
Patients with Disorders of Consciousness: Are They Nonconscious, Unconscious, or Subconscious? Expanding the Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. (Un)consciousness
- (i)
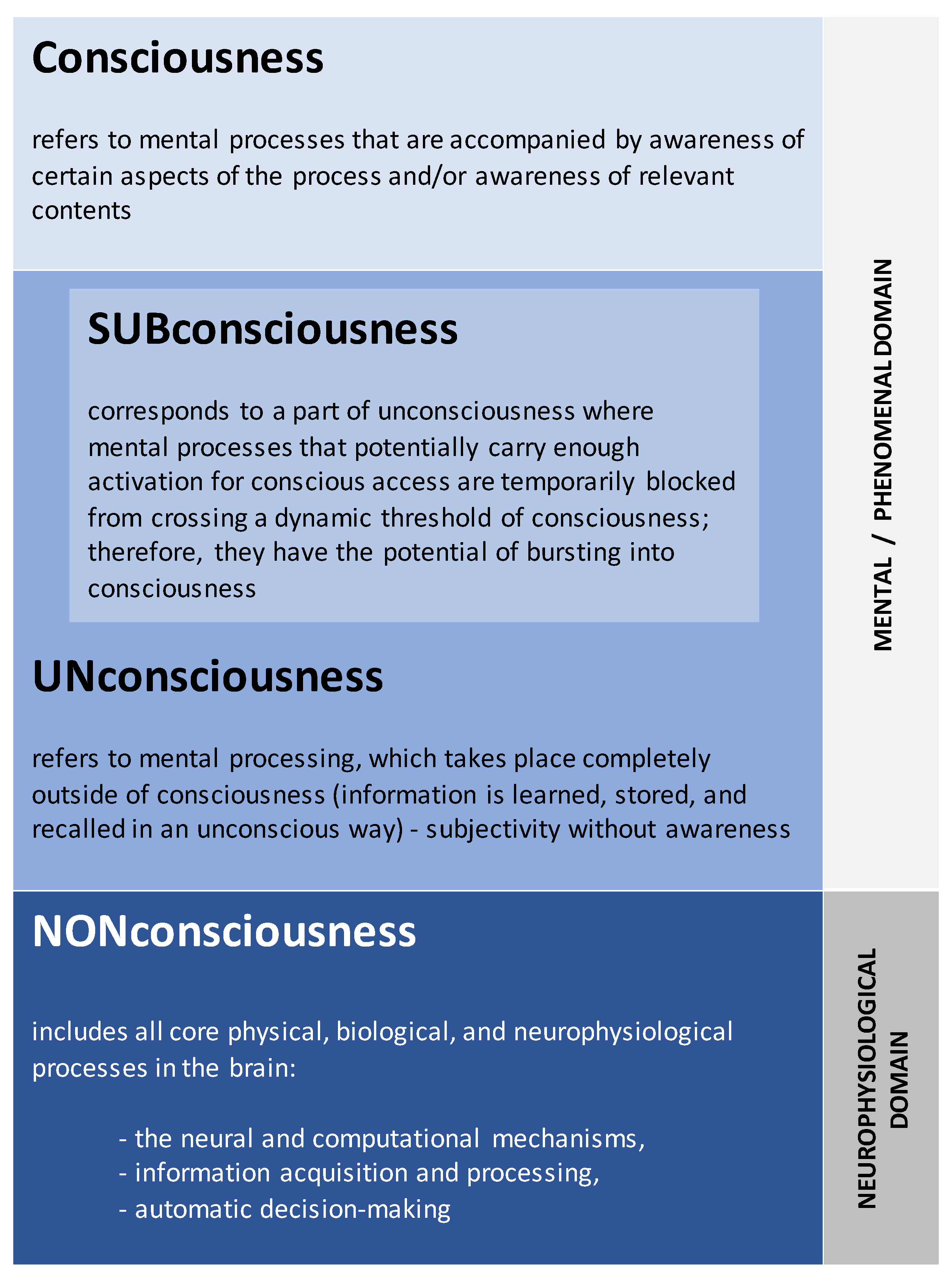
- Nonconsciousness—it does not belong to the mental/experiential/phenomenal domain (Figure 1); it is the myriad of neurophysiological, physical, and biological processes that take place exclusively in the brain (and also in nervous system) outside of the ‘mind-space’ [72]. They are always out of reach, i.e., inaccessible for mentality or phenomenal consciousness, and, hence, referring to unconsciousness as part of the brain’s physical (nonmental) mechanisms makes little conceptual sense [73]. This level of organization can be understood as an autonomous, fast, self-organizing, dynamic system that acquires, processes, stores, and retrieves information to secure its own wellbeing and survival, and the vast majority of life forms ‘possess’ it—though to varying degrees depending on their complexity [74,75,76]. Therefore, crucially, phenomenal consciousness is not necessary for information processing or for adaptation of the organism in general [77]. It is noteworthy that this level encompasses all physiological processes in entirety and is not restricted to any particular localized neural circuit or brain region.
- (ii)
- Unconsciousness—it belongs to the mental/phenomenal domain (Figure 1), although it lacks phenomenal awareness at any given time and therefore is not accessible for voluntary control (it cannot be inhibited, suspended, or terminated [78]) or for rational expression (subjectivity without awareness [79]). However, it can have an impact on various aspects of phenomenal consciousness, including motivation, feelings, goals, behavior, and decision making [36,54,61]. Because it shares sophisticated characteristics with its conscious counterpart [80], it determines significant portions of our personality, skills, preferences, and experience, and it is responsible for important aspects of our ability to adjust and function effectively [81,82]. At the same time, it is not always integrated with the knowledge and beliefs that are held consciously, and it may even sometimes be inconsistent with them, resulting in severe conflicts and occasionally leading to mental health issues [83].
- (iii)
- Subconsciousness—it also does fall under the mental/phenomenal domain (Figure 1) and refers to a part of the mind that is not at any given moment in the focus of attention but which has the potential for bursting into consciousness [84,85]. According to Jung, ”Such material has mostly become unconscious because—in a manner of speaking—there is no room for it in the conscious mind. Some of one’s thoughts lose their emotional energy and become subliminal (that is to say, they no longer receive so much of our conscious attention) because they have come to seem uninteresting or irrelevant, or because there is some reason why we wish to push them out of sight. It is, in fact, normal and necessary for us to ‘forget’ in this fashion, in order to make room in our conscious minds for new impressions and ideas” ([86], p. 37). Normally, attention enables the rapid actualization of subconscious information and its availability for conscious experience at any given temporal period [61,87,88] (for an extensive analysis and discussion, see [85]).

2.1. Neurophenomenology of Non-, Un-, and Sub-Consciousness
2.2. Non-, Un-, and Sub-Consciousness in Patients with DoC
3. Experiential Selfhood
3.1. Neurophenomenology of the Experiential Selfhood
3.2. Non-, Un-, and Sub-Consciousness of Selfhood in Patients with DoC
- (i)
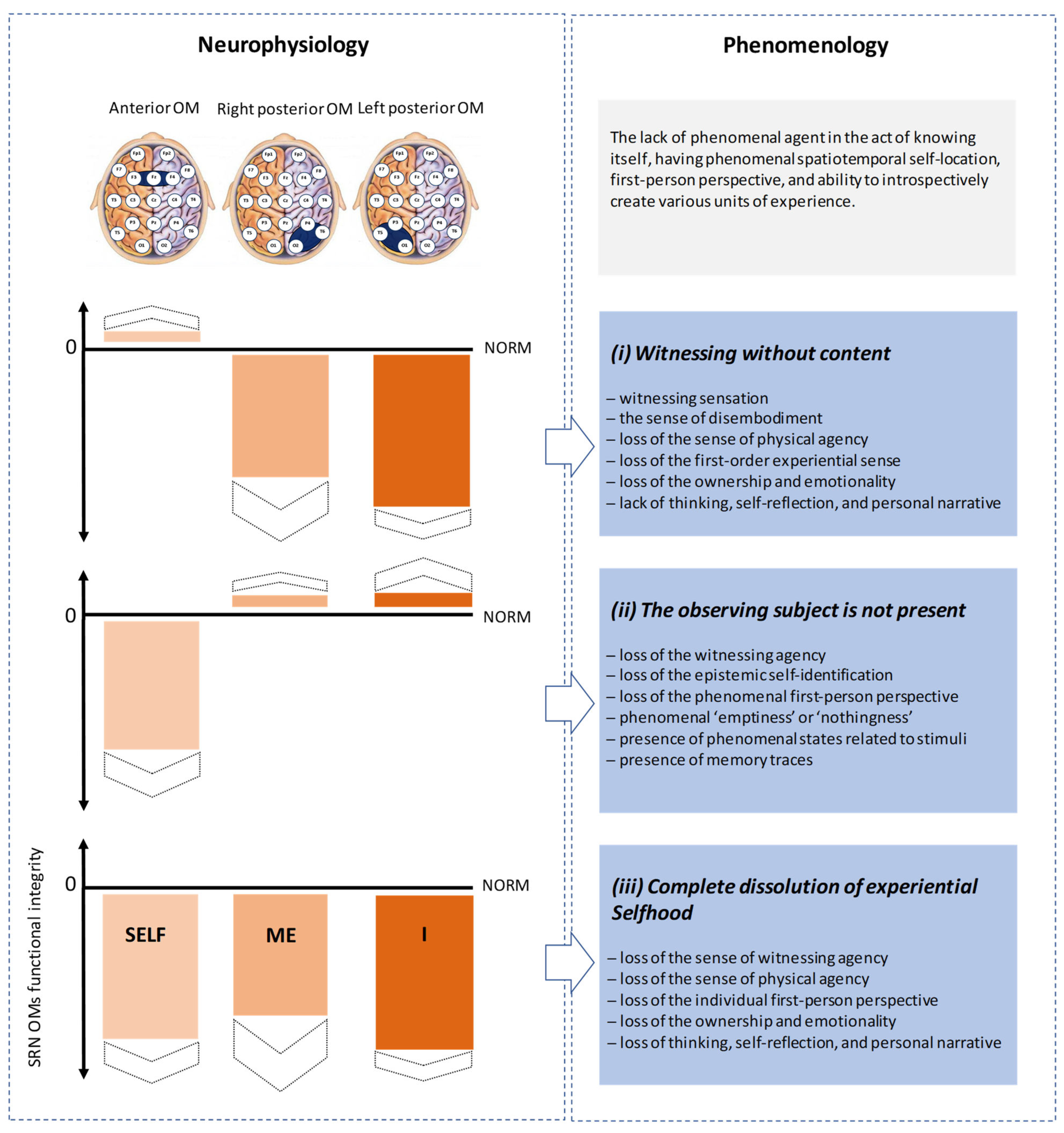
- The presence of normal or increased functional integrity of the Self-module of the brain SRN with simultaneous marked loss in the functional integrity (disintegration) of both Me- and I-modules (Figure 4): In such a state, there will be ”the feeling of being a phenomenal spatio-temporal (and often extensionless) point, that observes and witnesses itself and the world” ([164], p. 264) brought about by the Self module, which will be co-present with a complete loss of all contents stemming from the sense of disembodiment (that is accompanied by loss of the automatic and immediate sense of physical agency, along with a decrease in the first-order experiential sense of ownership and emotionality [113,124,147,183,184]) linked to a disintegrated Me-module and a lack of thinking, self-reflection, and personal narrative [151,185,186,187,188,189,190] associated with the disintegrated I-module. Additionally, given that it has been demonstrated that the phenomenal sense of time emerges as a result of the embodiment sense sustained across time [115,191,192,193], one should anticipate “a profound alteration in time perception (feeling of timelessness)” ([164], p. 265) when the sense of body disappears. We can define this state as a ‘witnessing without content’. According to Metzinger [51,194] and considering the recent empirical evidence [146,164], such ‘witnessing’ sensation is nevertheless “…sufficient for creating a phenomenological centre of gravity and self-identification that is tied to an individual phenomenological first-personal givenness…” ([164], p. 266), though as a ‘thin’ or ‘nonexplicit’ phenomenal experience (see [195,196]). Thus, referring to Levy’s ‘full moral status’ postulate [7], a patient in this state would have personhood with a distinct individual first-person perspective, though there would be a loss of awareness that it is the same person temporally extended across the time. This is because, for that, the intact self-narration and autobiographical memory that are instantiated by the I-module should be present, but they are not due to its (I-module) functional disintegration. Indeed, having access to autobiographical knowledge is essential for a cognitive selfhood because what one did and experienced in the past defines one’s personal identity in the present and actually shapes how one imagines the self in the future [197]. In this respect, given Levy’s definition [7], we may conclude that this state only ensures a partial moral status with a lack of experience of ‘life worth living’ [7,8,198].
- (ii)
- A significant loss of the Self-module’s functional integrity (disintegration) despite the normal levels of the Me- and I-modules’ functional integrity (Figure 4): Such a combination in the OM triad’s functional integrity, when viewed in light of the previous study’s findings regarding the causal relationships between the functional integrity of the three SRN OMs and their corresponding three phenomenological aspects of selfhood [146], could indicate that in this state there is phenomenal ‘emptiness’ or ‘nothingness’ because there is no one to whom the experience is happening, not even the unextended point capable of epistemic self-identification [51,194]. Since the other two brain SRN modules (Me-module and I-module) are functioning normally, there will be phenomenal states related to stimuli originating from both the outside and within the organism and that are also stored as memory traces, but they will not be integrated within the first-person meaningful perspective [146]. Reframing Baars et al. [199] in such a state, there is no blockage of the phenomenal objects of consciousness; rather, the observing subject is not at home. Furthermore, concerning Levy’s ‘full moral status’ postulate [7], it is reasonable to expect that the patient will not have a full moral status while being in this state because, despite the fact that autobiographical memory events are phenomenally present, they are not present to anyone since there is no witnessing agent who would be able to observe them from the phenomenal first-person perspective and to whom the experiences are occurring [146,164].
- (iii)
- A profound loss of the functional integrity (total disintegration) of all three brain SRN models (Self, Me, and I) (Figure 4). Such a state would signify the complete absence of all self-relevant phenomenological content characterized by the ”selfless, objectless and timeless presence” ([164], p. 272), when the self-referential mechanisms of forming the phenomenological events are suspended [51]. This state is generally characterized by a marked lack of individual first-person perspective, sense of witnessing agency, and ownership [146,164]. Additionally, subjective time (a sense of presence, past, or future) does not present anymore [146,164]. We define this state as a ‘complete dissolution of experiential selfhood’. This state could not sustain any phenomenality related to selfhood, and, thus, there is no sense in considering any moral status [7] for patients who are in such a state of lack of ”locus of experience and self-ascription” ([146], p. 23).

4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Young, M.J.; Bodien, Y.G.; Giacino, J.T.; Fins, J.J.; Truog, R.D.; Hochberg, L.R.; Edlow, B.L. The neuroethics of disorders of consciousness: A brief history of evolving ideas. Brain 2021, 144, 3291–3310. [Google Scholar] [CrossRef] [PubMed]
- Levy, N. What difference does consciousness make? Monash Bioeth. Rev. 2009, 28, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Roskies, A. Neuroethics for the new millenium. Neuron 2002, 35, 21–23. [Google Scholar] [CrossRef]
- Illes, J. Neuroethics: Defining the Issues in Theory, Practice, and Policy; Oxford University Press: Oxford, UK, 2006; p. 320. [Google Scholar]
- Salles, A.; Bjaalie, J.G.; Evers, K.; Farisco, M.; Fothergill, B.T.; Guerrero, M.; Maslen, H.; Muller, J.; Prescott, T.; Stahl, B.C.; et al. The human brain project: Responsible brain research for the benefit of society. Neuron 2019, 101, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A. Contemplating on the nature of selfhood in DoC patients: Neurophenomenological perspective. J. Integr. Neurosci. 2023, 22, 23. [Google Scholar] [CrossRef] [PubMed]
- Levy, N.; Savulescu, J. Moral significance of phenomenal consciousness. Prog. Brain Res. 2009, 177, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Peterson, A.; Bayne, T. Post-comatose disorders of consciousness. In The Routledge Handbook of Consciousness; Gennaro, R.J., Ed.; Routledge: Abingdon, VA, USA, 2018; pp. 351–365. [Google Scholar]
- Naccache, L.; Luauté, J.; Silva, S.; Sitt, J.D.; Rohaut, B. Toward a coherent structuration of disorders of consciousness expertise at a country scale: A proposal for France. Rev. Neurol. 2022, 178, 9–20. [Google Scholar] [CrossRef]
- Porcaro, C.; Nemirovsky, I.E.; Riganello, F.; Mansour, Z.; Cerasa, A.; Tonin, P.; Stojanoski, B.; Soddu, A. Diagnostic developments in differentiating unresponsive wakefulness syndrome and the minimally conscious state. Front. Neurol. 2022, 12, 778951. [Google Scholar] [CrossRef]
- Jennett, B.; Plum, F. Persistent vegetative state after brain damage. A syndrome in search of a name. Lancet 1972, 1, 734–737. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef]
- Multi-Society Task Force on PVS. Medical aspects of the persistent vegetative state (1). N. Engl. J. Med. 1994, 330, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Nakase-Richardson, R.; Yablon, S.A.; Sherer, M.; Nick, T.G.; Evans, C.C. Emergence from minimally conscious state: Insights from evaluation of posttraumatic confusion. Neurology 2009, 73, 1120–1126. [Google Scholar] [CrossRef]
- Stuss, D.T.; Binns, M.A.; Carruth, F.G.; Levine, B.; Brandys, C.E.; Moulton, R.J.; Snow, W.G.; Schwartz, M.L. The acute period of recovery from traumatic brain injury: Posttraumatic amnesia or posttraumatic confusional state? J. Neurosurg. 1999, 90, 635–643. [Google Scholar] [CrossRef]
- Bodien, Y.G.; Martens, G.; Ostrow, J.; Sheau, K.; Giacino, J.T. Cognitive impairment, clinical symptoms and functional disability in patients emerging from the minimally conscious state. NeuroRehabilitation 2020, 46, 65–74. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Bagnato, S.; Boccagni, C.; Galardi, G. Toward operational architectonics of consciousness: Basic evidence from patients with severe cerebral injuries. Cogn. Process. 2012, 13, 111–131. [Google Scholar] [CrossRef]
- Bennett, M.R.; Hacker, P.M.S. Philosophical Foundations of Neuroscience; Blackwell Publishing: Malden, MA, USA, 2003; p. 480. [Google Scholar]
- Young, M.J. “Consciousness” as a vague predicate. AJOB Neurosci. 2017, 8, 157–159. [Google Scholar] [CrossRef]
- Fins, J.J. Rights Come to Mind: Brain Injury, Ethics, and the Struggle for Consciousness; Cambridge University Press: Cambridge, UK, 2015; p. 379. [Google Scholar]
- Spill, G.R.; Vente, T.; Frader, J.; Smith, S.; Giacino, J.; Zafonte, R.; Coppard, B.; Jensen, G.; Mukherjee, D. Futility in rehabilitation. PM&R 2019, 11, 420–428. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Neves, C.F.H. Natural world physical, brain operational, and mind phenomenal space–time. Phys. Life Rev. 2010, 7, 195–249. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Neves, C.F.H. Consciousness as a phenomenon in the operational architectonics of brain organization: Criticality and self-organization considerations. Chaos Soliton. Fract. 2013, 55, 13–31. [Google Scholar] [CrossRef]
- Baars, B.J. A Cognitive Theory of Consciousness; Cambridge University Press: Cambridge, UK, 1988; p. 416. [Google Scholar]
- Edelman, G.M.; Tononi, G. A Universe of Consciousness: How Matter Becomes Imagination; Basic Books: New York, NY, USA, 2000; p. 274. [Google Scholar]
- Revonsuo, A. Inner Presence: Consciousness as a Biological Phenomenon; MIT Press: Cambridge, MA, USA, 2006. [Google Scholar]
- McFadden, J. The electromagnetic will. NeuroSci 2021, 2, 291–304. [Google Scholar] [CrossRef]
- Hales, C.G.; Ericson, M. Electromagnetism’s bridge across the explanatory gap: How a neuroscience/physics collaboration delivers explanation into all theories of consciousness. Front. Hum. Neurosci. 2022, 16, 836046. [Google Scholar] [CrossRef] [PubMed]
- Basar, E. Brain–Body–Mind in the Nebulous Cartesian System: A Holistic Approach by Oscillations; Springer: New York, NY, USA, 2011; p. 523. [Google Scholar]
- Freeman, W.J. Consciousness, intentionality and causality. J. Conscious. Stud. 1999, 6, 143–172. [Google Scholar]
- Davis, J.J.; Gillett, G.; Kozma, R. Revisiting Brentano on consciousness: A striking correlation with ECoG findings about the action-perception cycle and the emergence of knowledge and meaning. Mind Matter. 2015, 13, 45–69. [Google Scholar]
- Velmans, M. Understanding Consciousness, 2nd ed.; Routledge: London, UK, 2009; p. 406. [Google Scholar]
- Kozyreva, A. Non-representational approaches to the unconscious in the phenomenology of Husserl and Merleau-Ponty. Phenom. Cogn. Sci. 2018, 17, 199–224. [Google Scholar] [CrossRef]
- Dijksterhuis, A.; Aarts, H. Goals, Attention, and (Un)Consciousness. Annu. Rev. Psychol. 2010, 61, 467–490. [Google Scholar] [CrossRef]
- Sevenius Nilsen, A.; Juel, B.E.; Thürer, B.; Aamodt, A.; Storm, J.F. Are we really unconscious in “unconscious” states? Common assumptions revisited. Front. Hum. Neurosci. 2022, 16, 987051. [Google Scholar] [CrossRef]
- Husserl, E. Ideas Pertaining to a Pure Phenomenology and to a Phenomenological Philosophy. In Second Book: Studies in the Phenomenology of Constitution; Rojcewicz, R., Schuwer, A., Trans, Eds.; Kluwer Academic Publishers: Dordrecht, The Netherlands, 1989. [Google Scholar]
- Alcaraz-Sánchez, A.; Demšar, E.; Campillo-Ferrer, T.; Torres-Platas, S.G. Nothingness is all there is: An exploration of objectless awareness during sleep. Front. Psychol. 2022, 13, 901031. [Google Scholar] [CrossRef]
- Winter, U.; Levan, P.; Borghardt, T.L.; Akin, B.; Wittmann, M. Content-free awareness: EEG-FcMRI correlates of consciousness as such in an expert meditator. Front. Psychol. 2020, 10, 3064. [Google Scholar] [CrossRef]
- Fuchs, T. Body memory and the unconscious. In Founding Psychoanalysis Phenomenologically; Lohmar, D., Brudzinska, J., Eds.; Springer: Dordrecht, The Netherlands, 2012; Volume 199, pp. 69–82. [Google Scholar]
- Bernet, R. Unconscious consciousness in Husserl and Freud. Phenomenol. Cogn. Sci. 2002, 1, 327–351. [Google Scholar] [CrossRef]
- Brudzinska, J. Die phänomenologische Erfahrung und die Frage nach dem Unbewussten. überlegungen im Anschluss an Husserl und Freud. In Interdisziplinäre Perspektiven der Phänomenologie; Lohmar, D., Fonfara, D., Eds.; Springer: Dordrecht, The Netherlands, 2006; Volume 177, pp. 54–71. [Google Scholar]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Neves, C.F.H.; Kallio-Tamminen, T. Brain-mind operational architectonics: At the boundary between quantum physics and Eastern metaphysics. Phys. Life Rev. 2019, 31, 122–133. [Google Scholar] [CrossRef]
- Chadha, M. Meditation and unity of consciousness: A perspective from Buddhist epistemology. Phenomenol. Cogn. Sci. 2015, 14, 111–127. [Google Scholar] [CrossRef]
- Waldron, W.S. The Buddhist Unconscious: The Alaya-Vijnana in the Context of Indian Buddhist Thought; Routledge: London, UK, 2003; p. 288. [Google Scholar]
- Prasad, H.S. Dreamless sleep and soul: A controversy between Vedanta and Buddhism. Asian Philos. 2000, 10, 61–73. [Google Scholar] [CrossRef]
- Norbu, N. Dream Yoga and The Practice of Natural Light, revised ed.; Snow Lion Publications: Ithaca, NY, USA, 2002; p. 167. [Google Scholar]
- Thompson, E. Waking, Dreaming, Being: Self and Consciousness in Neuroscience, Meditation, and Philosophy; Columbia University Press: New York, NY, USA, 2014; p. 496. [Google Scholar]
- Josipovic, Z. Nondual awareness: Consciousness-as-such as non-representational reflexivity. Prog. Brain Res. 2019, 244, 273–298. [Google Scholar] [CrossRef] [PubMed]
- Metzinger, T. Minimal phenomenal experience: Meditation, tonic alertness, and the phenomenology of “pure” consciousness. PhiMiSci 2020, 1, 7. [Google Scholar] [CrossRef]
- Goldsmith, M. Franz Anton Mesmer: A History of Mesmerism; Doubleday, Doran & Company: Garden City, NY, USA, 1934; p. 308. [Google Scholar]
- Strachey, J. (Ed.) The Standard Edition of the Complete Psychological Works of Sigmund Freud; Hogarth Press: London, UK, 1961; Volume 20. [Google Scholar]
- Bargh, J.A.; Morsella, E. The unconscious mind. Perspect. Psychol. Sci. 2008, 3, 73–79. [Google Scholar] [CrossRef]
- James, W. Principles of Psychology; Henry Holt and Company: New York, NY, USA, 1890; Volume 2. [Google Scholar]
- Gazzaniga, M. The Social Brain; Basic Books: New York, NY, USA, 1985. [Google Scholar]
- Libet, B. Unconscious cerebral initiative and the role of conscious will in voluntary action. Behav. Brain. Sci. 1986, 8, 529–566. [Google Scholar] [CrossRef]
- Wegner, D.M. The Illusion of Conscious Will; MIT Press: Cambridge, MA, USA, 2002; p. 440. [Google Scholar]
- Vygotsky, L.S. Thought and Language; MIT Press: Cambridge, MA, USA, 1962; p. 168. [Google Scholar]
- Morsella, E. The function of phenomenal states: Supramodular interaction theory. Psychol. Rev. 2005, 112, 1000–1021. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. The 8 pillars of metacognition. Int. J. Emerg. Technol. Learn. 2020, 15, 162–178. [Google Scholar] [CrossRef]
- Kihlstrom, J.F. Unconscious processes. In The Oxford Handbook of Cognitive Psychology; Reisberg, D., Ed.; Oxford University Press: Oxford, UK, 2013; pp. 176–186. [Google Scholar] [CrossRef]
- Weiskrantz, L. Blindsight: A Case Study and Implications; Oxford University Press: Oxford, UK, 1986. [Google Scholar]
- DeGelder, B.; De Haan, E.H.F.; Heywood, C.A. (Eds.) Out of Mind: Varieties of Unconscious Processes; Oxford University Press: London, UK, 2001. [Google Scholar]
- Marcel, A.J. Conscious and unconscious perception: An approach to the relations between phenomenal experience and perceptual processes. Cogn. Psychol. 1983, 15, 238–300. [Google Scholar] [CrossRef] [PubMed]
- Young, A.W. (Ed.) Face and Mind; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Pedhazur, E.J.; Pedhazur Schmelkin, L. Measurement, Design, and Analysis: An Integrated Approach; Psychology Press: New York, NY, USA, 1991; p. 840. [Google Scholar]
- Searle, J.R. The Rediscovery of The Mind; MIT Press: Cambridge, MA, USA, 1992. [Google Scholar]
- Velmans, M. Consciousness and the “Causal Paradox”. Behav. Brain Sci. 1996, 19, 538–542. [Google Scholar] [CrossRef]
- McFadden, J. Consciousness: Matter or EMF? Front. Hum. Neurosci. 2023, 16, 1024934. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, P.D.; Hales, C.G. What neuroscientists yhink, and don’t think, about consciousness. Front. Hum. Neurosci. 2022, 16, 767612. [Google Scholar] [CrossRef] [PubMed]
- Williams, G. What is it like to be nonconscious? A defense of Julian Jaynes. Phenomenol. Cogn. Sci. 2011, 10, 217–239. [Google Scholar] [CrossRef]
- Allen, J.A. Delineating conscious and unconscious processes: Commentary on Baars on contrastive analysis. Psyche Int. J. Res. Consci. 1994, 1. Available online: http://psyche.cs.monash.edu.au/v1/psyche-1-09-allen.html (accessed on 5 February 2023).
- Thompson, E. Mind in Life: Biology, Phenomenology, and The Sciences of Mind; Harvard University Press: Cambridge, MA, USA, 2007. [Google Scholar]
- Augusto, L.M. Unconscious knowledge: A survey. Adv. Cogn. Psychol. 2010, 6, 116–141. [Google Scholar] [CrossRef]
- Dresp-Langley, B. Why the brain knows more than we do: Non-conscious representations and their role in the construction of conscious experience. Brain Sci. 2011, 2, 1–21. [Google Scholar] [CrossRef]
- Cleeremans, A. Conscious and unconscious cognition: A graded, dynamic perspective. In Progress in Psychological Science around the World; Jing, Q., Rosenzweig, M.R., d’Ydewalle, G., Zhang, H., Chen, H.-C., Zhang, K., Eds.; Psychology Press: London, UK, 2006; pp. 402–418. [Google Scholar]
- Metzinger, T. M-autonomy. J. Conscious. Stud. 2015, 22, 270–302. [Google Scholar]
- Neisser, J.U. Unconscious subjectivity. Psyche 2006, 12, 1–14. Available online: https://journalpsyche.org/files/0xaaf7.pdf (accessed on 5 February 2023).
- Wokke, M.E.; van Gaal, S.; Scholte, H.S.; Ridderinkhof, K.R.; Lamme, V.A. The flexible nature of unconscious cognition. PLoS ONE 2011, 6, e25729. [Google Scholar] [CrossRef] [PubMed]
- Lewicki, P.; Hill, T.; Czyzewska, M. Nonconscious acquisition of information. Am. Psychol. 1992, 47, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Kihlstrom, J.F. The psychological unconscious. In Handbook of Personality: Theory and Research, 3rd ed.; John, O., Robins, R., Pervin, L., Eds.; The Guilford Press: New York, NY, USA, 2008; pp. 583–602. [Google Scholar]
- Wegner, D.M. Who is the controller of controlled processes? Chapter 1. In The New Unconscious. Oxford Series in Social Cognition and Social Neuroscience Series; Hassin, R.R., Uleman, J.S., Bargh, J.A., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 19–37. [Google Scholar]
- Locke, E.A.; Kristof, A.L. Volitional choices in the goal achievement process. In The Psychology of Action: Linking Cognition and Motivation to Behavior; Gollwitzer, P.M., Bargh, J.A., Eds.; The Guilford Press: New York, NY, USA, 1996; pp. 365–384. [Google Scholar]
- Dehaene, S. Conscious and nonconscious processes: Distinct forms of evidence accumulation? In Better Than Conscious? Decision Making, The Human Mind, and Implications for Institutions; Engel, C., Singer, W., Eds.; MIT Press: Cambridge, MA, USA, 2008; pp. 21–49. [Google Scholar]
- Jung, C.G. Approaching the unconscious. In Man and His Symbols; Jung, C.G., Ed.; Doubleday: Garden City, NY, USA, 1964; pp. 18–103. [Google Scholar]
- Franklin, S.; Baars, B.J. Two varieties of unconscious processes. In New Horizons in the Neuroscience of Consciousness; Perry, E.K., Collerton, D., LeBeau, F.E.N., Ashton, H., Eds.; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2010; pp. 91–102. [Google Scholar]
- Marchetti, G. Consciousness, Attention and Meaning; Nova Science Publishers: Hauppauge, NY, USA, 2010. [Google Scholar]
- Fingelkurts, A.A.; Fingelkurts, A.A. Brain-mind operational architectonics imaging: Technical and methodological aspects. Open Neuroimag. J. 2008, 2, 73–93. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A. Operational architectonics methodology for EEG analysis: Theory and results. Neuromethods 2015, 91, 1–59. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Quantitative electroencephalogram (qEEG) as a natural and non-invasive window into living brain and mind in the functional continuum of healthy and pathological conditions. Appl. Sci. 2022, 12, 9560. [Google Scholar] [CrossRef]
- Young, M.J.; Edlow, B.L. The quest for covert consciousness: Bringing neuroethics to the bedside. Neurology 2021, 96, 893–896. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Operational architectonics of the human brain biopotential field: Towards solving the mind-brain problem. Brain Mind 2001, 2, 261–296. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Neves, C.F.H. Phenomenological architecture of a mind and Operational Architectonics of the brain: The unified metastable continuum. J. New Math. Nat. Comput. 2009, 5, 221–244. [Google Scholar] [CrossRef]
- Kelso, J.A.S.; Engstrøm, D. The Complementary Nature; MIT Press: Cambridge, MA, USA, 2006. [Google Scholar]
- Metzinger, T. Phenomenal transparency and cognitive self-reference. Phenomenol. Cogn. Sci. 2003, 2, 353–393. [Google Scholar] [CrossRef]
- Jirsa, V.K.; Kelso, J.A.S. Spatiotemporal pattern formation in neural systems with heterogeneous connection topologies. Phys. Rev. E 2000, 62, 8462–8465. [Google Scholar] [CrossRef]
- Freeman, W.J. How Brains Make Up Their Minds; Columbia University Press: New York, NY, USA, 2001; p. 146. [Google Scholar]
- Friston, K. The free-energy principle: A unified brain theory? Nat. Rev. Neurosci. 2010, 11, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A. Mapping of brain operational architectonics. In Focus on Brain Mapping Research; Chen, F.J., Ed.; Nova Science Publishers, Inc.: Hauppauge, NY, USA, 2005; pp. 59–98. [Google Scholar]
- Smirnova, L.; Caffo, B.S.; Gracias, D.H.; Huang, Q.; Morales Pantoja, I.E.; Tang, B.; Zack, D.J.; Berlinicke, C.A.; Boyd, J.L.; Harris, T.D.; et al. Organoid intelligence (OI): The new frontier in biocomputing and intelligence-in-a-dish. Front. Sci. 2023, 1, 1017235. [Google Scholar] [CrossRef]
- Isomura, T.; Kotani, K.; Jimbo, Y. Cultured cortical neurons can perform blind source separation according to the free-energy principle. PloS Comput. Biol. 2015, 11, e1004643. [Google Scholar] [CrossRef] [PubMed]
- Marom, S.; Shahaf, G. Development, learning and memory in large random networks of cortical neurons: Lessons beyond anatomy. Q. Rev. Biophys. 2002, 35, 63–87. [Google Scholar] [CrossRef]
- Shahaf, G.; Marom, S. Learning in networks of cortical neurons. J. Neurosci. 2001, 21, 8782–8788. [Google Scholar] [CrossRef]
- Tessadori, J.; Chiappalone, M. Closed-loop neuro-robotic experiments to test computational properties of neuronal networks. J. Vis. Exp. 2015, 97, 52341. [Google Scholar] [CrossRef]
- Kagan, B.J.; Kitchen, A.C.; Tran, N.T.; Habibollahi, F.; Khajehnejad, M.; Parker, B.J.; Bhat, A.; Rollo, B.; Razi, A.; Friston, K.J. In vitro neurons learn and exhibit sentience when embodied in a simulated game-world. Neuron 2022, 110, 3952–3969.e8. [Google Scholar] [CrossRef]
- Namdul, T. Re-examining death: Doors to resilience and wellbeing in Tibetan Buddhist practice. Religions 2021, 12, 522. [Google Scholar] [CrossRef]
- Deutsch, E. Advaita Vedanta. A Philosophical Reconstruction; University of Hawaii Press: Honolulu, HI, USA, 1969. [Google Scholar]
- Nash, J.D.; Newberg, A. Toward a unifying taxonomy and definition for meditation. Front. Psychol. 2013, 4, 806. [Google Scholar] [CrossRef]
- Dalai Lama, X.I.V.; Hopkins, J. Mind of Clear Light: Advice on Living Well and Dying Consciously; Atria Books: New York, NY, USA, 2004. [Google Scholar]
- Lott, D.T.; Yeshi, T.; Norchung, N.; Dolma, S.; Tsering, N.; Jinpa, N.; Woser, T.; Dorjee, K.; Desel, T.; Fitch, D.; et al. No detectable electroencephalographic activity after clinical declaration of death among Tibetan Buddhist meditators in apparent Tukdam, a putative post-mortem meditation state. Front. Psychol. 2021, 11, 599190. [Google Scholar] [CrossRef]
- Lingpa, K. The Tibetan Book of the Dead: Awakening Upon Dying; Lulu Press, Inc.: Morrisville, NC, USA, 2014. [Google Scholar]
- Seth, A.K. Interoceptive inference, emotion, and the embodied self. Trends Cogn. Sci. 2013, 17, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Hohwy, J. The self-evidencing brain. Noûs 2016, 50, 259–285. [Google Scholar] [CrossRef]
- Limanowski, J.; Friston, K. ‘Seeing the dark’: Grounding phenomenal transparency and opacity in precision estimation for active inference. Front. Psychol. 2018, 9, 643. [Google Scholar] [CrossRef] [PubMed]
- Medvedev, S.V.; Boytsova, J.A.; Bubeev, Y.A.; Kaplan, A.Y.; Kokurina, E.V.; Olsen, A.; Smoleevskiy, A.E.; Syrov, N.V.; Yakovlev, L.V.; Zhironkina, Y.S.; et al. Traditional Buddhist meditations reduce mismatch negativity in experienced monk- practitioners. Int. J. Psychophysiol. 2022, 181, 112–124. [Google Scholar] [CrossRef]
- Freeman, W.J. Neurodynamics. An Exploration of Mesoscopic Brain Dynamics; Springer: London, UK, 2000. [Google Scholar]
- Nunez, P.L. Toward a quantitative description of large-scale neocortical dynamic function and EEG. Behav. Brain Sci. 2000, 23, 371–398. [Google Scholar] [CrossRef]
- Barsalou, L.W. Perceptual symbol systems. Behav. Brain Sci. 1999, 22, 577–660. [Google Scholar] [CrossRef]
- Palmer, S.E. Color, consciousness, and the isomorphism constraint. Behav. Brain Sci. 1999, 22, 923–943. [Google Scholar] [CrossRef]
- Orpwood, R. Qualia could arise from information processing in local cortical networks. Front. Psychol. 2013, 4, 121. [Google Scholar] [CrossRef]
- Bayne, T.; Hohwy, J.; Owen, A.M. Are there levels of consciousness? Trends Cogn. Sci. 2016, 20, 405–413. [Google Scholar] [CrossRef]
- Millière, R.; Carhart-Harris, R.L.; Roseman, L.; Trautwein, F.-M.; Berkovich-Ohana, A. Psychedelics, meditation, and self-consciousness. Front. Psychol. 2018, 9, 1475. [Google Scholar] [CrossRef]
- Damasio, A. The Feeling of What Happens. Body, Emotion and the Making of Consciousness; Vintage: London, UK, 2000. [Google Scholar]
- Köhler, W. Dynamics in Psychology; Grove Press: New York, NY, USA, 1940. [Google Scholar]
- Fodor, J.A.; Pylyshyn, Z.W. Connectionism and cognitive architecture: A critical analysis. Cognition 1988, 28, 3–71. [Google Scholar] [CrossRef] [PubMed]
- Dainton, B. Stream of Consciousness; Routledge: London, UK, 2000. [Google Scholar]
- Feinberg, T.E. The nested hierarchy of consciousness: A neurobiological solution to the problem of mental unity. Neurocase 2000, 6, 75–81. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Attentional state: From automatic detection to willful focused concentration. In Attention and Meaning: The Attentional Basis of Meaning; Marchetti, G., Benedetti, G., Alharbi, A., Eds.; Nova Science Publishers: Hauppauge, NY, USA, 2015; pp. 133–150. [Google Scholar]
- Marchetti, G. Against the view that consciousness and attention are fully dissociable. Front. Psychol. 2012, 3, 36. [Google Scholar] [CrossRef] [PubMed]
- Yufik, Y.M. How the mind works: An exercise in pragmatism. In Proceedings of the 2002 International Joint Conference on Neural Networks, Honolulu, HI, USA, 12–17 May 2002; pp. 2265–2269. [Google Scholar] [CrossRef]
- Noack, R.A. Solving the “human problem”: The frontal feedback model. Conscious. Cogn. 2012, 21, 1043–1067. [Google Scholar] [CrossRef]
- James, W. Principles of Psychology; Henry Holt and Company: New York, NY, USA, 1890; Volume 1. [Google Scholar]
- Freeman, W.J. Indirect biological measures of consciousness from field studies of brains as dynamical systems. Neural Netw. 2007, 20, 1021–1031. [Google Scholar] [CrossRef]
- Metzinger, T. Being No One; MIT Press: Cambridge, MA, USA, 2003. [Google Scholar]
- Fingelkurts, A.A.; Fingelkurts, A.A. Alpha rhythm operational architectonics in the continuum of normal and pathological brain states: Current state of research. Int. J. Psychophysiol. 2010, 76, 93–106. [Google Scholar] [CrossRef]
- Velmans, M. Is human information processing conscious? Behav. Brain Sci. 1991, 14, 651–726. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Timing in cognition and EEG brain dynamics: Discreteness versus continuity. Cogn. Process. 2006, 7, 135–162. [Google Scholar] [CrossRef]
- Toates, F. The interaction of cognitive and stimulus–response processes in the control of behaviour. Neurosci. Biobehav. Rev. 1998, 22, 59–83. [Google Scholar] [CrossRef]
- Treisman, A.M.; Kanwisher, N.G. Perceiving visually presented objects: Recognition awareness and modularity. Curr. Opin. Neurobiol. 1998, 8, 218–226. [Google Scholar] [CrossRef]
- Libet, B. Timing of conscious experience: Reply to the 2002 commentaries on Libet’s findings. Conscious. Cogn. 2003, 12, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Bagnato, S.; Boccagni, C.; Galardi, G. Long-term (six years) clinical outcome discrimination of patients in the vegetative state could be achieved based on the operational architectonics EEG analysis: A pilot feasibility atudy. Open Neuroimag. J. 2016, 10, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Tononi, G. An information integration theory of consciousness. BMC Neurosci. 2004, 5, 42. [Google Scholar] [CrossRef] [PubMed]
- Fins, J.J. Rethinking disorders of consciousness: New research and its implications. Hastings Cent. Rep. 2005, 35, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, M. How can we know if patients in coma, vegetative state or minimally conscious state are conscious? Prog. Brain Res. 2009, 177, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Kallio-Tamminen, T. Selfhood triumvirate: From phenomenology to brain activity and back again. Conscious. Cogn. 2020, 86, 103031. [Google Scholar] [CrossRef]
- Gallagher, S. Philosophical conceptions of the self: Implications for cognitive science. Trends Cogn. Sci. 2000, 4, 14–21. [Google Scholar] [CrossRef]
- Zahavi, D. First-person thoughts and embodied self-awareness: Some reflections on the relation between recent analytic philosophy and phenomenology. Phenomenol. Cogn. Sci. 2002, 1, 7–26. [Google Scholar] [CrossRef]
- Metzinger, T. Empirical perspectives from the self-model theory of subjectivity: A brief summary with examples. Prog. Brain Res. 2008, 168, 215–245. [Google Scholar] [CrossRef]
- Lane, T.J. The minimal self hypothesis. Conscious. Cogn. 2020, 85, 103029. [Google Scholar] [CrossRef]
- Millière, R. The varieties of selflessness. PhiMiSci. 2020, 1, 1–41. [Google Scholar] [CrossRef]
- Sass, L.A. Madness and Modernism. In Insanity in The Light of Modern Art, Literature, and Thought; Oxford University Press: New York, NY, USA, 2017. [Google Scholar]
- Zahavi, D. Phenomenology. The Basics; Routledge: London, UK; New York, NY, USA, 2019. [Google Scholar]
- Musholt, K. Thinking about Oneself: From Nonconceptual Content to the Concept of a Self; MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Gallagher, S. A pattern theory of self. Front. Hum. Neurosci. 2013, 7, 443. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Daly, A. Dynamical relations in the self-pattern. Front. Psychol. 2018, 9, 664. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Persistent operational synchrony within brain de-fault-mode network and self-processing operations in healthy subjects. Brain Cogn. 2011, 75, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Raichle, M.E.; MacLeod, A.M.; Snyder, A.Z.; Powers, W.J.; Gusnard, D.A.; Shulman, G.L. A default mode of brain function. Proc. Natl. Acad. Sci. USA 2001, 98, 676–682. [Google Scholar] [CrossRef]
- Davey, C.G.; Pujol, J.; Harrison, B.J. Mapping the self in the brain’s default mode network. NeuroImage 2016, 132, 390–397. [Google Scholar] [CrossRef]
- Northoff, G. Is the self a higher-order or fundamental function of the brain? The “basis model of self-specificity” and its encoding by the brain’s spontaneous activity. Cogn. Neurosci. 2016, 7, 203–222. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Three-dimensional components of selfhood in treatment-naive patients with major depressive disorder: A resting-state qEEG imaging study. Neuropsychologia 2017, 99, 30–36. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Alterations in the three components of selfhood in persons with post-traumatic stress disorder symptoms: A pilot qEEG neuroimaging study. Open Neuroimag. J. 2018, 12, 42–54. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A. Longitudinal dynamics of 3-dimensional components of Selfhood after severe traumatic brain injury: A qEEG case study. Clin. EEG Neurosci. 2017, 48, 327–337. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Kallio-Tamminen, T. Self, Me and I in the repertoire of spontaneously occurring altered states of Selfhood: Eight neurophenomenological case study reports. Cogn. Neurodyn. 2022, 16, 255–282. [Google Scholar] [CrossRef] [PubMed]
- de Vignemont, F.; Fourneret, P. The sense of agency: A philosophical and empirical review of the “Who” system. Conscious. Cogn. 2004, 13, 1–19. [Google Scholar] [CrossRef]
- Hohwy, J. The sense of self in the phenomenology of agency and perception. Psyche 2007, 13, 1–20. Available online: https://journalpsyche.org/files/0xab11.pdf (accessed on 1 March 2023).
- Blanke, O.; Metzinger, T. Full-body illusions and minimal phenomenal selfhood. Trends Cogn. Sci. 2009, 13, 7–13. [Google Scholar] [CrossRef]
- Varela, F.J.; Thompson, E.; Rosch, E. The Embodied Mind: Cognitive Science and Human Experience; The MIT Press: Cambridge, MA, USA, 1991. [Google Scholar]
- Gallagher, S. How the Body Shapes the Mind; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Legrand, D. The bodily self: The sensori-motor roots of pre-reflective self-consciousness. Phenom. Cogn. Sci. 2006, 5, 89–118. [Google Scholar] [CrossRef]
- Seth, A.K.; Suzuki, K.; Critchley, H.D. An interoceptive predictive coding model of conscious presence. Front. Psychol. 2012, 2, 395. [Google Scholar] [CrossRef]
- Limanowski, J.; Blankenburg, F. Minimal self-models and the free energy principle. Front. Hum. Neurosci. 2013, 7, 547. [Google Scholar] [CrossRef]
- Apps, M.A.J.; Tsakiris, M. The free-energy self: A predictive coding account of self-recognition. Neurosci. Biobehav. Rev. 2014, 41, 85–97. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Bagnato, S.; Boccagni, C.; Galardi, G. DMN Operational synchrony relates to self-consciousness: Evidence from patients in vegetative and minimally conscious ctates. Open Neuroimag. J. 2012, 6, 55–68. [Google Scholar] [CrossRef]
- Kinsbourne, M. A continuum of self-consciousness that emerges in phylogeny and ontogeny. In The Missing Link in Cognition: Origins of Self-Reflective Consciousness; Terrace, H.S., Metcalfe, J., Eds.; Oxford University Press: New York, NY, USA, 2005; pp. 142–156. [Google Scholar]
- Oakley, D.A.; Halligan, P.W. Chasing the rainbow: The non-conscious nature of being. Front. Psychol. 2017, 8, 1924. [Google Scholar] [CrossRef] [PubMed]
- Boly, M.; Tshibanda, L.; Vanhaudenhuyse, A.; Noirhomme, Q.; Schnakers, C.; Ledoux, D.; Boveroux, P.; Garweg, C.; Lambermont, B.; Phillips, C.; et al. Functional connectivity in the default network during resting state is preserved in a vegetative but not in a brain dead patient. Hum. Brain Map. 2009, 30, 2393–2400. [Google Scholar] [CrossRef]
- Norton, L.; Hutchison, R.M.; Young, G.B.; Lee, D.H.; Sharpe, M.D.; Mirsattari, S.M. Disruptions of functional connectivity in the default mode network of comatose patients. Neurology 2012, 78, 175–181. [Google Scholar] [CrossRef]
- Vanhaudenhuyse, A.; Noirhomme, Q.; Tshibanda, L.J.; Bruno, M.; Boveroux, P.; Schnakers, C.; Soddu, A.; Perlbarg, V.; Ledoux, D.; Brichant, J.F.; et al. Default network connectivity reflects the level of consciousness in non-communicative brain-damaged patients. Brain 2010, 133, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Allegrini, P.; Paradisi, P.; Menicucci, D.; Laurino, M.; Bedini, R.; Piarulli, A.; Gemignani, A. Sleep unconsciousness and breakdown of serial critical in-termittency: New vistas on the global workspace. Chaos Solit. Fractals 2013, 55, 32–43. [Google Scholar] [CrossRef]
- Pistoia, F.; Mattiacci, G.; Sarà, M.; Padua, L.; Macchi, C.; Sacco, S. Development of the Italian version of the near-death experience scale. Front. Hum. Neurosci. 2018, 12, 45. [Google Scholar] [CrossRef]
- Charland-Verville, V.; Jourdan, J.; Thonnard, M.; Ledoux, D.; Donneau, A.; Quertemont, E.; Laureys, S. Near-death experiences in non-life-threatening events and coma of different etiologies. Front. Hum. Neurosci. 2014, 8, 203. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002, 3, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Tsakiris, M. My body in the brain: A neurocognitive model of body-ownership. Neuropsychologia 2010, 48, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Grof, S. Realms of the Human Unconscious: Observations from LSD Research; Plume Books: New York, NY, USA, 1976. [Google Scholar]
- Parnas, J.; Handest, P. Phenomenology of anomalous self-experience in early schizophrenia. Compr. Psychiatry 2003, 44, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Ataria, Y.; Dor-Ziderman, Y.; Berkovich-Ohana, A. How does it feel to lack a sense of boundaries? A case study of a long-term mind-fulness meditator. Conscious. Cogn. 2015, 37, 133–147. [Google Scholar] [CrossRef]
- Lebedev, A.V.; Kaelen, M.; Lövdén, M.; Nilsson, J.; Feilding, A.; Nutt, D.; Carhart-Harris, R.L. LSD-induced entropic brain activity predicts subsequent personality change. Hum. Brain Mapp. 2016, 37, 3203–3213. [Google Scholar] [CrossRef] [PubMed]
- Millière, R. Looking for the self: Phe-nomenology, neurophysiology and philosophical significance of drug-induced ego dissolution. Front. Hum. Neurosci. 2017, 11, 245. [Google Scholar] [CrossRef] [PubMed]
- Girn, M.; Christoff, K. Expanding the scientific study of self-experience with psychedelics. J. Conscious. Stud. 2018, 25, 131–154. [Google Scholar]
- Wittmann, M. The inner sense of time: How the brain creates a representation of duration. Nat. Rev. Neurosci. 2013, 14, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Berkovich-Ohana, A.; Wittmann, M. A typology of altered states according to the conscious-ness state space (CSS) model. J. Conscious. Stud. 2017, 24, 37–61. [Google Scholar]
- Friston, K. Am I self-conscious? (Or does self-organization entail self-consciousness?). Front. Psychol. 2018, 9, 579. [Google Scholar] [CrossRef]
- Metzinger, T. Why are dreams interesting for philosophers? The example of minimal phenomenal selfhood, plus an agenda for future research. Conscious. Res. 2013, 4, 746. [Google Scholar] [CrossRef]
- Zahavi, D. Subjectivity and Selfhood; The MIT Press: Cambridge, MA, USA, 2006. [Google Scholar]
- Velmans, M. Conscious agency and the preconscious/unconscious Self. In Interdisciplinary Perspectives on Consciousness and the Self; Menon, S., Sinha, A., Sreekantan, B.V., Eds.; Springer: New Delhi, India, 2014; pp. 11–25. [Google Scholar]
- Morin, A. Self-awareness Part 1: Definition, measures, effects, functions, and antecedents. Soc. Personal. Psychol. Compass 2011, 5, 807–823. [Google Scholar] [CrossRef]
- Singer, P. Practical Ethics; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Baars, B.J.; Ramsøy, T.Z.; Laureys, S. Brain, conscious experience and the observing self. Trends Neurosci. 2003, 26, 671–675. [Google Scholar] [CrossRef]
- Kriegel, U. The value of consciousness. Analysis 2019, 79, 503–520. [Google Scholar] [CrossRef]
- Mashour, G.M.; LaRock, E. Inverse zombies, anesthesia awareness, and the hard problem of unconsciousness. Conscious. Cogn. 2008, 17, 1163–1168. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fingelkurts, A.A.; Fingelkurts, A.A. Patients with Disorders of Consciousness: Are They Nonconscious, Unconscious, or Subconscious? Expanding the Discussion. Brain Sci. 2023, 13, 814. https://doi.org/10.3390/brainsci13050814
Fingelkurts AA, Fingelkurts AA. Patients with Disorders of Consciousness: Are They Nonconscious, Unconscious, or Subconscious? Expanding the Discussion. Brain Sciences. 2023; 13(5):814. https://doi.org/10.3390/brainsci13050814
Chicago/Turabian StyleFingelkurts, Andrew A., and Alexander A. Fingelkurts. 2023. "Patients with Disorders of Consciousness: Are They Nonconscious, Unconscious, or Subconscious? Expanding the Discussion" Brain Sciences 13, no. 5: 814. https://doi.org/10.3390/brainsci13050814
APA StyleFingelkurts, A. A., & Fingelkurts, A. A. (2023). Patients with Disorders of Consciousness: Are They Nonconscious, Unconscious, or Subconscious? Expanding the Discussion. Brain Sciences, 13(5), 814. https://doi.org/10.3390/brainsci13050814