


Novel Approaches for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review of Non-Invasive Brain Stimulation Interventions and Insights from Clinical Trials
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Formula
2.2. Eligibility Criteria
- Participants: Studies conducted on adult participants (i.e., of 18 years of age or older) with a primary diagnosis of PTSD according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), or Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR; [1]) classifications. Studies in which participants reported highly severe PTSD symptoms, i.e., a total score on the Post-Traumatic Stress Disorder Checklist—Civilian Version (PCL-C) greater than 50, were also included.
- Intervention: Studies in which NIBS was administered as a mono-therapy or combined with other evidence-based and non-surgical interventions, e.g., psychotherapy. Both TMS and TES, including tDCS, tACS, and tRNS, were considered to be eligible treatments.
- Comparison: The presence of at least one control group or condition that could be treated with a sham, i.e., inactive, stimulation, or active stimulation over a control site, e.g., Vertex, was not mandatory for inclusion.
- Outcome measure: Studies that evaluated potential reductions in participants’ PTSD symptoms’ severity according to standardized instruments. Overall PTSD symptoms’ severity was considered as the primary outcome, whereas general anxiety and depressive symptoms’ severity, assessed through standardized instruments, were considered secondary outcomes.
- Study Design: All types of quantitative clinical trials were included, as long as they met the above-mentioned inclusion criteria. Specifically, retrospective, controlled, or open-label studies with or without randomization were accepted if they provided at least one pre- and one post-treatment assessment of participants’ symptomatology.
- The sample included children, adolescents (i.e., of 16 years of age or below), adults with a secondary diagnosis of PTSD, or animal models.
- Stimulation was delivered invasively, e.g., through the implantation of electrodes in the brain, or coupled with other surgical procedures.
- PTSD symptoms’ severity was not assessed or compared among groups or conditions.
- They were non-original research studies (e.g., secondary sources, opinion-based, editorials, policy reviews and statements, commentaries), Master-level dissertations, conference presentations, conference proceedings where full-length articles were not available, preprints, single-case studies, correlational studies, narrative articles or reviews, or meta-analyses.
- Papers written in a language other than English were also excluded.
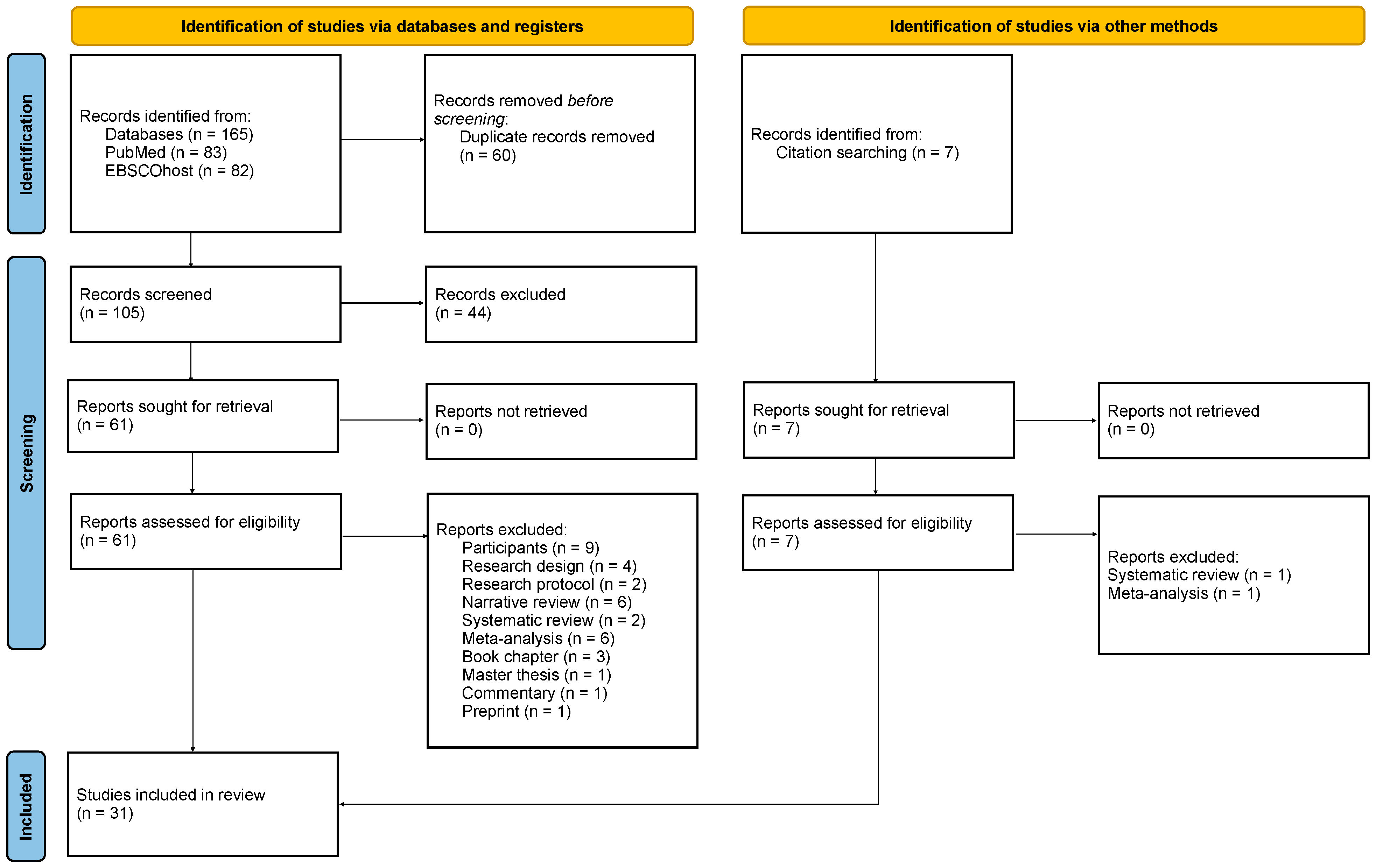
2.3. Study Screening and Selection Process
2.4. Data Extraction and Quality Assessment
3. Results
3.1. Demographic Characteristics of the Sample
3.2. Effects of Transcranial Magnetic Stimulation on Post-Traumatic Stress Disorder Symptoms’ Severity
3.2.1. Low-Frequency rTMS Protocols
3.2.2. High-Frequency rTMS Protocols
3.2.3. Low- versus High-Frequency rTMS Protocols
3.2.4. TBS Protocols
3.2.5. Integrated Protocols
3.3. Effects of Transcranial Magnetic Stimulation on Anxiety and Depressive Symptoms’ Severity
3.3.1. Low-Frequency rTMS Protocols
3.3.2. High-Frequency rTMS Protocols
3.3.3. Low- versus High-Frequency rTMS Protocols
3.3.4. TBS Protocols
3.3.5. Integrated Protocols
3.4. Effects of Transcranial Electrical Stimulation on Post-Traumatic Stress Disorder Symptoms’ Severity
3.4.1. Anodal tDCS Protocols
3.4.2. Cathodal tDCS Protocols
3.4.3. Integrated tDCS Protocols
3.5. Effects of Transcranial Electrical Stimulation on Anxiety and Depressive Symptoms’ Severity
3.5.1. Anodal tDCS Protocols
3.5.2. Cathodal tDCS Protocols
3.5.3. Integrated tDCS Protocols
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR, 5th ed.; Text Revision; American Psychiatric Association: Arlington, VA, USA, 2022. [Google Scholar]
- Flory, J.D.; Yehuda, R. Comorbidity between Post-Traumatic Stress Disorder and Major Depressive Disorder: Alternative Explanations and Treatment Considerations. Dialogues Clin. Neurosci. 2015, 17, 141–150. [Google Scholar] [CrossRef]
- Qassem, T.; Aly-ElGabry, D.; Alzarouni, A.; Abdel-Aziz, K.; Arnone, D. Psychiatric Co-Morbidities in Post-Traumatic Stress Disorder: Detailed Findings from the Adult Psychiatric Morbidity Survey in the English Population. Psychiatr. Q. 2021, 92, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic Stress Disorder in the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, Severity, and Comorbidity of 12-Month DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef]
- Koenen, K.C.; Ratanatharathorn, A.; Ng, L.; McLaughlin, K.A.; Bromet, E.J.; Stein, D.J.; Karam, E.G.; Meron Ruscio, A.; Benjet, C.; Scott, K.; et al. Posttraumatic Stress Disorder in the World Mental Health Surveys. Psychol. Med. 2017, 47, 2260–2274. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, R.H.; Goldstein, R.B.; Southwick, S.M.; Grant, B.F. Prevalence and Axis I Comorbidity of Full and Partial Posttraumatic Stress Disorder in the United States: Results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Anxiety Disord. 2011, 25, 456–465. [Google Scholar] [CrossRef]
- Wisco, B.E.; Marx, B.P.; Wolf, E.J.; Miller, M.W.; Southwick, S.M.; Pietrzak, R.H. Posttraumatic Stress Disorder in the US Veteran Population: Results from the National Health and Resilience in Veterans Study. J. Clin. Psychiatry 2014, 75, 1338–1346. [Google Scholar] [CrossRef]
- Wisco, B.E.; Nomamiukor, F.O.; Marx, B.P.; Krystal, J.H.; Southwick, S.M.; Pietrzak, R.H. Posttraumatic Stress Disorder in US Military Veterans: Results From the 2019–2020 National Health and Resilience in Veterans Study. J. Clin. Psychiatry 2022, 83, 20m14029. [Google Scholar] [CrossRef]
- Bisson, J.I.; Roberts, N.P.; Andrew, M.; Cooper, R.; Lewis, C. Psychological Therapies for Chronic Post-Traumatic Stress Disorder (PTSD) in Adults. Cochrane Database Syst. Rev. 2013, 2013, CD003388. [Google Scholar] [CrossRef]
- Cipriani, A.; Williams, T.; Nikolakopoulou, A.; Salanti, G.; Chaimani, A.; Ipser, J.; Cowen, P.J.; Geddes, J.R.; Stein, D.J. Comparative Efficacy and Acceptability of Pharmacological Treatments for Post-Traumatic Stress Disorder in Adults: A Network Meta-Analysis. Psychol. Med. 2018, 48, 1975–1984. [Google Scholar] [CrossRef]
- NICEG. Post-Traumatic Stress Disorder; National Institute for Health and Care Excellence: London, UK, 2018; ISBN 978-1-4731-3181-1. [Google Scholar]
- Watkins, L.E.; Sprang, K.R.; Rothbaum, B.O. Treating PTSD: A Review of Evidence-Based Psychotherapy Interventions. Front. Behav. Neurosci. 2018, 12, 258. [Google Scholar] [CrossRef]
- Chen, Y.-R.; Hung, K.-W.; Tsai, J.-C.; Chu, H.; Chung, M.-H.; Chen, S.-R.; Liao, Y.-M.; Ou, K.-L.; Chang, Y.-C.; Chou, K.-R. Efficacy of Eye-Movement Desensitization and Reprocessing for Patients with Posttraumatic-Stress Disorder: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2014, 9, e103676. [Google Scholar] [CrossRef]
- McLean, C.P.; Levy, H.C.; Miller, M.L.; Tolin, D.F. Exposure Therapy for PTSD: A Meta-Analysis. Clin. Psychol. Rev. 2022, 91, 102115. [Google Scholar] [CrossRef]
- Phelps, A.J.; Lethbridge, R.; Brennan, S.; Bryant, R.A.; Burns, P.; Cooper, J.A.; Forbes, D.; Gardiner, J.; Gee, G.; Jones, K.; et al. Australian Guidelines for the Prevention and Treatment of Posttraumatic Stress Disorder: Updates in the Third Edition. Aust. N. Z. J. Psychiatry 2022, 56, 230–247. [Google Scholar] [CrossRef]
- Kline, A.C.; Cooper, A.A.; Rytwinksi, N.K.; Feeny, N.C. Long-Term Efficacy of Psychotherapy for Posttraumatic Stress Disorder: A Meta-Analysis of Randomized Controlled Trials. Clin. Psychol. Rev. 2018, 59, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Schumacher, S.; Hannig, W.; Barth, J.; Lotzin, A.; Schäfer, I.; Ehring, T.; Kleim, B. Long-Term Outcomes of Psychological Treatment for Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. Psychol. Med. 2021, 51, 1420–1430. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and Recommendations for TMS Use in Healthy Subjects and Patient Populations, with Updates on Training, Ethical and Regulatory Issues: Expert Guidelines. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]
- Heim, C.; Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. CNS Spectr. 2009, 14, 13–24. [Google Scholar] [PubMed]
- Im, J.J.; Namgung, E.; Choi, Y.; Kim, J.Y.; Rhie, S.J.; Yoon, S. Molecular Neuroimaging in Posttraumatic Stress Disorder. Exp. Neurobiol. 2016, 25, 277–295. [Google Scholar] [CrossRef]
- Ross, M.C.; Cisler, J.M. Altered Large-Scale Functional Brain Organization in Posttraumatic Stress Disorder: A Comprehensive Review of Univariate and Network-Level Neurocircuitry Models of PTSD. NeuroImage Clin. 2020, 27, 102319. [Google Scholar] [CrossRef]
- Etkin, A.; Egner, T.; Kalisch, R. Emotional Processing in Anterior Cingulate and Medial Prefrontal Cortex. Trends Cogn. Sci. 2011, 15, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Koenigs, M.; Grafman, J. Posttraumatic Stress Disorder: The Role of Medial Prefrontal Cortex and Amygdala. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2009, 15, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Lamanna, J.; Isotti, F.; Ferro, M.; Racchetti, G.; Anchora, L.; Rucco, D.; Malgaroli, A. Facilitation of Dopamine-Dependent Long-Term Potentiation in the Medial Prefrontal Cortex of Male Rats Follows the Behavioral Effects of Stress. J. Neurosci. Res. 2021, 99, 662–678. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.S.; Barredo, J.; van’t Wout-Frank, M.; Tyrka, A.R.; Price, L.H.; Carpenter, L.L. Network Mechanisms of Clinical Response to Transcranial Magnetic Stimulation in Posttraumatic Stress Disorder and Major Depressive Disorder. Biol. Psychiatry 2018, 83, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.S.; Jovanovic, T.; Fani, N.; Ely, T.D.; Glover, E.M.; Bradley, B.; Ressler, K.J. Disrupted Amygdala-Prefrontal Functional Connectivity in Civilian Women with Posttraumatic Stress Disorder. J. Psychiatr. Res. 2013, 47, 1469–1478. [Google Scholar] [CrossRef] [PubMed]
- Vanelzakker, M.B.; Dahlgren, M.K.; Davis, F.C.; Dubois, S.; Shin, L.M. From Pavlov to PTSD: The Extinction of Conditioned Fear in Rodents, Humans, and Anxiety Disorders. Neurobiol. Learn. Mem. 2014, 113, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.P.; Vanelzakker, M.B.; Shin, L.M. Emotion and Cognition Interactions in PTSD: A Review of Neurocognitive and Neuroimaging Studies. Front. Integr. Neurosci. 2012, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Lamanna, J.; Isotti, F.; Ferro, M.; Spadini, S.; Racchetti, G.; Musazzi, L.; Malgaroli, A. Occlusion of Dopamine-Dependent Synaptic Plasticity in the Prefrontal Cortex Mediates the Expression of Depressive-like Behavior and Is Modulated by Ketamine. Sci. Rep. 2022, 12, 11055. [Google Scholar] [CrossRef]
- Richter-Levin, G.; Stork, O.; Schmidt, M.V. Animal Models of PTSD: A Challenge to Be Met. Mol. Psychiatry 2019, 24, 1135–1156. [Google Scholar] [CrossRef]
- Akiki, T.J.; Averill, C.L.; Abdallah, C.G. A Network-Based Neurobiological Model of PTSD: Evidence From Structural and Functional Neuroimaging Studies. Curr. Psychiatry Rep. 2017, 19, 81. [Google Scholar] [CrossRef]
- Miller, D.R.; Hayes, S.M.; Hayes, J.P.; Spielberg, J.M.; Lafleche, G.; Verfaellie, M. Default Mode Network Subsystems Are Differentially Disrupted in Posttraumatic Stress Disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 363–371. [Google Scholar] [CrossRef]
- Tursich, M.; Ros, T.; Frewen, P.A.; Kluetsch, R.C.; Calhoun, V.D.; Lanius, R.A. Distinct Intrinsic Network Connectivity Patterns of Post-Traumatic Stress Disorder Symptom Clusters. Acta Psychiatr. Scand. 2015, 132, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, F.V.; Gidyk, D.C.; Giacobbe, P.; Ng, E.; Meng, Y.; Davidson, B.; Abrahao, A.; Lipsman, N.; Hamani, C. Neuromodulation Strategies in Post-Traumatic Stress Disorder: From Preclinical Models to Clinical Applications. Brain Sci. 2019, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Klomjai, W.; Katz, R.; Lackmy-Vallée, A. Basic Principles of Transcranial Magnetic Stimulation (TMS) and Repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef]
- Downar, J.; Daskalakis, Z.J. New Targets for rTMS in Depression: A Review of Convergent Evidence. Brain Stimulat. 2013, 6, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Vida, R.G.; Sághy, E.; Bella, R.; Kovács, S.; Erdősi, D.; Józwiak-Hagymásy, J.; Zemplényi, A.; Tényi, T.; Osváth, P.; Voros, V. Efficacy of Repetitive Transcranial Magnetic Stimulation (rTMS) Adjunctive Therapy for Major Depressive Disorder (MDD) after Two Antidepressant Treatment Failures: Meta-Analysis of Randomized Sham-Controlled Trials. BMC Psychiatry 2023, 23, 545. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Fattore, L.; Sestito, L.; Di Giuda, D.; Diana, M.; Addolorato, G. Transcranial Magnetic Stimulation: A Review about Its Efficacy in the Treatment of Alcohol, Tobacco and Cocaine Addiction. Addict. Behav. 2021, 114, 106760. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.; Li, H.; Bu, X.; Li, X.; Cao, L.; Liu, J.; Gao, Y.; Li, B.; Qiu, C.; Bao, W.; et al. Efficacy and Tolerability of Repetitive Transcranial Magnetic Stimulation for the Treatment of Obsessive-Compulsive Disorder in Adults: A Systematic Review and Network Meta-Analysis. Transl. Psychiatry 2021, 11, 332. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial Direct Current Stimulation: State of the Art 2008. Brain Stimulat. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Reed, T.; Cohen Kadosh, R. Transcranial Electrical Stimulation (tES) Mechanisms and Its Effects on Cortical Excitability and Connectivity. J. Inherit. Metab. Dis. 2018, 41, 1123–1130. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Hegefeld, T.L.; Petersen, M.; Patterson, J.C.; Yossi, C.; Slizewski, J.; Osumi, A.; Cornett, E.M.; Kaye, A.; Kaye, J.S.; et al. Transcranial Magnetic Stimulation for Post-Traumatic Stress Disorder. Front. Psychiatry 2022, 13, 701348. [Google Scholar] [CrossRef]
- Kan, R.L.D.; Zhang, B.B.B.; Zhang, J.J.Q.; Kranz, G.S. Non-Invasive Brain Stimulation for Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. Transl. Psychiatry 2020, 10, 168. [Google Scholar] [CrossRef]
- McGirr, A.; Devoe, D.J.; Raedler, A.; Debert, C.T.; Ismail, Z.; Berlim, M.T. Repetitive Transcranial Magnetic Stimulation for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review and Network Meta-Analysis: La Stimulation Magnétique Transcrânienne Répétitive Pour Le Traitement Du Trouble de Stress Post-Traumatique: Une Revue Systématique et Une Méta-Analyse En Réseau. Can. J. Psychiatry Rev. Can. Psychiatr. 2021, 66, 763–773. [Google Scholar] [CrossRef]
- McNally, R.J. Mechanisms of Exposure Therapy: How Neuroscience Can Improve Psychological Treatments for Anxiety Disorders. Clin. Psychol. Rev. 2007, 27, 750–759. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Bowling, A.; Ebrahim, S. Handbook of Health Research Methods: Investigation, Measurement and Analysis; McGraw-Hill Education: London, UK, 2005; ISBN 0-335-21460-6. [Google Scholar]
- Strothmann, M. Zotero: A Guide for Librarians, Researchers and Educators. Ref. User Serv. Q. 2018, 57, 222–223. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizadeh, M.-J.; Rezaei, M.; Fitzgerald, P.B. Transcranial Direct Current Stimulation (tDCS) for Post-Traumatic Stress Disorder (PTSD): A Randomized, Double-Blinded, Controlled Trial. Brain Res. Bull. 2019, 153, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizadeh, M.-J.; Rezaei, M. Unilateral Right and Bilateral Dorsolateral Prefrontal Cortex Transcranial Magnetic Stimulation in Treatment Post-Traumatic Stress Disorder: A Randomized Controlled Study. Brain Res. Bull. 2018, 140, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Boggio, P.S.; Rocha, M.; Oliveira, M.O.; Fecteau, S.; Cohen, R.B.; Campanhã, C.; Ferreira-Santos, E.; Meleiro, A.; Corchs, F.; Zaghi, S.; et al. Noninvasive Brain Stimulation with High-Frequency and Low-Intensity Repetitive Transcranial Magnetic Stimulation Treatment for Posttraumatic Stress Disorder. J. Clin. Psychiatry 2010, 71, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Bozzay, M.L.; Brigido, S.; van’t Wout-Frank, M.; Aiken, E.; Swift, R.; Philip, N.S. Intermittent Theta Burst Stimulation in Veterans with Mild Alcohol Use Disorder. J. Affect. Disord. 2021, 293, 314–319. [Google Scholar] [CrossRef]
- Cohen, H.; Kaplan, Z.; Kotler, M.; Kouperman, I.; Moisa, R.; Grisaru, N. Repetitive Transcranial Magnetic Stimulation of the Right Dorsolateral Prefrontal Cortex in Posttraumatic Stress Disorder: A Double-Blind, Placebo-Controlled Study. Am. J. Psychiatry 2004, 161, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Fryml, L.D.; Pelic, C.G.; Acierno, R.; Tuerk, P.; Yoder, M.; Borckardt, J.J.; Juneja, N.; Schmidt, M.; Beaver, K.L.; George, M.S. Exposure Therapy and Simultaneous Repetitive Transcranial Magnetic Stimulation: A Controlled Pilot Trial for the Treatment of Posttraumatic Stress Disorder. J. ECT 2019, 35, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Grisaru, N.; Amir, M.; Cohen, H.; Kaplan, Z. Effect of Transcranial Magnetic Stimulation in Posttraumatic Stress Disorder: A Preliminary Study. Biol. Psychiatry 1998, 44, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Isserles, M.; Shalev, A.Y.; Roth, Y.; Peri, T.; Kutz, I.; Zlotnick, E.; Zangen, A. Effectiveness of Deep Transcranial Magnetic Stimulation Combined with a Brief Exposure Procedure in Post-Traumatic Stress Disorder—A Pilot Study. Brain Stimulat. 2013, 6, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Isserles, M.; Tendler, A.; Roth, Y.; Bystritsky, A.; Blumberger, D.M.; Ward, H.; Feifel, D.; Viner, L.; Duffy, W.; Zohar, J.; et al. Deep Transcranial Magnetic Stimulation Combined with Brief Exposure for Posttraumatic Stress Disorder: A Prospective Multisite Randomized Trial. Biol. Psychiatry 2021, 90, 721–728. [Google Scholar] [CrossRef]
- Kozel, F.A.; Motes, M.A.; Didehbani, N.; DeLaRosa, B.; Bass, C.; Schraufnagel, C.D.; Jones, P.; Morgan, C.R.; Spence, J.S.; Kraut, M.A.; et al. Repetitive TMS to Augment Cognitive Processing Therapy in Combat Veterans of Recent Conflicts with PTSD: A Randomized Clinical Trial. J. Affect. Disord. 2018, 229, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Kozel, F.A.; Van Trees, K.; Larson, V.; Phillips, S.; Hashimie, J.; Gadbois, B.; Johnson, S.; Gallinati, J.; Barrett, B.; Toyinbo, P.; et al. One Hertz versus Ten Hertz Repetitive TMS Treatment of PTSD: A Randomized Clinical Trial. Psychiatry Res. 2019, 273, 153–162. [Google Scholar] [CrossRef]
- Leong, K.; Chan, P.; Ong, L.; Zwicker, A.; Willan, S.; Lam, R.W.; McGirr, A. A Randomized Sham-Controlled Trial of 1-Hz and 10-Hz Repetitive Transcranial Magnetic Stimulation (rTMS) of the Right Dorsolateral Prefrontal Cortex in Civilian Post-Traumatic Stress Disorder: Un Essai Randomisé Contrôlé Simulé de Stimulation Magnétique Transcrânienne Repetitive (SMTr) de 1 Hz et 10 Hz Du Cortex Préfrontal Dorsolatéral Droit Dans Le Trouble de Stress Post-Traumatique Chez Des Civils. Can. J. Psychiatry Rev. Can. Psychiatr. 2020, 65, 770–778. [Google Scholar] [CrossRef]
- Madore, M.R.; Kozel, F.A.; Williams, L.M.; Green, L.C.; George, M.S.; Holtzheimer, P.E.; Yesavage, J.A.; Philip, N.S. Prefrontal Transcranial Magnetic Stimulation for Depression in US Military Veterans—A Naturalistic Cohort Study in the Veterans Health Administration. J. Affect. Disord. 2022, 297, 671–678. [Google Scholar] [CrossRef]
- Marcolin, K.A.D.S.; da Cunha, Â.B.M.; Yoneyama, B.C.; Ribeiro, T.A. Effects of Transcranial Direct Current Stimulation (tDCS) in “Kiss Nightclub Fire” Patients with Post-Traumatic Stress Disorder (PTSD): A Phase II Clinical Trial. SAGE Open Med. 2023, 11, 20503121231160953. [Google Scholar] [CrossRef]
- Nam, D.-H.; Pae, C.-U.; Chae, J.-H. Low-Frequency, Repetitive Transcranial Magnetic Stimulation for the Treatment of Patients with Posttraumatic Stress Disorder: A Double-Blind, Sham-Controlled Study. Clin. Psychopharmacol. Neurosci. Off. Sci. J. Korean Coll. Neuropsychopharmacol. 2013, 11, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Nursey, J.; Sbisa, A.; Knight, H.; Ralph, N.; Cowlishaw, S.; Forbes, D.; O’Donnell, M.; Hinton, M.; Cooper, J.; Hopwood, M.; et al. Exploring Theta Burst Stimulation for Post-Traumatic Stress Disorder in Australian Veterans—A Pilot Study. Mil. Med. 2020, 185, e1770–e1778. [Google Scholar] [CrossRef] [PubMed]
- Osuch, E.A.; Benson, B.E.; Luckenbaugh, D.A.; Geraci, M.; Post, R.M.; McCann, U. Repetitive TMS Combined with Exposure Therapy for PTSD: A Preliminary Study. J. Anxiety Disord. 2009, 23, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Oznur, T.; Akarsu, S.; Celik, C.; Bolu, A.; Ozdemir, B.; Akcay, B.D.; Ozselek, S.; Bozkurt, A.; Ozmenler, K.N. Is Transcranial Magnetic Stimulation Effective in Treatment-Resistant Combat Related Posttraumatic Stress Disorder? Neurosci. Riyadh Saudi Arab. 2014, 19, 29–32. [Google Scholar]
- Philip, N.S.; Ridout, S.J.; Albright, S.E.; Sanchez, G.; Carpenter, L.L. 5-Hz Transcranial Magnetic Stimulation for Comorbid Posttraumatic Stress Disorder and Major Depression. J. Trauma. Stress 2016, 29, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.S.; Barredo, J.; Aiken, E.; Larson, V.; Jones, R.N.; Shea, M.T.; Greenberg, B.D.; van’t Wout-Frank, M. Theta-Burst Transcranial Magnetic Stimulation for Posttraumatic Stress Disorder. Am. J. Psychiatry 2019, 176, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.B.; Mehndiratta, R.B.; Mehndiratta, Y.P.; Wamer, A.; Rosse, R.B.; Balish, M. Repetitive Transcranial Magnetic Stimulation Treatment of Comorbid Posttraumatic Stress Disorder and Major Depression. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 270–276. [Google Scholar] [CrossRef]
- Smits, F.M.; Geuze, E.; Schutter, D.J.L.G.; van Honk, J.; Gladwin, T.E. Effects of tDCS during Inhibitory Control Training on Performance and PTSD, Aggression and Anxiety Symptoms: A Randomized-Controlled Trial in a Military Sample. Psychol. Med. 2021, 52, 3964–3974. [Google Scholar] [CrossRef]
- Thierrée, S.; Raulin-Briot, M.; Legrand, M.; Le Gouge, A.; Vancappel, A.; Tudorache, A.-C.; Brizard, B.; Clarys, D.; Caille, A.; El-Hage, W. Combining Trauma Script Exposure with rTMS to Reduce Symptoms of Post-Traumatic Stress Disorder: Randomized Controlled Trial. Neuromodulation J. Int. Neuromodulation Soc. 2022, 25, 549–557. [Google Scholar] [CrossRef]
- van’t Wout-Frank, M.; Shea, M.T.; Larson, V.C.; Greenberg, B.D.; Philip, N.S. Combined Transcranial Direct Current Stimulation with Virtual Reality Exposure for Posttraumatic Stress Disorder: Feasibility and Pilot Results. Brain Stimulat. 2019, 12, 41–43. [Google Scholar] [CrossRef]
- van’t Wout-Frank, M.; Shea, M.T.; Sorensen, D.O.; Faucher, C.R.; Greenberg, B.D.; Philip, N.S. A Secondary Analysis on Effects of Theta Burst Transcranial Magnetic Stimulation to Reduce Anger in Veterans with Posttraumatic Stress Disorder. Neuromodulation J. Int. Neuromodulation Soc. 2021, 24, 870–878. [Google Scholar] [CrossRef] [PubMed]
- van’t Wout-Frank, M.; Philip, N.S. Simultaneous Application of Transcranial Direct Current Stimulation during Virtual Reality Exposure. J. Vis. Exp. JoVE 2021, 167, e61795. [Google Scholar] [CrossRef]
- Watts, B.V.; Landon, B.; Groft, A.; Young-Xu, Y. A Sham Controlled Study of Repetitive Transcranial Magnetic Stimulation for Posttraumatic Stress Disorder. Brain Stimulat. 2012, 5, 38–43. [Google Scholar] [CrossRef]
- Wilkes, S.; Ona, C.; Yang, M.; Liu, P.; Benton, A.; Lustik, M.; Coleman, J. Impacts of rTMS on Refractory Depression and Comorbid PTSD Symptoms at a Military Treatment Facility. Mil. Med. 2020, 185, e1420–e1427. [Google Scholar] [CrossRef]
- Yuan, H.; Liu, B.; Li, F.; Jin, Y.; Zheng, S.; Ma, Z.; Wu, Z.; Chen, C.; Zhang, L.; Gu, Y.; et al. Effects of Intermittent Theta-Burst Transcranial Magnetic Stimulation on Post-Traumatic Stress Disorder Symptoms: A Randomized Controlled Trial. Psychiatry Res. 2023, 329, 115533. [Google Scholar] [CrossRef] [PubMed]
- Zandvakili, A.; Philip, N.S.; Jones, S.R.; Tyrka, A.R.; Greenberg, B.D.; Carpenter, L.L. Use of Machine Learning in Predicting Clinical Response to Transcranial Magnetic Stimulation in Comorbid Posttraumatic Stress Disorder and Major Depression: A Resting State Electroencephalography Study. J. Affect. Disord. 2019, 252, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Pell, G.S.; Roth, Y.; Zangen, A. Modulation of Cortical Excitability Induced by Repetitive Transcranial Magnetic Stimulation: Influence of Timing and Geometrical Parameters and Underlying Mechanisms. Prog. Neurobiol. 2011, 93, 59–98. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-Z.; Edwards, M.J.; Rounis, E.; Bhatia, K.P.; Rothwell, J.C. Theta Burst Stimulation of the Human Motor Cortex. Neuron 2005, 45, 201–206. [Google Scholar] [CrossRef]
- Foa, E.B.; Hembree, E.; Rothbaum, B. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences, Therapist Guide; Oxford University Press: Oxford, UK, 2007; ISBN 978-0-19-530850-1. [Google Scholar]
- Resick, P.A.; Monson, C.M.; Chard, K.M. Cognitive Processing Therapy for PTSD: A Comprehensive Manual; Guilford Publications: New York, NY, USA, 2016; ISBN 1-4625-2864-3. [Google Scholar]
- Nitsche, M.A.; Paulus, W. Excitability Changes Induced in the Human Motor Cortex by Weak Transcranial Direct Current Stimulation. J. Physiol. 2000, 527 Pt 3, 633–639. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained Excitability Elevations Induced by Transcranial DC Motor Cortex Stimulation in Humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef] [PubMed]
- Aupperle, R.L.; Allard, C.B.; Grimes, E.M.; Simmons, A.N.; Flagan, T.; Behrooznia, M.; Cissell, S.H.; Twamley, E.W.; Thorp, S.R.; Norman, S.B.; et al. Dorsolateral Prefrontal Cortex Activation during Emotional Anticipation and Neuropsychological Performance in Posttraumatic Stress Disorder. Arch. Gen. Psychiatry 2012, 69, 360–371. [Google Scholar] [CrossRef] [PubMed]
- Olson, E.A.; Kaiser, R.H.; Pizzagalli, D.A.; Rauch, S.L.; Rosso, I.M. Regional Prefrontal Resting-State Functional Connectivity in Posttraumatic Stress Disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Kunimatsu, A.; Yasaka, K.; Akai, H.; Kunimatsu, N.; Abe, O. MRI Findings in Posttraumatic Stress Disorder. J. Magn. Reson. Imaging JMRI 2020, 52, 380–396. [Google Scholar] [CrossRef] [PubMed]
- Iwabuchi, S.J.; Raschke, F.; Auer, D.P.; Liddle, P.F.; Lankappa, S.T.; Palaniyappan, L. Targeted Transcranial Theta-Burst Stimulation Alters Fronto-Insular Network and Prefrontal GABA. NeuroImage 2017, 146, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Haris, E.M.; Bryant, R.A.; Williamson, T.; Korgaonkar, M.S. Functional Connectivity of Amygdala Subnuclei in PTSD: A Narrative Review. Mol. Psychiatry 2023, 28, 3581–3594. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Troubat, R.; Brizard, B.; Le Guisquet, A.-M.; Belzung, C.; El-Hage, W. Prefrontal Cortex rTMS Reverses Behavioral Impairments and Differentially Activates C-Fos in a Mouse Model of Post-Traumatic Stress Disorder. Brain Stimulat. 2019, 12, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Alexandra Kredlow, M.; Fenster, R.J.; Laurent, E.S.; Ressler, K.J.; Phelps, E.A. Prefrontal Cortex, Amygdala, and Threat Processing: Implications for PTSD. Neuropsychopharmacology 2022, 47, 247–259. [Google Scholar] [CrossRef]
- Ferro, M.; Lamanna, J.; Spadini, S.; Nespoli, A.; Sulpizio, S.; Malgaroli, A. Synaptic Plasticity Mechanisms behind TMS Efficacy: Insights from Its Application to Animal Models. J. Neural Transm. Vienna Austria 1996 2022, 129, 25–36. [Google Scholar] [CrossRef]
- Bao, W.; Gao, Y.; Cao, L.; Li, H.; Liu, J.; Liang, K.; Hu, X.; Zhang, L.; Hu, X.; Gong, Q.; et al. Alterations in Large-Scale Functional Networks in Adult Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis of Resting-State Functional Connectivity Studies. Neurosci. Biobehav. Rev. 2021, 131, 1027–1036. [Google Scholar] [CrossRef]
- Mowinckel, A.M.; Vidal-Piñeiro, D. Visualization of Brain Statistics with R Packages Ggseg and Ggseg3d. Adv. Methods Pract. Psychol. Sci. 2020, 3, 466–483. [Google Scholar] [CrossRef]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T. An Automated Labeling System for Subdividing the Human Cerebral Cortex on MRI Scans into Gyral Based Regions of Interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; Van Der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S. Whole Brain Segmentation: Automated Labeling of Neuroanatomical Structures in the Human Brain. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef] [PubMed]
- Barsaglini, A.; Sartori, G.; Benetti, S.; Pettersson-Yeo, W.; Mechelli, A. The Effects of Psychotherapy on Brain Function: A Systematic and Critical Review. Prog. Neurobiol. 2014, 114, 1–14. [Google Scholar] [CrossRef]
- Farrow, T.F.D.; Hunter, M.D.; Wilkinson, I.D.; Gouneea, C.; Fawbert, D.; Smith, R.; Lee, K.-H.; Mason, S.; Spence, S.A.; Woodruff, P.W.R. Quantifiable Change in Functional Brain Response to Empathic and Forgivability Judgments with Resolution of Posttraumatic Stress Disorder. Psychiatry Res. 2005, 140, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.J.; Francis, J.; Friedlander, J.; Banks-Williams, L.; Lande, R.G.; Taylor, P.; Blair, J.; McLellan, J.; Law, W.; Tarpley, V.; et al. Improvement in Cerebral Function with Treatment of Posttraumatic Stress Disorder. Ann. N. Y. Acad. Sci. 2010, 1208, 142–149. [Google Scholar] [CrossRef]
- Felmingham, K.; Kemp, A.; Williams, L.; Das, P.; Hughes, G.; Peduto, A.; Bryant, R. Changes in Anterior Cingulate and Amygdala after Cognitive Behavior Therapy of Posttraumatic Stress Disorder. Psychol. Sci. 2007, 18, 127–129. [Google Scholar] [CrossRef]
- Lindauer, R.J.L.; Booij, J.; Habraken, J.B.A.; van Meijel, E.P.M.; Uylings, H.B.M.; Olff, M.; Carlier, I.V.E.; den Heeten, G.J.; van Eck-Smit, B.L.F.; Gersons, B.P.R. Effects of Psychotherapy on Regional Cerebral Blood Flow during Trauma Imagery in Patients with Post-Traumatic Stress Disorder: A Randomized Clinical Trial. Psychol. Med. 2008, 38, 543–554. [Google Scholar] [CrossRef]
- Peres, J.F.P.; Newberg, A.B.; Mercante, J.P.; Simão, M.; Albuquerque, V.E.; Peres, M.J.P.; Nasello, A.G. Cerebral Blood Flow Changes during Retrieval of Traumatic Memories before and after Psychotherapy: A SPECT Study. Psychol. Med. 2007, 37, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.; Lee, S.; Cho, T.; Kim, S.-W.; Kim, M.; Yoon, Y.; Kim, K.K.; Byun, J.; Kim, S.J.; Jeong, J.; et al. Neural Circuits Underlying a Psychotherapeutic Regimen for Fear Disorders. Nature 2019, 566, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Montesano, G.; Belfiore, M.; Ripamonti, M.; Arena, A.; Lamanna, J.; Ferro, M.; Zimarino, V.; Ambrosi, A.; Malgaroli, A. Effects of the Concomitant Activation of ON and OFF Retinal Ganglion Cells on the Visual Thalamus: Evidence for an Enhanced Recruitment of GABAergic Cells. Front. Neural Circuits 2015, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Rothbaum, B.O.; Cahill, S.P.; Foa, E.B.; Davidson, J.R.T.; Compton, J.; Connor, K.M.; Astin, M.C.; Hahn, C.-G. Augmentation of Sertraline with Prolonged Exposure in the Treatment of Posttraumatic Stress Disorder. J. Trauma. Stress 2006, 19, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Chervyakov, A.V.; Chernyavsky, A.Y.; Sinitsyn, D.O.; Piradov, M.A. Possible Mechanisms Underlying the Therapeutic Effects of Transcranial Magnetic Stimulation. Front. Hum. Neurosci. 2015, 9, 303. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Tang, Y.; Lin, J.; Faulkner, G.; Tsang, H.W.H.; Chan, S.H.W. Non-Invasive Brain Stimulation Combined with Psychosocial Intervention for Depression: A Systematic Review and Meta-Analysis. BMC Psychiatry 2022, 22, 273. [Google Scholar] [CrossRef]
- Tatti, E.; Phillips, A.L.; Paciorek, R.; Romanella, S.M.; Dettore, D.; Di Lorenzo, G.; Ruffini, G.; Rossi, S.; Santarnecchi, E. Boosting Psychological Change: Combining Non-Invasive Brain Stimulation with Psychotherapy. Neurosci. Biobehav. Rev. 2022, 142, 104867. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.C. Metaplasticity: Tuning Synapses and Networks for Plasticity. Nat. Rev. Neurosci. 2008, 9, 387. [Google Scholar] [CrossRef]
- Lamanna, J.; Malgaroli, A.; Cerutti, S.; Signorini, M.G. Detection of Fractal Behavior in Temporal Series of Synaptic Quantal Release Events: A Feasibility Study. Comput. Intell. Neurosci. 2012, 2012, 704673. [Google Scholar] [CrossRef]
- Lamanna, J.; Signorini, M.G.; Cerutti, S.; Malgaroli, A. A Pre-Docking Source for the Power-Law Behavior of Spontaneous Quantal Release: Application to the Analysis of LTP. Front. Cell. Neurosci. 2015, 9, 44. [Google Scholar] [CrossRef]
- D’Acunzo, P.; Badaloni, A.; Ferro, M.; Ripamonti, M.; Zimarino, V.; Malgaroli, A.; Consalez, G.G. A Conditional Transgenic Reporter of Presynaptic Terminals Reveals Novel Features of the Mouse Corticospinal Tract. Front. Neuroanat. 2014, 7, 50. [Google Scholar] [CrossRef]
- Ferro, M.; Lamanna, J.; Ripamonti, M.; Racchetti, G.; Arena, A.; Spadini, S.; Montesano, G.; Cortese, R.; Zimarino, V.; Malgaroli, A. Functional Mapping of Brain Synapses by the Enriching Activity-Marker SynaptoZip. Nat. Commun. 2017, 8, 1229. [Google Scholar] [CrossRef]
- Schulte, C.; Lamanna, J.; Moro, A.S.; Piazzoni, C.; Borghi, F.; Chighizola, M.; Ortoleva, S.; Racchetti, G.; Lenardi, C.; Podestà, A.; et al. Neuronal Cells Confinement by Micropatterned Cluster-Assembled Dots with Mechanotransductive Nanotopography. ACS Biomater. Sci. Eng. 2018, 4, 4062–4075. [Google Scholar] [CrossRef]
- Armenta, R.F.; Walter, K.H.; Geronimo-Hara, T.R.; Porter, B.; Stander, V.A.; LeardMann, C.A.; Bauer, L.; Boparai, S.; Bukowinski, A.; Carballo, C.; et al. Longitudinal Trajectories of Comorbid PTSD and Depression Symptoms among U.S. Service Members and Veterans. BMC Psychiatry 2019, 19, 396. [Google Scholar] [CrossRef]
- Brier, Z.M.F.; Connor, J.; Legrand, A.C.; Price, M. Different Trajectories of PTSD Symptoms during the Acute Post-Trauma Period. J. Psychiatr. Res. 2020, 131, 127–131. [Google Scholar] [CrossRef]
- Phelps, A.J.; Steele, Z.; Cowlishaw, S.; Metcalf, O.; Alkemade, N.; Elliott, P.; O’Donnell, M.; Redston, S.; Kerr, K.; Howard, A.; et al. Treatment Outcomes for Military Veterans with Posttraumatic Stress Disorder: Response Trajectories by Symptom Cluster. J. Trauma. Stress 2018, 31, 401–409. [Google Scholar] [CrossRef]
- Xu, Y.; Vandeleur, C.; Müller, M.; Seifritz, E.; Kleim, B.; von Känel, R.; Wagner, E.-Y.N.; Strippoli, M.-P.F.; Castelao, E.; Gholamrezaee, M.M.; et al. Retrospectively Assessed Trajectories of PTSD Symptoms and Their Subsequent Comorbidities. J. Psychiatr. Res. 2021, 136, 71–79. [Google Scholar] [CrossRef]
- Maya Vetencourt, J.F.; Sale, A.; Viegi, A.; Baroncelli, L.; De Pasquale, R.; O’Leary, O.F.; Castrén, E.; Maffei, L. The Antidepressant Fluoxetine Restores Plasticity in the Adult Visual Cortex. Science 2008, 320, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Popova, D.; Castrén, E.; Taira, T. Chronic Fluoxetine Administration Enhances Synaptic Plasticity and Increases Functional Dynamics in Hippocampal CA3-CA1 Synapses. Neuropharmacology 2017, 126, 250–256. [Google Scholar] [CrossRef]
- Puścian, A.; Winiarski, M.; Łęski, S.; Charzewski, Ł.; Nikolaev, T.; Borowska, J.; Dzik, J.M.; Bijata, M.; Lipp, H.-P.; Dziembowska, M.; et al. Chronic Fluoxetine Treatment Impairs Motivation and Reward Learning by Affecting Neuronal Plasticity in the Central Amygdala. Br. J. Pharmacol. 2021, 178, 672–688. [Google Scholar] [CrossRef]
- Liebetanz, D.; Nitsche, M.A.; Tergau, F.; Paulus, W. Pharmacological Approach to the Mechanisms of Transcranial DC-Stimulation-Induced after-Effects of Human Motor Cortex Excitability. Brain J. Neurol. 2002, 125, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Grundey, J.; Liebetanz, D.; Lang, N.; Tergau, F.; Paulus, W. Catecholaminergic Consolidation of Motor Cortical Neuroplasticity in Humans. Cereb. Cortex 2004, 14, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Kuo, M.-F.; Karrasch, R.; Wächter, B.; Liebetanz, D.; Paulus, W. Serotonin Affects Transcranial Direct Current-Induced Neuroplasticity in Humans. Biol. Psychiatry 2009, 66, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Dietch, J.R.; Ruggero, C.J.; Schuler, K.; Taylor, D.J.; Luft, B.J.; Kotov, R. Posttraumatic Stress Disorder Symptoms and Sleep in the Daily Lives of World Trade Center Responders. J. Occup. Health Psychol. 2019, 24, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Dossi, G.; Delvecchio, G.; Prunas, C.; Soares, J.C.; Brambilla, P. Neural Bases of Cognitive Impairments in Post-Traumatic Stress Disorders: A Mini-Review of Functional Magnetic Resonance Imaging Findings. Front. Psychiatry 2020, 11, 176. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, X. Sudden Gains in Social Functioning and PTSD Improvement. Nat. Rev. Psychol. 2023, 2, 718. [Google Scholar] [CrossRef]
- Moro, A.S.; Saccenti, D.; Ferro, M.; Scaini, S.; Malgaroli, A.; Lamanna, J. Neural Correlates of Delay Discounting in the Light of Brain Imaging and Non-Invasive Brain Stimulation: What We Know and What Is Missed. Brain Sci. 2023, 13, 403. [Google Scholar] [CrossRef]
- Moro, A.S.; Saccenti, D.; Vergallito, A.; Scaini, S.; Malgaroli, A.; Ferro, M.; Lamanna, J. Transcranial Direct Current Stimulation (tDCS) over the Orbitofrontal Cortex Reduces Delay Discounting. Front. Behav. Neurosci. 2023, 17, 1239463. [Google Scholar] [CrossRef]
- Moro, A.S.; Saccenti, D.; Seccia, A.; Ferro, M.; Malgaroli, A.; Lamanna, J. Poke and Delayed Drink Intertemporal Choice Task (POKE-ADDICT): An Open-Source Behavioral Apparatus for Intertemporal Choice Testing in Rodents. Anim. Models Exp. Med. 2023, 6, 619–626. [Google Scholar] [CrossRef]
- Misitano, A.; Moro, A.S.; Ferro, M.; Forresi, B. The Dissociative Subtype of Post-Traumatic Stress Disorder: A Systematic Review of the Literature Using the Latent Profile Analysis. J. Trauma Dissociation 2022. online ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ID | Mean Age (Standard Deviation) | Biological Sex | Population Type | Diagnosis | Comorbidity | Traumatic Event | Mean Years Elapsed since Trauma |
|---|---|---|---|---|---|---|---|
| Grisaru et al., 1998 [57] | 40.50 (10.67) | 7 males 3 females | Outpatients | PTSD | - | Accident, assault, combat | 5.5 |
| Rosenberg et al., 2002 [71] | 54.80 (9.10) | 12 males | Veterans | PTSD | MDD | Combat | 28.9 |
| Cohen et al., 2004 [55] | 41.80 (6.93) | 17 males 7 females | Outpatients | PTSD | - | Abuse, accident, assault, combat, death of a relative | 5.5 |
| Osuch et al., 2009 [67] | 41.40 (12.30) | 1 male 8 females | Treatment-refractory Patients | PTSD | - | - | 22.3 |
| Boggio et al., 2010 [53] | 44.50 (4.40) | 9 males 21 females | Outpatients | PTSD | - | Abuse, assault, combat, death of a relative, perceived threat of harm | 3.9 |
| Watts et al., 2012 [77] | 55.90 (12.05) | 18 males 2 females | Treatment-refractory Patients | PTSD | MDD, PD, OCD, SUD | Abuse, accident, assault, combat, multiple | 39.8 |
| Nam et al., 2013 [65] | 34.31 (7.71) | 6 males 10 females | Outpatients | PTSD | - | Accident, assault, domestic violence | 3.3 |
| Isserles et al., 2013 [58] | 43.30 (10.93) | 20 males 6 females | Treatment-refractory Patients | PTSD | - | - | 15.8 |
| Oznur et al., 2014 [68] | 28.70 (3.30) | 20 males | Veterans | PTSD | MDD | Combat | 7.3 |
| Philip et al., 2016 [69] | 58.10 (13.9) | 8 males 2 females | Veterans | PTSD | MDD | Combat | - |
| Kozel et al., 2018 [60] | - | 103 males | Veterans | PTSD | - | Combat | - |
| Ahmadizadeh & Rezaei, 2018 [52] | 50.45 (7.31) | 58 males | Veterans | PTSD | - | Combat | 25.8 |
| Philip et al., 2018 [26] | 51.30 (11.10) | 10 males 13 females | Outpatients | PTSD | MDD | - | - |
| Fryml et al., 2019 [56] | 28.50 (2.35) | 7 males 1 female | Veterans | PTSD | - | Combat | - |
| Zandvakili et al., 2019 [80] | 51.60 (10.30) | 21 males 14 females | Veterans | PTSD | MDD | Combat | - |
| Philip et al., 2019 [70] | 50.50 (12.50) | 42 males 8 females | Veterans | PTSD | MDD, SUD | Combat | - |
| Kozel et al., 2019 [61] | 38.50 (6.35) | 25 males 10 females | Veterans | PTSD | - | Combat | 9.3 |
| Ahmadizadeh et al., 2019 [51] | 43.75 (10.56) | 14 males 26 females | Outpatients | PTSD | - | - | - |
| Marcolin et al., 2023 [64] | 30.88 (7.74) | 1 male 7 females | Civilians | PTSD | - | Perceived threat of harm, witnessing death, or serious injury | - |
| Van’t Wout-Frank et al., 2019 [74] | 40.50 (8.80) | 12 males | Veterans | PTSD | - | Combat | - |
| Leong et al., 2020 [62] | 44.07 (10.93) | 5 males 24 females | Outpatients | PTSD | MDD, GAD, SP, PD, OCD | Perceived threat of harm, sexual violence, witnessing death, serious injury, multiple | - |
| Nursey et al., 2020 [66] | 37.52 (6.93) | 7 males 1 female | Veterans | PTSD | - | Combat | - |
| Wilkes et al., 2020 [78] | 39.50 (13.70) | 41 males 36 females | Outpatients | PTSD | MDD | - | - |
| Van’t Wout-Frank et al., 2021 [75] | 50.90 (12.20) | 42 males 8 females | Veterans | PTSD | MDD, SUD | Combat | - |
| Isserles et al., 2021 [59] | 44.25 (12.72) | 42 males 83 females | Outpatients | PTSD | - | - | - |
| Bozzay et al., 2021 [54] | 50.10 (12.30) | 42 males 8 females | Veterans | PTSD | SUD | Combat | - |
| Thierreé et al., 2021 [73] | 32.40 (10.55) | 23 males 15 females | Outpatients | PTSD | - | Accident, assault, combat, perceived threat of harm | 11.5 |
| Smits et al., 2021 [72] | 42.45 (10.00) | 89 males 7 females | Veterans | PTSD | - | Combat | - |
| Van’t Wout-Frank & Philip, 2021 [76] | - | 4 males | Veterans | PTSD | - | Combat | - |
| Madore et al., 2022 [63] | 51.84 (14.11) | 118 males 31 females | Veterans | PTSD | MDD | Combat | - |
| Yuan et al., 2023 [79] | 34.71 (7.96) | 20 males 55 females | Civilians | Highly Severe PTSD Symptoms | - | - | - |
| ID | Study Design | N | Brain Site TG | Protocol TG | Brain Site CG | Protocol CG | Augmentation | Clinical Measures | Effect | Assessment Timepoints | Study Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Grisaru et al., 1998 [57] | Open-label | 10 | Bilateral motor cortex | 0.3 Hz rTMS, 100% RMT, 1 session, 30 pulses per session. | - | - | Antidepressants | IES, SCL-90 | Decreased Avoidance, Anxiety, and Somatization. | Pre- and post-treatment, 1-week, and 1-month follow-ups | 2 |
| Rosenberg et al., 2002 [71] | Open-label | 12 | Left dlPFC | 1 Hz or 5 Hz rTMS, 90% RMT, 10 sessions, 600 pulses per session. | - | - | Antidepressants | MISS, HDRS, POMS | Decreased Overall PTSD Symptoms’ Severity, Anxiety, and Depression. | Pre- and post-treatment, 1-month and 2-month follow-ups | 1 |
| Cohen et al., 2004 [55] | RCT | 24 | Right dlPFC | 1 Hz or 10 Hz rTMS, 80% RMT, 10 sessions, 100 or 400 pulses per session. | Right dlPFC | Sham | Antidepressants, Anxiolytics, Mood Stabilizers, Antipsychotics | PCL, HARS, HDRS | Decreased Avoidance, Hyperarousal, Re-experiencing Anxiety, and Depression. | Pre- and post-treatment, 2-week follow-up | 1 |
| Osuch et al., 2009 [67] | Cross-over | 9 | Right dlPFC | 1 Hz rTMS, 100% RMT, 20 sessions, 1800 pulses per session. | Right dlPFC | Sham | Exposure Therapy | CAPS, IES, HDRS | Decreased Hyperarousal. | Pre- and post-treatment | 2 |
| Boggio et al., 2010 [53] | RCT | 30 | Left or Right dlPFC | 10 Hz rTMS, 80% RMT, 10 sessions, 1600 pulses per session. | Left or Right dlPFC | Sham | - | PCL, HARS, HDRS | Decreased Avoidance, Hyperarousal, Re-experiencing, Anxiety, and Depression. | Pre- and post-treatment, 2-week, 1-month, 2-month and 3-month follow-ups | 1 |
| Watts et al., 2012 [77] | RCT | 20 | Right dlPFC | 1 Hz rTMS, 90% RMT, 10 sessions, 400 pulses per session. | Right dlPFC | Sham | - | CAPS, PCL, BDI, STAI | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month and 2-month follow-ups | 1 |
| Nam et al., 2013 [65] | RCT | 16 | Right dlPFC | 1 Hz rTMS, 100% RMT, 15 sessions, 1200 pulses per session. | Right dlPFC | Sham | Antidepressants | CAPS | Decreased Avoidance and Re-experiencing. | Pre- and post-treatment, 1-month follow-up | 1 |
| Isserles et al., 2013 [58] | RCT | 26 | mPFC | dTMS, 120% RMT, 12 sessions, 1680 pulses per session. | mPFC | Sham | Antidepressants, Anxiolytics, Antipsychotics + Exposure Therapy | CAPS, PSS, BDI, HDRS | Decreased Intrusion. | Pre- and post-treatment, 2-week and 2-month follow-ups | 1 |
| Oznur et al., 2014 [68] | Open-label, retrospective | 20 | Right dlPFC | 1 Hz rTMS, 80% RMT, 20 sessions, 600 pulses per session. | - | - | - | IES, BAI, BDI | Decreased Hyperarousal. | Pre- and post-treatment | 2 |
| Philip et al., 2016 [69] | Open-label | 10 | Left dlPFC | 5 Hz rTMS, 120% RMT, 36 sessions, 3000 pulses per session. | - | - | - | PCL, QIDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment | 1 |
| Kozel et al., 2018 [60] | RCT | 103 | Right dlPFC | 1 Hz rTMS, 110% RMT, 12 sessions, 1800 pulses per session. | Right dlPFC | Sham | Cognitive Processing Therapy | CAPS, PCL, QIDS | Decreased Overall PTSD Symptoms’ Severity. | Pre- and post-treatment, 1-month, 3-month, and 6-month follow-ups | 1 |
| Ahmadizadeh & Rezaei, 2018 [52] | RCT | 58 | Bilateral or Right dlPFC | 20 Hz rTMS, 100% RMT, 10 sessions, 2400 pulses per session. | Bilateral dlPFC | Sham | - | PCL | Decreased Overall PTSD Symptoms’ Severity. | Pre- and post-treatment | 1 |
| Philip et al., 2018 [26] | Open-label | 33 | Left dlPFC | 5 Hz rTMS, 120% RMT, 36 sessions, 3000 pulses per session. | - | - | - | PCL, IDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment | 2 |
| Fryml et al., 2019 [56] | RCT | 8 | Left or Right dlPFC | 10 Hz rTMS, 120% RMT, 8 sessions, 6000 pulses per session. | Left or Right dlPFC | Sham | Antidepressants, Antipsychotics + Exposure Therapy | CAPS, PCL, HARS, HDRS | Decreased Depression. | Pre- and post-treatment | 1 |
| Kozel et al., 2019 [61] | Open-label | 35 | Right dlPFC | 1 Hz or 10 Hz rTMS, 110% RMT, 36 sessions, 2400 pulses per session. | - | - | - | CAPS, PCL, MADRS, QIDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month and 3-month follow-ups | 1 |
| Philip et al., 2019 [70] | RCT | 50 | Right dlPFC | iTBS, 80% AMT, 10 sessions, 1800 pulses per session. | Right dlPFC | Sham | - | CAPS, PCL, IDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month follow-up | 1 |
| Zandvakili et al., 2019 [80] | Open-label | 35 | Left dlPFC | 5 Hz rTMS, 120% RMT, 36 sessions, 3000 pulses per session. | - | - | - | PCL, IDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment | 2 |
| Leong et al., 2020 [62] | RCT | 29 | Right dlPFC | 1 Hz or 10 Hz rTMS, 120% RMT, 10 sessions, 2250 or 3000 pulses per session. | Right dlPFC | Sham | Antidepressants, Anxiolytics, Antipsychotics | CAPS, PCL, HDRS, QIDS, BAI, GAD-7 | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 3-month follow-up | 1 |
| Wilkes et al., 2020 [78] | Open-label, retrospective | 77 | - | 10 Hz rTMS, 120% RMT, 31 sessions. | - | - | Antidepressants | PCL, BDI | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 2-week follow-up | 2 |
| Nursey et al., 2020 [66] | Case series | 8 | Bilateral dlPFC | iTBS, 120% RMT, 20 sessions, 600 pulses per session. | - | - | Antidepressants, Anxiolytics, Mood Stabilizers, Antipsychotics | CAPS, HDRS | Decreased Avoidance, Negative Alterations in Cognition and Mood, and Depression. | Pre- and post-treatment, 3-month | 1 |
| Van’t Wout-Frank et al., 2021 [75] | RCT | 50 | Right dlPFC | iTBS, 80% AMT, 10 sessions, 1800 pulses per session. | Right dlPFC | Sham | - | PCL, IDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month follow-up | 1 |
| Bozzay et al., 2021 [54] | RCT | 50 | Right dlPFC | iTBS, 80% AMT, 10 sessions, 1800 pulses per session. | Right dlPFC | Sham | - | PCL, IDS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month follow-up | 1 |
| Isserles et al., 2021 [59] | RCT | 125 | mPFC | dTMS, 120% RMT, 12 sessions, 1680 pulses per session. | mPFC | Sham | Antidepressants, Anxiolytics + Exposure Therapy | CAPS, MPSS, HDRS | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment, 1-month follow-up | 1 |
| Thierreé et al., 2021 [73] | RCT | 38 | Right dlPFC | 1 Hz or 10 Hz rTMS, 70% or 110% RMT, 8 sessions, 300 or 3000 pulses per session. | - | - | Antidepressants + Exposure Therapy | CAPS, PCL, HARS, HDRS | Decreased Overall PTSD Symptoms’ Severity, Anxiety, and Depression. | Pre-treatment, 1-month and 3-month follow-ups | 1 |
| Madore et al., 2022 [63] | Open-label, retrospective | 149 | Left dlPFC | 10 Hz rTMS, 120% RMT, 36 sessions, 3000 pulses per session. | - | - | - | PCL, PHQ-9 | Decreased Overall PTSD Symptoms’ Severity and Depression. | Pre- and post-treatment | 1 |
| Yuan et al., 2023 [79] | RCT | 75 | Right dlPFC | 10 Hz rTMS or iTBS, 80% RMT, 15 sessions, 1800 pulses per session. | Right dlPFC | Sham | - | PCL | Decreased Overall PTSD Symptoms’ Severity. | Pre- and post-treatment, 1-month follow-up | 1 |
| ID | Study Design | N | Anodal/Cathodal Site TG | Protocol TG | Anodal/Cathodal Site CG | Protocol CG | Augmentation | Clinical Measures | Effect | Assessment Timepoints | Study Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ahmadizadeh et al., 2019 [51] | RCT | 40 | Left dlPFC/Right dlPFC | 2.0 mA, 0.57 A/m2, 10 sessions | Left dlPFC/Right dlPFC | Sham | - | PCL, BAI, BDI | Decreased Re-experiencing, Hyperarousal, Negative Alterations in Cognition and Mood, Depression, and Anxiety | Pre- and post-treatment, 1-month follow-up | 1 |
| Van’t Wout-Frank et al., 2019 [74] | Open-label | 12 | Left vmPFC/Right OC | 2.0 mA, 0.22 A/m2, 6 sessions | - | - | Exposure Therapy | PCL | Decreased Overall PTSD Symptoms’ Severity | Pre- and post-treatment, 1-month follow-up | 1 |
| Van’t Wout-Frank & Philip, 2021 [76] | Pilot | 4 | Left vmPFC/Right OC | 2.0 mA, 0.22 A/m2, 6 sessions | Left vmPFC/Right OC | Sham | Exposure Therapy | CAPS, PCL, QIDS | Decreased Overall PTSD Symptoms’ Severity | Pre- and post-treatment | 2 |
| Smits et al., 2021 [72] | RCT | 96 | Right IFG/Left OFC | 1.25 mA, 0.04 A/m2, 5 sessions | Right IFG/Left OFC | Sham | Antidepressants, Anxiolytics, Mood Stabilizers, Antipsychotics, EMDR, and CBT + Inhibitory Control Training | PCL, STAI, BDI | - | Pre- and post-treatment, 3-month and 1-year follow-ups | 1 |
| Marcolin et al., 2023 [64] | Open-label | 8 | Left Deltoid Muscle | 2.0 mA, 0.08 A/m2, 10 sessions | - | - | - | PCL, HARS, HDRS | Decreased Overall PTSD Symptoms’ Severity, Anxiety, and Depression | Pre- and post-treatment, 1-month and 3-month follow-ups | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saccenti, D.; Lodi, L.; Moro, A.S.; Scaini, S.; Forresi, B.; Lamanna, J.; Ferro, M. Novel Approaches for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review of Non-Invasive Brain Stimulation Interventions and Insights from Clinical Trials. Brain Sci. 2024, 14, 210. https://doi.org/10.3390/brainsci14030210
Saccenti D, Lodi L, Moro AS, Scaini S, Forresi B, Lamanna J, Ferro M. Novel Approaches for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review of Non-Invasive Brain Stimulation Interventions and Insights from Clinical Trials. Brain Sciences. 2024; 14(3):210. https://doi.org/10.3390/brainsci14030210
Chicago/Turabian StyleSaccenti, Daniele, Leandro Lodi, Andrea Stefano Moro, Simona Scaini, Barbara Forresi, Jacopo Lamanna, and Mattia Ferro. 2024. "Novel Approaches for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review of Non-Invasive Brain Stimulation Interventions and Insights from Clinical Trials" Brain Sciences 14, no. 3: 210. https://doi.org/10.3390/brainsci14030210
APA StyleSaccenti, D., Lodi, L., Moro, A. S., Scaini, S., Forresi, B., Lamanna, J., & Ferro, M. (2024). Novel Approaches for the Treatment of Post-Traumatic Stress Disorder: A Systematic Review of Non-Invasive Brain Stimulation Interventions and Insights from Clinical Trials. Brain Sciences, 14(3), 210. https://doi.org/10.3390/brainsci14030210