
Is Balance Training Using Biofeedback Effective in the Prophylaxis of Falls in Women over the Age of 65?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Report on Ageing and Health; World Health Organization: Geneva, Switzerland. 2015. Available online: http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf (accessed on 4 December 2015).
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults—Present status and future implications. Lancet 2014, 385, 563–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oo, W.M.; Little, C.; Duong, V.; Hunter, D.J. The Development of Disease-Modifying Therapies for Osteoarthritis (DMOADs): The Evidence to Date. Drug Des. Dev. Ther. 2021, 15, 2921–2945. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Golightly, Y. State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 276–283. [Google Scholar] [CrossRef]
- Harris, E.C.; Coggon, D. HIP osteoarthritis and work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 462–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzat, A.M.; Li, L.C. Occupational Physical Loading Tasks and Knee Osteoarthritis: A Review of the Evidence. Physiother. Can. 2014, 66, 91–107. [Google Scholar] [CrossRef] [Green Version]
- MBerková, M.; Berka, Z. Falls: A significant cause of morbidity and mortality in elderly people. Vnitr. Lek. 2018, 64, 1076–1083. [Google Scholar] [CrossRef]
- Sharif, S.I.; Al-Harbi, A.B.; Al-Shihabi, A.M.; Al-Daour, D.S.; Sharif, R.S. Falls in the elderly: Assessment of prevalence and risk factors. Pharm. Pract. 2018, 16, 1206. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Tiedemann, A. Physiotherapy in the prevention of falls in older people. J. Physiother. 2015, 61, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Medical Advisory Secretariat. Prevention of falls and fall-related injuries in community-dwelling seniors: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2008, 8, 1–78. [Google Scholar]
- Alghwiri, A.A.; Whitney, S.L. Balance and falls. In Geriatric Physical Therapy, 3rd ed.; Guccione, A.A., Wong, R.A., Avers, D., Eds.; Elsevier Mosby: St. Louis, MO, USA, 2012; pp. 389–419. [Google Scholar]
- Chen, T.; Yoshida, Y. Effects of Power on Balance and Fall Prevention in Aging and Older Adults. Top. Geriatr. Rehabil. 2021, 37, 7–11. [Google Scholar] [CrossRef]
- Guirguis-Blake, J.M.; Michael, Y.L.; Perdue, L.A.; Coppola, E.L.; Beil, T.L. Interventions to Prevent Falls in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 1705–1716. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Eichberg, S.; Marston, H.R.; Ejupi, A.; Rosario, H.; Kroll, M.; Drobics, M.; Annegarn, J.; Wieching, R.; Lord, S.R.; et al. ICT-based system to predict and prevent falls (iStoppFalls): Study protocol for an international multicenter randomized controlled trial. BMC Geriatrs 2014, 14, 91. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Maranesi, E.; Riccardi, G.R.; Donna, V.D.; Pelliccioni, P.; Luzi, R.; Lattanzio, F.; Pelliccioni, G. Non-Immersive Virtual Reality for Rehabilitation of the Older People: A Systematic Review into Efficacy and Effectiveness. J. Clin. Med. 2019, 8, 1882. [Google Scholar] [CrossRef] [Green Version]
- Czerwosz, L.; Mraz, M.; Mraz, M. Posturography as a rehabilitation, diagnostic, or imbalance assessment tool. Biophilia 2011, 1, 4_23. [Google Scholar] [CrossRef] [Green Version]
- Maranesi, E.; Casoni, E.; Baldoni, R.; Barboni, I.; Rinaldi, N.; Tramontana, B.; Amabili, G.; Benadduci, M.; Barbarossa, F.; Luzi, R.; et al. The Effect of Non-Immersive Virtual Reality Exergames versus Traditional Physiotherapy in Parkinson’s Disease Older Patients: Preliminary Results from a Randomized-Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 14818. [Google Scholar] [CrossRef]
- Sokołowska, B.; Sadura-Sieklucka, T.; Czerwosz, L.; Hallay-Suszek, M.; Lesyng, B.; Księżopolska-Orłowska, K. Estimation of Posturographic Trajectory using k-Nearest Neighbors Classifier in Patients with Rheumatoid Arthritis and Osteoarthritis. Adv. Exp. Med. Biol. 2018, 39, 85–95. [Google Scholar] [CrossRef]
- Czerwosz, L.; Mraz, M.; Curzytek, M.; Blaszczyk, J. Application of Virtual Reality in Postural Stability Rehabilitation. In Proceedings of the 2009 Virtual Rehabilitation International Conference, Haifa, Israel, 29 June–2 July 2009. [Google Scholar] [CrossRef]
- Litvinenkova, V.; Hlavacka, F. The visual feed-back gain influence upon the regulation of the upright posture in man. Agressologie 1973, 14, 95–99. [Google Scholar]
- Pinsault, N.; Vuillerme, N. The effects of scale display of visual feedback on postural control during quiet standing in healthy elderly subjects. Arch. Phys. Med. Rehabil. 2008, 89, 1772–1774. [Google Scholar] [CrossRef]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C. Effective exercise for the prevention of falls: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef]
- Urabe, Y.; Fukui, K.; Harada, K.; Tashiro, T.; Komiya, M.; Maeda, N. The Application of Balance Exercise Using Virtual Reality for Rehabilitation. Healthcare 2022, 10, 680. [Google Scholar] [CrossRef]
- Liu, M.; Zhou, K.; Chen, Y.; Zhou, L.; Bao, D.; Zhou, J. Is Virtual Reality Training More Effective Than Traditional Physical Training on Balance and Functional Mobility in Healthy Older Adults? A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2022, 16, 843481. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, H.; Jehu, D.A.; Daneshjoo, A.; Shakoor, E.; Razeghi, M.; Amani, A.; Hakim, M.N.; Yusof, A. Effects of 8 Weeks of Balance Training, Virtual Reality Training, and Combined Exercise on Lower Limb Muscle Strength, Balance, and Functional Mobility Among Older Men: A Randomized Controlled Trial. Sports Health 2021, 13, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Babadi, S.Y.; Daneshmandi, H. Effects of virtual reality versus conventional balance training on balance of the elderly. Exp. Gerontol. 2021, 153, 111498. [Google Scholar] [CrossRef] [PubMed]
- Komar, M.; Czerwosz, L. Physical Aspects of Posturography in Virtual Reality. Acta Phys. Pol. A 2021, 4, 468–472. [Google Scholar] [CrossRef]
- Imaizumi, S.; Asai, T.; Hiromitsu, K.; Imamizu, H. Voluntarily controlled but not merely observed visual feedback affects postural sway. PeerJ 2018, 6, e4643. [Google Scholar] [CrossRef] [Green Version]
- Dault, M.C.; De Haart, M.; Geurts, A.C.; Arts, I.M.; Nienhuis, B. Effects of visual center of pressure feedback on postural control in young and elderly healthy adults and in stroke patients. Hum. Mov. Sci. 2003, 22, 221–236. [Google Scholar] [CrossRef]
- Freitas, S.M.; Duarte, M. Joint coordination in young and older adults during quiet stance: Effect of visual feedback of the centre of pressure. Gait Posture 2012, 35, 83–87. [Google Scholar] [CrossRef]
- Dite, W.; Temple, V.A. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch. Phys. Med. Rehabil. 2002, 83, 1566–1571. [Google Scholar] [CrossRef]
- Whitney, S.L.; Marchetti, G.F.; Morris, L.O.; Sparto, P.J. The reliability and validity of the Four Square Step Test for people with balance deficits secondary to a vestibular disorder. Arch. Phys. Med. Rehabil. 2007, 88, 99–104. [Google Scholar] [CrossRef]
- Ambrens, M.; van Schooten, K.S.; Lung, T.; Clemson, L.; Close, J.C.; Howard, K.; Lord, S.R.; Zijlstra, G.R.; Tiedemann, A.; Valenzuela, T.; et al. Economic evaluation of the e-Health StandingTall balance exercise programme for fall prevention in people aged 70 years and over. Age Ageing 2022, 51, afac130. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| FPT | GT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Examination (N) | I (28) | II (28) | III (27) | Comparison of Examinations | I (29) | II (29) | III (28) | Comparison of Examinations | ||
| I vs. II | II vs. III | I vs. II | II vs. III | |||||||
| Lequesne index | 12.6 ± 3.9 | 10.0 ± 4.2 | 9.5 ± 3.9 | p < 0.02 | ns | 11.6 ± 5.7 | 9.1 ± 6.1 | 9.7 ± 6.9 | ns | ns |
| Laitinen scale | 6.3 ± 1.9 | 4.4 ± 2.3 | 4.0 ± 2.1 | p < 0.004 | ns | 6.1 ± 3.3 | 4.2 ± 3.2 | 4.8 ± 3.8 | p < 0.04 | ns |
| TUG | 7.5 ± 1.6 | 6.9 ± 1.3 | 6.9 ± 1.0 | ns | ns | 7.6 ± 2.1 | 6.8 ± 1.1 | 6.8 ± 1.04 | ns | ns |
| FSST | 10.0 ± 2.0 | 9.1 ± 1.5 | 8.9 ± 1.5 | p < 0.05 | ns | 10.5 ± 3.7 | 8.9 ± 1.9 | 8.8 ± 1.8 | p < 0.05 | ns |
| Number of stumbling | 9.1 ± 11.0 | --- | 2.8 ± 4.2 | p < 0.02 * | --- | 6.9 ± 10.5 | --- | 4.0 ± 6.4 | ns * | --- |
| Number of falls | 0.2 ± 0.6 | --- | 0.0 ± 0.2 | ns * | --- | 0.3 ± 0.8 | --- | 0.1 ± 0.3 | ns * | --- |
| FPT | GT | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Examination (N) | I (36) | II (34) | III (29) | Comparison of Examinations | I (36) | II (32) | III (28) | Comparison of Examinations | Group Comparison FPT vs. GT | ||
| Eyes open EO | I vs. II | II vs. III | I vs. II | II vs. III | |||||||
| R_mm | 3.82 ± 1.24 | 3.32 ± 0.86 | 3.77 ± 1.24 | ns | ns | 4.28 ± 2.01 | 3.93 ± 1.50 | 3.70 ± 0.98 | ns | ns | I, II, III: ns |
| L_cm | 34.4 ± 7.8 | 35.3 ± 7.5 | 34.3 ± 9.2 | ns | ns | 34.6 ± 9.0 | 36.3 ± 8.4 | 34.9 ± 9.3 | ns | ns | I, II, III: ns |
| Eyes closed EC | I vs. II | II vs. III | I vs. II | II vs. III | |||||||
| R_mm | 4.80 ± 1.57 | 4.29 ± 1.40 | 4.56 ± 1.42 | ns | ns | 4.98 ± 2.06 | 4.81 ± 1.58 | 4.21 ± 1.02 | ns | ns | I, II, III: ns |
| L_cm | 45.9 ± 12.4 | 46.7 ± 13.0 | 44.9 ± 14.3 | ns | ns | 47.8 ± 15.5 | 53.6 ± 25.5 | 47.0 ± 14.4 | ns | ns | I, II, III: ns |
| Feedback FB | I vs. II | II vs. III | I vs. II | II vs. III | |||||||
| R_mm | 4.57 ± 2.01 | 2.92 ± 0.66 | 3.12 ± 0.92 | p < 0.00002 | ns | 4.14 ± 1.95 | 4.44 ± 2.35 | 3.56 ± 1.01 | ns | ns | I, III: ns II p < 0.0006 |
| L_cm | 46.7 ± 17.9 | 44.4 ± 9.4 | 41.7 ± 10.1 | ns | ns | 44.6 ± 18.7 | 49.9 ± 25.6 | 42.6 ± 14.60 | ns | ns | I, II, III: ns |
| K% | 80.0 ± 18.2 | 92.1 ± 10.0 | 93.4 ± 7.5 | p < 0.001 | 84.1 ± 16.3 | 81.2 ± 17.8 | 88.8 ± 9.3 | ns | ns | I, III: ns II p < 0.003 | |
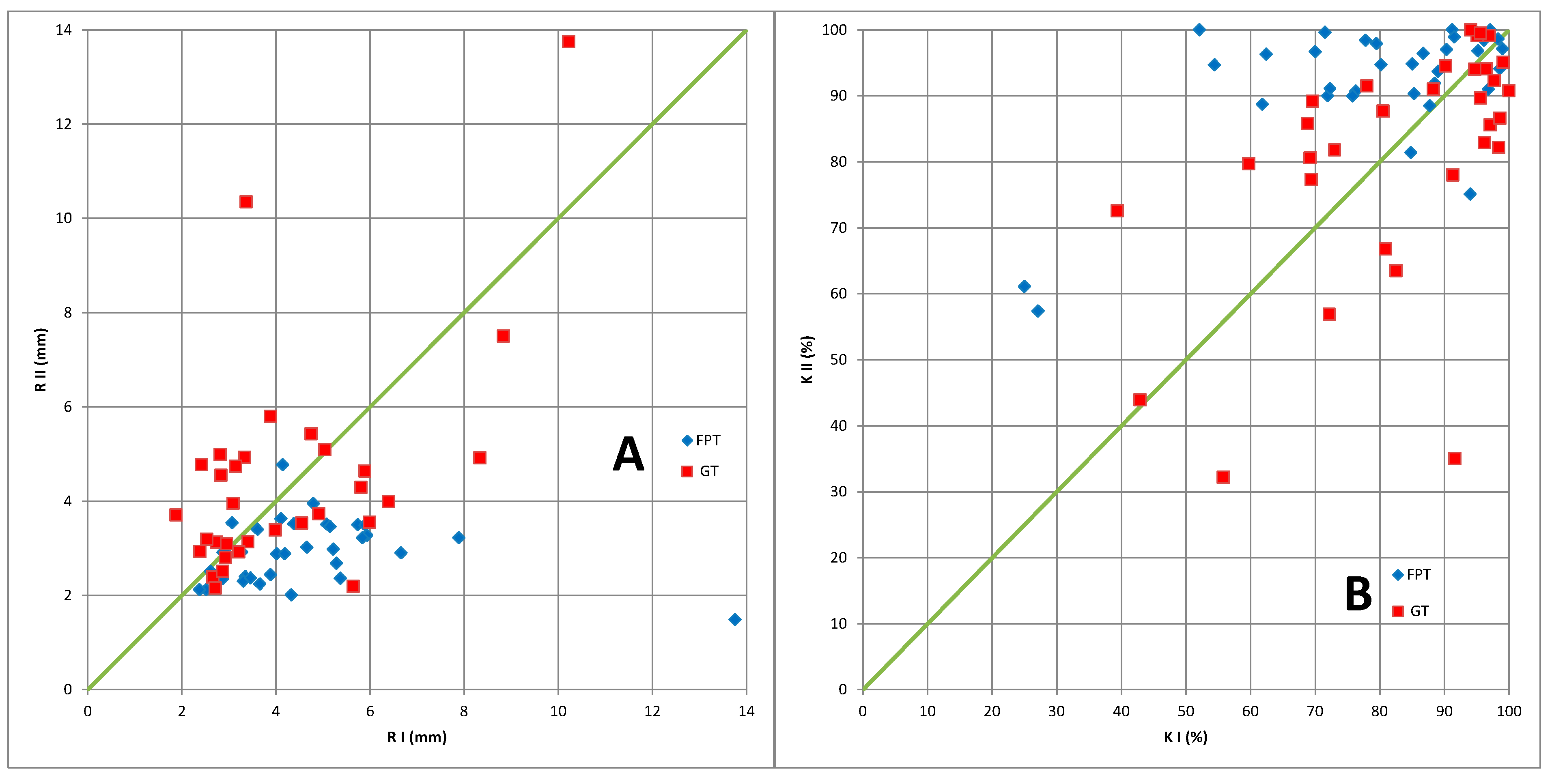
| R | K% | |||||
|---|---|---|---|---|---|---|
| RII < RI | RII > RI | Total | KII < KI | KII > KI | Total | |
| FPT | 30 | 4 | 34 | 5 | 29 | 34 |
| GT | 16 | 16 | 32 | 16 | 16 | 32 |
| Total | 46 | 20 | 66 | 46 | 20 | 66 |
| χ2 = 11.4 p < 0.0007 | χ2 = 9.5 p < 0.002 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadura-Sieklucka, T.; Czerwosz, L.T.; Kądalska, E.; Kożuchowski, M.; Księżopolska-Orłowska, K.; Targowski, T. Is Balance Training Using Biofeedback Effective in the Prophylaxis of Falls in Women over the Age of 65? Brain Sci. 2023, 13, 629. https://doi.org/10.3390/brainsci13040629
Sadura-Sieklucka T, Czerwosz LT, Kądalska E, Kożuchowski M, Księżopolska-Orłowska K, Targowski T. Is Balance Training Using Biofeedback Effective in the Prophylaxis of Falls in Women over the Age of 65? Brain Sciences. 2023; 13(4):629. https://doi.org/10.3390/brainsci13040629
Chicago/Turabian StyleSadura-Sieklucka, Teresa, Leszek Tomasz Czerwosz, Ewa Kądalska, Marcin Kożuchowski, Krystyna Księżopolska-Orłowska, and Tomasz Targowski. 2023. "Is Balance Training Using Biofeedback Effective in the Prophylaxis of Falls in Women over the Age of 65?" Brain Sciences 13, no. 4: 629. https://doi.org/10.3390/brainsci13040629
APA StyleSadura-Sieklucka, T., Czerwosz, L. T., Kądalska, E., Kożuchowski, M., Księżopolska-Orłowska, K., & Targowski, T. (2023). Is Balance Training Using Biofeedback Effective in the Prophylaxis of Falls in Women over the Age of 65? Brain Sciences, 13(4), 629. https://doi.org/10.3390/brainsci13040629