Behavioral and Brain Activity Indices of Cognitive Control Deficits in Binge Drinkers

Abstract
:1. Introduction
2. Materials and Method
2.1. Research Participants
2.2. Experimental Protocol
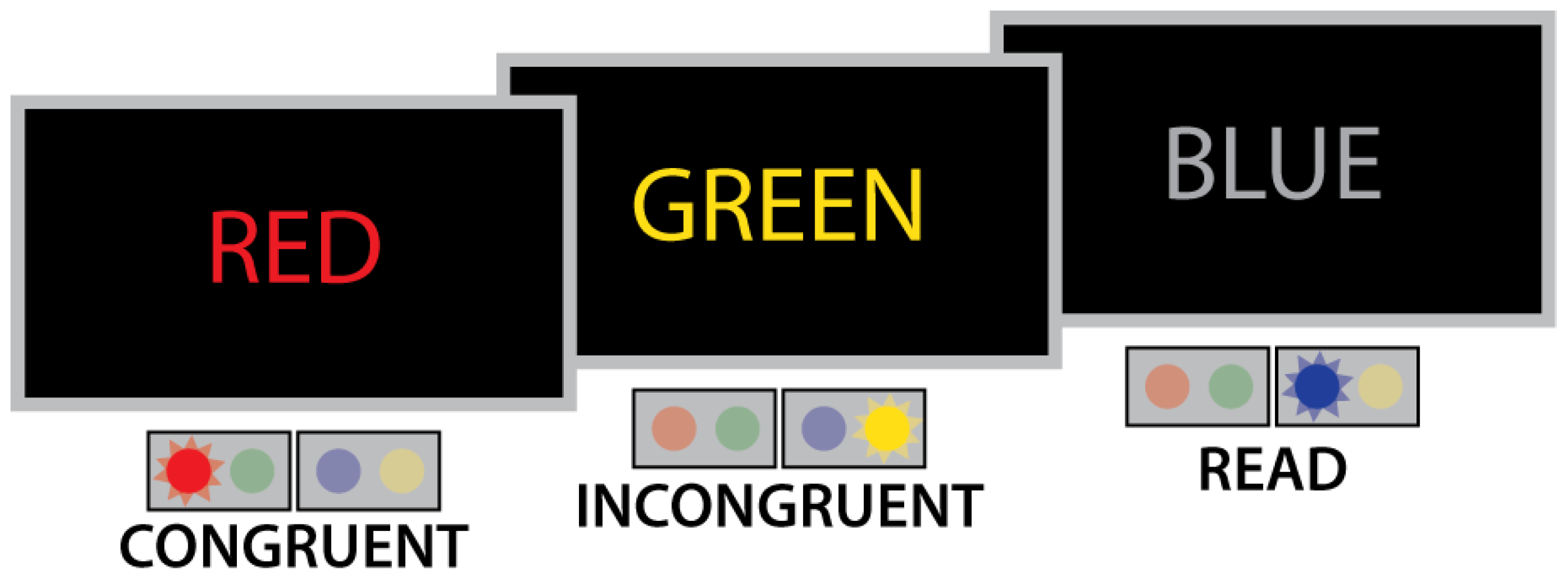
2.3. Task
2.4. Image Acquisition and Analysis
3. Results
3.1. Drinking and Personality Variables
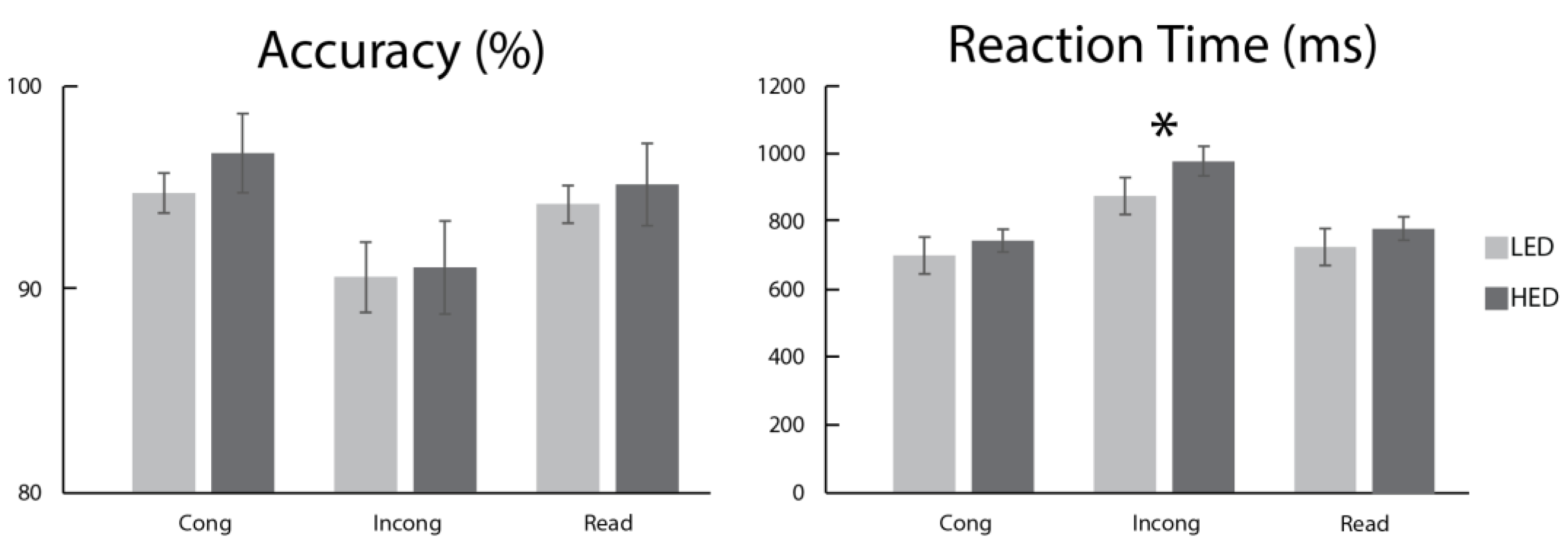
3.2. Task Performance
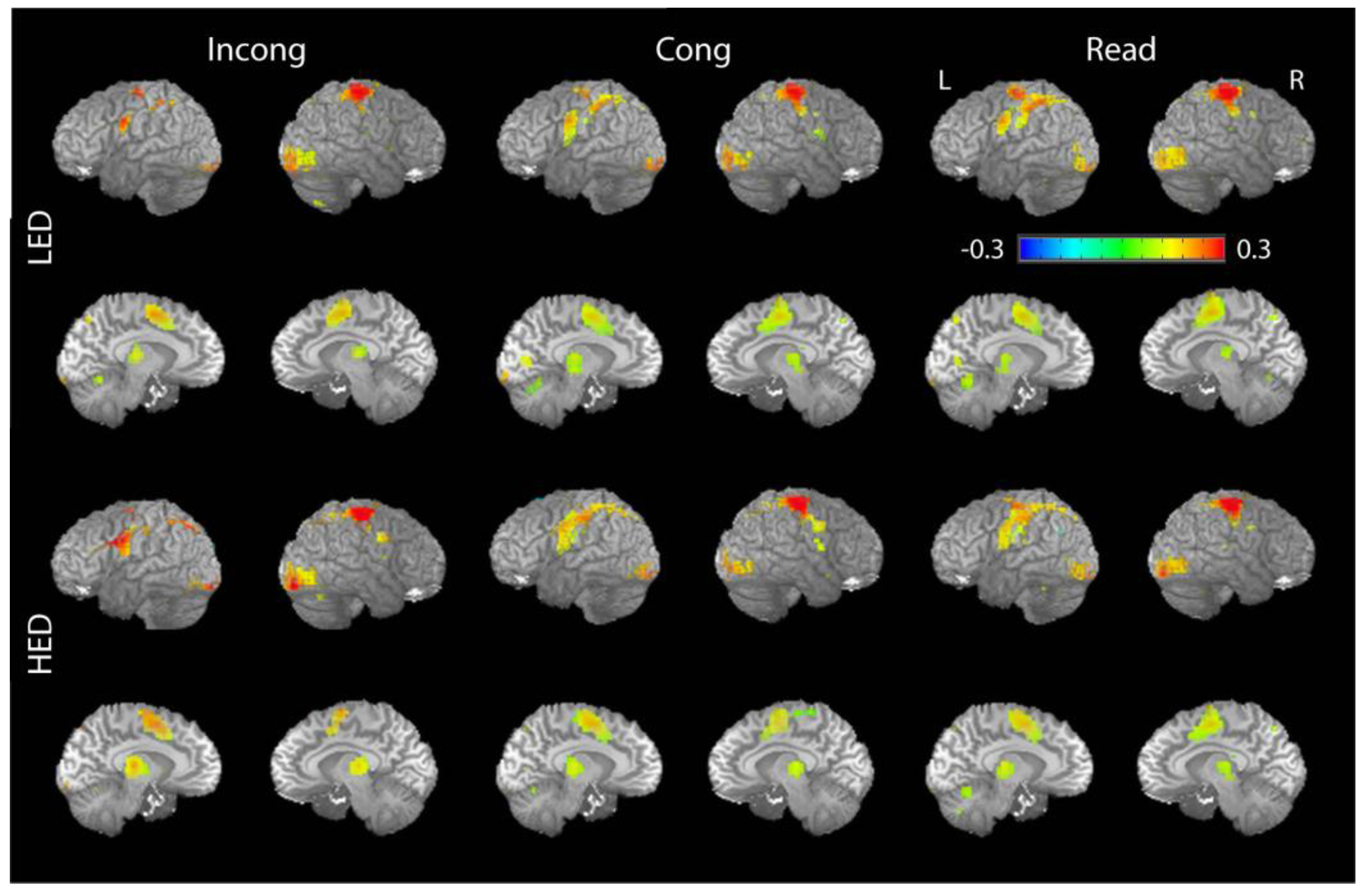
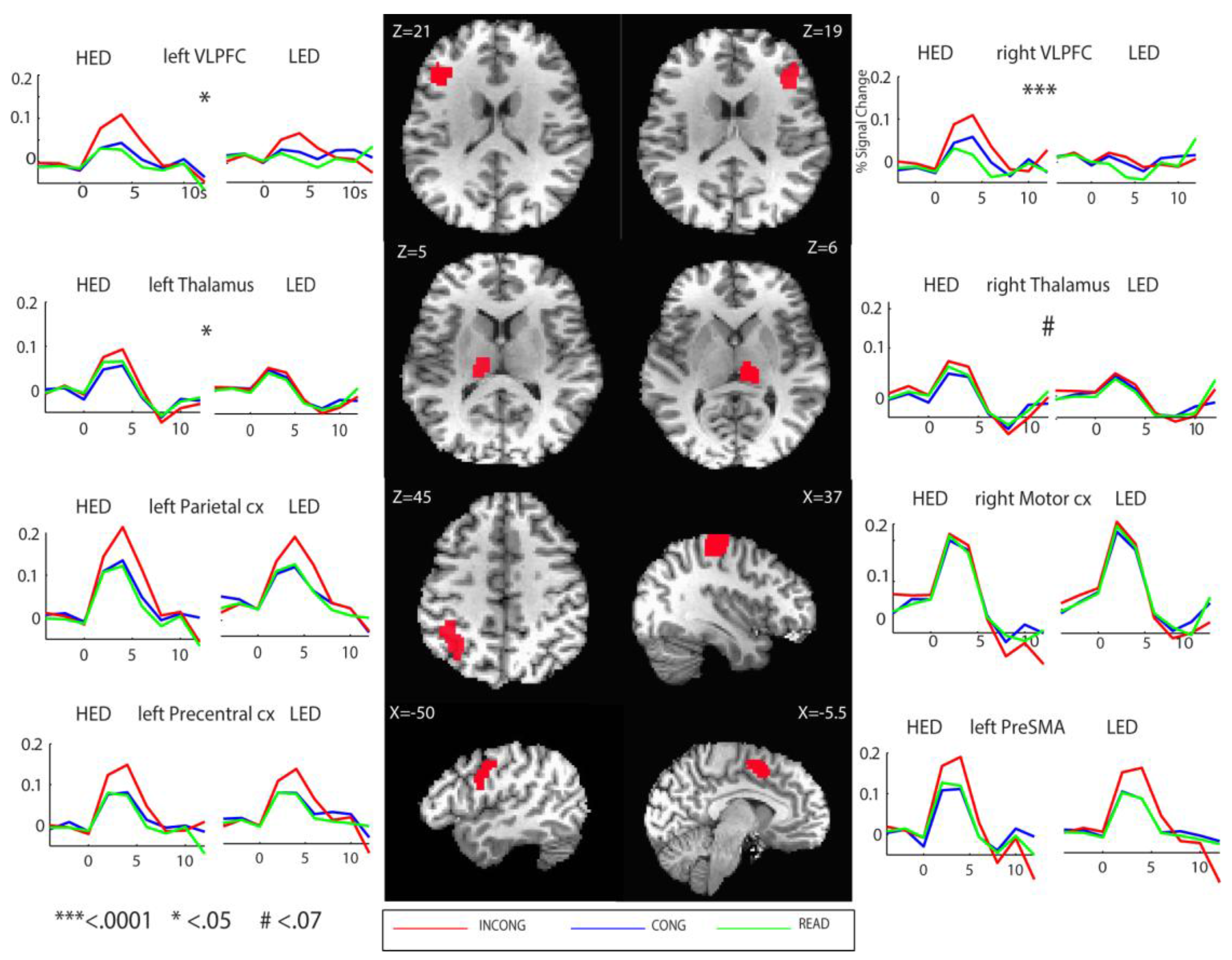
3.3. Neuroimaging Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Posner, M.; Snyder, C.R.R. Attention and cognitive control. In Information Processing and Cognition; Solso, R.L., Ed.; Erlbaum: Hillsdale, NJ, USA, 1975; pp. 55–85. [Google Scholar]
- Miller, E.K. The prefrontal cortex and cognitive control. Nat. Rev. Neurosci. 2000, 1, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Badre, D. Cognitive control, hierarchy, and the rostro-caudal organization of the frontal lobes. Trends Cogn. Sci. 2008, 12, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Niendam, T.A.; Laird, A.R.; Ray, K.L.; Dean, Y.M.; Glahn, D.C.; Carter, C.S. Meta-analytic evidence for a superordinate cognitive control network subserving diverse executive functions. Cogn. Affect. Behav. Neurosci. 2012, 12, 241–268. [Google Scholar] [CrossRef] [PubMed]
- Kennerley, S.W.; Walton, M.E. Decision making and reward in frontal cortex: Complementary evidence from neurophysiological and neuropsychological studies. Behav. Neurosci. 2011, 125, 297–317. [Google Scholar] [CrossRef] [PubMed]
- Laird, A.R.; McMillan, K.M.; Lancaster, J.L.; Kochunov, P.; Turkeltaub, P.E.; Pardo, J.V.; Fox, P.T. A comparison of label-based review and ALE meta-analysis in the Stroop task. Hum. Brain Mapp. 2005, 25, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.; Lohmann, G.; Derrfuss, J.; von Cramon, D.Y. Meta-analysis of functional imaging data using replicator dynamics. Hum. Brain Mapp. 2005, 25, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Nee, D.E.; Wager, T.D.; Jonides, J. Interference resolution: Insights from a meta-analysis of neuroimaging tasks. Cogn. Affect. Behav. Neurosci. 2007, 7, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.L.; Hall, D.A. Examining a supramodal network for conflict processing: A systematic review and novel functional magnetic resonance imaging data for related visual and auditory Stroop tasks. J. Cogn. Neurosci. 2008, 20, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Summerfield, C.; Koechlin, E. Decision making and prefrontal executive function. In The Cognitive Neurosciences; Gazzaniga, M., Ed.; MIT Press: Cambridge, MA, USA, 2009; pp. 1019–1030. [Google Scholar]
- Ridderinkhof, K.R.; Ullsperger, M.; Crone, E.A.; Nieuwenhuis, S. The role of the medial frontal cortex in cognitive control. Science 2004, 306, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Rothbart, M.K.; Sheese, B.E.; Voelker, P. Control networks and neuromodulators of early development. Dev. Psychol. 2011, 48, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Brass, M.; Derrfuss, J.; Forstmann, B.; von Cramon, D.Y. The role of the inferior frontal junction area in cognitive control. Trends Cogn. Sci. 2005, 9, 314–316. [Google Scholar] [CrossRef] [PubMed]
- Botvinick, M.M. Conflict monitoring and decision making: Reconciling two perspectives on anterior cingulate function. Cogn. Affect. Behav. Neurosci. 2007, 7, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.S.; van Veen, V. Anterior cingulate cortex and conflict detection: An update of theory and data. Cogn. Affect. Behav. Neurosci. 2007, 7, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Aron, A.R.; Robbins, T.W.; Poldrack, R.A. Inhibition and the right inferior frontal cortex: One decade on. Trends Cogn. Sci. 2014, 18, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, K.; Rickenbacher, E.; Azma, S.; Artsy, E. Acute alcohol intoxication impairs top-down regulation of Stroop incongruity as revealed by blood oxygen level-dependent functional magnetic resonance imaging. Hum. Brain Mapp. 2012, 33, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, K.; Rickenbacher, E.; Azma, S.; Artsy, E.; Lee, A.K. Effects of acute alcohol intoxication on saccadic conflict and error processing. Psychopharmacology 2013, 230, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, S.; Azma, S.; Irimia, A.; Sherfey, J.; Halgren, E.; Marinkovic, K. Theta oscillations are sensitive to both early and late conflict processing stages: Effects of alcohol intoxication. PLoS ONE 2012, 7, e43957. [Google Scholar] [CrossRef] [PubMed]
- Moselhy, H.F.; Georgiou, G.; Kahn, A. Frontal lobe changes in alcoholism: A review of the literature. Alcohol Alcohol. 2001, 36, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Oscar-Berman, M.; Marinković, K. Alcohol: Effects on neurobehavioral functions and the brain. Neuropsychol. Rev. 2007, 17, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Le Berre, A.P.; Fama, R.; Sullivan, E.V. Executive functions, memory, and social cognitive deficits and recovery in chronic alcoholism: A critical review to inform future research. Alcohol. Clin. Exp. Res. 2017, 41, 1432–1443. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.V.; Pfefferbaum, A. Neurocircuitry in alcoholism: A substrate of disruption and repair. Psychopharmacology 2005, 180, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.V.; Harris, R.A.; Pfefferbaum, A. Alcohol’s effects on brain and behavior. Alcohol Res. Health 2010, 33, 127–143. [Google Scholar] [PubMed]
- Zahr, N.M.; Pfefferbaum, A.; Sullivan, E.V. Perspectives on fronto-fugal circuitry from human imaging of alcohol use disorders. Neuropharmacology 2017, 122, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Harris, G.J.; Jaffin, S.K.; Hodge, S.M.; Kennedy, D.; Caviness, V.S.; Marinkovic, K.; Papadimitriou, G.M.; Makris, N.; Oscar-Berman, M. Frontal white matter and cingulum diffusion tensor imaging deficits in alcoholism. Alcohol. Clin. Exp. Res. 2008, 32, 1001–1013. [Google Scholar] [CrossRef] [PubMed]
- Fortier, C.B.; Leritz, E.C.; Salat, D.H.; Venne, J.R.; Maksimovskiy, A.L.; Williams, V.; Milberg, W.P.; McGlinchey, R.E. Reduced cortical thickness in abstinent alcoholics and association with alcoholic behavior. Alcohol. Clin. Exp. Res. 2011, 35, 2193–2201. [Google Scholar] [CrossRef] [PubMed]
- Chanraud, S.; Martelli, C.; Delain, F.; Kostogianni, N.; Douaud, G.; Aubin, H.J.; Reynaud, M.; Martinot, J.L. Brain morphometry and cognitive performance in detoxified alcohol-dependents with preserved psychosocial functioning. Neuropsychopharmacology 2007, 32, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, S.M.; Oscar-Berman, M.; Sawyer, K.S.; Valmas, M.M.; Urban, T.; Harris, G.J. Drinking history associations with regional white matter volumes in alcoholic men and women. Alcohol. Clin. Exp. Res. 2013, 37, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, T.C.; Mon, A.; Gazdzinski, S.; Meyerhoff, D.J. Regional brain volume changes in alcohol-dependent individuals during early abstinence: Associations with relapse following treatment. Addict. Biol. 2017, 22, 1416–1425. [Google Scholar] [CrossRef] [PubMed]
- Li, C.S.; Luo, X.; Yan, P.; Bergquist, K.; Sinha, R. Altered impulse control in alcohol dependence: Neural measures of stop signal performance. Alcohol. Clin. Exp. Res. 2009, 33, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Claus, E.D.; Feldstein Ewing, S.W.; Filbey, F.M.; Hutchison, K.E. Behavioral control in alcohol use disorders: Relationships with severity. J. Stud. Alcohol Drugs 2013, 74, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Zhang, S.; Chao, H.H.; Krystal, J.H.; Li, C.S.R. Association of drinking problems and duration of alcohol use to inhibitory control in nondependent young adult social drinkers. Alcohol. Clin. Exp. Res. 2016, 40, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Czapla, M.; Baeuchl, C.; Simon, J.J.; Richter, B.; Kluge, M.; Friederich, H.-C.; Mann, K.; Herpertz, S.C.; Loeber, S. Do alcohol-dependent patients show different neural activation during response inhibition than healthy controls in an alcohol-related fmri go/no-go-task? Psychopharmacology 2017, 234, 1001–1015. [Google Scholar] [CrossRef] [PubMed]
- Karch, S.; Jager, L.; Karamatskos, E.; Graz, C.; Stammel, A.; Flatz, W.; Lutz, J.; Holtschmidt-Taschner, B.; Genius, J.; Leicht, G.; et al. Influence of trait anxiety on inhibitory control in alcohol-dependent patients: Simultaneous acquisition of ERPs and BOLD responses. J. Psychiatr. Res. 2008, 42, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Claus, E.D.; Kiehl, K.A.; Hutchison, K.E. Neural and behavioral mechanisms of impulsive choice in alcohol use disorder. Alcohol. Clin. Exp. Res. 2011, 35, 1209–1219. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.E.; Mayer, A.R.; Bogenschutz, M.P.; Ling, J.; Dekonenko, C.; Cumbo, H. Cognitive control network function in alcohol use disorder before and during treatment with lorazepam. Subst. Use Misuse 2015, 50, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, A.; Desmond, J.E.; Galloway, C.; Menon, V.; Glover, G.H.; Sullivan, E.V. Reorganization of frontal systems used by alcoholics for spatial working memory: An fMRI study. NeuroImage 2001, 14, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Desmond, J.E.; Chen, S.A.; DeRosa, E.; Pryor, M.R.; Pfefferbaum, A.; Sullivan, E.V. Increased frontocerebellar activation in alcoholics during verbal working memory: An fMRI study. NeuroImage 2003, 19, 1510–1520. [Google Scholar] [CrossRef]
- Dager, A.D.; Jamadar, S.; Stevens, M.C.; Rosen, R.; Jiantonio-Kelly, R.E.; Sisante, J.-F.; Raskin, S.A.; Tennen, H.; Austad, C.S.; Wood, R.M. FMRI response during figural memory task performance in college drinkers. Psychopharmacology 2014, 231, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Patrick, M.E.; Terry-McElrath, Y.M.; Kloska, D.D.; Schulenberg, J.E. High-intensity drinking among young adults in the United States: Prevalence, frequency, and developmental change. Alcohol. Clin. Exp. Res. 2016, 40, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Le Moal, M. Neurobiological mechanisms for opponent motivational processes in addiction. Philos. Trans. R. Soc. Lond. B 2008, 363, 3113–3123. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F. Neurobiology of addiction. Focus 2011, 9, 55–65. [Google Scholar] [CrossRef]
- Koob, G.F. Theoretical frameworks and mechanistic aspects of alcohol addiction: Alcohol addiction as a reward deficit disorder. Curr. Top. Behav. Neurosci. 2013, 13, 3–30. [Google Scholar] [PubMed]
- Roberto, M.; Varodayan, F.P. Synaptic targets: Chronic alcohol actions. Neuropharmacology 2017, 122, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Burnett, E.J.; Chandler, L.J.; Trantham-Davidson, H. Glutamatergic plasticity and alcohol dependence-induced alterations in reward, affect and cognition. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 65, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Le Moal, M. Neurobiology of Addiction; Elsevier Academic Press: San Diego, CA, USA, 2005. [Google Scholar]
- Crabbe, J.C.; Harris, R.A.; Koob, G.F. Preclinical studies of alcohol binge drinking. Ann. N. Y. Acad. Sci. 2011, 1216, 24–40. [Google Scholar] [CrossRef] [PubMed]
- Becker, H.C.; Mulholland, P.J. Neurochemical mechanisms of alcohol withdrawal. Handb. Clin. Neurol. 2014, 125, 133–156. [Google Scholar] [PubMed]
- Duka, T.; Gentry, J.; Malcolm, R.; Ripley, T.L.; Borlikova, G.; Stephens, D.N.; Veatch, L.M.; Becker, H.C.; Crews, F.T. Consequences of multiple withdrawals from alcohol. Alcohol. Clin. Exp. Res. 2004, 28, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Le Moal, M. Addiction and the brain antireward system. Annu. Rev. Psychol. 2008, 59, 29–53. [Google Scholar] [CrossRef] [PubMed]
- Enoch, M.A. Genetic and environmental influences on the development of alcoholism. Ann. N. Y. Acad. Sci. 2006, 1094, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Lannoy, S.; Heeren, A.; Moyaerts, N.; Bruneau, N.; Evrard, S.; Billieux, J.; Maurage, P. Differential impairments across attentional networks in binge drinking. Psychopharmacology 2017, 234, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Petit, G.; Maurage, P.; Kornreich, C.; Verbanck, P.; Campanella, S. Binge drinking in adolescents: A review of neurophysiological and neuroimaging research. Alcohol Alcohol. 2013, 49, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Jacobus, J.; Tapert, S.F. Neurotoxic effects of alcohol in adolescence. Annu. Rev. Clin. Psychol. 2013, 9, 703–721. [Google Scholar] [CrossRef] [PubMed]
- Silveri, M.M.; Dager, A.D.; Cohen-Gilbert, J.E.; Sneider, J.T. Neurobiological signatures associated with alcohol and drug use in the human adolescent brain. Neurosci. Biobehav. Rev. 2016, 70, 244–259. [Google Scholar] [CrossRef] [PubMed]
- Cservenka, A.; Brumback, T. The burden of binge and heavy drinking on the brain: Effects on adolescent and young adult neural structure and function. Front. Psychol. 2017, 8, 1111. [Google Scholar] [CrossRef] [PubMed]
- Gil-Hernandez, S.; Garcia-Moreno, L.M. Executive performance and dysexecutive symptoms in binge drinking adolescents. Alcohol 2016, 51, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Parada, M.; Corral, M.; Mota, N.; Crego, A.; Rodriguez Holguin, S.; Cadaveira, F. Executive functioning and alcohol binge drinking in university students. Addict. Behav. 2012, 37, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Scaife, J.C.; Duka, T. Behavioural measures of frontal lobe function in a population of young social drinkers with binge drinking pattern. Pharmacol. Biochem. Behav. 2009, 93, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Hermens, D.F.; Lagopoulos, J.; Tobias-Webb, J.; de Regt, T.; Dore, G.; Juckes, L.; Latt, N.; Hickie, I.B. Pathways to alcohol-induced brain impairment in young people: A review. Cortex 2013, 49, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Pearlson, G.D.; Meda, S.A.; Dager, A.; Potenza, M.N.; Rosen, R.; Austad, C.S.; Raskin, S.A.; Fallahi, C.R.; Tennen, H. Influence of alcohol use on neural response to go/no-go task in college drinkers. Neuropsychopharmacology 2013, 38, 2197–2208. [Google Scholar] [CrossRef] [PubMed]
- Wetherill, R.R.; Squeglia, L.M.; Yang, T.T.; Tapert, S.F. A longitudinal examination of adolescent response inhibition: Neural differences before and after the initiation of heavy drinking. Psychopharmacology 2013, 230, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Kashfi, K.; Fang, D.; Hou, J.; Al-Khalil, K.; Anderson, R.; Syapin, P.J.; O’Boyle, M.W. Spatial attention in binge-drinking and moderate-drinking college students: An fMRI investigation. Alcohol. Treat. Q. 2017, 35, 260–278. [Google Scholar] [CrossRef]
- Campanella, S.; Peigneux, P.; Petit, G.; Lallemand, F.; Saeremans, M.; Noël, X.; Metens, T.; Nouali, M.; de Tiège, X.; de Witte, P. Increased cortical activity in binge drinkers during working memory task: A preliminary assessment through a functional magnetic resonance imaging study. PLoS ONE 2013, 8, e62260. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Wiers, R.W.; Christiansen, P.; Fillmore, M.T.; Verster, J.C. Acute alcohol effects on inhibitory control and implicit cognition: Implications for loss of control over drinking. Alcohol. Clin. Exp. Res. 2010, 34, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Fillmore, M.T. Drug abuse as a problem of impaired control: Current approaches and findings. Behav. Cogn. Neurosci. Rev. 2003, 2, 179–197. [Google Scholar] [CrossRef] [PubMed]
- Finn, P. Acute effects of alcohol on cognition and impulsive-disinhibited behavior. In Review of NIAAA’s Neuroscience and Behavioral Research Portfolio; Noronha, A., Eckardt, M., Warren, K., Eds.; US Department of Health and Human Services: Bethesda, MD, USA, 2000; Volume 34, pp. 337–356. [Google Scholar]
- Lyvers, M. “Loss of control” in alcoholism and drug addiction: A neuroscientific interpretation. Exp. Clin. Psychopharmacol. 2000, 8, 225–249. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Jimenez, R.; Avila, C.; Ponce, G.; Ibanez, M.I.; Rubio, G.; Jimenez-Arriero, M.A.; Ampuero, I.; Ramos, J.A.; Hoenicka, J.; Palomo, T. The TaqIA polymorphism linked to the DRD2 gene is related to lower attention and less inhibitory control in alcoholic patients. Eur. Psychiatry 2006, 21, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T.; Wong, M.M.; Martel, M.M.; Jester, J.M.; Puttler, L.I.; Glass, J.M.; Adams, K.M.; Fitzgerald, H.E.; Zucker, R.A. Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Fowler, J.S.; Wang, G.J.; Swanson, J.M.; Telang, F. Dopamine in drug abuse and addiction: Results of imaging studies and treatment implications. Arch. Neurol. 2007, 64, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Crego, A.; Holguin, S.R.; Parada, M.; Mota, N.; Corral, M.; Cadaveira, F. Binge drinking affects attentional and visual working memory processing in young university students. Alcohol. Clin. Exp. Res. 2009, 33, 1870–1879. [Google Scholar] [CrossRef] [PubMed]
- Maurage, P.; Pesenti, M.; Philippot, P.; Joassin, F.; Campanella, S. Latent deleterious effects of binge drinking over a short period of time revealed only by electrophysiological measures. J. Psychiatry Neurosci. 2009, 34, 111–118. [Google Scholar] [CrossRef]
- MacLeod, C.M.; MacDonald, P.A. Interdimensional interference in the Stroop effect: Uncovering the cognitive and neural anatomy of attention. Trends Cogn. Sci. 2000, 4, 383–391. [Google Scholar] [CrossRef]
- Roelofs, A.; van Turennout, M.; Coles, M.G. Anterior cingulate cortex activity can be independent of response conflict in Stroop-like tasks. Proc. Natl. Acad. Sci. USA 2006, 103, 13884–13889. [Google Scholar] [CrossRef] [PubMed]
- Lange, J.E.; Voas, R.B. Defining binge drinking quantities through resulting blood alcohol concentrations. Psychol. Addict. Behav. 2001, 15, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Read, J.P.; Beattie, M.; Chamberlain, R.; Merrill, J.E. Beyond the “binge” threshold: Heavy drinking patterns and their association with alcohol involvement indices in college students. Addict. Behav. 2008, 33, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Coutlee, C.G.; Politzer, C.S.; Hoyle, R.H.; Huettel, S.A. An abbreviated impulsiveness scale constructed through confirmatory factor analysis of the Barratt Impulsiveness Scale version 11. Arch. Sci. Psychol. 2014, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hoyle, R.H.; Stephenson, M.T.; Palmgreen, P.; Lorch, E.P.; Donohew, R.L. Reliability and validity of a brief measure of sensation seeking. Personal. Individ. Differ. 2002, 32, 401–414. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Selzer, M.L.; Vinokur, A.; van Rooijen, L. A self-administered Short Michigan Alcoholism Screening Test (SMAST). J. Stud. Alcohol 1975, 36, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Sobell, L.C.; Sobell, M.B. Timeline follow-back. In Measuring Alcohol Consumption; Springer: New York, NY, USA, 1992; pp. 41–72. [Google Scholar]
- Flannery, B.; Volpicelli, J.; Pettinati, H. Psychometric properties of the Penn Alcohol Craving scale. Alcohol. Clin. Exp. Res. 1999, 23, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Kuntsche, E.; Kuntsche, S. Development and validation of the Drinking Motive Questionnaire Revised Short Form (DMQ-R SF). J. Clin. Child Adolesc. Psychol. 2009, 38, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Kahler, C.W.; Strong, D.R.; Read, J.P. Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: The brief young adult alcohol consequences questionnaire. Alcohol. Clin. Exp. Res. 2005, 29, 1180–1189. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, H.J.; Eysenck, S.B.G. Manual of the Eysenck Personality Questionnaire; Hodder & Staughton: London, UK, 1975. [Google Scholar]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Adler, L.; Ames, M.; Demler, O.; Faraone, S.; Hiripi, E.; Howes, M.J.; Jin, R.; Secnik, K.; Spencer, T. The world health organization adult ADHD self-report scale (ASRS): A short screening scale for use in the general population. Psychol. Med. 2005, 35, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence (WASI-II); The Psychological Corporation: San Antonio, TX, USA, 1999. [Google Scholar]
- Rice, J.P.; Reich, T.; Bucholz, K.K.; Neuman, R.J.; Fishman, R.; Rochberg, N.; Hesselbrock, V.M.; Nurnberger, J.I.; Schuckit, M.A.; Begleiter, H. Comparison of direct interview and family history diagnoses of alcohol dependence. Alcohol. Clin. Exp. Res. 1995, 19, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0. Armonk. Available online: http://www-01.ibm.com/support/docview.wss?uid=swg27047057 (accessed on 20 December 2017).
- Repovs, G. The mode of response and the stroop effect: A reaction time analysis. Horiz. Psychol. 2004, 13, 105–114. [Google Scholar]
- Burock, M.A.; Buckner, R.L.; Woldorff, M.G.; Rosen, B.R.; Dale, A.M. Randomized event-related experimental designs allow for extremely rapid presentation rates using functional MRI. Neuroreport 1998, 9, 3735–3739. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.W. AFNI: What a long strange trip it’s been. NeuroImage 2012, 62, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comput. Biomed. Res. 1996, 29, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Saad, Z.S.; Nath, A.R.; Beauchamp, M.S.; Cox, R.W. FMRI group analysis combining effect estimates and their variances. Neuroimage 2012, 60, 747–765. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.J.; Rotshtein, P.; Geng, J.J.; Sterzer, P.; Henson, R.N. A critique of functional localisers. NeuroImage 2006, 30, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Poldrack, R.A. Region of interest analysis for fMRI. Soc. Cogn. Affect. Neurosci. 2007, 2, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, L.C.; Schweinsburg, A.D.; Nagel, B.J.; Barlett, V.C.; Brown, S.A.; Tapert, S.F. Gender and adolescent alcohol use disorders on BOLD (Blood Oxygen Level Dependent) response to spatial working memory. Alcohol Alcohol. 2005, 40, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Squeglia, L.M.; Schweinsburg, A.D.; Pulido, C.; Tapert, S.F. Adolescent binge drinking linked to abnormal spatial working memory brain activation: Differential gender effects. Alcohol. Clin. Exp. Res. 2011, 35, 1831–1841. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, K.; Rickenbacher, E.; Azma, S. Effects of alcohol intoxication on response conflict in a flanker task. J. Addict. Res. Ther. 2012. [Google Scholar] [CrossRef] [PubMed]
- Tapert, S.F.; Pulido, C.; Paulus, M.P.; Schuckit, M.A.; Burke, C. Level of response to alcohol and brain response during visual working memory. J. Stud. Alcohol. 2004, 65, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.E.; Dekonenko, C.J.; Mayer, A.R.; Bogenschutz, M.P.; Turner, J.A. Cognitive control in alcohol use disorder: Deficits and clinical relevance. Rev. Neurosci. 2014, 25, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Chanraud, S.; Sullivan, E. Compensatory recruitment of neural resources in chronic alcoholism. Handb. Clin. Neurol. 2014, 125, 369–380. [Google Scholar] [PubMed]
- Oscar-Berman, M.; Valmas, M.M.; Sawyer, K.S.; Ruiz, S.M.; Luhar, R.B.; Gravitz, Z.R. Profiles of impaired, spared, and recovered neuropsychological processes in alcoholism. Handb. Clin. Neurol. 2014, 125, 183–210. [Google Scholar] [PubMed]
- Marinkovic, K.; Oscar-Berman, M.; Urban, T.; O’Reilly, C.E.; Howard, J.A.; Sawyer, K.; Harris, G.J. Alcoholism and dampened temporal limbic activation to emotional faces. Alcohol. Clin. Exp. Res. 2009, 33, 1880–1892. [Google Scholar] [CrossRef] [PubMed]
- Chikazoe, J.; Konishi, S.; Asari, T.; Jimura, K.; Miyashita, Y. Activation of right inferior frontal gyrus during response inhibition across response modalities. J. Cogn. Neurosci. 2007, 19, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Erika-Florence, M.; Leech, R.; Hampshire, A. A functional network perspective on response inhibition and attentional control. Nat. Commun. 2014, 5, 4073. [Google Scholar] [CrossRef] [PubMed]
- Chatham, C.H.; Claus, E.D.; Kim, A.; Curran, T.; Banich, M.T.; Munakata, Y. Cognitive control reflects context monitoring, not motoric stopping, in response inhibition. PLoS ONE 2012, 7, e31546. [Google Scholar] [CrossRef] [PubMed]
- Hampshire, A. Putting the brakes on inhibitory models of frontal lobe function. NeuroImage 2015, 113, 340–355. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.J.; Wagner, A.D. Cognitive control and right ventrolateral prefrontal cortex: Reflexive reorienting, motor inhibition, and action updating. Ann. N. Y. Acad. Sci. 2011, 1224, 40–62. [Google Scholar] [CrossRef] [PubMed]
- Braun, U.; Schäfer, A.; Walter, H.; Erk, S.; Romanczuk-Seiferth, N.; Haddad, L.; Schweiger, J.I.; Grimm, O.; Heinz, A.; Tost, H. Dynamic reconfiguration of frontal brain networks during executive cognition in humans. Proc. Natl. Acad. Sci. USA 2015, 112, 11678–11683. [Google Scholar] [CrossRef] [PubMed]
- Goulas, A.; Uylings, H.B.; Stiers, P. Unravelling the intrinsic functional organization of the human lateral frontal cortex: A parcellation scheme based on resting state fMRI. J. Neurosci. 2012, 32, 10238–10252. [Google Scholar] [CrossRef] [PubMed]
- Bullmore, E.; Sporns, O. The economy of brain network organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Breakspear, M.; Stam, C.J. Dynamics of a neural system with a multiscale architecture. Philos. Trans. R. Soc. Lond. B 2005, 360, 1051–1074. [Google Scholar] [CrossRef] [PubMed]
- Fornito, A.; Zalesky, A.; Breakspear, M. The connectomics of brain disorders. Nat. Rev. Neurosci. 2015, 16, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Müller-Oehring, E.M.; Jung, Y.-C.; Pfefferbaum, A.; Sullivan, E.V.; Schulte, T. The resting brain of alcoholics. Cereb. Cortex 2014, 25, 4155–4168. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.Q.; Padovan, N.; Marinkovic, K. Alcohol hits you when it is hard: Intoxication, task difficulty, and theta brain oscillations. Alcohol. Clin. Exp. Res. 2016, 40, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.K.; Cohen, J.D. An integrative theory of prefrontal cortex function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef] [PubMed]
- Oscar-Berman, M.; Marinkovic, K. Alcoholism and the brain: An overview. Alcohol Res. Health 2004, 27, 125–133. [Google Scholar]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12, 652–669. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Volkow, N.D. Neurocircuitry of addiction. Neuropsychopharmacology 2010, 35, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Kwako, L.E.; Momenan, R.; Litten, R.Z.; Koob, G.F.; Goldman, D. Addictions neuroclinical assessment: A neuroscience-based framework for addictive disorders. Biol. Psychiatry 2016, 80, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Weafer, J.; Fillmore, M.T. Acute alcohol effects on attentional bias in heavy and moderate drinkers. Psychol. Addict. Behav. 2013, 27, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Paz, A.L.; Keim, C.A.; Rosselli, M. Inhibitory performance predicting drinking behaviours among young adults. Alcohol Alcohol. 2016, 51, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Grüsser, S.M.; Wrase, J.; Klein, S.; Hermann, D.; Smolka, M.N.; Ruf, M.; Weber-Fahr, W.; Flor, H.; Mann, K.; Braus, D.F. Cue-induced activation of the striatum and medial prefrontal cortex is associated with subsequent relapse in abstinent alcoholics. Psychopharmacology 2004, 175, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Tapert, S.F.; Brown, G.G.; Kindermann, S.S.; Cheung, E.H.; Frank, L.R.; Brown, S.A. FMRI measurement of brain dysfunction in alcohol-dependent young women. Alcohol. Clin. Exp. Res. 2001, 25, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M. Thalamus plays a central role in ongoing cortical functioning. Nat. Neurosci. 2016, 19, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.K.; Dunlop, K.; Downar, J. Cortico-striatal-thalamic loop circuits of the salience network: A central pathway in psychiatric disease and treatment. Front. Syst. Neurosci. 2016, 10, 104. [Google Scholar] [CrossRef] [PubMed]
- Minamimoto, T.; Hori, Y.; Yamanaka, K.; Kimura, M. Neural signal for counteracting pre-action bias in the centromedian thalamic nucleus. Front. Syst. Neurosci. 2014, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Saalmann, Y.B. Intralaminar and medial thalamic influence on cortical synchrony, information transmission and cognition. Front. Syst. Neurosci. 2014, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Ridderinkhof, K.R.; van den Wildenberg, W.P.; Segalowitz, S.J.; Carter, C.S. Neurocognitive mechanisms of cognitive control: The role of prefrontal cortex in action selection, response inhibition, performance monitoring, and reward-based learning. Brain Cogn. 2004, 56, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Verguts, T.; Notebaert, W. Adaptation by binding: A learning account of cognitive control. Trends Cogn. Sci. 2009, 13, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Critchley, H.D. Psychophysiology of neural, cognitive and affective integration: FMRI and autonomic indicants. Int. J. Psychophysiol. 2009, 73, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Schiff, N.D. Central thalamic contributions to arousal regulation and neurological disorders of consciousness. Ann. N. Y. Acad. Sci. 2008, 1129, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Kirouac, G.J. Placing the paraventricular nucleus of the thalamus within the brain circuits that control behavior. Neurosci. Biobehav. Rev. 2015, 56, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Pitel, A.L.; Segobin, S.H.; Ritz, L.; Eustache, F.; Beaunieux, H. Thalamic abnormalities are a cardinal feature of alcohol-related brain dysfunction. Neurosci. Biobehav. Rev. 2015, 54, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Segobin, S.H.; Chetelat, G.; Le Berre, A.P.; Lannuzel, C.; Boudehent, C.; Vabret, F.; Eustache, F.; Beaunieux, H.; Pitel, A.L. Relationship between brain volumetric changes and interim drinking at six months in alcohol-dependent patients. Alcohol. Clin. Exp. Res. 2014, 38, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Moeller, F.G.; Dougherty, D.M. Antisocial personality disorder, alcohol, and aggression. Alcohol Res. Health 2001, 25, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.R.; Potenza, M.N. Addictions and personality traits: Impulsivity and related constructs. Curr. Behav. Neurosci. Rep. 2014, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sher, K.J.; Trull, T.J. Personality and disinhibitory psychopathology: Alcoholism and antisocial personality disorder. J. Abnorm. Psychol. 1994, 103, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Dick, D.M.; Smith, G.; Olausson, P.; Mitchell, S.H.; Leeman, R.F.; O’Malley, S.S.; Sher, K. Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addict. Biol. 2010, 15, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Leeman, R.F.; Patock-Peckham, J.A.; Potenza, M.N. Impaired control over alcohol use: An under-addressed risk factor for problem drinking in young adults? Exp. Clin. Psychopharmacol. 2012, 20, 92–106. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.J.; Belin, D.; Economidou, D.; Pelloux, Y.; Dalley, J.W.; Robbins, T.W. Neural mechanisms underlying the vulnerability to develop compulsive drug-seeking habits and addiction. Philos. Trans. R. Soc. Lond. B 2008, 363, 3125–3135. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, J.D.; Pennington, Z.T. Reward, interrupted: Inhibitory control and its relevance to addictions. Neuropharmacology 2014, 76, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Begleiter, H.; Porjesz, B. What is inherited in the predisposition toward alcoholism? A proposed model. Alcohol. Clin. Exp. Res. 1999, 23, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Schuckit, M.A.; Smith, T.L.; Kalmijn, J. The search for genes contributing to the low level of response to alcohol: Patterns of findings across studies. Alcohol. Clin. Exp. Res. 2004, 28, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Buckholtz, J.W.; Treadway, M.T.; Cowan, R.L.; Woodward, N.D.; Li, R.; Ansari, M.S.; Baldwin, R.M.; Schwartzman, A.N.; Shelby, E.S.; Smith, C.E.; et al. Dopaminergic network differences in human impulsivity. Science 2010, 329, 532. [Google Scholar] [CrossRef] [PubMed]
- Basar, K.; Sesia, T.; Groenewegen, H.; Steinbusch, H.W.; Visser-vandewalle, V.; Temel, Y. Nucleus accumbens and impulsivity. Prog. Neurobiol. 2010, 92, 533–557. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, L.; Doly, S.; Kaprio, J.; Yuan, Q.; Tikkanen, R.; Paunio, T.; Zhou, Z.; Wedenoja, J.; Maroteaux, L.; Diaz, S.; et al. A population-specific HTR2B stop codon predisposes to severe impulsivity. Nature 2010, 468, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Goldman, D.; Oroszi, G.; Ducci, F. The genetics of addictions: Uncovering the genes. Nat. Rev. Genet. 2005, 6, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Wetherill, R.R.; Castro, N.; Squeglia, L.M.; Tapert, S.F. Atypical neural activity during inhibitory processing in substance-naive youth who later experience alcohol-induced blackouts. Drug Alcohol Depend. 2013, 128, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Müller-Oehring, E.M.; Sullivan, E.V.; Pfefferbaum, A. Synchrony of corticostriatal-midbrain activation enables normal inhibitory control and conflict processing in recovering alcoholic men. Biol. Psychiatry 2012, 71, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Sher, K.J.; Grekin, E.R.; Williams, N.A. The development of alcohol use disorders. Annu. Rev. Clin. Psychol. 2005, 1, 493–523. [Google Scholar] [CrossRef] [PubMed]
- Goldman, D. Gene × environment interactions in complex behavior: First, build a telescope. Biol. Psychiatry 2010, 67, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Dick, D.M.; Riley, B.; Kendler, K.S. Nature and nurture in neuropsychiatric genetics: Where do we stand? Dialogues Clin. Neurosci. 2010, 12, 7–23. [Google Scholar] [PubMed]
- Van der Zwaluw, C.S.; Engels, R.C. Gene-environment interactions and alcohol use and dependence: Current status and future challenges. Addiction 2009, 104, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Spanagel, R. Alcoholism: A systems approach from molecular physiology to addictive behavior. Physiol. Rev. 2009, 89, 649–705. [Google Scholar] [CrossRef] [PubMed]
- Crews, F.T.; Vetreno, R.P.; Broadwater, M.A.; Robinson, D.L. Adolescent alcohol exposure persistently impacts adult neurobiology and behavior. Pharmacol. Rev. 2016, 68, 1074–1109. [Google Scholar] [CrossRef] [PubMed]
- Watson, T.D.; Sweeney, J.F.; Louis, H. Neurocognitive, psychological and behavioral correlates of binge drinking and use of alcohol with caffeinated beverages in college-aged adults. Am. J. Drug Alcohol Abuse 2014, 40, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Petit, G.; Kornreich, C.; Maurage, P.; Noel, X.; Letesson, C.; Verbanck, P.; Campanella, S. Early attentional modulation by alcohol-related cues in young binge drinkers: An event-related potentials study. Clin. Neurophysiol. 2012, 123, 925–936. [Google Scholar] [CrossRef] [PubMed]
- Kimbrough, A.; Kim, S.; Cole, M.; Brennan, M.; George, O. Intermittent access to ethanol drinking facilitates the transition to excessive drinking after chronic intermittent ethanol vapor exposure. Alcohol. Clin. Exp. Res. 2017, 41, 1502–1509. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HED (n = 14) | LED (n = 17) | Stat. Value (U/chi a) | p | |
|---|---|---|---|---|
| % Female | 64.3% | 52.9% | 0.406 a | ns a |
| Age | 23.8 ± 3.4 | 25.5 ± 4.1 | 90.5 | ns |
| Family History Positive | 50% | 58.8% | 0.241 a | ns a |
| Education Years | 15.1 ± 1.9 | 15.9 ± 2.3 | 81 | ns |
| Undergraduate Grade Point Avg. | 3.40 ± 0.38 | 3.59 ± 0.33 | 79 | ns |
| Stroop Task Difficulty Ratings | 3.07 ± 0.62 | 2.00 ± 0.78 | 32 | 0.001 |
| In the past 6 months | ||||
| No. of drinking days/wk | 2.67 ± 1.2 | 1.35 ± 0.96 | 46 | 0.003 |
| No. of drinks/occasion | 5.25 ± 2.6 | 2.2 ± 1.2 | 34 | 0.001 |
| No. of binge episodes | 15.21 ± 15.2 | 0.41 ± 0.7 | 0.000 | <0.001 |
| No. of alcohol-induced blackouts | 3.14 ± 2.9 | 0.18 ± 0.5 | 33 | <0.001 |
| Max No. of drinks in 24 h | 12.57 ± 9.8 | 3.41 ± 2.06 | 11 | <0.001 |
| Age Onset of Alcohol Use | 15.72 ± 1.49 | 18.13 ± 2.13 | 31.5 | 0.007 |
| Severity of Alcoholism (SMAST) | 2.86 ± 2.4 | 0.76 ± 1.0 | 47 | 0.003 |
| Alc. Use Disorder Ident. Test (AUDIT) | 13.43 ± 5.80 | 3.82 ± 1.55 | 4.5 | <0.001 |
| Motivation | ||||
| Enhancement | 2.33 ± 0.333 | 1.69 ± 0.46 | 26.5 | <0.001 |
| Social | 2.62 ± 0.405 | 2.04 ± 0.44 | 40.5 | 0.002 |
| Conformity | 1.41 ± 0.564 | 1.43 ± 0.45 | 104 | ns |
| Coping | 1.67 ± 0.472 | 1.19 ± 0.29 | 37.5 | 0.002 |
| Drinking Consequences (B-YAACQ) | 8.86 ± 6.11 | 2.76 ± 3.09 | 47 | 0.004 |
| Alcohol Craving (PACS) | 7.71 ± 4.53 | 2.53 ± 2.27 | 36 | 0.001 |
| Anxiety (GAD-7) | 2.07 ± 1.68 | 3.06 ± 2.63 | 100 | ns |
| Depression (PHQ-9) | 3.07 ± 2.70 | 3.18 ± 2.96 | 118 | ns |
| ADHD Symptomology (ASRS) | 1.64 ± 1.59 | 1.06 ± 1.34 | 94.5 | ns |
| Impulsivity | ||||
| Attention | 2.06 ± 0.478 | 1.83 ± 0.39 | 75 | ns |
| Motor | 2.23 ± 0.632 | 1.78 ± 0.42 | 61 | 0.036 |
| Non-Planning | 2.09 ± 0.739 | 1.78 ± 0.48 | 84.5 | ns |
| Sensation Seeking | ||||
| Experience | 4.23 ± 0.806 | 3.97 ± 0.86 | 90 | ns |
| Boredom | 4.11 ± 0.650 | 3.59 ± 0.76 | 65.5 | 0.05 |
| Thrill | 3.69 ± 1.15 | 3.41 ± 1.28 | 97.5 | ns |
| Disinhibition | 3.81 ± 0.722 | 2.94 ± 1.03 | 54.5 | 0.018 |
| WASI-II Percentile | 69.36 ± 21.11 | 72.81 ± 21.40 | 99.5 | ns |
| Eysenck Personality | ||||
| Neuroticism | 3.08 ± 2.29 | 3.71 ± 3.75 | 110 | ns |
| Psychoticism | 2.38 ± 2.26 | 2.18 ± 1.38 | 110 | ns |
| Extraversion | 9.46 ± 2.63 | 7.71 ± 3.57 | 80.5 | ns |
| Area | Tal. Coord (LPI) | m.e.Group (F2,58) | m.e.Cond (F2,58) | Cond x Group | HED: INC > C + R (F1,13) | LED: INC > C + R (F1,16) |
|---|---|---|---|---|---|---|
| L. VLPFC | −40.1, 25.8, 21.3 | 5.3 < 0.05 | 56.3 < 0.0001 | ns | 17.6 < 0.001 | 116.2 < 0.001 |
| L. Thalamus | −11.6, 20.6, 5.2 | 5.9 < 0.05 | 14.6 < 0.001 | ns | 11.2 < 0.006 | ns |
| L. PreSMA | −5.5, 4.7, 49.2 | ns | 63.9 < 0.0001 | ns | 29.4 < 0.001 | 35.6 < 0.0001 |
| L. PreCent. cx | −50.6, 0.6, 31 | ns | 48.3 < 0.0001 | ns | 17.2 < 0.001 | 36.6 < 0.0001 |
| L. Parietal cx | −37.5, −49.3, 45.5 | ns | 43.1 < 0.0001 | ns | 23.9 < 0.001 | 18.8 < 0.001 |
| L. Insula | −28.7, 16.6, 9.9 | ns | 30.2 < 0.0001 | ns | 9.2 < 0.01 | 26.3 < 0.0001 |
| R. VLPFC | 42.1, 28.7, 19.4 | 17.7 < 0.0003 | 32.4 < 0.0001 | 4.4 < 0.05 | 17.7 < 0.001 | 12.1 < 0.01 |
| R. Thalamus | 12.6, −22.2, 6.1 | 3.6 < 0.07 | 5.9 < 0.05 | ns | ns | ns |
| R. Insula | 40.0, 5.4, 11.2 | ns | 6.9 < 0.05 | ns | ns | 5.86 < 0.05 |
| R. PreCent. cx | 37.3, −26.4, 54.5 | ns | ns | ns | ns | ns |
| R. Motor cx | 37.1, −21, 56.1 | ns | ns | ns | ns | ns |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molnar, S.M.; Beaton, L.E.; Happer, J.P.; Holcomb, L.A.; Huang, S.; Arienzo, D.; Marinkovic, K. Behavioral and Brain Activity Indices of Cognitive Control Deficits in Binge Drinkers. Brain Sci. 2018, 8, 9. https://doi.org/10.3390/brainsci8010009
Molnar SM, Beaton LE, Happer JP, Holcomb LA, Huang S, Arienzo D, Marinkovic K. Behavioral and Brain Activity Indices of Cognitive Control Deficits in Binge Drinkers. Brain Sciences. 2018; 8(1):9. https://doi.org/10.3390/brainsci8010009
Chicago/Turabian StyleMolnar, Sean M., Lauren E. Beaton, Joseph P. Happer, Lee A. Holcomb, Siyuan Huang, Donatello Arienzo, and Ksenija Marinkovic. 2018. "Behavioral and Brain Activity Indices of Cognitive Control Deficits in Binge Drinkers" Brain Sciences 8, no. 1: 9. https://doi.org/10.3390/brainsci8010009
APA StyleMolnar, S. M., Beaton, L. E., Happer, J. P., Holcomb, L. A., Huang, S., Arienzo, D., & Marinkovic, K. (2018). Behavioral and Brain Activity Indices of Cognitive Control Deficits in Binge Drinkers. Brain Sciences, 8(1), 9. https://doi.org/10.3390/brainsci8010009