
The Impact of Intradialytic Cognitive and Physical Training Program on the Physical and Cognitive Abilities in End-Stage Kidney Disease Patients: A Randomized Clinical Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
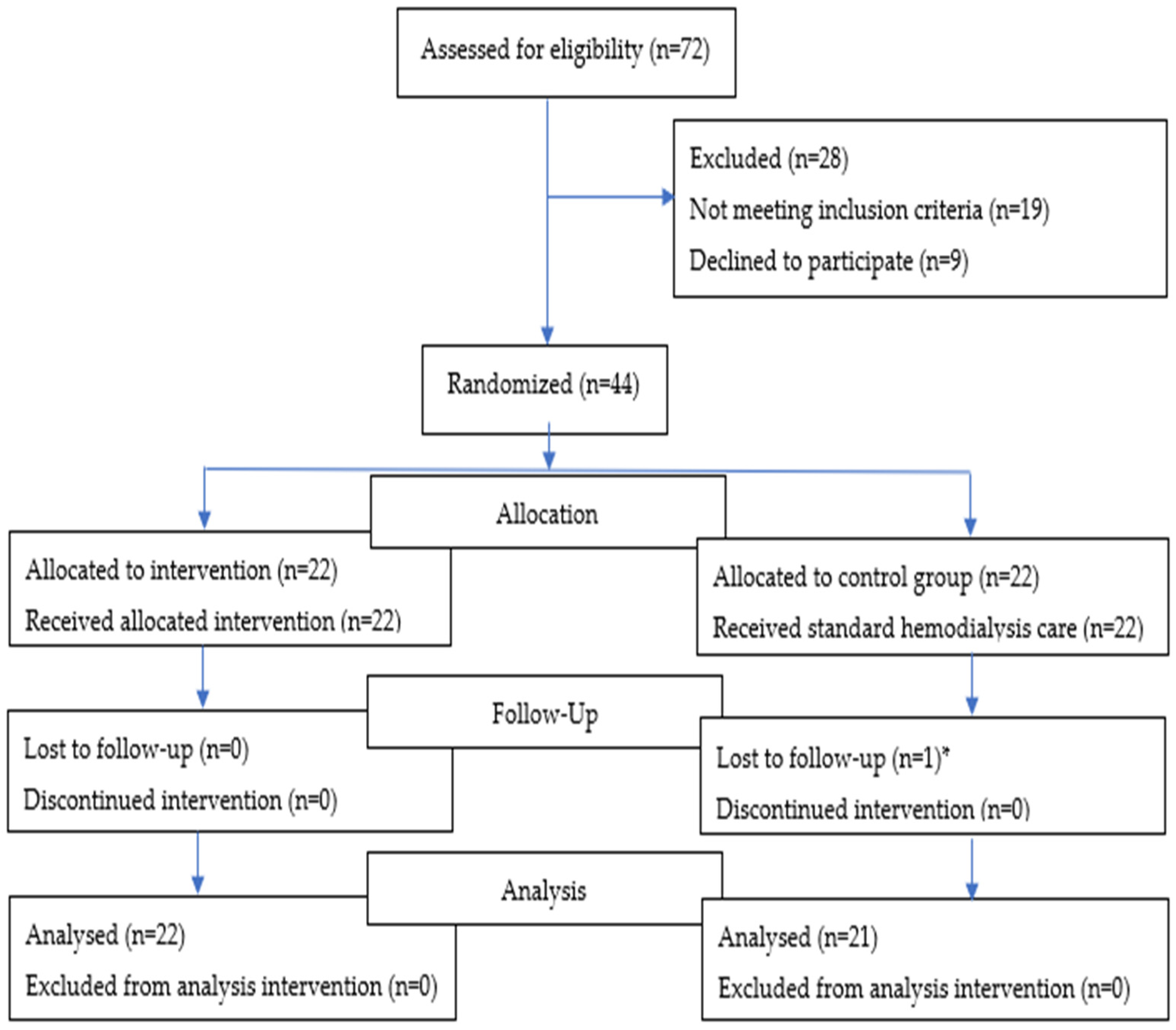
2.1. Participants
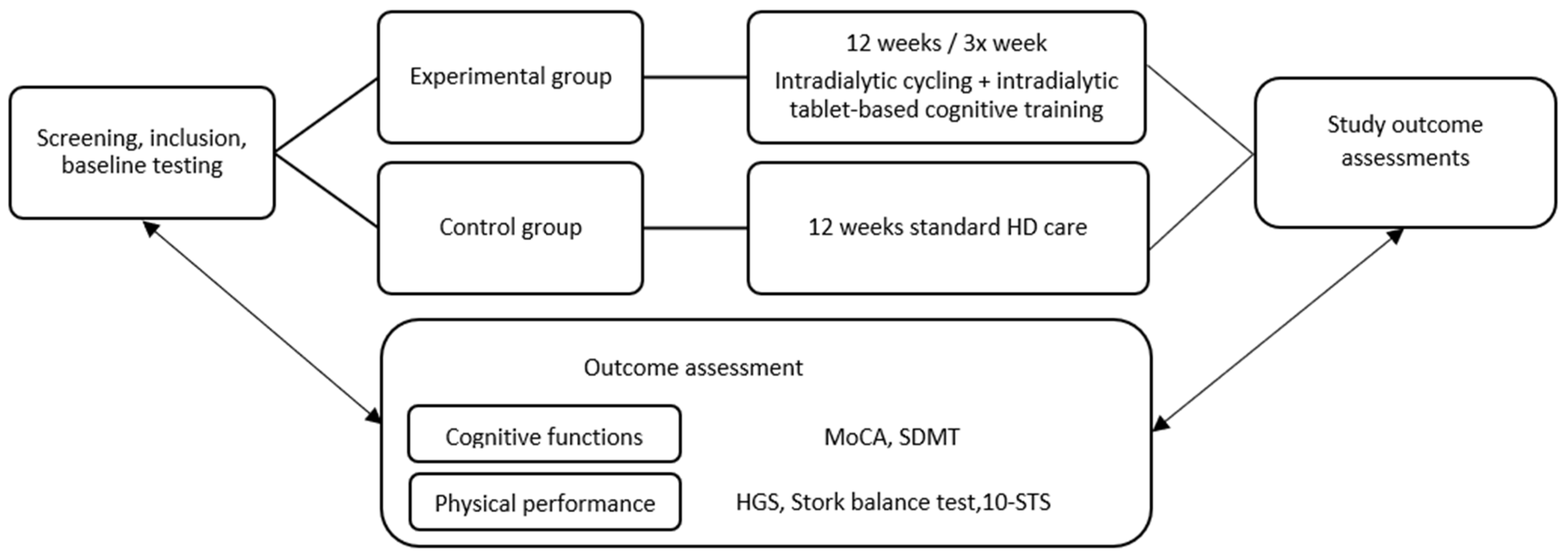
2.2. Outcome Measures
2.3. Procedure
2.4. Statistics
3. Results
Participants’ General Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Kumar Agarwal, S.; Agudelo-Botero, M.; et al. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Foreman, K.J.; Dolgert, A.; Fukutaki, K.B.; Fullman MPH, N.; McGaughey, M.B.; Pletcher BS, M.A.; Smith MPA, A.E.; Tang, K.B.; Yuan, C.; Brown, J.C.; et al. Forecasting Life Expectancy, Years of Life Lost, and All-Cause and Cause-Specific Mortality for 250 Causes of Death: Reference and Alternative Scenarios for 2016-40 for 195 Countries and Territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Beberashvili, I.; Azar, A.; Sinuani, I.; Shapiro, G.; Feldman, L.; Stav, K.; Sandbank, J.; Averbukh, Z. Bioimpedance Phase Angle Predicts Muscle Function, Quality of Life and Clinical Outcome in Maintenance Hemodialysis Patients. Eur. J. Clin. Nutr. 2014, 68, 683–689. [Google Scholar] [CrossRef]
- Hornik, B.; Duława, J. Frailty, Quality of Life, Anxiety, and Other Factors Affecting Adherence to Physical Activity Recommendations by Hemodialysis Patients. Int. J. Environ. Res. Public Health 2019, 16, 1827. [Google Scholar] [CrossRef]
- Choi, B.; Crouzet, C.; Lau, W.L.; Cribbs, D.H.; Fisher, M.J. Cerebral Blood Flow in Chronic Kidney Disease. J. Stroke Cerebrovasc. Dis. 2021, 30, 105702. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.M.; Tupper, D.E.; Knopman, D.S.; Gilbertson, D.T.; Pederson, S.L.; Li, S.; Smith, G.E.; Hochhalter, A.K.; Collins, A.J.; Kane, R.L. Cognitive Impairment in Hemodialysis Patients Is Common. Neurology 2006, 67, 216–223. [Google Scholar] [CrossRef]
- Brodski, J.; Rossell, S.L.; Castle, D.J.; Tan, E.J. A Systematic Review of Cognitive Impairments Associated With Kidney Failure in Adults Before Natural Age-Related Changes. J. Int. Neuropsychol. Soc. 2019, 25, 101–114. [Google Scholar] [CrossRef]
- Drew, D.A.; Weiner, D.E.; Sarnak, M.J. Cognitive Impairment in CKD: Pathophysiology, Management, and Prevention. Am. J. Kidney Dis. 2019, 74, 782–790. [Google Scholar] [CrossRef]
- Nicholas, P.; Green, T.; Purtell, L.; Bonner, A. A Cross-Sectional Study Exploring Cognitive Impairment in Kidney Failure. J. Ren. Care 2022, 48, 93–101. [Google Scholar] [CrossRef]
- Oh, H.S.; Mo, J.A.; Seo, W.S. Correlates of Cognitive Impairment in Patients with Chronic Kidney Failure on Haemodialysis: Systematic Review and Meta-Analysis. J. Adv. Nurs. 2019, 75, 962–978. [Google Scholar] [CrossRef]
- Luo, Y.; Murray, A.M.; Guo, Y.D.; Tian, R.; Ye, P.P.; Li, X.; Li, G.G.; Lu, F.P.; Ma, Y.C.; Sun, Y.; et al. Cognitive Impairment and Associated Risk Factors in Older Adult Hemodialysis Patients: A Cross-Sectional Survey. Sci. Rep. 2020, 10, 12542. [Google Scholar] [CrossRef] [PubMed]
- Drew, D.A.; Weiner, D.E.; Tighiouart, H.; Duncan, S.; Gupta, A.; Scott, T.; Sarnak, M.J. Cognitive Decline and Its Risk Factors in Prevalent Hemodialysis Patients. Am. J. Kidney Dis. 2017, 69, 780. [Google Scholar] [CrossRef] [PubMed]
- Thancharoen, O.; Waleekhachonloet, O.; Limwattananon, C.; Anutrakulchai, S. Cognitive Impairment, Quality of Life and Healthcare Utilization in Patients with Chronic Kidney Disease Stages 3 to 5. Nephrology 2020, 25, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Drew, D.A.; Weiner, D.E.; Tighiouart, H.; Scott, T.; Lou, K.; Kantor, A.; Fan, L.; Strom, J.A.; Singh, A.K.; Sarnak, M.J. Cognitive Function and All-Cause Mortality in Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2015, 65, 303–311. [Google Scholar] [CrossRef]
- Murtaza, A.; Dasgupta, I. Chronic Kidney Disease and Cognitive Impairment. J. Stroke Cerebrovasc. Dis. 2021, 30, 105529. [Google Scholar] [CrossRef]
- Noguchi, Y.; Ito, M.; Mushika, M.; Ito, T.; Kawamura, N. The Effect of N-Back Training during Hemodialysis on Cognitive Function in Hemodialysis Patients: A Non-Blind Clinical Trial. Ren. Replace. Ther. 2020, 6, 38. [Google Scholar] [CrossRef]
- Bogataj, Š.; Mesarič, K.K.; Pajek, M.; Petrušič, T.; Pajek, J. Physical Exercise and Cognitive Training Interventions to Improve Cognition in Hemodialysis Patients: A Systematic Review. Front. Public Health 2022, 10, 1032076. [Google Scholar] [CrossRef]
- Crowe, K.; Quinn, T.J.; Mark, P.B.; Findlay, M.D. “Is It Removed During Dialysis?”—Cognitive Dysfunction in Advanced Kidney Failure—A Review Article. Front. Neurol. 2021, 12, 787370. [Google Scholar] [CrossRef]
- Cobo, G.; Gallar, P.; Gama-Axelsson, T.; Di Gioia, C.; Qureshi, A.R.; Camacho, R.; Vigil, A.; Heimbürger, O.; Ortega, O.; Rodriguez, I.; et al. Clinical Determinants of Reduced Physical Activity in Hemodialysis and Peritoneal Dialysis Patients. J. Nephrol. 2015, 28, 503–510. [Google Scholar] [CrossRef]
- Kim, J.C.; Shapiro, B.B.; Zhang, M.; Li, Y.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Kalantar-Zadeh, K.; Kopple, J.D. Daily Physical Activity and Physical Function in Adult Maintenance Hemodialysis Patients. J. Cachexia Sarcopenia Muscle 2014, 5, 209. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.A.; Lantz, B.; Morgenstern, H.; Wang, M.; Bieber, B.A.; Gillespie, B.W.; Li, Y.; Painter, P.; Jacobson, S.H.; Rayner, H.C.; et al. Associations of Self-Reported Physical Activity Types and Levels with Quality of Life, Depression Symptoms, and Mortality in Hemodialysis Patients: The DOPPS. Clin. J. Am. Soc. Nephrol. 2014, 9, 1702–1712. [Google Scholar] [CrossRef] [PubMed]
- Pešak, J. Gibanje in Kognicija. eSiNAPSA. Available online: https://www.sinapsa.org/eSinapsa/stevilke/2019-17/266/gibanje_in_kognicija (accessed on 2 April 2023).
- Zhang, Y.; Li, C.; Zou, L.; Liu, X.; Song, W. The Effects of Mind-Body Exercise on Cognitive Performance in Elderly: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2791. [Google Scholar] [CrossRef]
- Zaletel, M. Nevroplastičnost Po Možganski Kapi. eSiNAPSA. Available online: https://www.sinapsa.org/eSinapsa/stevilke/2014-7/100/Nevroplasti%C4%8Dnost%20po%20mo%C5%BEganski%20kapi (accessed on 2 April 2023).
- Wallace, L.M.K.; Theou, O.; Godin, J.; Andrew, M.K.; Bennett, D.A.; Rockwood, K. Investigation of Frailty as a Moderator of the Relationship between Neuropathology and Dementia in Alzheimer’s Disease: A Cross-Sectional Analysis of Data from the Rush Memory and Aging Project. Lancet Neurol. 2019, 18, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Fabre, C.; Chamari, K.; Mucci, P.; Massé-Biron, J.; Préfaut, C. Improvement of Cognitive Function by Mental and/or Individualized Aerobic Training in Healthy Elderly Subjects. Int. J. Sports Med. 2002, 23, 415–421. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; et al. Exergaming and Older Adult Cognition: A Cluster Randomized Clinical Trial. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Konel, J.; Warsame, F.; Ying, H.; Fernández, M.G.; Carlson, M.C.; Fine, D.M.; Appel, L.J.; Segev, D.L. Intradialytic Cognitive and Exercise Training May Preserve Cognitive Function. Kidney Int. Rep. 2018, 3, 81. [Google Scholar] [CrossRef]
- Myers, J.; Chan, K.; Chen, Y.; Lit, Y.; Patti, A.; Massaband, P.; Kiratli, B.J.; Tamura, M.; Chertow, G.M.; Rabkin, R. Effect of a Home-Based Exercise Program on Indices of Physical Function and Quality of Life in Elderly Maintenance Hemodialysis Patients. Kidney Blood Press. Res. 2021, 46, 196–206. [Google Scholar] [CrossRef]
- Filipčič, T.; Bogataj, Š.; Pajek, J.; Pajek, M. Physical Activity and Quality of Life in Hemodialysis Patients and Healthy Controls: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1978. [Google Scholar] [CrossRef]
- Michou, V.; Davioti, M.; Syrakou, N.; Liakopoulos, V.; Deligiannis, A.; Kouidi, E. Effects of a Combined Intradialytic Exercise Training Program on Functional Capacity and Body Composition in Kidney Transplant Candidates. J. Funct. Morphol. Kinesiol. 2023, 8, 9. [Google Scholar] [CrossRef]
- Bogataj, Š.; Pajek, M.; Pajek, J.; Buturović Ponikvar, J.; Paravlic, A. Exercise-Based Interventions in Hemodialysis Patients: A Systematic Review with a Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 43. [Google Scholar] [CrossRef]
- Giannaki, C.D.; Hadjigeorgiou, G.M.; Karatzaferi, C.; Maridaki, M.D.; Koutedakis, Y.; Founta, P.; Tsianas, N.; Stefanidis, I.; Sakkas, G.K. A Single-Blind Randomized Controlled Trial to Evaluate the Effect of 6 Months of Progressive Aerobic Exercise Training in Patients with Uraemic Restless Legs Syndrome. Nephrol. Dial. Transplant. 2013, 28, 2834–2840. [Google Scholar] [CrossRef]
- Sember, V.; Bogataj, Š.; Ribeiro, J.C.; Paravlić, A.; Pajek, M.; Pajek, J. Accelerometry Correlates in Body Composition, Physical Fitness, and Disease Symptom Burden: A Pilot Study in End-Stage Renal Disease. Front. Physiol. 2021, 12, 737069. [Google Scholar] [CrossRef]
- Chu, N.M.; McAdams-DeMarco, M.A. Exercise and Cognitive Function in Patients with End-Stage Kidney Disease. Semin. Dial. 2019, 32, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Bogataj, Š.; Pajek, M.; Mesarič, K.K.; Kren, A.; Pajek, J. Twelve Weeks of Combined Physical and Cognitive Intradialytic Training Preserves Alertness and Improves Gait Speed: A Randomized Controlled Trial. Aging Clin. Exp. Res. 2023, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, L.K.; Fitzgerald, H.E.; Adams, K.M.; Nigg, J.T.; Martel, M.M.; Puttler, L.I.; Wong, M.M.; Zucker, R.A. Normative Symbol Digit Modalities Test Performance in a Community-Based Sample. Arch. Clin. Neuropsychol. 2006, 21, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.H.B.; Deluca, J.; Phillips, G.; LaRocca, N.; Hudson, L.D.; Rudick, R. Validity of the Symbol Digit Modalities Test as a Cognition Performance Outcome Measure for Multiple Sclerosis. Mult. Scler. J. 2017, 23, 721. [Google Scholar] [CrossRef]
- Lee, S.Y. Handgrip Strength: An Irreplaceable Indicator of Muscle Function. Ann. Rehabil. Med. 2021, 45, 167–169. [Google Scholar] [CrossRef]
- Bučar Pajek, M.; Leskošek, B.; Vivoda, T.; Svilan, K.; Čuk, I.; Pajek, J. Integrative Examination of Motor Abilities in Dialysis Patients and Selection of Tests for a Standardized Physical Function Assessment. Ther. Apher. Dial. 2016, 20, 286–294. [Google Scholar] [CrossRef]
- Muñoz-Bermejo, L.; Adsuar, J.C.; Mendoza-Muñoz, M.; Barrios-Fernández, S.; Garcia-Gordillo, M.A.; Pérez-Gómez, J.; Carlos-Vivas, J. Test-Retest Reliability of Five Times Sit to Stand Test (FTSST) in Adults: A Systematic Review and Meta-Analysis. Biology 2021, 10, 510. [Google Scholar] [CrossRef]
- Bogataj, Š.; Pajek, J.; Buturović Ponikvar, J.; Hadžić, V.; Pajek, M. Kinesiologist-Guided Functional Exercise in Addition to Intradialytic Cycling Program in End-Stage Kidney Disease Patients: A Randomised Controlled Trial. Sci. Rep. 2020, 10, 5717. [Google Scholar] [CrossRef] [PubMed]
- Bogataj, Š.; Trajković, N.; Pajek, M.; Pajek, J. Effects of Intradialytic Cognitive and Physical Exercise Training on Cognitive and Physical Abilities in Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial. Front. Psychol. 2022, 13, 62. [Google Scholar] [CrossRef] [PubMed]
- Research Randomizer. Available online: https://www.randomizer.org/ (accessed on 30 May 2023).
- Pierce, C.A.; Block, R.A.; Aguinis, H. Cautionary note on reporting eta-squared values from multifactor ANOVA designs Regardless of One’s Position on NHST, Most. Educ. Psychol. Meas. 2001, 64, 916–924. [Google Scholar] [CrossRef]
- Colangeli, S.; Boccia, M.; Verde, P.; Guariglia, P.; Bianchini, F.; Piccardi, L. Cognitive Reserve in Healthy Aging and Alzheimer’s Disease: A Meta-Analysis of FMRI Studies. Am. J. Alzheimer’s Dis. Other Dementias® 2016, 31, 443–449. [Google Scholar] [CrossRef]
- Viggiano, D.; Wagner, C.A.; Blankestijn, P.J.; Bruchfeld, A.; Fliser, D.; Fouque, D.; Frische, S.; Gesualdo, L.; Gutiérrez, E.; Goumenos, D.; et al. Mild Cognitive Impairment and Kidney Disease: Clinical Aspects. Nephrol. Dial. Transplant. 2020, 35, 10–17. [Google Scholar] [CrossRef]
- Van Zwieten, A.; Wong, G.; Ruospo, M.; Palmer, S.C.; Barulli, M.R.; Iurillo, A.; Saglimbene, V.; Natale, P.; Gargano, L.; Murgo, M.; et al. Prevalence and Patterns of Cognitive Impairment in Adult Hemodialysis Patients: The COGNITIVE-HD Study. Nephrol. Dial. Transplant. 2018, 33, 1197–1206. [Google Scholar] [CrossRef]
- Vanderlinden, J.A.; Ross-White, A.; Holden, R.; Shamseddin, M.K.; Day, A.; Boyd, J.G. Quantifying Cognitive Dysfunction across the Spectrum of End-Stage Kidney Disease: A Systematic Review and Meta-Analysis. Nephrology 2019, 24, 5–16. [Google Scholar] [CrossRef]
- Guo, Y.; Tian, R.; Ye, P.; Li, X.; Li, G.; Lu, F.; Ma, Y.; Sun, Y.; Wang, Y.; Xiao, Y.; et al. Cognitive Domain Impairment and All-Cause Mortality in Older Patients Undergoing Hemodialysis. Front. Endocrinol. 2022, 13, 1. [Google Scholar] [CrossRef]
- O’Lone, E.; Connors, M.; Masson, P.; Wu, S.; Kelly, P.J.; Gillespie, D.; Parker, D.; Whiteley, W.; Strippoli, G.F.M.; Palmer, S.C.; et al. Cognition in People with End-Stage Kidney Disease Treated with Hemodialysis: A Systematic Review and Meta-Analysis. Am. J. Kidney Dis. 2016, 67, 925–935. [Google Scholar] [CrossRef]
- Liu, H.; Song, Y.; Zhao, D.; Zhan, M. Effect of Exercise on Cognitive Impairment in Patients Undergoing Haemodialyses: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. J. Ren. Care 2022, 48, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Bennett, E.L.; Diamond, M.C.; Krech, D.; Rosenzweig, M.R. Chemical and Anatomical Plasticity of Brain. Science 1964, 146, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Spatz, H.C. Hebb’s Concept of Synaptic Plasticity and Neuronal Cell Assemblies. Behav. Brain Res. 1996, 78, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Rebok, G.W.; Ball, K.; Guey, L.T.; Jones, R.N.; Kim, H.Y.; King, J.W.; Marsiske, M.; Morris, J.N.; Tennstedt, S.L.; Unverzagt, F.W.; et al. Ten-Year Effects of the Advanced Cognitive Training for Independent and Vital Elderly Cognitive Training Trial on Cognition and Everyday Functioning in Older Adults. J. Am. Geriatr. Soc. 2014, 62, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, R.; Hoshi, K.; Yoneki, K.; Harada, M.; Watanabe, T.; Shimoda, T.; Yamamoto, S.; Matsunaga, A. Exercise Training in Elderly People Undergoing Hemodialysis: A Systematic Review and Meta-Analysis. Kidney Int. Rep. 2017, 2, 1096–1110. [Google Scholar] [CrossRef]
- Clarkson, M.J.; Bennett, P.N.; Fraser, S.F.; Warmington, S.A. Exercise Interventions for Improving Objective Physical Function in Patients with End-Stage Kidney Disease on Dialysis: A Systematic Review and Meta-Analysis. Am. J. Physiol. Ren. Physiol. 2019, 316, F856–F872. [Google Scholar] [CrossRef]
- Zhang, F.; Bai, Y.; Zhao, X.; Huang, L.; Wang, W.; Zhou, W.; Zhang, H. Therapeutic Effects of Exercise Interventions for Patients with Chronic Kidney Disease: An Umbrella Review of Systematic Reviews and Meta-Analyses. BMJ Open 2022, 12, e054887. [Google Scholar] [CrossRef]
- Nascimento Alves, M.; Souza Soares, A.; Melo Marinho, P. Efficacy of Resistance Exercise during Hemodialysis on Improving Lower Limb Muscle Strength in Patients with Chronic Kidney Disease: A Meta-Analysis of Randomized Clinical Trials. Physiother. Theory Pract. 2022. [Google Scholar] [CrossRef]
- Csuka, M.; McCarty, D.J. Simple Method for Measurement of Lower Extremity Muscle Strength. Am. J. Med. 1985, 78, 77–81. [Google Scholar] [CrossRef]
- Hellberg, M.; Höglund, P.; Svensson, P.; Clyne, N. Randomized Controlled Trial of Exercise in CKD—The RENEXC Study. Kidney Int. Rep. 2019, 4, 963–976. [Google Scholar] [CrossRef]
- Yuguero-Ortiz, A.; Gomez, M.; Arias-Guillén, M.; Ojeda, R.; Fontseré, N.; Rodas, L.; Jesús Broseta, J.; Vera, M.; Hernandez-Sanchez, S.; Maduell, F. Impact and Safety Outcomes of an Intradialytic Physical Exercise Program. Nefrología 2021, 41, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Junqué-Jiménez, A.; Esteve-Simó, V.; Andreu-Periz, L.; Segura-Ortí, E. A Nurse-Led Home-Based Exercise Program for Patients with Chronic Kidney Disease. Worldviews Evid. Based Nurs. 2023, 20, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Isoyama, N.; Qureshi, A.R.; Avesani, C.M.; Lindholm, B.; Bárány, P.; Heimbürger, O.; Cederholm, T.; Stenvinkel, P.; Carrero, J.J. Comparative Associations of Muscle Mass and Muscle Strength with Mortality in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.C.; Bufarah, M.N.B.; Balbi, A.L. Handgrip Strength in End Stage of Renal Disease—A Narrative Review. Nutrire 2018, 43, 14. [Google Scholar] [CrossRef]
- Hwang, S.H.; Lee, D.H.; Min, J.; Jeon, J.Y. Handgrip Strength as a Predictor of All-Cause Mortality in Patients With Chronic Kidney Disease Undergoing Dialysis: A Meta-Analysis of Prospective Cohort Studies. J. Ren. Nutr. 2019, 29, 471–479. [Google Scholar] [CrossRef]
- Desai, M.; Mohamed, A.; Davenport, A. A Pilot Study Investigating the Effect of Pedalling Exercise during Dialysis on 6-Min Walking Test and Hand Grip and Pinch Strength. Int. J. Artif. Organs 2019, 42, 161–166. [Google Scholar] [CrossRef]
- Krase, A.A.; Terzis, G.; Giannaki, C.D.; Stasinaki, A.N.; Wilkinson, T.J.; Smith, A.C.; Zorz, C.; Karatzaferi, C.; Stefanidis, I.; Sakkas, G.K. Seven Months of Aerobic Intradialytic Exercise Training Can Prevent Muscle Loss in Haemodialysis Patients: An Ultrasonography Study. Int. Urol. Nephrol. 2022, 54, 447–456. [Google Scholar] [CrossRef]
- Bogataj, Š.; Pajek, J.; Buturović Ponikvar, J.; Pajek, M. Functional Training Added to Intradialytic Cycling Lowers Low-Density Lipoprotein Cholesterol and Improves Dialysis Adequacy: A Randomized Controlled Trial. BMC Nephrol. 2020, 21, 352. [Google Scholar] [CrossRef]
- Bučar Pajek, M.; Pajek, J. Characterization of Deficits across the Spectrum of Motor Abilities in Dialysis Patients and the Impact of Sarcopenic Overweight and Obesity. Clin. Nutr. 2018, 37, 870–877. [Google Scholar] [CrossRef]
- Shirai, N.; Yamamoto, S.; Osawa, Y.; Tsubaki, A.; Morishita, S.; Narita, I. Dysfunction in Dynamic, but Not Static Balance Is Associated with Risk of Accidental Falls in Hemodialysis Patients: A Prospective Cohort Study. BMC Nephrol. 2022, 23, 237. [Google Scholar] [CrossRef]
- Liu, X.; Chen, S.; Liu, C.; Dang, X.; Wei, M.; Xin, X.; Gao, J. Novel Risk-Factor Analysis and Risk-Evaluation Model of Falls in Patients Receiving Maintenance Hemodialysis. Ren. Fail. 2023, 45, 2182608. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-Leg Balance Is an Important Predictor of Injurious Falls in Older Persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Wong-Yu, I.S.K.; Mak, M.K.Y. Effects of Exercise on Falls, Balance, and Gait Ability in Parkinson’s Disease: A Meta-Analysis. Neurorehabilit. Neural Repair 2016, 30, 512–527. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Bo, L.; Zhu, H.; Chen, B.; Wu, Z.; Du, H.; Huo, X. Effects of Lower Limb Resistance Exercise on Muscle Strength, Physical Fitness, and Metabolism in Pre-Frail Elderly Patients: A Randomized Controlled Trial. BMC Geriatr. 2021, 21, 447. [Google Scholar] [CrossRef] [PubMed]
- Perneczky, R. Dementia Treatment versus Prevention. Dialogues Clin. Neurosci. 2022, 21, 43–51. [Google Scholar] [CrossRef]
- Patel, M.; Dasgupta, I.; Tadros, G.; Baharani, J. Cognitive Impairment in Hemodialysis Patients: What Can Slow This Decline? Hong Kong J. Nephrol. 2016, 18, 4–10. [Google Scholar] [CrossRef]
- Harciarek, M.; Biedunkiewicz, B.; Lichodziejewska-Niemierko, M.; Dȩbska-Ślizie, A.; Rutkowski, B. Continuous Cognitive Improvement 1 Year Following Successful Kidney Transplant. Kidney Int. 2011, 79, 1353–1360. [Google Scholar] [CrossRef]
- Pickett, J.L.; Theberge, D.C.; Brown, W.S.; Schweitzer, S.U.; Nissenson, A.R. Normalizing Hematocrit in Dialysis Patients Improves Brain Function. Am. J. Kidney Dis. 1999, 33, 1122–1130. [Google Scholar] [CrossRef]
- Sharp, J.; Wild, M.R.; Gumley, A.I.; Deighan, C.J. A Cognitive Behavioral Group Approach to Enhance Adherence to Hemodialysis Fluid Restrictions: A Randomized Controlled Trial. Am. J. Kidney Dis. 2005, 45, 1046–1057. [Google Scholar] [CrossRef]
- Jassal, S.V.; Devins, G.M.; Chan, C.T.; Bozanovic, R.; Rourke, S. Improvements in Cognition in Patients Converting from Thrice Weekly Hemodialysis to Nocturnal Hemodialysis: A Longitudinal Pilot Study. Kidney Int. 2006, 70, 956–962. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Experimental Group (n = 22) | Control Group (n = 21) | All Participants (n = 44) | |
|---|---|---|---|
| Male sex (%) | 54% | 77% | 66% |
| Age (years) | 65.7 ± 9.7 | 67.2 ± 12.5 | 66.5 ± 11.0 |
| Height (cm) | 169.6 ± 12.5 | 171.0 ± 10.5 | 170.3 ± 11.4 |
| Weight (kg) | 77.1 ± 21.9 | 74.2 ± 14.3 | 75.6 ± 18.3 |
| BMI (kg/m2) | 26.8 ± 6.0 | 24.9 ± 3.8 | 25.9 ± 5.1 |
| Heart rate (bpm) | 72.7 ± 10.4 | 72.8 ± 15.1 | 72.8 ± 12.7 |
| Systolic blood pressure (mm Hg) | 160 ± 22 | 151 ± 22 | 156 ± 22 |
| Diastolic blood pressure (mm Hg) | 88 ± 13 | 85 ± 9 | 87 ± 11 |
| Fat tissue index (kg/m2) | 14.6 ± 6.6 | 12.4 ± 4.0 | 13.5 ± 5.5 |
| Experimental Group (n = 22) | |
|---|---|
| Intradialytic cycling | 79.9% |
| Cycling time (min/session) | 37.6 |
| Cognitive training | 84.2% |
| Cognitive training (min/session) | 30 |
| Experimental (n = 22) | Control (n = 21) | Time × Group | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 12 Weeks | Baseline | 12 Weeks | F | p | η2 | |
| 10 STS (s) | 24.3 ± 6.6 | 22.8 ± 6.3 | 25.4 ± 7.3 | 25.5 ± 7.3 | 1.5 | 0.227 | 0.035 |
| HGS (kg) | 31.3 ± 8.2 | 30.8 ± 8.8 | 32.4 ± 9.5 | 30.6 ± 9.5 | 4.0 | 0.051 | 0.091 |
| Stork test (s) | 1.9 ± 1.4 | 3.2 ± 2.4 | 2.4 ± 2.2 | 2.6 ± 3.5 | 3.0 | 0.089 | 0.069 |
| Experimental (n = 22) | Control (n = 21) | Time × Group | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 12 Weeks | Baseline | 12 Weeks | F | p | η2 | |
| MoCA test | 25.0 ± 2.7 | 27.3 ± 2.3 | 24.2 ± 3.0 | 24.7 ± 3.5 | 14.8 | <0.001 | 0.266 |
| SDMT test | 27.5 ± 11.6 | 28.5 ± 11.8 | 27.8 ± 12.4 | 27.5 ± 12.6 | 14.9 | <0.001 | 0.267 |
| Adverse Event | Experimental Group (n) | Comments |
|---|---|---|
| Hypotension episodes | 3 | Three patients presented hypotension after a cycling session. |
| Dyspnea | 1 | One patient could not perform the cycling session due to dyspnea unrelated to exercise. |
| Hypertension episodes | 3 | Three patients could not perform the cycling session due to hypertension unrelated to exercise. |
| Vascular access hematoma | 3 | Three patients could not perform the cycling session due to hematoma unrelated to exercise. |
| Fatigue episodes | 7 | Seven patients could not perform the cycling session due to fatigue unrelated to exercise. |
| Joint pain | 4 | Four patients could not perform the cycling session due to knee or hip pain unrelated to exercise. |
| Infection | 4 | Three patients missed a few exercise and cognitive sessions due to COVID-19 infection and one due to influenza infection. |
| Vacation | 2 | Two patients missed a few exercise and cognitive sessions due to vacation. |
| MACE | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kren, A.; Bogataj, Š. The Impact of Intradialytic Cognitive and Physical Training Program on the Physical and Cognitive Abilities in End-Stage Kidney Disease Patients: A Randomized Clinical Controlled Trial. Brain Sci. 2023, 13, 1228. https://doi.org/10.3390/brainsci13081228
Kren A, Bogataj Š. The Impact of Intradialytic Cognitive and Physical Training Program on the Physical and Cognitive Abilities in End-Stage Kidney Disease Patients: A Randomized Clinical Controlled Trial. Brain Sciences. 2023; 13(8):1228. https://doi.org/10.3390/brainsci13081228
Chicago/Turabian StyleKren, Aljaž, and Špela Bogataj. 2023. "The Impact of Intradialytic Cognitive and Physical Training Program on the Physical and Cognitive Abilities in End-Stage Kidney Disease Patients: A Randomized Clinical Controlled Trial" Brain Sciences 13, no. 8: 1228. https://doi.org/10.3390/brainsci13081228
APA StyleKren, A., & Bogataj, Š. (2023). The Impact of Intradialytic Cognitive and Physical Training Program on the Physical and Cognitive Abilities in End-Stage Kidney Disease Patients: A Randomized Clinical Controlled Trial. Brain Sciences, 13(8), 1228. https://doi.org/10.3390/brainsci13081228