Taiwan | ND | Y | 3 months | 32 | 30 mL/day 5 days | PBO | 44.8 | 21 | 66 | 0/32 |
| Khalili et al., 2017 [20] | Iran | academia | N | 6 months | 129 | 10 mL/day 30 days | NA | 33.3 | 109 | 85 | Y |
| Lucena et al., 2022 [26] | Philippines | ND | N | 28 days | 87 | 30 mL/day Cerebrolysin for 14 days, 10 mL/day dosage for another 14 days | NA | 34 | 73 | 84 | ND |
| Poon et al., 2019 [27] | Hong Kong, Taiwan, Republic of Korea, Singapore, Philippines | industry | Y | 30 days | 40 | 50 mL of Cerebrolysin daily for 10 days, followed by two additional treatment cycles with 10 mL daily for 10 days | PBO | 38.1 | 32 | 80 | ND |
| Wong et al., 2005 [14] | China | ND | N | 6 months | 21 | 50 mL/day, 20 days | NA | 64 | 13 | 62 | ND |
| Ashgari et al., 2014 [21] | Iran | ND | N | 1 month | 53 | 10 mL/day, 10 days | NA | 30 | 49 | 92 | ND |
| Murescanu et al., 2015 [22] | Romania | ND | N | 1 month | 7693 | 20 mL/day, 10 days | NA | 47 | 5415 | 70 | ND |
| Murescanu et al., 2015a [22] | Romania | ND | N | 1 month | 6627 | 30 mL/day, 10 days | NA | 47 | 5415 | 70 | ND |
| Muresanu et al., 2020 [15] | Romania | ND | Y | 3 months | 139 | 50 mL/day for 10 days, two additional treatment cycles with 10 mL per day for 10 days) | PBO | 47.4 | 123 | 88.5 | ND |
| Reference | Surgery Qualification | Adverse Events | |||
|---|---|---|---|---|---|
| Craniotomy (Y/N) | Cerebrolysin Events | Cerebrolysin n | Comparator Events | Comparator n | |
| Alvarez et al., 2008 [23] | ND | ND | ND | ND | ND |
| Alvarez et al., 2003 [24] | ND | 5 | 20 | NA | NA |
| Chet et al., 2012 [25] | N | ND | 32 | ND | 21 |
| Khalil et al., 2017 [20] | 42/36 | 9 | 65 | 4 | 64 |
| Lucena et al., 2022 [26] | N | ND | 42 | ND | 45 |
| Poon et al., 2019 [27] | ND | 0 | 22 | 0 | 24 |
| Wong et al., 2005 [14] | ND | 0 | 21 | 0 | 21 |
| Ashgari et al., 2014 [21] | ND | 0 | 25 | 0 | 28 |
| Murescanu et al., 2015 [22] | ND | 97 | 1142 | 541 | 6151 |
| Reference | Treatment Initiation Time | Initial GCS | TBI Severity [n] | ||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||
| Alvarez et al., 2008 [23] | 23 months | 5.5 | 4 | 3 | 32 |
| Alvarez et al., 2003 [24] | 23 and 1107 days | 6.1 | 3 | 1 | 16 |
| Chet et al., 2012 [25] | 24 h | >14 | 32 | 0 | 0 |
| Khalil et al., 2017 [20] | 1 month | 6.02 | 0 | 0 | 129 |
| Lucena et al., 2022 [26] | <1 month | 5.84 | 0 | 0 | 87 |
| Poon et al., 2019 [27] | 6 h | 9.9 | 0 | 40 | |
| Ashgari et al., 2014 [21] | 48 h | 6.75 | 0 | 0 | 53 |
| Murescanu et al., 2015 [22] | 48 h | 12.72 | 5125 | 587 | 1227 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarosz, K.; Kojder, K.; Andrzejewska, A.; Solek-Pastuszka, J.; Jurczak, A. Cerebrolysin in Patients with TBI: Systematic Review and Meta-Analysis. Brain Sci. 2023, 13, 507. https://doi.org/10.3390/brainsci13030507
Jarosz K, Kojder K, Andrzejewska A, Solek-Pastuszka J, Jurczak A. Cerebrolysin in Patients with TBI: Systematic Review and Meta-Analysis. Brain Sciences. 2023; 13(3):507. https://doi.org/10.3390/brainsci13030507
Chicago/Turabian StyleJarosz, Konrad, Klaudyna Kojder, Agata Andrzejewska, Joanna Solek-Pastuszka, and Anna Jurczak. 2023. "Cerebrolysin in Patients with TBI: Systematic Review and Meta-Analysis" Brain Sciences 13, no. 3: 507. https://doi.org/10.3390/brainsci13030507
APA StyleJarosz, K., Kojder, K., Andrzejewska, A., Solek-Pastuszka, J., & Jurczak, A. (2023). Cerebrolysin in Patients with TBI: Systematic Review and Meta-Analysis. Brain Sciences, 13(3), 507. https://doi.org/10.3390/brainsci13030507