

International Trends in Lithium Use for Pharmacotherapy and Clinical Correlates in Bipolar Disorder: A Scoping Review


Abstract
:1. Introduction
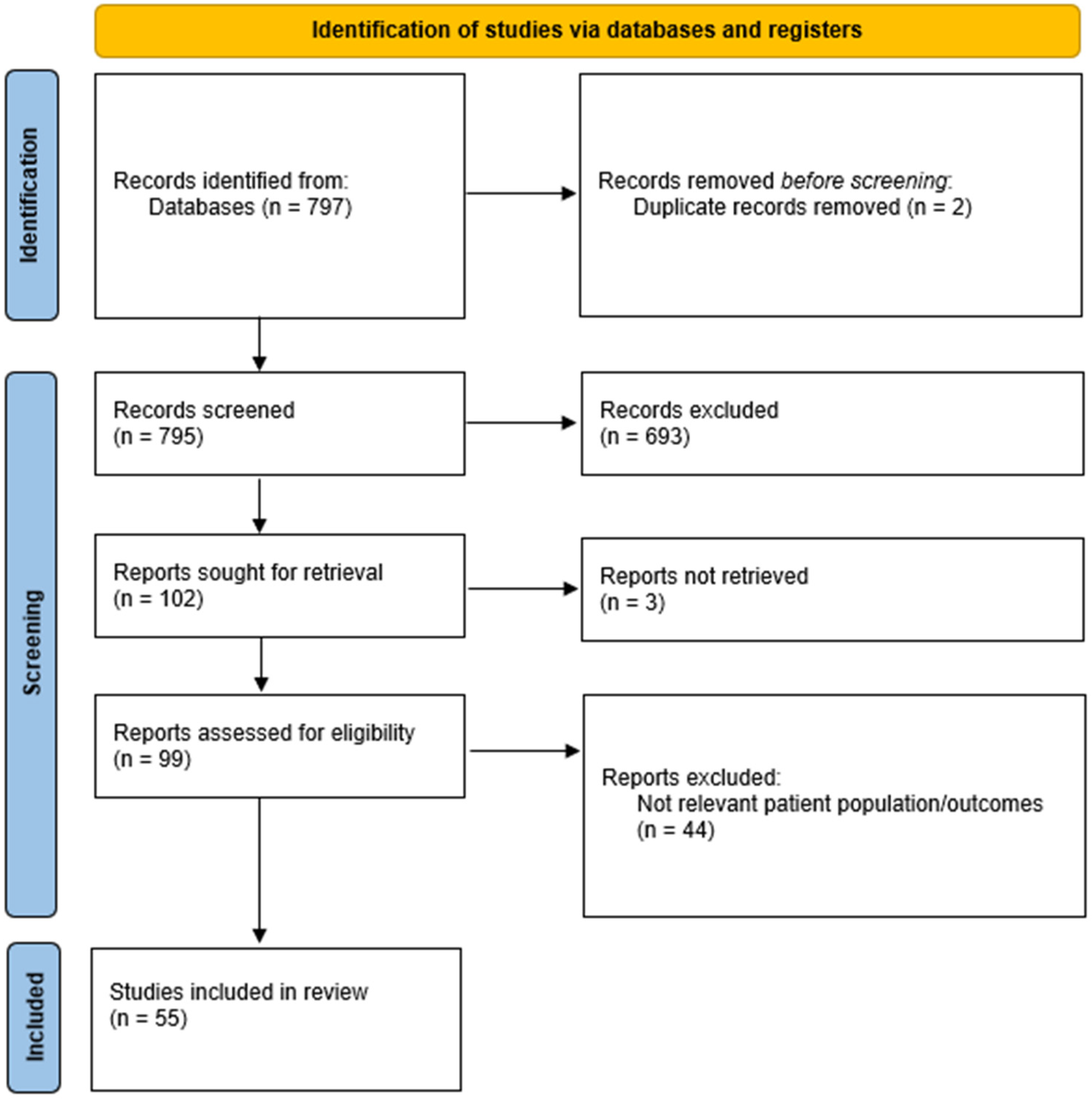
2. Materials and Methods
3. Results
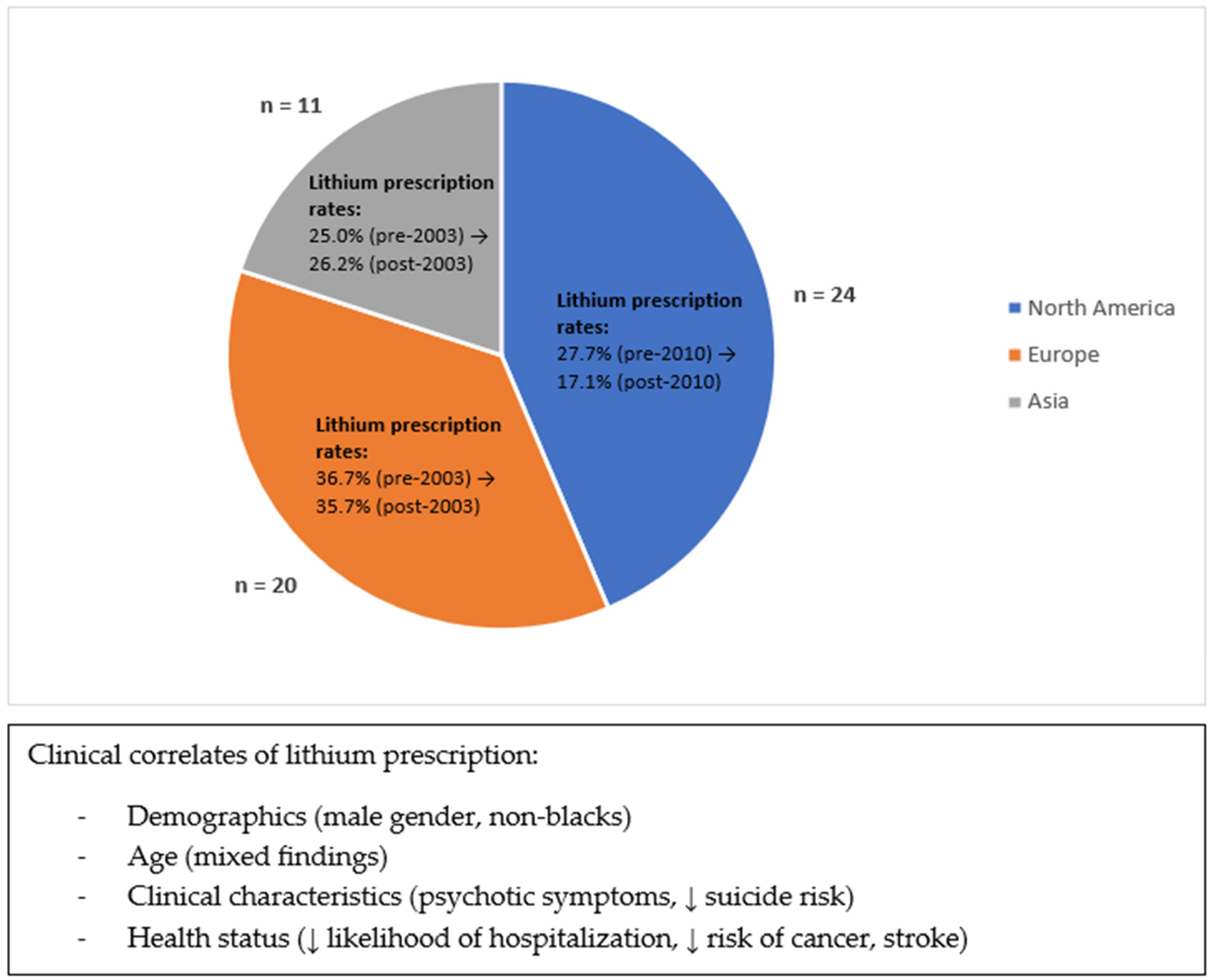
3.1. By Region
3.2. By Time
3.3. By Special Demographics
3.4. By Clinical Setting
3.5. By Treatment Regimen
3.6. Clinical Correlates of Lithium Prescription
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Goes, F.S. Diagnosis and Management of Bipolar Disorders. BMJ 2023, 381, e073591. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.R.; Jin, R.; He, J.-P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and Correlates of Bipolar Spectrum Disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.F.; Firth, J.; Vieta, E. Bipolar Disorder. N. Engl. J. Med. 2020, 383, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Grande, I.; Berk, M.; Birmaher, B.; Vieta, E. Bipolar Disorder. Lancet 2016, 387, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Plans, L.; Barrot, C.; Nieto, E.; Rios, J.; Schulze, T.G.; Papiol, S.; Mitjans, M.; Vieta, E.; Benabarre, A. Association between Completed Suicide and Bipolar Disorder: A Systematic Review of the Literature. J. Affect. Disord. 2019, 242, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Dembek, C.; de Mauri, M.; Modi, K.; Zhu, Y.; Niu, X.; Grinnell, T. The Economic and Humanistic Burden of Bipolar Disorder in Adults in the United States. Ann. Gen. Psychiatry 2023, 22, 13. [Google Scholar] [CrossRef]
- Geddes, J.R.; Miklowitz, D.J. Treatment of Bipolar Disorder. Lancet 2013, 381, 1672–1682. [Google Scholar] [CrossRef]
- Nestsiarovich, A.; Gaudiot, C.E.S.; Baldessarini, R.J.; Vieta, E.; Zhu, Y.; Tohen, M. Preventing New Episodes of Bipolar Disorder in Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2022, 54, 75–89. [Google Scholar] [CrossRef]
- Emamghoreishi, M.; Keshavarz, M.; Nekooeian, A.A. Acute and Chronic Effects of Lithium on BDNF and GDNF mRNA and Protein Levels in Rat Primary Neuronal, Astroglial and Neuroastroglia Cultures. Iran. J. Basic Med. Sci. 2015, 18, 240–246. [Google Scholar]
- Cunha, A.B.M.; Frey, B.N.; Andreazza, A.C.; Goi, J.D.; Rosa, A.R.; Gonçalves, C.A.; Santin, A.; Kapczinski, F. Serum Brain-Derived Neurotrophic Factor Is Decreased in Bipolar Disorder during Depressive and Manic Episodes. Neurosci. Lett. 2006, 398, 215–219. [Google Scholar] [CrossRef]
- Machado-Vieira, R.; Dietrich, M.O.; Leke, R.; Cereser, V.H.; Zanatto, V.; Kapczinski, F.; Souza, D.O.; Portela, L.V.; Gentil, V. Decreased Plasma Brain Derived Neurotrophic Factor Levels in Unmedicated Bipolar Patients during Manic Episode. Biol. Psychiatry 2007, 61, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Benard, V.; Vaiva, G.; Masson, M.; Geoffroy, P.A. Lithium and Suicide Prevention in Bipolar Disorder. L’Encephale 2016, 42, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Tohen, M.; Zarate, C.A. Lithium Treatment of Bipolar Disorder in Adults: A Systematic Review of Randomized Trials and Meta-Analyses. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2022, 54, 100–115. [Google Scholar] [CrossRef] [PubMed]
- Karanti, A.; Kardell, M.; Lundberg, U.; Landén, M. Changes in Mood Stabilizer Prescription Patterns in Bipolar Disorder. J. Affect. Disord. 2016, 195, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Kessing, L.V.; Vradi, E.; Andersen, P.K. Nationwide and Population-Based Prescription Patterns in Bipolar Disorder. Bipolar Disord. 2016, 18, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.J.; Leahy, L.; Arcona, S.; Gause, D.; Zhang, W.; Hennen, J. Patterns of Psychotropic Drug Prescription for U.S. Patients with Diagnoses of Bipolar Disorders. Psychiatr. Serv. Wash. 2007, 58, 85–91. [Google Scholar] [CrossRef]
- Bohlken, J.; Bauer, M.; Kostev, K. Drug Treatment for Patients with Bipolar Disorders in Psychiatric Practices in Germany in 2009 and 2018. Psychiatry Res. 2020, 289, 112965. [Google Scholar] [CrossRef]
- Greene, M.; Paladini, L.; Lemmer, T.; Piedade, A.; Touya, M.; Clark, O. Systematic Literature Review on Patterns of Pharmacological Treatment and Adherence among Patients with Bipolar Disorder Type I in the USA. Neuropsychiatr. Dis. Treat. 2018, 14, 1545–1559. [Google Scholar] [CrossRef]
- Blanco, C.; Laje, G.; Olfson, M.; Marcus, S.C.; Pincus, H.A. Trends in the Treatment of Bipolar Disorder by Outpatient Psychiatrists. Am. J. Psychiatry 2002, 159, 1005–1010. [Google Scholar] [CrossRef]
- Hooshmand, F.; Miller, S.; Dore, J.; Wang, P.W.; Hill, S.J.; Portillo, N.; Ketter, T.A. Trends in Pharmacotherapy in Patients Referred to a Bipolar Specialty Clinic, 2000–2011. J. Affect. Disord. 2014, 155, 283–287. [Google Scholar] [CrossRef]
- Gitlin, M. Lithium Side Effects and Toxicity: Prevalence and Management Strategies. Int. J. Bipolar Disord. 2016, 4, 27. [Google Scholar] [CrossRef]
- Baldessarini, R.J. Chemotherapy in Psychiatry; Springer: New York, NY, USA, 2013; ISBN 978-1-4614-7926-0. [Google Scholar]
- Mandal, S.; Mamidipalli, S.S.; Mukherjee, B.; Hara, S.K.H. Perspectives, Attitude, and Practice of Lithium Prescription among Psychiatrists in India. Indian J. Psychiatry 2019, 61, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Pérez de Mendiola, X.; Hidalgo-Mazzei, D.; Vieta, E.; González-Pinto, A. Overview of Lithium’s Use: A Nationwide Survey. Int. J. Bipolar Disord. 2021, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, M.R.; Goldfield, M. Cardiovascular Malformations with Lithium Use during Pregnancy. Am. J. Psychiatry 1975, 132, 529–531. [Google Scholar] [CrossRef]
- Nguyen, H.T.T.; Sharma, V.; McIntyre, R.S. Teratogenesis Associated with Antibipolar Agents. Adv. Ther. 2009, 26, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Diav-Citrin, O.; Shechtman, S.; Tahover, E.; Finkel-Pekarsky, V.; Arnon, J.; Kennedy, D.; Erebara, A.; Einarson, A.; Ornoy, A. Pregnancy Outcome Following in Utero Exposure to Lithium: A Prospective, Comparative, Observational Study. Am. J. Psychiatry 2014, 171, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.J. Psychotropic Medication during Pregnancy and Lactation. Arch. Gynecol. Obstet. 2008, 277, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.M.; Gundlapalli, S.P.; Ryan, W.G.; Ryals, T.; Passman, T.E. Effects of Antimanic Mood-Stabilizing Drugs on Fetuses, Neonates, and Nursing Infants. South. Med. J. 2001, 94, 304–322. [Google Scholar] [CrossRef]
- Lähteenvuo, M.; Paljärvi, T.; Tanskanen, A.; Taipale, H.; Tiihonen, J. Real-World Effectiveness of Pharmacological Treatments for Bipolar Disorder: Register-Based National Cohort Study. Br. J. Psychiatry J. Ment. Sci. 2023, 223, 456–464. [Google Scholar] [CrossRef]
- Singh, B.; Yocum, A.K.; Strawbridge, R.; Burdick, K.E.; Millett, C.E.; Peters, A.T.; Sperry, S.H.; Fico, G.; Vieta, E.; Verdolini, N.; et al. Patterns of Pharmacotherapy for Bipolar Disorder: A GBC Survey. Bipolar Disord. 2023, 1–11. [Google Scholar] [CrossRef]
- Lin, C.-H.; Chan, H.-Y.; Lin, H.-Y.; Chen, C.-C. Fourteen-Year Trends in the Prescribing Patterns of Pediatric Bipolar Patients Discharged from Two Public Mental Hospitals in Taiwan. Asia-Pac. Psychiatry Off. J. Pac. Rim Coll. Psychiatr. 2023, 15, e12525. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, M.; Yasui-Furukori, N.; Adachi, N.; Ueda, H.; Hongo, S.; Azekawa, T.; Kubota, Y.; Katsumoto, E.; Edagawa, K.; Goto, E.; et al. Differences in Prescription Patterns between Real-World Outpatients with Bipolar I and II Disorders in the MUSUBI Survey. Asian J. Psychiatry 2022, 67, 102935. [Google Scholar] [CrossRef] [PubMed]
- Uwai, Y.; Nabekura, T. Relationship between Lithium Carbonate and the Risk of Parkinson-like Events in Patients with Bipolar Disorders: A Multivariate Analysis Using the Japanese Adverse Drug Event Report Database. Psychiatry Res. 2022, 314, 114687. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.W.S.; Man, K.K.C.; Gao, L.; Chan, E.W.; Lee, E.H.M.; Hayes, J.F.; Wong, I.C.K. Bipolar Disorder Prevalence and Psychotropic Medication Utilisation in Hong Kong and the United Kingdom. Pharmacoepidemiol. Drug Saf. 2021, 30, 1588–1600. [Google Scholar] [CrossRef] [PubMed]
- Prillo, J.; Soh, J.F.; Park, H.; Beaulieu, S.; Linnaranta, O.; Rej, S. Obesity and Metabolic Comorbidity in Bipolar Disorder: Do Patients on Lithium Comprise a Subgroup? A Naturalistic Study. BMC Psychiatry 2021, 21, 558. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Avasthi, A.; Chakravarty, R.; Dan, A.; Chakraborty, K.; Neogi, R.; Desouza, A.; Nayak, O.; Praharaj, S.K.; Menon, V.; et al. Prescription Patterns in Clinically Stable Patients with Bipolar Disorder: Findings from the Bipolar Disorder Course and Outcome from India (BiD-CoIN) Study. Asian J. Psychiatry 2021, 57, 102549. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Mojtabai, R.; Goes, F.S.; Zandi, P.P. Trends in Prescriptions of Lithium and Other Medications for Patients with Bipolar Disorder in Office-Based Practices in the United States: 1996–2015. J. Affect. Disord. 2020, 276, 883–889. [Google Scholar] [CrossRef]
- Karanti, A.; Kardell, M.; Joas, E.; Runeson, B.; Pålsson, E.; Landén, M. Characteristics of Bipolar I and II Disorder: A Study of 8766 Individuals. Bipolar Disord. 2020, 22, 392–400. [Google Scholar] [CrossRef]
- Salazar de Pablo, G.; Guinart, D.; Cornblatt, B.A.; Auther, A.M.; Carrión, R.E.; Carbon, M.; Jiménez-Fernández, S.; Vernal, D.L.; Walitza, S.; Gerstenberg, M.; et al. Demographic and Clinical Characteristics, Including Subsyndromal Symptoms Across Bipolar-Spectrum Disorders in Adolescents. J. Child Adolesc. Psychopharmacol. 2020, 30, 222–234. [Google Scholar] [CrossRef]
- Rhee, T.G.; Olfson, M.; Nierenberg, A.A.; Wilkinson, S.T. 20-Year Trends in the Pharmacologic Treatment of Bipolar Disorder by Psychiatrists in Outpatient Care Settings. Am. J. Psychiatry 2020, 177, 706–715. [Google Scholar] [CrossRef]
- Lyall, L.M.; Penades, N.; Smith, D.J. Changes in Prescribing for Bipolar Disorder between 2009 and 2016: National-Level Data Linkage Study in Scotland. Br. J. Psychiatry J. Ment. Sci. 2019, 215, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Musetti, L.; Tundo, A.; Benedetti, A.; Massimetti, G.; Cambiali, E.; Pergentini, I.; Del Grande, C.; Dell’Osso, L. Lithium, Valproate, and Carbamazepine Prescribing Patterns for Long-Term Treatment of Bipolar I and II Disorders: A Prospective Study. Hum. Psychopharmacol. 2018, 33, e2676. [Google Scholar] [CrossRef] [PubMed]
- Jaracz, J.; Rudnicka, E.T.; Bierejszyk, M.; Witczyk, K.; Raczyńska, A.; Nowak, W.; Pisarczyk, A.; Woźniak, K.; Czernaś, W.; Moniakowski, A.; et al. The Pattern of Pharmacological Treatment of Bipolar Patients Discharged from Psychiatric Units in Poland. Pharmacol. Rep. 2018, 70, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Broeks, S.C.; Thisted Horsdal, H.; Glejsted Ingstrup, K.; Gasse, C. Psychopharmacological Drug Utilization Patterns in Pregnant Women with Bipolar Disorder—A Nationwide Register-Based Study. J. Affect. Disord. 2017, 210, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Rej, S.; Herrmann, N.; Shulman, K.; Fischer, H.D.; Fung, K.; Gruneir, A. Current Psychotropic Medication Prescribing Patterns in Late-Life Bipolar Disorder. Int. J. Geriatr. Psychiatry 2017, 32, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.S.; Miller, C.J.; Li, M.; Bajor, L.A.; Lee, A. A Population-Based Study of the Comparative Effectiveness of Second-Generation Antipsychotics vs Older Antimanic Agents in Bipolar Disorder. Bipolar Disord. 2016, 18, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.-Y.; Hsieh, K.-P.; Huang, W.-W.; Yang, Y.-H. Use of Lithium and Cancer Risk in Patients with Bipolar Disorder: Population-Based Cohort Study. Br. J. Psychiatry J. Ment. Sci. 2016, 209, 393–399. [Google Scholar] [CrossRef]
- Chang, C.-M.; Wu, C.-S.; Huang, Y.-W.; Chau, Y.-L.; Tsai, H.-J. Utilization of Psychopharmacological Treatment Among Patients With Newly Diagnosed Bipolar Disorder From 2001 to 2010. J. Clin. Psychopharmacol. 2016, 36, 32–44. [Google Scholar] [CrossRef]
- Arıkan, M.K.; Poyraz, C.A.; Baş, A.; Sağlam, N.G.U.; Batun, G.C.; Gültekin, G.; Poyraz, B.Ç. Changing Trends in Treatment of Acute Mania: Experience of a Tertiary Centre Over a Decade. Psychiatr. Q. 2016, 87, 305–313. [Google Scholar] [CrossRef]
- Kleimann, A.; Schrader, V.; Stübner, S.; Greil, W.; Kahl, K.G.; Bleich, S.; Grohmann, R.; Frieling, H.; Toto, S. Psychopharmacological Treatment of 1650 In-Patients with Acute Mania-Data from the AMSP Study. J. Affect. Disord. 2016, 191, 164–171. [Google Scholar] [CrossRef]
- Carlborg, A.; Ferntoft, L.; Thuresson, M.; Bodegard, J. Population Study of Disease Burden, Management, and Treatment of Bipolar Disorder in Sweden: A Retrospective Observational Registry Study. Bipolar Disord. 2015, 17, 76–85. [Google Scholar] [CrossRef]
- Lan, C.-C.; Liu, C.-C.; Lin, C.-H.; Lan, T.-Y.; McInnis, M.G.; Chan, C.-H.; Lan, T.-H. A Reduced Risk of Stroke with Lithium Exposure in Bipolar Disorder: A Population-Based Retrospective Cohort Study. Bipolar Disord. 2015, 17, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Toffol, E.; Hätönen, T.; Tanskanen, A.; Lönnqvist, J.; Wahlbeck, K.; Joffe, G.; Tiihonen, J.; Haukka, J.; Partonen, T. Lithium is Associated with Decrease in All-Cause and Suicide Mortality in High-Risk Bipolar Patients: A Nationwide Registry-Based Prospective Cohort Study. J. Affect. Disord. 2015, 183, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Karanti, A.; Bobeck, C.; Osterman, M.; Kardell, M.; Tidemalm, D.; Runeson, B.; Lichtenstein, P.; Landén, M. Gender Differences in the Treatment of Patients with Bipolar Disorder: A Study of 7354 Patients. J. Affect. Disord. 2015, 174, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.H.; Ha, K.; Yatham, L.N.; Chang, J.S.; Ha, T.H.; Jeon, H.J.; Hong, K.S.; Chang, S.M.; Ahn, Y.M.; Cho, H.S.; et al. Pattern of Pharmacotherapy by Episode Types for Patients with Bipolar Disorders and Its Concordance with Treatment Guidelines. J. Clin. Psychopharmacol. 2014, 34, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Ko, A.; Swampillai, B.; Timmins, V.; Scavone, A.; Collinger, K.; Goldstein, B.I. Clinical Characteristics Associated with Lithium Use among Adolescents with Bipolar Disorder. J. Child Adolesc. Psychopharmacol. 2014, 24, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Grande, I.; de Arce, R.; Jiménez-Arriero, M.Á.; Lorenzo, F.G.I.; Valverde, J.I.F.; Balanzá-Martínez, V.; Zaragoza, S.; Cobaleda, S.; Vieta, E.; SIN-DEPRES Group. Patterns of Pharmacological Maintenance Treatment in a Community Mental Health Services Bipolar Disorder Cohort Study (SIN-DEPRES). Int. J. Neuropsychopharmacol. 2013, 16, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, J.K.; Sareen, H.; Yadav, V.S.; Rai, S.B. Prescription Pattern of Mood Stabilizers for Bipolar Disorder at a Tertiary Health Care Centre in North India. Indian J. Psychiatry 2013, 55, 131–134. [Google Scholar] [CrossRef]
- Haeberle, A.; Greil, W.; Russmann, S.; Grohmann, R. Mono- and Combination Drug Therapies in Hospitalized Patients with Bipolar Depression. Data from the European Drug Surveillance Program AMSP. BMC Psychiatry 2012, 12, 153. [Google Scholar] [CrossRef]
- Greil, W.; Häberle, A.; Haueis, P.; Grohmann, R.; Russmann, S. Pharmacotherapeutic Trends in 2231 Psychiatric Inpatients with Bipolar Depression from the International AMSP Project between 1994 and 2009. J. Affect. Disord. 2012, 136, 534–542. [Google Scholar] [CrossRef]
- Walpoth-Niederwanger, M.; Kemmler, G.; Grunze, H.; Weiss, U.; Hörtnagl, C.; Strauss, R.; Blasko, I.; Hausmann, A. Treatment Patterns in Inpatients with Bipolar Disorder at a Psychiatric University Hospital over a 9-Year Period: Focus on Mood Stabilizers. Int. Clin. Psychopharmacol. 2012, 27, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Dusetzina, S.B.; Gaynes, B.N.; Weinberger, M.; Farley, J.F.; Sleath, B.; Hansen, R.A. Receipt of Guideline-Concordant Pharmacotherapy among Children with New Diagnoses of Bipolar Disorder. Psychiatr. Serv. Wash. 2011, 62, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Post, R.M.; Leverich, G.S.; Altshuler, L.L.; Frye, M.A.; Suppes, T.; Keck, P.E.; McElroy, S.L.; Nolen, W.A.; Kupka, R.; Grunze, H.; et al. Differential Clinical Characteristics, Medication Usage, and Treatment Response of Bipolar Disorder in the US versus The Netherlands and Germany. Int. Clin. Psychopharmacol. 2011, 26, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Porsdal, V.; Aarre, T.F.; Koponen, H.J.; Aarnio, J.; Kleivenes, O.K. Emblem Advisory Board Mania in the Nordic Countries: Patients and Treatment in the Acute Phase of the EMBLEM Study. Nord. J. Psychiatry 2009, 63, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Jerrell, J.M. Pharmacotherapy in the Community-Based Treatment of Children with Bipolar I Disorder. Hum. Psychopharmacol. 2008, 23, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Baldessarini, R.; Henk, H.; Sklar, A.; Chang, J.; Leahy, L. Psychotropic Medications for Patients with Bipolar Disorder in the United States: Polytherapy and Adherence. Psychiatr. Serv. Wash. 2008, 59, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Al Jurdi, R.K.; Marangell, L.B.; Petersen, N.J.; Martinez, M.; Gyulai, L.; Sajatovic, M. Prescription Patterns of Psychotropic Medications in Elderly Compared to Younger Participants Who Achieved a “Recovered” Status in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2008, 16, 922–933. [Google Scholar] [CrossRef] [PubMed]
- Wolfsperger, M.; Greil, W.; Rössler, W.; Grohmann, R. Pharmacological Treatment of Acute Mania in Psychiatric In-Patients between 1994 and 2004. J. Affect. Disord. 2007, 99, 9–17. [Google Scholar] [CrossRef]
- Baldessarini, R.J.; Tondo, L.; Davis, P.; Pompili, M.; Goodwin, F.K.; Hennen, J. Decreased Risk of Suicides and Attempts during Long-Term Lithium Treatment: A Meta-Analytic Review. Bipolar Disord. 2006, 8, 625–639. [Google Scholar] [CrossRef]
- Kilbourne, A.M.; Pincus, H.A. Patterns of Psychotropic Medication Use by Race among Veterans with Bipolar Disorder. Psychiatr. Serv. Wash. 2006, 57, 123–126. [Google Scholar] [CrossRef]
- Sajatovic, M.; Blow, F.C.; Ignacio, R.V.; Kales, H.C. Age-Related Modifiers of Clinical Presentation and Health Service Use among Veterans with Bipolar Disorder. Psychiatr. Serv. Wash. 2004, 55, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Bhangoo, R.K.; Lowe, C.H.; Myers, F.S.; Treland, J.; Curran, J.; Towbin, K.E.; Leibenluft, E. Medication Use in Children and Adolescents Treated in the Community for Bipolar Disorder. J. Child Adolesc. Psychopharmacol. 2003, 13, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.; Chengappa, K.N.; Brar, J.S.; Gershon, S.; Yablonsky, E.; Stapf, D.; Kupfer, D.J. Psychotropic Drug Prescription Patterns among Patients with Bipolar I Disorder. Bipolar Disord. 2000, 2, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Unützer, J.; Simon, G.; Pabiniak, C.; Bond, K.; Katon, W. The Treated Prevalence of Bipolar Disorder in a Large Staff-Model HMO. Psychiatr. Serv. Wash. 1998, 49, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Sajatovic, M.; Gerhart, C.; Semple, W. Association between Mood-Stabilizing Medication and Mental Health Resource Use in the Management of Acute Mania. Psychiatr. Serv. Wash. 1997, 48, 1037–1041. [Google Scholar] [CrossRef]
- Chou, J.C.; Zito, J.M.; Vitrai, J.; Craig, T.J.; Allingham, B.H.; Czobor, P. Neuroleptics in Acute Mania: A Pharmacoepidemiologic Study. Ann. Pharmacother. 1996, 30, 1396–1398. [Google Scholar] [CrossRef] [PubMed]
- Fenn, H.H.; Robinson, D.; Luby, V.; Dangel, C.; Buxton, E.; Beattie, M.; Kraemer, H.; Yesavage, J.A. Trends in Pharmacotherapy of Schizoaffective and Bipolar Affective Disorders: A 5-Year Naturalistic Study. Am. J. Psychiatry 1996, 153, 711–713. [Google Scholar] [CrossRef] [PubMed]
- Sajatovic, M.; Popli, A.; Semple, W. Ten-Year Use of Hospital-Based Services by Geriatric Veterans with Schizophrenia and Bipolar Disorder. Psychiatr. Serv. Wash. 1996, 47, 961–965. [Google Scholar] [CrossRef]
- Hes, J.P. Lithium Therapy in Israel. Acta Psychiatr. Scand. 1976, 54, 333–335. [Google Scholar] [CrossRef]
- Etain, B.; Lajnef, M.; Bellivier, F.; Mathieu, F.; Raust, A.; Cochet, B.; Gard, S.; M’Bailara, K.; Kahn, J.-P.; Elgrabli, O.; et al. Clinical Expression of Bipolar Disorder Type I as a Function of Age and Polarity at Onset: Convergent Findings in Samples from France and the United States. J. Clin. Psychiatry 2012, 73, e561–e566. [Google Scholar] [CrossRef]
- Connolly, K.R.; Thase, M.E. The Clinical Management of Bipolar Disorder: A Review of Evidence-Based Guidelines. Prim. Care Companion CNS Disord. 2011, 13, PCC.10r01097. [Google Scholar] [CrossRef] [PubMed]
- Pillarella, J.; Higashi, A.; Alexander, G.C.; Conti, R. Trends in Use of Second-Generation Antipsychotics for Treatment of Bipolar Disorder in the United States, 1998–2009. Psychiatr. Serv. Wash. 2012, 63, 83–86. [Google Scholar] [CrossRef]
- Miller, C.J.; Li, M.; Penfold, R.B.; Lee, A.F.; Smith, E.G.; Osser, D.N.; Bajor, L.; Bauer, M.S. Patterns of Initiation of Second Generation Antipsychotics for Bipolar Disorder: A Month-by-Month Analysis of Provider Behavior. BMC Psychiatry 2014, 14, 339. [Google Scholar] [CrossRef] [PubMed]
- Bowden, C.L.; Grunze, H.; Mullen, J.; Brecher, M.; Paulsson, B.; Jones, M.; Vågerö, M.; Svensson, K. A Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Study of Quetiapine or Lithium as Monotherapy for Mania in Bipolar Disorder. J. Clin. Psychiatry 2005, 66, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Sanchez-Moreno, J. Acute and Long-Term Treatment of Mania. Dialogues Clin. Neurosci. 2008, 10, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Malhi, G.S.; Bell, E.; Hamilton, A.; Morris, G.; Gitlin, M. Lithium Mythology. Bipolar Disord. 2021, 23, 7–10. [Google Scholar] [CrossRef]
- Kessing, L.V. Lithium as the Drug of Choice for Maintenance Treatment in Bipolar Disorder. Acta Psychiatr. Scand. 2019, 140, 91–93. [Google Scholar] [CrossRef]
- Yatham, L.N.; Kennedy, S.H.; Parikh, S.V.; Schaffer, A.; Bond, D.J.; Frey, B.N.; Sharma, V.; Goldstein, B.I.; Rej, S.; Beaulieu, S.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 Guidelines for the Management of Patients with Bipolar Disorder. Bipolar Disord. 2018, 20, 97–170. [Google Scholar] [CrossRef]
- Malhi, G.S.; Gessler, D.; Outhred, T. The Use of Lithium for the Treatment of Bipolar Disorder: Recommendations from Clinical Practice Guidelines. J. Affect. Disord. 2017, 217, 266–280. [Google Scholar] [CrossRef]
- Kendall, T.; Morriss, R.; Mayo-Wilson, E.; Marcus, E. Assessment and Management of Bipolar Disorder: Summary of Updated NICE Guidance. BMJ 2014, 349, g5673. [Google Scholar] [CrossRef]
- Barroilhet, S.A.; Ghaemi, S.N. When and How to Use Lithium. Acta Psychiatr. Scand. 2020, 142, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Ketter, T.A.; Miller, S.; Dell’Osso, B.; Wang, P.W. Treatment of Bipolar Disorder: Review of Evidence Regarding Quetiapine and Lithium. J. Affect. Disord. 2016, 191, 256–273. [Google Scholar] [CrossRef] [PubMed]
- Tohen, M.; Zarate, C.A.; Hennen, J.; Khalsa, H.-M.K.; Strakowski, S.M.; Gebre-Medhin, P.; Salvatore, P.; Baldessarini, R.J. The McLean-Harvard First-Episode Mania Study: Prediction of Recovery and First Recurrence. Am. J. Psychiatry 2003, 160, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Post, R.M.; Denicoff, K.D.; Leverich, G.S.; Altshuler, L.L.; Frye, M.A.; Suppes, T.M.; Rush, A.J.; Keck, P.E.; McElroy, S.L.; Luckenbaugh, D.A.; et al. Morbidity in 258 Bipolar Outpatients Followed for 1 Year with Daily Prospective Ratings on the NIMH Life Chart Method. J. Clin. Psychiatry 2003, 64, 680–690, quiz 738–739. [Google Scholar] [CrossRef] [PubMed]
- Ephraim, E.; Prettyman, R. Attitudes of Old Age Psychiatrists in England and Wales to the Use of Mood Stabilizer Drugs. Int. Psychogeriatr. 2009, 21, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Shulman, K.I.; Rochon, P.; Sykora, K.; Anderson, G.; Mamdani, M.; Bronskill, S.; Tran, C.T.T. Changing Prescription Patterns for Lithium and Valproic Acid in Old Age: Shifting Practice without Evidence. BMJ 2003, 326, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Strejilevich, S.A.; Urtueta-Baamonde, M.; Teitelbaum, J.; Martino, D.J.; Marengo, E.; Igoa, A.; Fassi, G.; Cetkovich-Bakmas, M. Clinical concepts associated with lithium underutilization in the treatment of bipolar disorder. Vertex B Aires Argent. 2011, 22, 3–20. [Google Scholar]
- Maj, M.; Pirozzi, R.; Kemali, D. Long-Term Outcome of Lithium Prophylaxis in Patients Initially Classified as Complete Responders. Psychopharmacology 1989, 98, 535–538. [Google Scholar] [CrossRef]
- Suppes, T.; Baldessarini, R.J.; Faedda, G.L.; Tohen, M. Risk of Recurrence Following Discontinuation of Lithium Treatment in Bipolar Disorder. Arch. Gen. Psychiatry 1991, 48, 1082–1088. [Google Scholar] [CrossRef]
- Faedda, G.L.; Tondo, L.; Baldessarini, R.J.; Suppes, T.; Tohen, M. Outcome after Rapid vs Gradual Discontinuation of Lithium Treatment in Bipolar Disorders. Arch. Gen. Psychiatry 1993, 50, 448–455. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (UK). Bipolar Disorder: The NICE Guideline on the Assessment and Management of Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care; National Institute for Health and Care Excellence: Clinical Guidelines; The British Psychological Society and The Royal College of Psychiatrists: London, UK, 2014. [Google Scholar]
- Maruki, T.; Utsumi, T.; Takeshima, M.; Fujiwara, Y.; Matsui, M.; Aoki, Y.; Toda, H.; Watanabe, N.; Watanabe, K.; Takaesu, Y. Efficacy and Safety of Adjunctive Therapy to Lamotrigine, Lithium, or Valproate Monotherapy in Bipolar Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Bipolar Disord. 2022, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C.; Baldessarini, R.J.; Mathiske-Schmidt, K.; Hennen, J.; Berghöfer, A.; Müller-Oerlinghausen, B.; Bschor, T.; Adli, M.; Bauer, M. Long-Term Combination Therapy versus Monotherapy with Lithium and Carbamazepine in 46 Bipolar I Patients. J. Clin. Psychiatry 2005, 66, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.; Boydell, J.; Kalidindi, S.; Fearon, P.; Jones, P.B.; van Os, J.; Murray, R.M. Gender Differences in Incidence and Age at Onset of Mania and Bipolar Disorder over a 35-Year Period in Camberwell, England. Am. J. Psychiatry 2005, 162, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M. Gender Differences in Bipolar Disorder. Psychiatr. Clin. N. Am. 2003, 26, 595–620. [Google Scholar] [CrossRef] [PubMed]
- Pillai, M.; Munoli, R.N.; Praharaj, S.K.; Bhat, S.M. Gender Differences in Clinical Characteristics and Comorbidities in Bipolar Disorder: A Study from South India. Psychiatr. Q. 2021, 92, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.G. Lithium Nephrotoxicity. Kidney Int. Suppl. 1993, 42, S93–S98. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, J.L.; da Silva Júnior, G.B.; de Abreu, K.L.S.; de Rocha, N.A.; Franco, L.F.L.G.; Araújo, S.M.H.A.; de Daher, E.F. Lithium Nephrotoxicity. Rev. Assoc. Med. Bras. 2010, 56, 600–606. [Google Scholar] [CrossRef]
- Davis, J.; Desmond, M.; Berk, M. Lithium and Nephrotoxicity: A Literature Review of Approaches to Clinical Management and Risk Stratification. BMC Nephrol. 2018, 19, 305. [Google Scholar] [CrossRef]
- Hayes, J.F.; Marston, L.; Walters, K.; Geddes, J.R.; King, M.; Osborn, D.P.J. Lithium vs. Valproate vs. Olanzapine vs. Quetiapine as Maintenance Monotherapy for Bipolar Disorder: A Population-Based UK Cohort Study Using Electronic Health Records. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2016, 15, 53–58. [Google Scholar] [CrossRef]
- Garver, D.L.; Hutchinson, L.J. Psychosis, Lithium-Induced Antipsychotic Response, and Seasonality. Psychiatry Res. 1988, 26, 279–286. [Google Scholar] [CrossRef]
- Kafantaris, V.; Coletti, D.J.; Dicker, R.; Padula, G.; Pollack, S. Are Childhood Psychiatric Histories of Bipolar Adolescents Associated with Family History, Psychosis, and Response to Lithium Treatment? J. Affect. Disord. 1998, 51, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Caldieraro, M.A.; Dufour, S.; Sylvia, L.G.; Gao, K.; Ketter, T.A.; Bobo, W.V.; Walsh, S.; Janos, J.; Tohen, M.; Reilly-Harrington, N.A.; et al. Treatment Outcomes of Acute Bipolar Depressive Episode with Psychosis. Depress. Anxiety 2018, 35, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Caldieraro, M.A.; Sylvia, L.G.; Dufour, S.; Walsh, S.; Janos, J.; Rabideau, D.J.; Kamali, M.; McInnis, M.G.; Bobo, W.V.; Friedman, E.S.; et al. Clinical Correlates of Acute Bipolar Depressive Episode with Psychosis. J. Affect. Disord. 2017, 217, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Kessing, L.V.; Vradi, E.; Andersen, P.K. Starting Lithium Prophylaxis Early v. Late in Bipolar Disorder. Br. J. Psychiatry J. Ment. Sci. 2014, 205, 214–220. [Google Scholar] [CrossRef]
- Bowden, C.; Boyer, P. Treatment Pathways for Bipolar Disorder in the USA and Europe: Convergence or Divergence? Eur. Psychiatry 2003, 18, 19s–24s. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, J.R.; Bowden, C.L.; Sachs, G.; Yatham, L.N.; Behnke, K.; Mehtonen, O.-P.; Montgomery, P.; Ascher, J.; Paska, W.; Earl, N.; et al. A Placebo-Controlled 18-Month Trial of Lamotrigine and Lithium Maintenance Treatment in Recently Depressed Patients with Bipolar I Disorder. J. Clin. Psychiatry 2003, 64, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Weisler, R.H.; Nolen, W.A.; Neijber, A.; Hellqvist, A.; Paulsson, B.; Trial 144 Study Investigators. Continuation of Quetiapine versus Switching to Placebo or Lithium for Maintenance Treatment of Bipolar I Disorder (Trial 144: A Randomized Controlled Study). J. Clin. Psychiatry 2011, 72, 1452–1464. [Google Scholar] [CrossRef]
- Hung, Y.-N.; Yang, S.-Y.; Huang, M.-C.; Lung, F.-W.; Lin, S.-K.; Chen, K.-Y.; Kuo, C.-J.; Chen, Y.-Y. Cancer Incidence in People with Affective Disorder: Nationwide Cohort Study in Taiwan, 1997–2010. Br. J. Psychiatry J. Ment. Sci. 2014, 205, 183–188. [Google Scholar] [CrossRef]
- Wu, H.-C.; Chou, F.H.-C.; Tsai, K.-Y.; Su, C.-Y.; Shen, S.-P.; Chung, T.-C. The Incidence and Relative Risk of Stroke among Patients with Bipolar Disorder: A Seven-Year Follow-up Study. PLoS ONE 2013, 8, e73037. [Google Scholar] [CrossRef]
- Lin, H.-C.; Tsai, S.-Y.; Lee, H.-C. Increased Risk of Developing Stroke among Patients with Bipolar Disorder after an Acute Mood Episode: A Six-Year Follow-up Study. J. Affect. Disord. 2007, 100, 49–54. [Google Scholar] [CrossRef]
- Prieto, M.L.; Cuéllar-Barboza, A.B.; Bobo, W.V.; Roger, V.L.; Bellivier, F.; Leboyer, M.; West, C.P.; Frye, M.A. Risk of Myocardial Infarction and Stroke in Bipolar Disorder: A Systematic Review and Exploratory Meta-Analysis. Acta Psychiatr. Scand. 2014, 130, 342–353. [Google Scholar] [CrossRef] [PubMed]
- McElroy, S.L.; Keck, P.E. Obesity in Bipolar Disorder: An Overview. Curr. Psychiatry Rep. 2012, 14, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Greil, W.; de Bardeci, M.; Müller-Oerlinghausen, B.; Nievergelt, N.; Stassen, H.; Hasler, G.; Erfurth, A.; Cattapan, K.; Rüther, E.; Seifert, J.; et al. Controversies Regarding Lithium-Associated Weight Gain: Case–Control Study of Real-World Drug Safety Data. Int. J. Bipolar Disord. 2023, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Calkin, C.V.; Ruzickova, M.; Uher, R.; Hajek, T.; Slaney, C.M.; Garnham, J.S.; O’Donovan, M.C.; Alda, M. Insulin Resistance and Outcome in Bipolar Disorder. Br. J. Psychiatry J. Ment. Sci. 2015, 206, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Steardo, L.; Fabrazzo, M.; Sampogna, G.; Monteleone, A.M.; D’Agostino, G.; Monteleone, P.; Maj, M. Impaired Glucose Metabolism in Bipolar Patients and Response to Mood Stabilizer Treatments. J. Affect. Disord. 2019, 245, 174–179. [Google Scholar] [CrossRef]
- Patorno, E.; Huybrechts, K.F.; Bateman, B.T.; Cohen, J.M.; Desai, R.J.; Mogun, H.; Cohen, L.S.; Hernandez-Diaz, S. Lithium Use in Pregnancy and the Risk of Cardiac Malformations. N. Engl. J. Med. 2017, 376, 2245–2254. [Google Scholar] [CrossRef]
- Overview|Bipolar Disorder: Assessment and Management|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/cg185 (accessed on 14 December 2023).
- ACOG Committee on Practice Bulletins. Obstetrics ACOG Practice Bulletin: Clinical Management Guidelines for Obstetrician-Gynecologists Number 92, April 2008 (Replaces Practice Bulletin Number 87, November 2007). Use of Psychiatric Medications during Pregnancy and Lactation. Obstet. Gynecol. 2008, 111, 1001–1020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Publication Details | Study Details | Main Findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Country | Study Design | N | Mean Age (SD) | Percentage of Females | Inpatient (IP) or Outpatient (OP) | Special Demographic | Diagnosis | Year of Study Sample | Prescription Rate (PR) for Lithium (CI) | Clinical Correlates |
| Lähteenvuo et al., 2023 [30] | Finland | Longitudinal | 60,045 | 41.7 (15.8) | 56.4% | IP OP | NA | BD | 1996–2018 | NA | Lithium users were associated with a lower risk of hospitalization for psychiatric reasons than those not using medication from the same medicine class. |
| Singh et al., 2023 [31] | North America, Europe, and Australia | Cross-sectional | 7748 | 41.4 | 60.6% | IP OP | NA | BD | 1998–2020 | 30.3% | |
| Lin et al., 2023 [32] | Taiwan | Longitudinal | 420 | 17.2 (1.9) | 53.8% | OP | Children (below 20) | BD | 2006–2019 | 23.1% | |
| Shinozaki et al., 2022 [33] | Japan | Cross-sectional | 2563 | 50.7 (13.8) | 54.1% | OP | NA | BD | 2017 | 47.5% (ALL) 55.1% (BD-I) 43.2% (BD-II) | |
| Uwai and Nabekura, 2022 [34] | Japan | Cross-sectional | 3521 | Not reported | 58.9% | Not reported | NA | BD | 2004–2020 | NA | Lithium use was not associated with Parkinson-like events. |
| Ng et al., 2021 [35] | Hong Kong and the UK | Cross-sectional, cohort (time trend) | HK: 15,287 UK: 30,140 | HK: 38.92 (22.46) UK: 44.18 (26.69) | HK: 60.5% UK: 61.4% | IP OP | NA | BD | 2001–2018 | Hong Kong 2001—20.1% 2002—24.4% 2003—25.8% 2004—25.8% 2005—25.8% 2006—25.0% 2007—23.8% 2008—22.9% 2009—22.1% 2010—21.3% 2011—20.5% 2012—20.1% 2013—19.0% 2014—18.6% 2015—17.9% 2016—17.8% 2017—17.9% 2018—17.6% *** United Kingdom 2001—30.7% 2002—30.0% 2003—29.1% 2004—28.9% 2005—27.5% 2006—26.4% 2007—25.6% 2008—24.3% 2009—23.0% 2010—21.8% 2011—20.9% 2012—19.3% 2013—18.7% 2014—17.7% 2015—16.9% 2016—16.5% 2017—16.5% 2018—16.1% *** | |
| Prillo et al., 2021 [36] | Canada | Cross-sectional | 129 | Li users: 49.05 (11.78) Non-Li users: 46.71 (11.20) | Li users: 56.1% Non-Li users: 46.0% | OP | NA | BD | NA | NA | Lithium use was associated with significantly lower HbA1c and triglyceride levels. Lithium use was not associated with obesity, BMI, metabolic syndrome, hypertension, or thyroid disease. |
| Grover et al., 2021 [37] | India | Cross-sectional | 773 | 45.7 (10.5) | 36.4% | OP | NA | BD | Not stated | 38.9% on lithium monotherapy | |
| Lin et al., 2020 [38] | USA | Cross-sectional, cohort (time trend) | 5400 | Not reported | 61.6% | OP | NA | BD | 1996–2015 | 1996–1997: 38.0% 1998–1999: 28.2% 2000–2001: 22.7% 2002–2003: 18.9% 2004–2005: 21.8% 2006–2007: 14.4% 2008–2009: 12.5% 2010–2011: 12.6% 2012–2013: 14.1% 2014–2015: 14.7% ** | |
| Karanti et al., 2020 [39] | Sweden | Cross-sectional | 8766 | BD I 50.2 (15.7) BD II 45.38 (15.6) | 61.9% | OP | NA | BD | 2004–2013 | BD I 68.6% BD II 44.7% | |
| Salazar de Pablo et al., 2020 [40] | USA | Cross-sectional | 76 | 15.6 (1.4) (12–18) | 59.2% | IP | Children (age 12–18) | BD | 2009–2017 | 22.4% on admission 35.5% on discharge | |
| Bohlken et al., 2020 [17] | Germany | Cross-sectional, cohort (time trend) | 4137 | 2009: 53.5 (15.0) 2018: 56.4 (15.0) | 67.9% | OP | NA | BD | 2009 and 2018 | 2009: 31.4% 2018: 26.2% | Non-blacks have a significantly higher prescription rate for lithium (34.2%) compared to blacks (26.2%). |
| Rhee et al., 2020 [41] | USA | Cross-sectional, cohort (time trend) | 4419 | Not reported | 59.4–63.8% | OP | NA | BD | 1997–2016 | 1997–2000: 30.4% 2001–2004: 20.7% 2005–2008: 17.3% 2009–2012: 13.9% 2013–2016: 17.6% | |
| Lyall et al., 2019 [42] | Scotland | Cross-sectional, cohort (time trend) | 20,796 | Not reported | Not reported | IP/OP | NA | BD | 2009–2016 | 2009: 26.1% 2010: 25.5% 2011: 25.2% 2012: 24.1% 2013: 23.7% 2014: 23.1% 2015: 22.4% 2016: 21.9% *** | Lithium use was more common in males and older patients. |
| Musetti et al., 2018 [43] | Italy | Longitudinal | 234 | 38.6 (12.7) | 60.2% | OP | NA | BD | 2002–2006 | 76.10% | |
| Jaracz et al., 2018 [44] | Poland | Cross-sectional | 127 | 46.2 (13.8) | 44.9% | IP | NA | BD | 2015–2016 | 23.60% | |
| Broeks et al., 2017 [45] | Denmark | Longitudinal | 336 | 29.85 (26.3–34.03) | 100.0% | Not reported | Pregnant women | BD | 1997–2012 | 18.5% None redeemed during pregnancy: 5.7% Redeemed during pregnancy: 29.8% | |
| Rej et al., 2017 [46] | Canada | Cross-sectional | 1443 | 72.24 (5.63) | 63.8% | IP | NA | BD | 2006–2012 | 23.40% | |
| Bauer et al., 2016 [47] | USA | Longitudinal | 27,727 | Lithium only: 44.85 (13.50) Lithium + SGA: 43.50 (13.29) | Lithium only: 26.8% Lithium + SGA: 16.7% | OP | NA | BD | 2003–2010 | NA | Patients on lithium monotherapy and valproate monotherapy were associated with a significantly lower likelihood of all-cause hospitalizations compared to patients on second-generation antipsychotic monotherapy. The initiation of lithium or valproate was associated with a significantly lower likelihood of mental health hospitalizations than second-generation antipsychotics. |
| Kessing et al., 2016 [15] | Denmark | Longitudinal | 3205 | 2000: 51.0 (35.7–64.5) 2008: 40.9 (30.3–55.6) | 45.1–55.8% | IP OP | NA | Single manic episode or BD | 2000–2011 | 2000: 41.1% 2001: 40.2% 2002: 39.0% 2003: 36.9% 2004: 30.8% 2005: 32.3% 2006: 35.0% 2007: 39.4% 2008: 38.0% 2009: 33.2% 2010: 30.8% 2011: 34.0% * | |
| Huang et al., 2016 [48] | Taiwan | Longitudinal | 4729 | Not reported | Not reported | IP OP | NA | BD | 1998–2009 | NA | Lithium use was associated with a significantly lower risk of cancer compared to anticonvulsant users. Higher cumulative and daily doses of lithium were significantly associated with lower cancer risk. |
| Chang et al., 2016 [49] | Taiwan | Longitudinal and cross-sectional (time trend) | 2703 | 40.5 (18.8) | 52.5% | IP OP | NA | BD | 2001–2010 | 2001: 18.3% 2002: 13.9% 2003: 11.2% 2004: 13.9% 2005: 14.6% 2006: 13.2% 2007: 11.5% 2008: 10.2% 2009: 7.8% 2010: 6.9% ** | |
| Arikan et al., 2016 [50] | Istanbul | Cross-sectional, cohort (time trend) | 2001–2002: 78 2011–2012: 87 | 2001–2002: 36.4 (12.1) 18–73 2011–2012: 37.2 (14.4) 16–70 | 56.4–59.8% | IP | NA | BD | 2001–2002 and 2011–2012 | 2001–2002: 49.1% 2011–2012: 36.5% | |
| Kleimann et al., 2016 [51] | Austria, Switzerland, and Germany | Cross-sectional, cohort (time trend) | 1650 | 48.87 (14.91) | 53.1% | Not reported | NA | Acute mania | 2005–2012 | 2005: 27.5% 2006: 27.5% 2007: 23.6% 2008: 26.3% 2009: 29.3% 2010: 37.7% 2011: 31.3% 2012: 28.2% | Lithium use was significantly less common in patients over 70 years old. |
| Karanti et al., 2016 [14] | Sweden | Cross-sectional, cohort (time trend) | 32,019 | Male: 51.9 (15.3) Female: 49.6 (15.9) | 61.0% | Not reported | NA | BD | 2007–2013 | Male: 2007: 71.2% 2008: 70.0% 2009: 67.8% 2010: 66.4% 2011: 65.1% 2012: 62.9% 2013: 59.3% *** Female: 2007: 64.0% 2008: 65.0% 2009: 62.5% 2010: 59.2% 2011: 57.1% 2012: 54.9% 2013: 52.8% *** | Lithium use was significantly more common in men than women. Lithium users were, on average, 5.4 years older than non-users. |
| Carlborg et al., 2015 [52] | Sweden | Cross-sectional, cohort | 10,273 | 42.6 | 62.3% | IP OP | NA | BD | 2006–2010 | 2006—40.8% 2007—40.3% 2008—37.5% 2009—35.3% 2010—32.6% ** | |
| Lan et al., 2015 [53] | Taiwan | Cross-sectional | 3681 | Not reported | Not reported | IP OP | NA | BD | 2001–2011 | NA | Lithium use was associated with a significantly lower risk of stroke than non-users. |
| Toffol et al., 2015 [54] | Finland | Longitudinal | 826 | Not reported | Unable to access tables | IP | NA | BD | 1996–2003 | 37% | Lithium use was associated with a lower risk of suicidal behavior and overall mortality. |
| Karanti et al., 2015 [55] | Sweden | Cross-sectional | 7354 | 47.9 (23.3) | 61.0% | OP | NA | BD | 2004–2011 | NA | Lithium use was significantly more common in men than women. |
| Baek et al., 2014 [56] | Korea | Longitudinal | 1447 | B1 MI 37.32 (1.8) B1 DI 27.59 (13.7) B1 O 37.90 (14.6) B2 DI 16.89 (16.0) B2 O 35.4 (14.3) | 59.7% | IP OP | NA | BD | 2009 | B1 MI 37.9% B1 DI 29.6% B1 O 38.3% B2 DI 29.1% B2 O 27.5% | |
| Ko et al., 2014 [57] | Canada | Cross-sectional | 100 | Li users: 17.05 (1.10) Non-Li users: 15.98 (1.47) | Li users: 75% Non-Li: users 65% | OP | Children (age 13–19) | BD | NA | NA | Lithium use was associated with older patients, a diagnosis of BD-I, psychosis, self-injurious behavior, previous psychiatric hospitalizations, and lifetime use of antimanics/anticonvulsants/second-generation antipsychotics. Lithium use was not associated with suicide ideation or suicide attempts. |
| Grande et al., 2013 [58] | Spain | Cross-sectional | 739 | 46.1 (13.7) | 59.3% | OP | NA | BD | 2006–2007 | 10.40% | Lithium monotherapy was associated with a family history of psychiatric disorders, longer duration from previous BD episodes, and younger patients. |
| Trivedi et al., 2013 [59] | India | Cross-sectional | 100 | 31.0 (11.9) | 18.0% | OP | NA | BD | Not stated | 57.0% | |
| Haeberle et al., 2012 [60] | Germany, Switzerland, and Austria | Cross-sectional, cohort (time trend) | 2246 | Not reported | Not reported | IP | NA | Bipolar depression | 1994–2009 | 1994–1997: 44.7% 1998–2001: 36.4% 2002–2005: 30.5% 2006–2009: 34.7% | |
| Greil et al., 2012 [61] | Germany, Switzerland, and Austria | Cross-sectional, cohort (time trend) | 2231 | 57 | 62.0% | IP | NA | Bipolar depression | 1994–2009 | 1994: 47.9% 1995: 54.6% 1996: 47.3% 1997: 37.8% 1998: 39.2% 1999: 44.1% 2000: 30.3% 2001: 31.8% 2002: 28.5% 2003: 30.3% 2004: 30.7% 2005: 30.8% 2006: 30.6% 2007: 37.0% 2008: 35.1% 2009: 35.7% ** | |
| Walpoth-Niederwanger et al., 2012 [62] | Austria | Cross-sectional, cohort (time trend) | 531 | 48.9 | 68.1% | IP | NA | BD | 1999–2007 | 1999–2003: 19.3% 2004–2007: 13.3% | Lithium use was significantly more common in men compared to women. |
| Dusetzina et al., 2011 [63] | USA | Longitudinal | 412 | Not reported | 53.0% | IP OP | Children (age 6–17) | BD-I | 2005–2007 | 11% | |
| Post et al., 2011 [64] | USA, the Netherlands, and Germany | Cross-sectional (?) | 525 | US: 18.6 Europe: 24.80 | Not reported | OP | NA | BD | ??? | US: 53.33% Europe: 81.40% | |
| Larsen et al., 2009 [65] | Finland, Norway, Denmark, France, Italy, Germany, Greece, the Netherlands, the UK and Ireland, Belgium, Spain, Portugal, and Switzerland | Longitudinal | 3459 | Nordic: 46.9 (14.00) European: 44.6 (13.39) | Not reported | IP OP | NA | BD | 2002–2004 | Nordic—34% Lithium monotherapy 12% AP + Lithium 11% AP + Lithium + Anticonvulsants 11% European—33% Lithium monotherapy 5% AP + Lithium 21% AP + Lithium + Anticonvulsants 7% | |
| Jerrell et al., 2008 [66] | USA | Longitudinal | 82 | 6–17 | 52.0% | IP | Children (age 6–17) | BD-I | 2003–2004 | 4.90% | |
| Baldessarini et al. et al., 2008 [67] | USA | Longitudinal | 7406 | 35.4 (12.4) | 56.5% | IP OP | NA | BD | 2001–2004 | 9.5% at initial treatment/baseline 14.5% at final treatment/12 months | Patients given lithium as the single mood stabilizer were much less likely to receive adjunctive psychotropic agents during the following year than those whose single mood stabilizer was an anticonvulsant. |
| Al Jurdi et al., 2008 [68] | USA | Longitudinal | 2442 | Not reported | 56.6% | IP OP | NA | BD | 1998–2005 | Total: 37.2% 20–59: 37.8% 60 and above: 29.5% | Lithium use was more common in younger patients (age 20–59) compared to older patients (over 60). Lithium dosing was higher in younger patients compared to older patients. |
| Baldessarini et al., 2007 [16] | USA | Longitudinal | 7760 | 40.1 | 39.9% | IP OP | NA | BD | 2002–2003 | 7.50% | |
| Wolfsperger et al., 2007 [69] | Germany, Switzerland, and Austria | Cross-sectional, cohort (time trend) | 998 | 46.9 | 50.5% | IP | NA | BD | 1994–2004 | Bipolar mania: 1994–1999: 46.7% 2000–2004: 36.7% | |
| Baldessarini et al., 2006 [70] | Many | Meta-analysis | NA | Not reported | Not reported | Not reported | NA | BD | 1970–2006 | NA | Lithium use was associated with a significantly lower suicidal risk than non-users. |
| Kilbourne et al., 2006 [71] | USA | Cross-sectional | 2958 | 52 (12) | 10.6% | IP OP | NA | BD | 2001 | 33.20% | |
| Sajatovic et al., 2004 [72] | USA | Cross-sectional | 65,556 | 52.7 (12.7) | 11.4% | IP OP | NA | BD | 2001 | 25% | |
| Bhangoo et al., 2003 [73] | USA | Cross-sectional | 111 | 10.98 (2.64) | 35.0% | OP | Children (age 6–17) | BD | Unknown | 51% | |
| Levine et al., 2000 [74] | USA | Cross-sectional | 457 | 40 (10) | 67.0% | OP | NA | BD-I | 1995–1996 | 50.10% | |
| Unutzer et al., 1998 [75] | USA | Cross-sectional | 1236 | 43.1 (14) | 66.1% | IP OP | NA | BD | 1995–1996 | 60.30% | |
| Sajatovic et al., 1997 [76] | USA | Cross-sectional | 96 | 50 (12.3) (23–83) | 8.3% | IP | NA | BD | 1993–1995 | 62.50% | No difference in the length of stay between patients on lithium monotherapy compared to anticonvulsant monotherapy was observed. Use of psychotropic medication was not associated with the drug regime. |
| Chou et al., 1996 [77] | USA | Cross-sectional | 528 | 42.0 (13.0) | 49.1% | IP | NA | BD | 1990 | 61% | |
| Fenn et al., 1996 [78] | USA | Cross-sectional, cohort (time trend) | 829 | Not reported | Not reported | IP | NA | BD | 1989–1994 | Lithium monotherapy: 1989: 84% 1994: 43% | |
| Sajatovic et al., 1996 [79] | USA | Longitudinal | 23 | Not reported | Not reported | IP | Elderly (age above 65) | BD | 1992–1994 | 70% | |
| Hes et al., 1976 [80] | Israel | Cross-sectional | 314 | Not reported | Not reported | NS | NA | BD | 1967–1974 | 76% | |
| Region | Lithium Prescription Rate 2 | Number of Studies | Sample Size (n) | |||
|---|---|---|---|---|---|---|
| Pre-Cutoff | Post-Cutoff | Pre-Cutoff | Post-Cutoff | Pre-Cutoff | Post-Cutoff | |
| North America 1 | 27.7% | 17.1% | 13 | 8 | 19,356 | 19,782 |
| Europe | 36.7% | 35.7% | 18 | 13 | 63,581 | 62,592 |
| Asia | 25.0% | 26.2% | 6 | 5 | 12,270 | 10,917 |
| Overall | 33.4% | 30.6% | 37 | 26 | 95,207 | 93,291 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shuy, Y.K.; Santharan, S.; Chew, Q.H.; Sim, K. International Trends in Lithium Use for Pharmacotherapy and Clinical Correlates in Bipolar Disorder: A Scoping Review. Brain Sci. 2024, 14, 102. https://doi.org/10.3390/brainsci14010102
Shuy YK, Santharan S, Chew QH, Sim K. International Trends in Lithium Use for Pharmacotherapy and Clinical Correlates in Bipolar Disorder: A Scoping Review. Brain Sciences. 2024; 14(1):102. https://doi.org/10.3390/brainsci14010102
Chicago/Turabian StyleShuy, Yao Kang, Sanjana Santharan, Qian Hui Chew, and Kang Sim. 2024. "International Trends in Lithium Use for Pharmacotherapy and Clinical Correlates in Bipolar Disorder: A Scoping Review" Brain Sciences 14, no. 1: 102. https://doi.org/10.3390/brainsci14010102
APA StyleShuy, Y. K., Santharan, S., Chew, Q. H., & Sim, K. (2024). International Trends in Lithium Use for Pharmacotherapy and Clinical Correlates in Bipolar Disorder: A Scoping Review. Brain Sciences, 14(1), 102. https://doi.org/10.3390/brainsci14010102