
Application of Quantitative Computed Tomographic Perfusion in the Prognostic Assessment of Patients with Aneurysmal Subarachnoid Hemorrhage Coexistent Intracranial Atherosclerotic Stenosis
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Setting, and Data Sources
2.2. Study Population
2.3. Baseline Characteristics
2.4. CTP Parameter and RAPID
2.5. Outcome Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Association between Perfusion Parameter and 3-Month mRS
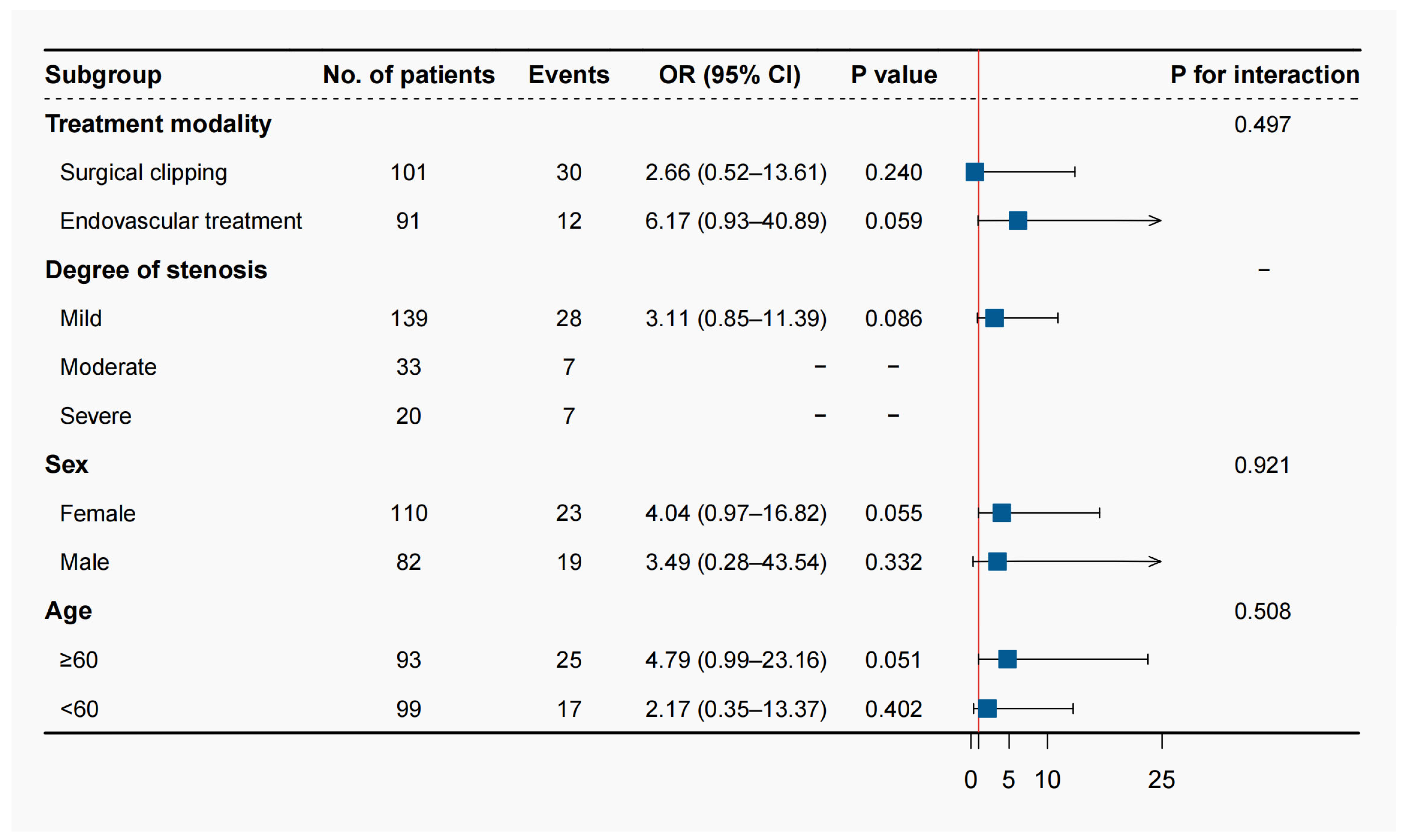
3.3. Prespecified Subgroup Analysis and Additive Value Assessment
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Petridis, A.K.; Kamp, M.A.; Cornelius, J.F.; Beez, T.; Beseoglu, K.; Turowski, B.; Steiger, H.J. Aneurysmal Subarachnoid Hemorrhage. Dtsch. Arztebl. Int. 2017, 114, 226–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappelle, L.; Eliasziw, M.; Fox, A.; Barnett, H.M. For the North American Symptomatic Carotid Endarterectomy Trial Group. Small, unruptured intracranial aneurysms and management of symptomatic carotid artery stenosis. Neurology 2000, 55, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Dippel, D.W.; Vermeulen, M.; Braakman, R.; Habbema, J.D. Transient ischemic attacks, carotid stenosis, and an incidental intracranial aneurysm. A decision analysis. Neurosurgery 1994, 34, 449–457, discussion 457–458. [Google Scholar] [CrossRef]
- Cherednychenko, Y.; Engelhorn, T.; Miroshnychenko, A.; Zorin, M.; Dzyak, L.; Tsurkalenko, O.; Cherednychenko, N. Endovascular treatment of patient with multiple extracranial large vessel stenosis and coexistent unruptured wide-neck intracranial aneurysm using a WEB device and Szabo-technique. Radiol. Case Rep. 2020, 15, 2522–2529. [Google Scholar] [CrossRef] [PubMed]
- Vergouwen, M.D.; Vermeulen, M.; van Gijn, J.; Rinkel, G.J.; Wijdicks, E.F.; Muizelaar, J.P.; Mendelow, A.D.; Juvela, S.; Yonas, H.; Terbrugge, K.G.; et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: Proposal of a multidisciplinary research group. Stroke 2010, 41, 2391–2395. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.A.; Patel, J.; Desikan, S.; Chrencik, M.; Martinez-Delcid, J.; Caraballo, B.; Yokemick, J.; Gray, V.L.; Sorkin, J.D.; Cebral, J.; et al. A symptomatic carotid artery stenosis is associated with cerebral hypoperfusion. J. Vasc. Surg. 2020, 73, 1611–1621.e2. [Google Scholar] [CrossRef]
- Fragata, I.; Alves, M.; Papoila, A.L.; Diogo, M.; Canhão, P.; Canto-Moreira, N. Temporal evolution of cerebral computed tomography perfusion after acute subarachnoid hemorrhage: A prospective cohort study. Acta Radiol. 2020, 61, 376–385. [Google Scholar] [CrossRef]
- Dankbaar, J.W.; de Rooij, N.K.; Rijsdijk, M.; Velthuis, B.K.; Frijns, C.J.; Rinkel, G.J.; van der Schaaf, I.C. Diagnostic Threshold Values of Cerebral Perfusion Measured with Computed Tomography for Delayed Cerebral Ischemia after Aneurysmal Subarachnoid Hemorrhage. Stroke 2010, 41, 1927–1932. [Google Scholar] [CrossRef] [Green Version]
- Mir, D.I.A.; Gupta, A.; Dunning, A.; Puchi, L.; Robinson, C.L.; Epstein, H.A.; Sanelli, P.C. CT perfusion for detection of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. AJNR Am. J. Neuroradiol. 2014, 35, 866–871. [Google Scholar] [CrossRef] [Green Version]
- Malinova, V.; Dolatowski, K.; Schramm, P.; Moerer, O.; Rohde, V.; Mielke, D. Early whole-brain CT perfusion for detection of patients at risk for delayed cerebral ischemia after sub-arachnoid hemorrhage. J. Neurosurg. 2016, 125, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Lin, F.; Chen, Y.; Lu, J.; Han, H.; Yan, D.; Li, R.; Yang, J.; Li, Z.; Zhang, H.; et al. In-hospital complication-related risk factors for discharge and 90-day outcomes in patients with aneurysmal subarachnoid hemorrhage after surgical clipping and endovascular coiling: A propensity score-matched analysis. J. Neurosurg. 2021, 137, 381–392. [Google Scholar] [CrossRef]
- Ahn, S.-H.; Savarraj, J.P.; Pervez, M.; Jones, W.; Park, J.; Jeon, S.-B.; Kwon, S.U.; Chang, T.R.; Lee, K.; Kim, D.H.; et al. The Subarachnoid Hemorrhage Early Brain Edema Score Predicts Delayed Cerebral Ischemia and Clinical Outcomes. Neurosurgery 2017, 83, 137–145. [Google Scholar] [CrossRef]
- Tallarita, T.; Sorenson, T.J.; Rinaldo, L.; Oderich, G.S.; Bower, T.C.; Meyer, F.B.; Lanzino, G. Management of carotid artery stenosis in patients with coexistent unruptured intracranial aneurysms. J. Neurosurg. 2019, 132, 94–97. [Google Scholar] [CrossRef]
- Samuels, O.B.; Joseph, G.J.; Lynn, M.J.; Smith, H.A.; Chimowitz, M.I. A Standardized Method for Measuring Intracranial Arterial Stenosis. AJNR Am. J. Neuroradiol. 2000, 21, 643–646. [Google Scholar]
- Barnett, H.J.; Taylor, D.W.; Eliasziw, M.; Fox, A.J.; Ferguson, G.G.; Haynes, R.B.; Rankin, R.N.; Clagett, G.P.; Hachinski, V.C.; Sackett, D.L.; et al. Benefit of Carotid Endarterectomy in Patients with Symptomatic Moderate or Severe Stenosis. N. Engl. J. Med. 1998, 339, 1415–1425. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Jaja, B.N.R.; Saposnik, G.; Lingsma, H.F.; Macdonald, E.; Thorpe, K.; Mamdani, M.; Steyerberg, E.W.; Molyneux, A.; Manoel, A.L.D.O.; Schatlo, B.; et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: The SAHIT multinational cohort study. BMJ 2018, 360, j5745. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Lin, F.; Chen, Y.; Lu, J.; Han, H.; Ma, L.; Zhao, Y.; Yan, D.; Li, R.; Yang, J.; et al. A 90-Day Prognostic Model Based on the Early Brain Injury Indicators after Aneurysmal Subarachnoid Hem-orrhage: The TAPS Score. Transl. Stroke Res. 2022, 14, 200–210. [Google Scholar] [CrossRef]
- Flusty, B.; de Havenon, A.; Prabhakaran, S.; Liebeskind, D.S.; Yaghi, S. Intracranial Atherosclerosis Treatment: Past, Present, and Future. Stroke 2020, 51, e49–e53. [Google Scholar] [CrossRef] [Green Version]
- Borkon, M.J.; Hoang, H.; Rockman, C.; Mussa, F.; Cayne, N.S.; Riles, T.; Jafar, J.J.; Veith, F.J.; Adelman, M.A.; Maldonado, T.S. Concomitant Unruptured Intracranial Aneurysms and Carotid Artery Stenosis: An Institutional Review of Patients Undergoing Carotid Revascularization. Ann. Vasc. Surg. 2013, 28, 102–107. [Google Scholar] [CrossRef]
- Harrigan, M.R.; Magnano, C.R.; Guterman, L.R.; Hopkins, L.N. Computed Tomographic Perfusion in the Management of Aneurysmal Subarachnoid Hemorrhage: New Application of an Existent Technique. Neurosurgery 2005, 56, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Conzen, C.; Becker, K.; Albanna, W.; Weiss, M.; Bach, A.; Lushina, N.; Steimers, A.; Pinkernell, S.; Clusmann, H.; Lindauer, U.; et al. The Acute Phase of Experimental Subarachnoid Hemorrhage: Intracranial Pressure Dynamics and Their Effect on Cerebral Blood Flow and Autoregulation. Transl. Stroke Res. 2018, 10, 566–582. [Google Scholar] [CrossRef] [PubMed]
- Schubert, G.A.; Seiz, M.; Hegewald, A.A.; Manville, J.; Thomé, C. Hypoperfusion in the Acute Phase of Subarachnoid Hemorrhage. Acta Neurochir. Suppl. 2011, 110 Pt 1, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, M.; Liu, Z.; Wang, Y.; Xiong, K. Molecular mechanisms of neuronal death in brain injury after subarachnoid hemorrhage. Front. Cell. Neurosci. 2022, 16, 1025708. [Google Scholar] [CrossRef] [PubMed]
- Laiwalla, A.N.; Ooi, Y.C.; Van De Wiele, B.; Ziv, K.; Brown, A.; Liou, R.; Saver, J.L.; Gonzalez, N.R. Rigorous anaesthesia management protocol for patients with intracranial arterial stenosis: A prospective controlled-cohort study. BMJ Open 2016, 6, e009727. [Google Scholar] [CrossRef] [Green Version]
- McKetton, L.; Venkatraghavan, L.; Poublanc, J.; Sobczyk, O.; Crawley, A.P.; Rosen, C.; Silver, F.L.; Duffin, J.; Fisher, J.A.; Mikulis, D.J. Importance of Collateralization in Patients with Large Artery Intracranial Occlusive Disease: Long-Term Longitudinal Assessment of Cerebral Hemodynamic Function. Front. Neurol. 2018, 9, 226. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Chen, Y.; Li, R.; Lin, F.; Lu, J.; Chen, X.; Wang, S. The value of early CT perfusion parameters for predicting delayed cerebral ischemia after aneurysmal sub-arachnoid hemorrhage: A systematic review and meta-analysis. Neurosurg. Rev. 2022, 45, 2517–2531. [Google Scholar] [CrossRef]
- Amukotuwa, S.; Wu, A.; Zhou, K.; Page, I.; Brotchie, P.; Bammer, R. Time-to-Maximum of the Tissue Residue Function Improves Diagnostic Performance for Detecting Distal Vessel Occlusions on CT Angiography. Am. J. Neuroradiol. 2021, 42, 65–72. [Google Scholar] [CrossRef]
- Cereda, C.W.; Bianco, G.; Mlynash, M.; Yuen, N.; Qureshi, A.Y.; Hinduja, A.; Dehkharghani, S.; Goldman-Yassen, A.E.; Hsieh, K.L.; Giurgiutiu, D.; et al. Perfusion Imaging Predicts Favorable Outcomes after Basilar Artery Thrombectomy. Ann. Neurol. 2022, 91, 23–32. [Google Scholar] [CrossRef]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Pavia, J.M.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85 Pt 1, 6–27. [Google Scholar] [CrossRef]
- Schwartz, J. Calculating percent stenosis. AJNR Am. J. Neuroradiol. 2001, 22, 227. [Google Scholar]



{kind=link}
{kind=link}
| Patients | Value |
|---|---|
| Total no. | 192 |
| Average age in years (SD) | 59.3 (10.8) |
| Sex, Female/Male | 1:1.34 |
| Neurological score | |
| H-H grade 4–5 | 35 (18.2%) |
| WFNS grade 4–5 | 59 (30.7%) |
| mFS grade 3–4 | 130 (67.7%) |
| Graeb score 5–12 | 21 (10.9%) |
| SEBES score 3–4 | 79 (41.1%) |
| Degree of stenosis | |
| >99% | 20 (10.4%) |
| 70–99% | 33 (17.2%) |
| <70% | 139 (72.4%) |
| Average dome size in mm (SD) | 6.2 (3.9) |
| Location | |
| ICA | 82 (42.7%) |
| ACoA | 36 (18.8%) |
| MCA | 38 (19.8%) |
| ACA | 11 (5.7%) |
| PICA | 4 (2.1%) |
| Treatment | |
| Clipping | 102 (53.1%) |
| Coiling | 90 (46.9%) |
| Periprocedural complication | |
| DCI | 67 (34.9%) |
| Mortality | 12 (6.3%) |
| Characteristics | mRS Score ≤ 2 | mRS Score > 2 | p Value | DCI | Non-DCI | p Value |
|---|---|---|---|---|---|---|
| Sample size | 150 (78.1%) | 42 (21.9%) | 67 (34.9) | 125 (65.1) | ||
| Age, years, mean ± SD | 58.29 ± 10.33 | 63.12 ± 11.57 | 0.010 | 58.27 ± 10.85 | 59.92 ± 10.73 | 0.313 |
| Female sex | 87 (58.0) | 23 (54.8) | 0.843 | 42 (62.7) | 68 (54.5) | 0.269 |
| Prior medical history | ||||||
| Smoking | 18 (12.0) | 6 (14.3) | 0.922 | 13 (19.4) | 16 (12.8) | 0.223 |
| Drinking | 8 (5.3) | 5 (11.9) | 0.196 | 7 (10.4) | 8 (6.4) | 0.319 |
| Hypertension | 82 (54.7) | 31 (73.8) | 0.040 | 45 (67.2) | 68 (54.4) | 0.087 |
| Diabetes mellitus | 13 (8.7) | 3 (7.1) | 1.000 | 4 (6.0) | 12 (9.6) | 0.386 |
| Prior infarction | 14 (9.3) | 1 (2.4) | 0.913 | 3 (4.5) | 12 (9.6) | 0.207 |
| Aneurysm characteristics | ||||||
| Posterior circulation | 20 (13.3) | 7 (16.7) | 0.766 | 9 (13.4) | 18 (14.4) | 0.854 |
| Early seizures | 5 (3.3) | 2 (4.8) | 1.000 | 3 (4.5) | 4 (3.2) | 0.653 |
| Early loss of consciousness | 36 (24.0) | 25 (59.5) | <0.001 | 28 (41.8) | 33 (26.4) | 0.029 |
| Acute hydrocephalus | 67 (44.7) | 16 (38.1) | 0.559 | 30 (44.8) | 53 (42.4) | 0.751 |
| Parent artery stenosis | 67 (44.7) | 21 (50.0) | 0.661 | 35 (52.2) | 53 (42.4) | 0.192 |
| Neurological score | ||||||
| H-H grade 4–5 | 15 (10.0) | 20 (47.6) | <0.001 | 15 (22.4) | 20 (16.0) | 0.274 |
| WFNS grade 4–5 | 32 (21.3) | 27 (64.3) | <0.001 | 27 (40.3) | 32 (25.6) | 0.035 |
| mFS grade 3–4 | 96 (64.0) | 34 (81.0) | 0.059 | 50 (74.6) | 80 (64.0) | 0.133 |
| Graeb score 5–12 | 13 (8.7) | 8 (19.0) | 0.104 | 6 (9.0) | 15 (12.0) | 0.519 |
| SEBES score 3–4 | 60 (40.0) | 19 (45.2) | 0.665 | 29 (43.3) | 50 (40.0) | 0.659 |
| CTP parameters, median (IQR) | ||||||
| Tmax > 8.0 s volume | 0.0 (0.0–0.0) | 0.0 (0.0–14.0) | 0.016 | 0.0 (0.0–6.0) | 0.0 (0.0–3.5) | <0.001 |
| Tmax > 6.0 s volume | 0.0 (0.0–3.0) | 4.0 (0.0–43.0) | <0.001 | 0.0 (0.0–16.0) | 0.0 (0.0–6.5) | <0.001 |
| Tmax > 4.0 s volume | 12.0 (0.0–73.3) | 123.0 (27.5–309.0) | <0.001 | 35 (0.0–151.0) | 17 (0.0–121.5) | <0.001 |
| rCBF < 38% volume | 0.0 (0.0–0.0) | 0.0 (0.0–20.8) | <0.001 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | <0.001 |
| Treatment modality | 0.010 | 0.002 | ||||
| Surgical clipping | 71 (47.3) | 30 (71.4) | 46 (68.7) | 56 (44.8) | ||
| Endovascular coiling | 79 (52.7) | 12 (28.6) | 21 (31.3) | 69 (55.2) | ||
| Degree of stenosis | 0.322 | 0.872 | ||||
| Mild (<70%) | 111 (74.0) | 28 (66.7) | 48 (71.6) | 91 (72.8) | ||
| Moderate (70–99%) | 26 (17.3) | 7 (16.7) | 11 (16.4) | 22 (17.6) | ||
| Severe (>99%) | 13 (8.7) | 7 (16.7) | 8 (11.9) | 12 (9.6) |
| Tmax > 8.0 s Volume > 0 mL | Tmax > 6.0 s Volume > 0 mL | Tmax > 4.0 s Volume > 0 mL | Tmax > 4.0 s Volume > 25 mL | rCBF < 38% Volume > 0 mL | |
|---|---|---|---|---|---|
| 3-month mRS | |||||
| Univariable analysis | 2.82 (1.37–5.78) | 3.13 (1.54–6.35) | 4.67 (1.73–12.56) a | 3.88 (1.88–8.02) | 3.75 (1.76–8.03) |
| Multivariable analysis 1 † | 0.76 (0.27–2.10) | 0.85 (0.31–2.39) | 3.46 (1.10–10.89) a | 1.59 (0.62–4.07) | 1.04 (0.36–3.07) |
| Multivariable analysis 2 ‡ | 0.76 (0.25–2.31) | 0.87 (0.28–2.74) | 3.90 (1.11–13.73) a | 1.29 (0.43–3.88) | 0.67 (0.19–2.34) |
| Perioperative DCI | |||||
| Univariable analysis | 1.33 (0.69–2.55) | 1.47 (0.78–2.76) | 1.23 (0.65–2.34) | 2.21 (1.21–4.06) | 1.32 (0.64–2.70) |
| Multivariable analysis 1 § | 0.76 (0.36–1.62) | 0.82 (0.39–1.73) | 0.83 (0.41–1.67) | 1.70 (0.86–3.38) | 0.66 (0.28–1.53) |
| Multivariable analysis 2 ¶ | 0.67 (0.27–1.66) | 0.84 (0.34–2.08) | 1.00 (0.43–2.31) | 2.07 (0.87–4.90) | 0.53 (0.19–1.46) |
| Model | AUC (95%CI) | p Value | cNRI (95%CI) | p Value | IDI (95%CI) | p Value |
|---|---|---|---|---|---|---|
| SAHIT | 0.821 (0.754–0.888) | Reference | Reference | Reference | Reference | Reference |
| SAHIT + CTP | 0.831 (0.763–0.899) | 0.591 | 0.535 (0.284–0.786) | <0.001 | 0.041 (0.018–0.064) | <0.001 |
| TAPS | 0.769 (0.689–0.848) | Reference | Reference | Reference | Reference | Reference |
| TAPS + CTP | 0.790 (0.709–0.871) | 0.379 | 0.541 (0.277–0.805) | <0.001 | 0.042 (0.021–0.062) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Han, H.; Chen, Y.; Lin, F.; Li, R.; Lu, J.; Li, R.; Li, Z.; Shi, G.; Wang, S.; et al. Application of Quantitative Computed Tomographic Perfusion in the Prognostic Assessment of Patients with Aneurysmal Subarachnoid Hemorrhage Coexistent Intracranial Atherosclerotic Stenosis. Brain Sci. 2023, 13, 625. https://doi.org/10.3390/brainsci13040625
Yang J, Han H, Chen Y, Lin F, Li R, Lu J, Li R, Li Z, Shi G, Wang S, et al. Application of Quantitative Computed Tomographic Perfusion in the Prognostic Assessment of Patients with Aneurysmal Subarachnoid Hemorrhage Coexistent Intracranial Atherosclerotic Stenosis. Brain Sciences. 2023; 13(4):625. https://doi.org/10.3390/brainsci13040625
Chicago/Turabian StyleYang, Jun, Heze Han, Yu Chen, Fa Lin, Runting Li, JunLin Lu, Ruinan Li, Zhipeng Li, Guangzhi Shi, Shuo Wang, and et al. 2023. "Application of Quantitative Computed Tomographic Perfusion in the Prognostic Assessment of Patients with Aneurysmal Subarachnoid Hemorrhage Coexistent Intracranial Atherosclerotic Stenosis" Brain Sciences 13, no. 4: 625. https://doi.org/10.3390/brainsci13040625
APA StyleYang, J., Han, H., Chen, Y., Lin, F., Li, R., Lu, J., Li, R., Li, Z., Shi, G., Wang, S., Zhao, Y., Chen, X., & Zhao, J. (2023). Application of Quantitative Computed Tomographic Perfusion in the Prognostic Assessment of Patients with Aneurysmal Subarachnoid Hemorrhage Coexistent Intracranial Atherosclerotic Stenosis. Brain Sciences, 13(4), 625. https://doi.org/10.3390/brainsci13040625