Transcranial Direct Current Stimulation for Obsessive-Compulsive Disorder: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
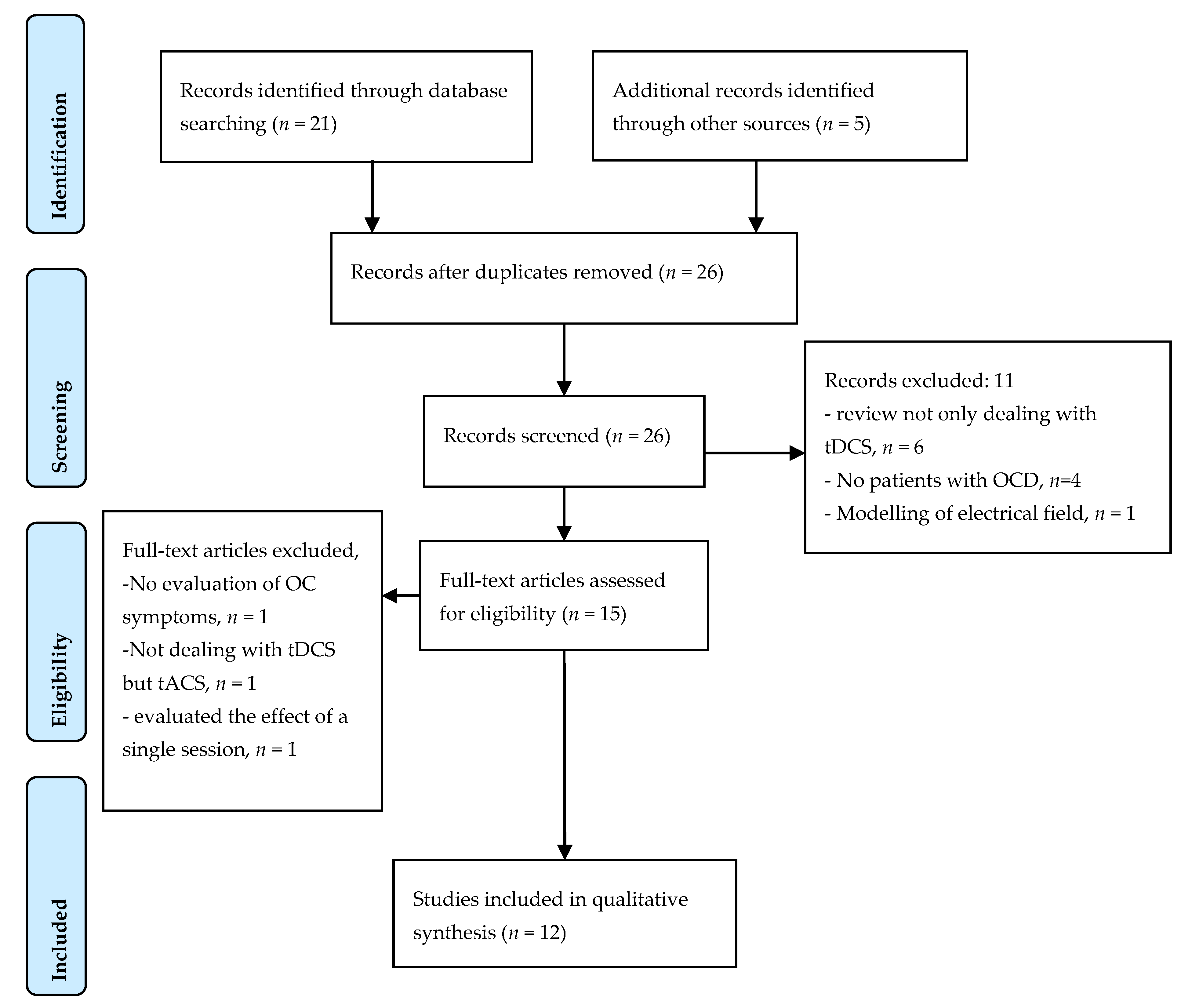
2. Materials and Methods
Search Strategy
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ruscio, A.M.; Stein, D.J.; Chiu, W.T.; Kessler, R.C. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol. Psychiatry 2010, 15, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Fontenelle, I.S.; Fontenelle, L.F.; Borges, M.C.; Prazeres, A.M.; Rangé, B.P.; Mendlowicz, M.V.; Versiani, M. Quality of life and symptom dimensions of patients with obsessive-compulsive disorder. Psychiatry Res. 2010, 179, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, N.A.; Reghunandanan, S.; Simpson, H.B.; Phillips, K.A.; Richter, M.A.; Matthews, K.; Stein, D.J.; Sareen, J.; Brown, A.; Sookman, D. Accreditation Task Force of The Canadian Institute for Obsessive Compulsive Disorders Obsessive-compulsive disorder (OCD): Practical strategies for pharmacological and somatic treatment in adults. Psychiatry Res. 2015, 227, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Pallanti, S.; Quercioli, L. Treatment-refractory obsessive-compulsive disorder: Methodological issues, operational definitions and therapeutic lines. Prog. Neuropsychopharmacol. Biol. Psychiatry 2006, 30, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Mondino, M.; Bennabi, D.; Poulet, E.; Galvao, F.; Brunelin, J.; Haffen, E. Can transcranial direct current stimulation (tDCS) alleviate symptoms and improve cognition in psychiatric disorders? World J. Biol. Psychiatry 2014, 15, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; de Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Keeser, D.; Meindl, T.; Bor, J.; Palm, U.; Pogarell, O.; Mulert, C.; Brunelin, J.; Moller, H.-J.; Reiser, M.; Padberg, F. Prefrontal Transcranial Direct Current Stimulation Changes Connectivity of Resting-State Networks during fMRI. J. Neurosci. 2011, 31, 15284–15293. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Wu, W.; Lin, Y.; Wang, J.; Zhou, D.; Guo, J.; Gu, S.; He, M.; Ahmed, S.; Hu, J.; et al. Localization of cerebral functional deficits in patients with obsessive-compulsive disorder: A resting-state fMRI study. J. Affect. Disord. 2012, 138, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Van der Straten, A.L.; Denys, D.; van Wingen, G. Impact of treatment on resting cerebral blood flow and metabolism in obsessive compulsive disorder: A meta-analysis. Sci. Rep. 2017, 7, 17464. [Google Scholar] [CrossRef] [PubMed]
- Nauczyciel, C.; le Jeune, F.; Naudet, F.; Douabin, S.; Esquevin, A.; Vérin, M.; Dondaine, T.; Robert, G.; Drapier, D.; Millet, B. Repetitive transcranial magnetic stimulation over the orbitofrontal cortex for obsessive-compulsive disorder: A double-blind, crossover study. Transl. Psychiatry 2014, 4, e436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauch, S.L.; Jenike, M.A.; Alpert, N.M.; Baer, L.; Breiter, H.C.; Fischman, A.J. Regional cerebral blood flow measured during symptom provocation in obsessive-compulsive disorder using oxygen 15-labeled carbon dioxide and positron emission tomography. Arch. Gen. Psychiatry 1994, 51, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Milad, M.R.; Rauch, S.L. Obsessive-compulsive disorder: Beyond segregated cortico-striatal pathways. Trends Cogn. Sci. 2012, 16, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Yekta, M.; Rostami, R.; Fayyaz, E. Transcranial Direct Current Stimulation of Dorsolateral Prefrontal Cortex in Patients with Obsessive Compulsive Disorder to Improve Decision Making and Reduce Obsession Symptoms. Pract. Clin. Psychol. 2015, 3, 185–194. [Google Scholar]
- Klimke, A.; Nitsche, M.A.; Maurer, K.; Voss, U. Case Report: Successful Treatment of Therapy-Resistant OCD with Application of Transcranial Alternating Current Stimulation (tACS). Brain Stimul. 2016, 9, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Todder, D.; Gershi, A.; Perry, Z.; Kaplan, Z.; Levine, J.; Avirame, K. Immediate Effects of Transcranial Direct Current Stimulation on Obsession-Induced Anxiety in Refractory Obsessive-Compulsive Disorder: A Pilot Study. J. ECT 2017. [Google Scholar] [CrossRef] [PubMed]
- Hazari, N.; Narayanaswamy, J.C.; Chhabra, H.; Bose, A.; Venkatasubramanian, G.; Reddy, Y.C.J. Response to Transcranial Direct Current Stimulation in a Case of Episodic Obsessive Compulsive Disorder. J. ECT 2016, 32, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Dinn, W.M.; Aycicegi-Dinn, A.; Göral, F.; Karamursel, S.; Yildirim, E.A.; Hacioglu-Yildirim, M.; Gansler, D.A.; Doruk, D.; Fregni, F. Treatment-resistant obsessive-compulsive disorder: Insights from an open trial of transcranial direct current stimulation (tDCS) to design a RCT. Neurol. Psychiatry Brain Res. 2016, 22, 146–154. [Google Scholar] [CrossRef]
- Alizadeh Goradel, J.; Pouresmali, A.; Mowlaie, M.; Sadeghi Movahed, F. The Effects of Transcranial Direct Current Stimulation on Obsession-compulsion, Anxiety, and Depression of a Patient Suffering from Obsessive-compulsive Disorder. Pract. Clin. Psychol. 2016, 4, 75–80. [Google Scholar] [CrossRef]
- Volpato, C.; Piccione, F.; Cavinato, M.; Duzzi, D.; Schiff, S.; Foscolo, L.; Venneri, A. Modulation of affective symptoms and resting state activity by brain stimulation in a treatment-resistant case of obsessive-compulsive disorder. Neurocase 2013, 19, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswamy, J.C.; Jose, D.; Chhabra, H.; Agarwal, S.M.; Shrinivasa, B.; Hegde, A.; Bose, A.; Kalmady, S.V.; Venkatasubramanian, G.; Reddy, Y.C.J. Successful Application of Add-on Transcranial Direct Current Stimulation (tDCS) for Treatment of SSRI Resistant OCD. Brain Stimul. 2015, 8, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Mondino, M.; Haesebaert, F.; Poulet, E.; Saoud, M.; Brunelin, J. Efficacy of Cathodal Transcranial Direct Current Stimulation Over the Left Orbitofrontal Cortex in a Patient With Treatment-Resistant Obsessive-Compulsive Disorder. J. ECT 2015, 31, 271–272. [Google Scholar] [CrossRef] [PubMed]
- D’Urso, G.; Brunoni, A.R.; Anastasia, A.; Micillo, M.; de Bartolomeis, A.; Mantovani, A. Polarity-dependent effects of transcranial direct current stimulation in obsessive-compulsive disorder. Neurocase 2016, 22, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.M.; Brunoni, A.R.; Miguel, E.C.; Shavitt, R.G. Transcranial direct current stimulation for treatment-resistant obsessive-compulsive disorder: report on two cases and proposal for a randomized, sham-controlled trial. Sao Paulo Med. J. 2016, 134, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Leitner, B.; Kirsch, B.; Behler, N.; Kumpf, U.; Wulf, L.; Padberg, F.; Hasan, A. Prefrontal tDCS and sertraline in obsessive compulsive disorder: A case report and review of the literature. Neurocase 2017, 23, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Bation, R.; Poulet, E.; Haesebaert, F.; Saoud, M.; Brunelin, J. Transcranial direct current stimulation in treatment-resistant obsessive-compulsive disorder: An open-label pilot study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 65, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Najafi, K.; Fakour, Y.; Zarrabi, H.; Heidarzadeh, A.; Khalkhali, M.; Yeganeh, T.; Farahi, H.; Rostamkhani, M.; Najafi, T.; Shabafroz, S.; et al. Efficacy of Transcranial Direct Current Stimulation in the Treatment: Resistant Patients who Suffer from Severe Obsessive-compulsive Disorder. Indian J. Psychol. Med. 2017, 39, 573–578. [Google Scholar] [CrossRef] [PubMed]
- D’Urso, G.; Brunoni, A.R.; Mazzaferro, M.P.; Anastasia, A.; de Bartolomeis, A.; Mantovani, A. Transcranial direct current stimulation for obsessive-compulsive disorder: A randomized, controlled, partial crossover trial. Depress. Anxiety 2016, 33, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Delgado, P.; Heninger, G.R.; Charney, D.S. The Yale-Brown Obsessive Compulsive Scale. II. Validity. Arch. Gen. Psychiatry 1989, 46, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Leckman, J.F.; Grice, D.E.; Boardman, J.; Zhang, H.; Vitale, A.; Bondi, C.; Alsobrook, J.; Peterson, B.S.; Cohen, D.J.; Rasmussen, S.A.; et al. Symptoms of obsessive-compulsive disorder. Am. J. Psychiatry 1997, 154, 911–917. [Google Scholar] [PubMed]
- Mansur, C.G.; Myczkowki, M.L.; de Barros Cabral, S.; Sartorelli, M.D.C.B.; Bellini, B.B.; Dias, A.M.; Bernik, M.A.; Marcolin, M.A. Placebo effect after prefrontal magnetic stimulation in the treatment of resistant obsessive-compulsive disorder: A randomized controlled trial. Int. J. Neuropsychopharmacol. 2011, 14, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Senço, N.M.; Huang, Y.; D’Urso, G.; Parra, L.C.; Bikson, M.; Mantovani, A.; Shavitt, R.G.; Hoexter, M.Q.; Miguel, E.C.; Brunoni, A.R. Transcranial direct current stimulation in obsessive-compulsive disorder: Emerging clinical evidence and considerations for optimal montage of electrodes. Expert Rev. Med. Devices 2015, 12, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Monte-Silva, K.; Kuo, M.F.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Shaping the Optimal Repetition Interval for Cathodal Transcranial Direct Current Stimulation (tDCS). J. Neurophysiol. 2010, 103, 1735–1740. [Google Scholar] [CrossRef] [PubMed]
- Monte-Silva, K.; Kuo, M.-F.; Hessenthaler, S.; Fresnoza, S.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Induction of Late LTP-Like Plasticity in the Human Motor Cortex by Repeated Non-Invasive Brain Stimulation. Brain Stimul. 2013, 6, 424–432. [Google Scholar] [CrossRef] [PubMed]
- McLaren, M.E.; Nissim, N.R.; Woods, A.J. The effects of medication use in transcranial direct current stimulation: A brief review. Brain Stimul. 2017, 11, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Kuo, M.-F.; Karrasch, R.; Wächter, B.; Liebetanz, D.; Paulus, W. Serotonin Affects Transcranial Direct Current-Induced Neuroplasticity in Humans. Biol. Psychiatry 2009, 66, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.-I.; Paulus, W.; Batsikadze, G.; Jamil, A.; Kuo, M.-F.; Nitsche, M.A. Chronic Enhancement of Serotonin Facilitates Excitatory Transcranial Direct Current Stimulation-Induced Neuroplasticity. Neuropsychopharmacology 2016, 41, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Valiengo, L.; Baccaro, A.; Zanão, T.A.; de Oliveira, J.F.; Goulart, A.; Boggio, P.S.; Lotufo, P.A.; Benseñor, I.M.; Fregni, F. The sertraline vs. electrical current therapy for treating depression clinical study: Results from a factorial, randomized, controlled trial. JAMA Psychiatry 2013, 70, 383–391. [Google Scholar] [CrossRef] [PubMed]
- D’Urso, G.; Dell’Osso, B.; Rossi, R.; Brunoni, A.R.; Bortolomasi, M.; Ferrucci, R.; Priori, A.; de Bartolomeis, A.; Altamura, A.C. Clinical predictors of acute response to transcranial direct current stimulation (tDCS) in major depression. J. Affect. Disord. 2017, 219, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Lewin, A.B.; de Nadai, A.S.; Park, J.; Goodman, W.K.; Murphy, T.K.; Storch, E.A. Refining clinical judgment of treatment outcome in obsessive–compulsive disorder. Psychiatry Res. 2011, 185, 394–401. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
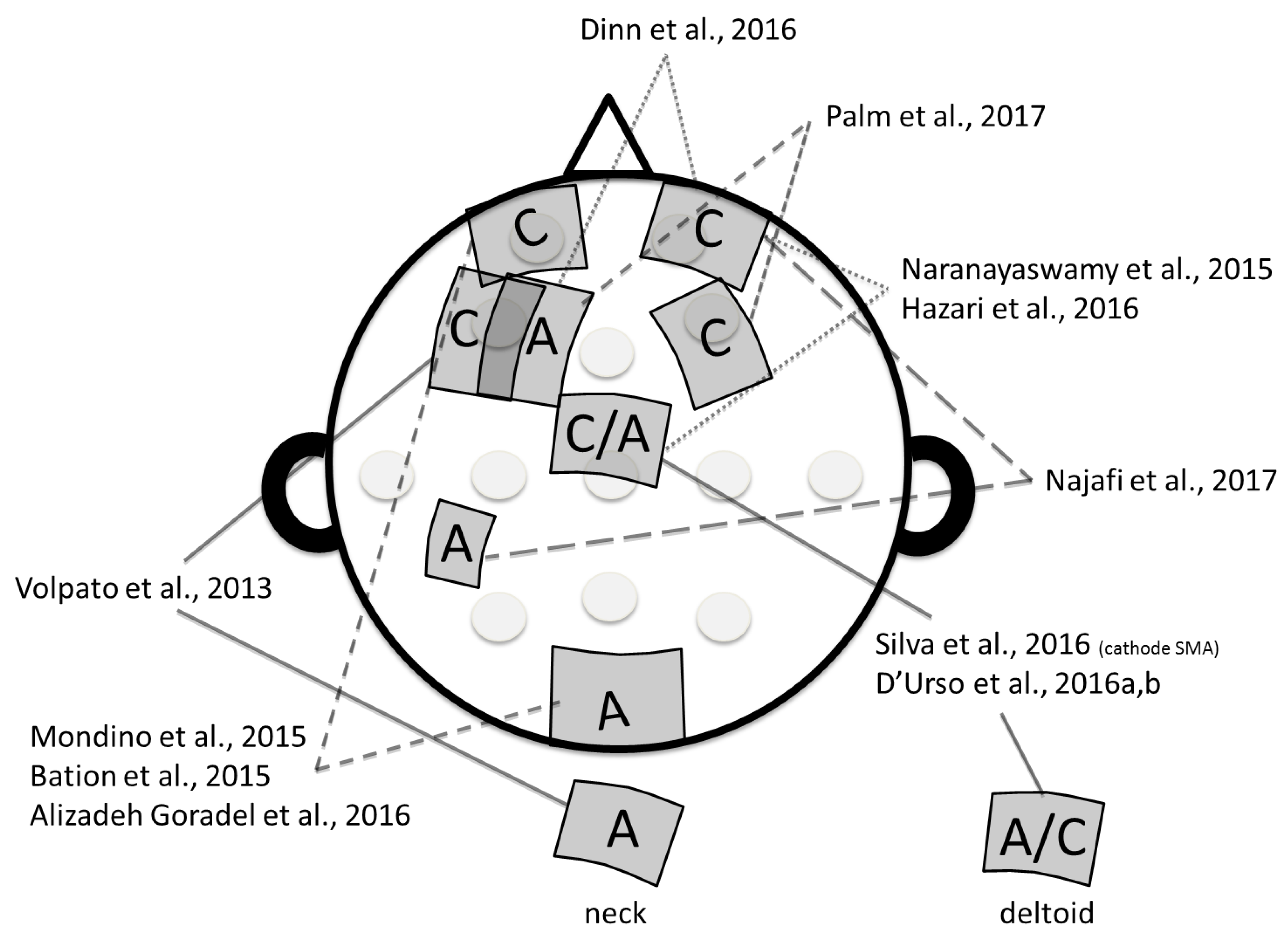
| Articles | N | Patients Characteristics | Target | Intensity Electrode Size | Duration and Number of Sessions | Main Results |
|---|---|---|---|---|---|---|
| Volpato et al., 2013 [20] | 1 | Age: 35, male | Anode: posterior neck-base Cathode: left DLPFC | 2 mA, 35 cm2 | 20 min, 10 sessions (1/day) | No effect on OC symptoms. Depression score decreased (−34% HDRS); anxiety score decreased (−17%). |
| Type*: 2,3,4 | ||||||
| Previous TTT: SSRI, SNRI, CBT | ||||||
| Mondino et al., 2015 [22] | 1 | Age: 52, female | Anode: right cerebello-occipital (100 cm2) Cathode: left OFC | 2 mA, 35 cm2 | 20 min, 10 sessions (2/day; 2 h between 2 sessions) | YBOCS score decreased (−26%) |
| Type*: 3,4 | ||||||
| Previous TTT: tricyclic, SSRI, SNRI, AP, Lithium, CBT | ||||||
| Hazari et al., 2016 [17] | 1 | Age: 24, male | Anode: SMA Cathode: right OFC | 2 mA, ND | 20 min, 20 sessions (2/day, at least 3 h between 2 sessions) | YBOCS decreased (−80%) during 7 months |
| Type*: 1,2 | ||||||
| Previous TTT: SSRI, ECT | ||||||
| D’Urso et al., 2016 [23] | 1 | Age: 33, female | Anode: Pre-SMA Cathode: right deltoid And then, Reverse montage | 2 mA, 25 cm2 | 20 min, 10 sessions (1/day) | Worsening of symptoms after anodal tDCS. |
| Type*: 3 | ||||||
| Previous TTT: SSRI, BZD, tricyclic, CBT | YBOCS score decreased (−30%) after cathodal tDCS, | |||||
| Alizadeh Goradel et al., 2016 [19] | 1 | Age: 23, female | Anode: right occipital Cathode: left OFC | 2 mA, 25 cm2 | 20 min, 10 sessions (1/day) | YBOCS score decreased (−64%); Depression score decreased (−87%); −100% anxiety |
| Type*: 1 | ||||||
| Previous TTT: SSRI | ||||||
| Palm et al., 2017 [25] | 1 | Age: 31, male | Anode: left DLPFC Cathode: Right DLPFC | 2 mA, 35 cm2 | 30 min, 20 sessions (2/day, 3 h between 2 sessions) | Combined with Sertraline, YBOCS score (−22%), depression (−10%) and anxiety (−21%) decreased |
| Type*: 1,3 | ||||||
| Previous TTT: tricyclic, SSRI, AP, CBT | ||||||
| Narayanaswamy et al., 2015 [21] | 2 | Age: 39, female | Anode: left pre-SMA Cathode: right OFC | 2 mA, 35 cm2 | 20 min, 20 sessions (2/day, at least 3 h between 2 sessions) | Patient 1: YBOCS score decreased (−40%), −52% at day 17 |
| Type*: 1 | ||||||
| Previous TTT: SSRI, exposure | ||||||
| Age: 24, male | Patient 2: YBOCS score decreased (−46.7%) | |||||
| Type*: 1 | ||||||
| Previous TTT: tricyclic, SSRI | ||||||
| Silva et al., 2016 [24] | 2 | Age: 37, male | Anode: right deltoid Cathode: bilateral SMA | 2 mA, 25 cm2 | 30 min, 20 sessions (1/day) | Patient 1: no effect at Week 4, YBOCS score decreased at week 12 (−18%). No changes in anxiety nor depression |
| Type*: 2 | ||||||
| Previous TTT: tricyclic, SSRI, CBT | ||||||
| Age: 31, male | Patient 2: YBOCS score decreased, (−17%) at Week 4; −55% at week 12). 50% improvement in anxiety and depression | |||||
| Type*: 1,3 | ||||||
| Previous TTT: tricyclic, SSRI | ||||||
| Dinn et al., 2016 [18] | 5 | Age: 40.4 (8.4), 4 females, 1 male | Anode: left DLPFC Cathode: right OFC | 2 mA, 35 cm2 | 20 min, 15 sessions (1/day) | Open Label Study |
| Type*: ND | ||||||
| Previous TTT: SSRI, SNRI, AP | OC symptoms decreased (−23%); depression decreased (−30%) | |||||
| Bation et al., 2015 [26] | 8 | Age: 44.2 (13.8), 6 females, 2 males | Anode: right cerebellum Cathode: left OFC | 2 mA, 35 cm2 | 20 min, 10 sessions (2/day, at least 3 h between 2 sessions) | Open Label Study |
| Type*: 1 (n = 5), 3 (n = 3) | ||||||
| Previous TTT: tricyclic, 3 SSRI, AP, CBT | YBOCS score decreased (−24.6%) | |||||
| D’Urso et al., 2016 [28] | 12 | Age: 39.0 (13.1), 7 females, 5 males | Anode midline pre SMA Cathode: right deltoid (n = 6) OR reverse montage | 2 mA, 25 cm2 | 20 min, 10 sessions (1/day) | RCT—10 patients completed the study |
| Type*: 1 (n = 4), 2 (n = 2), 3 (n = 6) | Cathodal tDCS was significantly more effective than anodal tDCS. In cathodal arm, YBOCS score decreased (−17.5%) after 10 sessions, −20.1% after 20 sessions | |||||
| Previous TTT: at least SSRI, CBT | ||||||
| Najafi et al., 2017 [27] | 42 | Age: 29.1 (10.1), 23 females, 19 males | Anode: parieto-temporo-occipital areas Cathode: right OFC | 2–3 mA, 5.5 cm² | 30 min, 15 sessions (1/day) | Open Label Study |
| YBOCS score decreased (−63.4%) | ||||||
| Type*: ND | ||||||
| Previous TTT: at least 2 SSRI, CBT | Maintenance of the effect at 3 months follow up (−77.6%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunelin, J.; Mondino, M.; Bation, R.; Palm, U.; Saoud, M.; Poulet, E. Transcranial Direct Current Stimulation for Obsessive-Compulsive Disorder: A Systematic Review. Brain Sci. 2018, 8, 37. https://doi.org/10.3390/brainsci8020037
Brunelin J, Mondino M, Bation R, Palm U, Saoud M, Poulet E. Transcranial Direct Current Stimulation for Obsessive-Compulsive Disorder: A Systematic Review. Brain Sciences. 2018; 8(2):37. https://doi.org/10.3390/brainsci8020037
Chicago/Turabian StyleBrunelin, Jérôme, Marine Mondino, Rémy Bation, Ulrich Palm, Mohamed Saoud, and Emmanuel Poulet. 2018. "Transcranial Direct Current Stimulation for Obsessive-Compulsive Disorder: A Systematic Review" Brain Sciences 8, no. 2: 37. https://doi.org/10.3390/brainsci8020037
APA StyleBrunelin, J., Mondino, M., Bation, R., Palm, U., Saoud, M., & Poulet, E. (2018). Transcranial Direct Current Stimulation for Obsessive-Compulsive Disorder: A Systematic Review. Brain Sciences, 8(2), 37. https://doi.org/10.3390/brainsci8020037