Frameless Stereotaxis for Subthalamic Nucleus Deep Brain Stimulation: An Innovative Method for the Direct Visualization of Electrode Implantation by Intraoperative X-ray Control


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgery Planning
2.3. Innovative Tools
- (a)
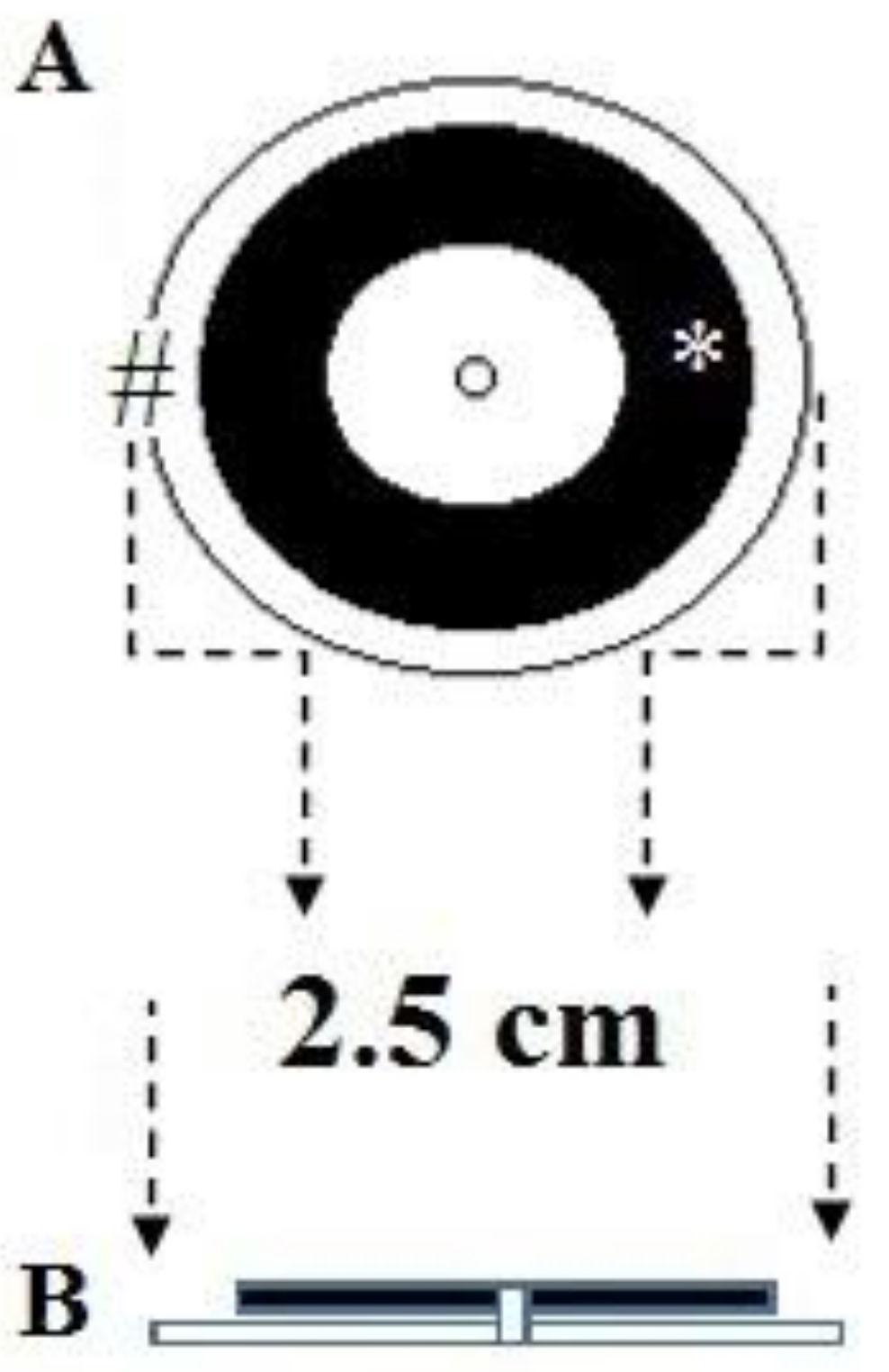
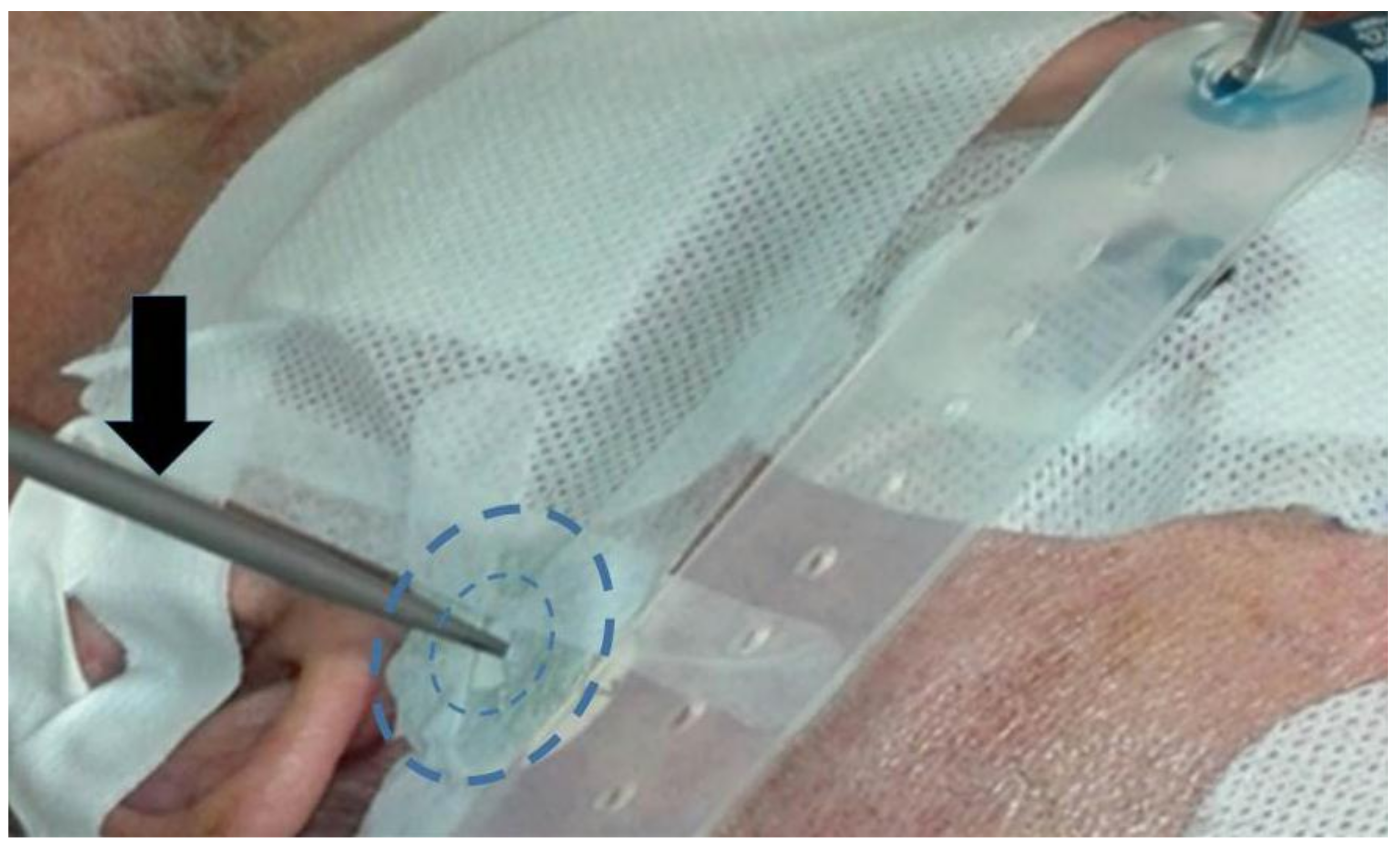
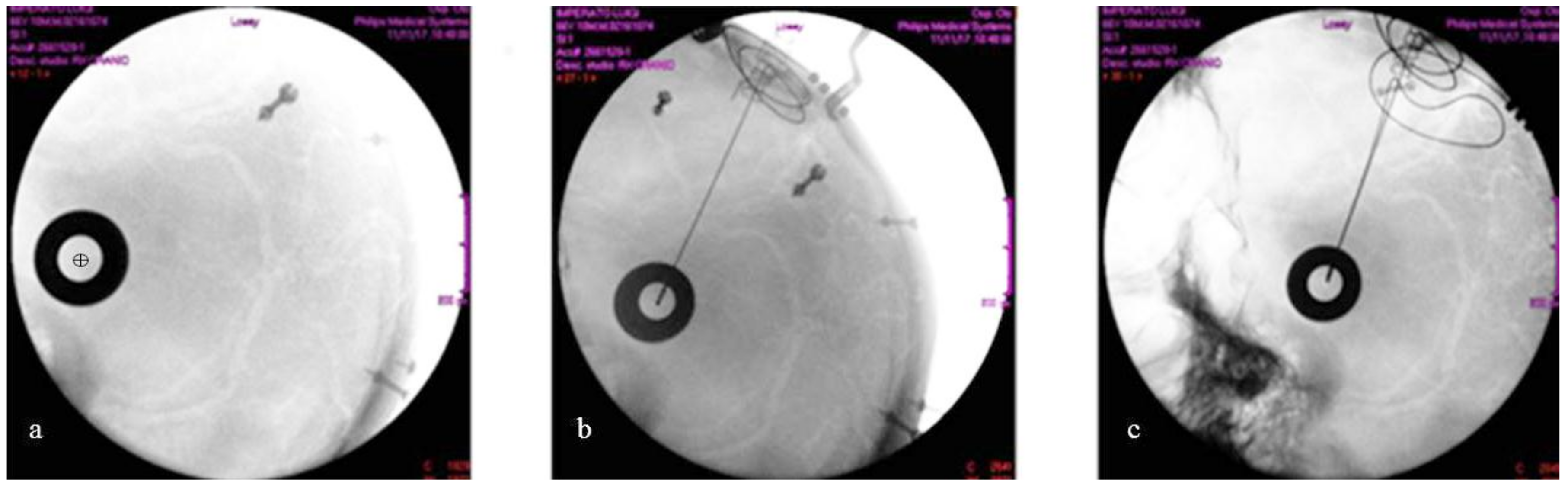
- A system of two fiducials visible to X-rays, which were used to align the two STN target points under intraoperative X-ray control. Each fiducial was a flat ring of radiopaque metal with an external diameter of 2.5 cm (Figure 3 and Figure 4). It was mounted on a plastic ring support provided with a central hole of the same size as the probe employed to determine the horizontal entry point line (Figure 3 and Figure 4).
- (b)
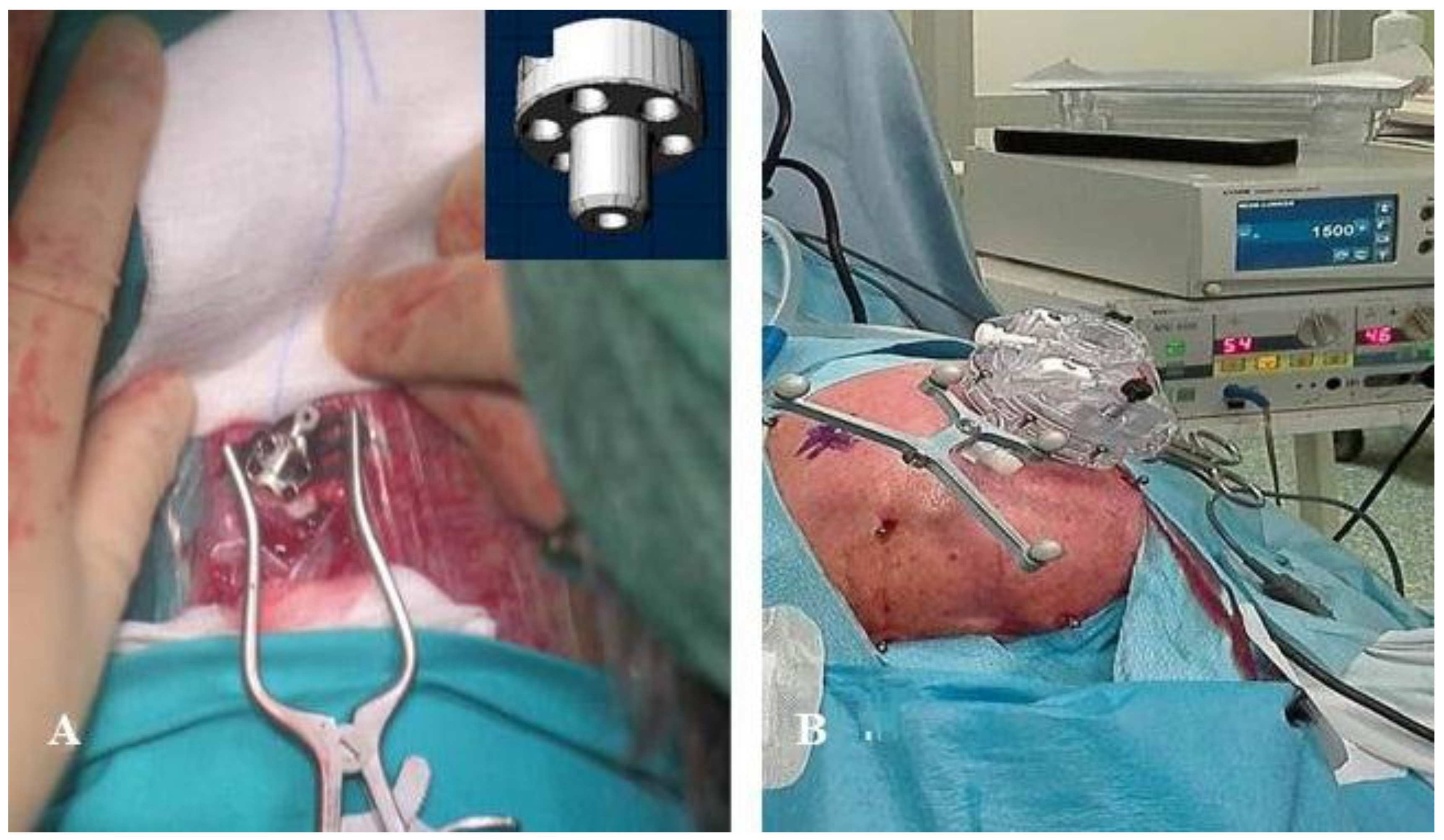
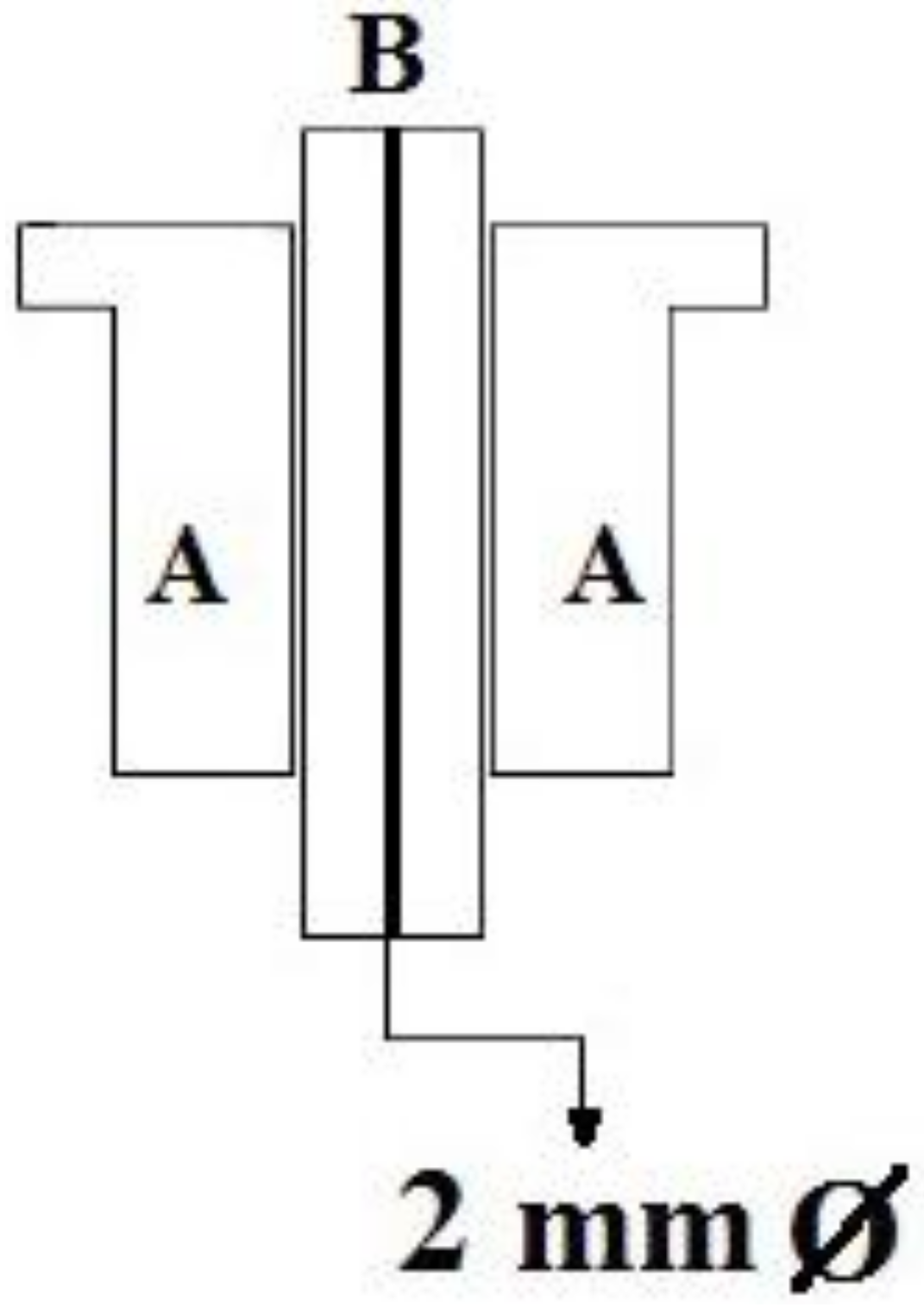
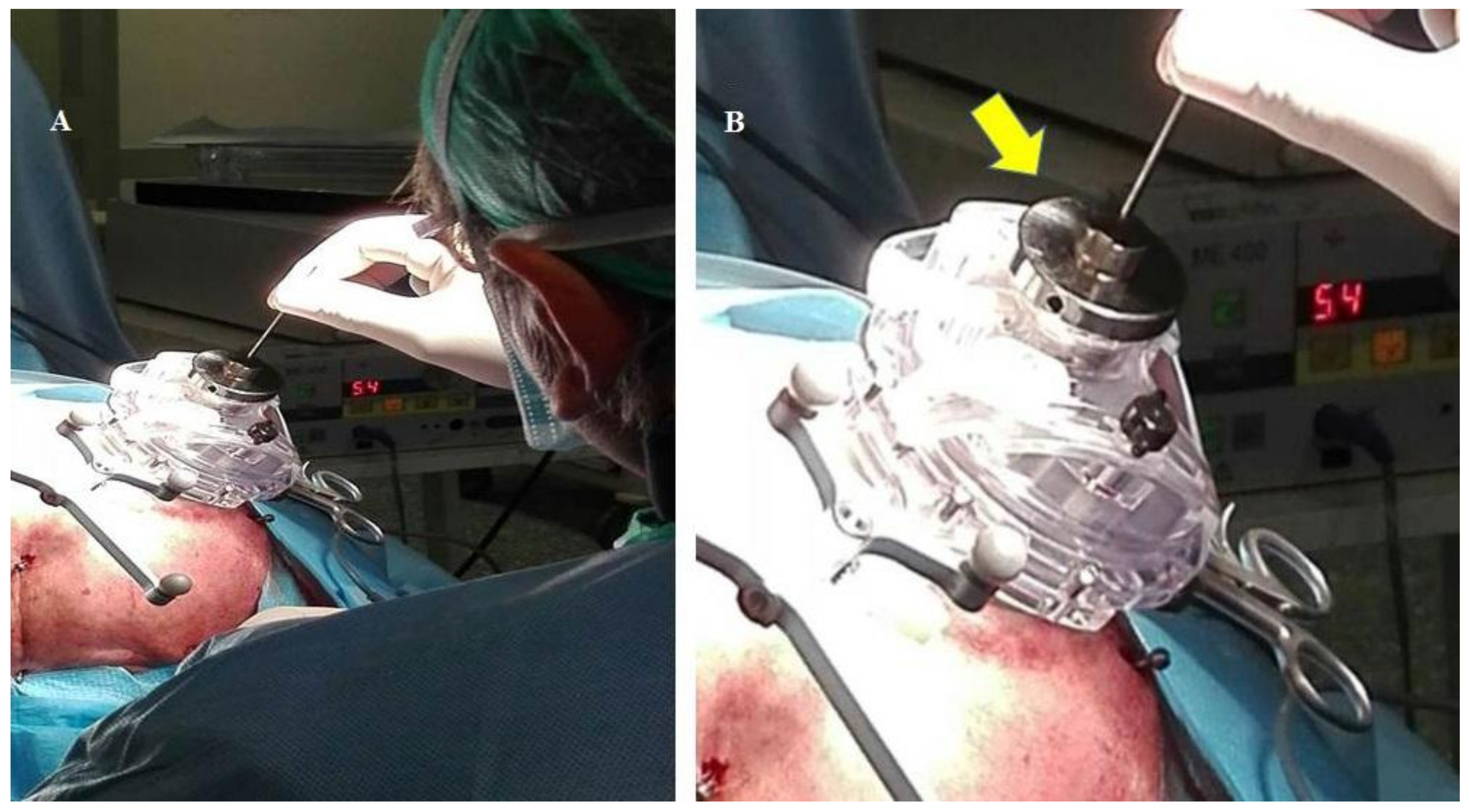
- An amagnetic stainless steel cylindrical rocket (Figure 5 and Figure 6). The rocket was designed to fit inside the tower body of the Nexframe. A second amagnetic stainless steel cylinder was fitted into the central part of the cylindrical rocket. Its height was variable with respect to the bone plane and the Nexframe tower body level. It served to measure the distance of the 0 plan from the target point. Inside the second cylinder a circular track with a diameter of 2 mm allowed a precise hole for inserting the electrode guide tube to be drilled with a calibrated bit (Figure 5 and Figure 6).
2.4. Surgical Procedure
2.5. Data Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Mazzone, P. Il sistema stereotassico 3P maranello. Eur. Medicophys. 2001, 3, 318–319. [Google Scholar]
- Holloway, K.L.; Gaede, S.E.; Starr, P.A.; Rosenow, J.M.; Ramakrishnan, V.; Henderson, J.M. Frameless stereotaxy using bone fiducial markers for deep brain stimulation. J. Neurosurg. 2005, 103, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Palys, V.; Holloway, K.L. Frameless Functional Stereotactic Approaches. Prog. Neurol. Surg. 2018, 33, 168–186. [Google Scholar] [PubMed]
- Verhagen, M.L.; Pilitsis, J.G.; Stebbins, G.T.; Bot, M.; Bakay, R.A. Intraoperative X-ray to measure distance between DBS leads: A reliability study. Mov. Disord. 2012, 27, 1056–1059. [Google Scholar] [CrossRef] [PubMed]
- Burchiel, K.J.; McCartney, S.; Lee, A.; Raslan, A.M. Accuracy of deep brain stimulation electrode placement using intraoperative computed tomography without microelectrode recording. J. Neurosurg. 2013, 119, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.J.; Larson, P.S.; Ostrem, J.L.; Keith, S.W.; Talke, P.; Weber, O.M.; Levesque, N.; Myers, J.; Starr, P.A. Placement of deep brain stimulator electrodes using real-time high-field interventional magnetic resonance imaging. Magn. Reson. Med. 2005, 54, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Deogaonkar, M. Accuracy and safety of targeting using intraoperative “O-arm” during placement of deep brain stimulation electrodes without electrophysiological recordings. J. Clin. Neurosci. 2016, 27, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.P.; Bakay, R.A. Frameless deep brain stimulation using intraoperative O-arm technology. Clinical article. J. Neurosurg. 2011, 115, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Slavin, K.V.; Anderson, G.J.; Burchiel, K.J. Comparison of three techniques for calculation of target coordinates in functional stereotactic procedures. Stereotact. Funct. Neurosurg. 1999, 72, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Slavin, K.V.; Thulborn, K.R.; Wess, C.; Nersesyan, H. Direct visualization of the human subthalamic nucleus with 3T MR imaging. AJNR Am. J. Neuroradiol. 2006, 27, 80–84. [Google Scholar] [PubMed]
- Metman, L.V.; Slavin, K.V. Advances in functional neurosurgery for Parkinson’s disease. Mov. Disord. 2015, 30, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, P. A new arch-less stereotactic device. Stereotact. Funct. Neurosurg. 2007, 85, 63. [Google Scholar]
- Mazzone, P.; Arena, P.; Cantelli, L.; Spampinato, G.; Sposato, S.; Cozzolino, S.; Demarinis, P.; Muscato, G. Experimental new automatic tools for robotic stereotactic neurosurgery: Towards “no hands” procedure of leads implantation into a brain target. J. Neural Transm. (Vienna) 2016, 123, 737–750. [Google Scholar] [CrossRef] [PubMed]
- Bot, M.; van den Munckhof, P.; Bakay, R.; Sierens, D.; Stebbins, G.; Verhagen, M.L. Analysis of Stereotactic Accuracy in Patients Undergoing Deep Brain Stimulation Using Nexframe and the Leksell Frame. Stereotact. Funct. Neurosurg. 2015, 93, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Hsing, M.T.; Chen, Y.H.; Wu, S.L.; Sy, H.N.; Chen, C.M.; Yang, Y.J.; Lee, M.C. Deep brain stimulation for Parkinson’s disease using frameless technology. Br. J. Neurosurg. 2014, 28, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Kelman, C.; Ramakrishnan, V.; Davies, A.; Holloway, K. Analysis of stereotactic accuracy of the cosman-robert-wells frame and nexframe frameless systems in deep brain stimulation surgery. Stereotact. Funct. Neurosurg. 2010, 88, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Bronte-Stewart, H.; Louie, S.; Batya, S.; Henderson, J.M. Clinical motor outcome of bilateral subthalamic nucleus deep-brain stimulation for Parkinson’s disease using image-guided frameless stereotaxy. Neurosurgery 2010, 67, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Rhiew, R.; Deogaonkar, M.; Rezai, A.; Boulis, N. Accuracy and precision of targeting using frameless stereotactic system in deep brain stimulator implantation surgery. Neurol. India 2014, 62, 503–509. [Google Scholar] [PubMed]
- Steinmeier, R.; Rachinger, J.; Kaus, M.; Ganslandt, O.; Huk, W.; Fahlbusch, R. Factors influencing the application accuracy of neuronavigation systems. Stereotact. Funct. Neurosurg. 2000, 75, 188–202. [Google Scholar] [CrossRef] [PubMed]
- Insola, A.; Mazzone, P.; Valeriani, M. Somatosensory evoked potential and clinical changes after electrode implant in basal ganglia of parkinsonian patients. Muscle Nerve 2005, 32, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, P.; Sposato, S.; Insola, A.; Scarnati, E. The deep brain stimulation of the pedunculopontine tegmental nucleus: Towards a new stereotactic neurosurgery. J. Neural Transm. 2011, 118, 1431–1451. [Google Scholar] [CrossRef] [PubMed]
- Delavallee, M.; Delaunois, J.; Ruwet, J.; Jeanjean, A.; Raftopoulos, C. STN DBS for Parkinson’s disease: Results from a series of ten consecutive patients implanted under general anaesthesia with intraoperative use of 3D fluoroscopy to control lead placement. Acta Neurochir. (Wien.) 2016, 158, 1783–1788. [Google Scholar] [CrossRef] [PubMed]
- Ritman, E.L. Vision 20/20: Increased image resolution versus reduced radiation exposure. Med. Phys. 2008, 35, 2502–2512. [Google Scholar] [CrossRef] [PubMed]
- Starr, P.A.; Martin, A.J.; Ostrem, J.L.; Talke, P.; Levesque, N.; Larson, P.S. Subthalamic nucleus deep brain stimulator placement using high-field interventional magnetic resonance imaging and a skull-mounted aiming device: Technique and application accuracy. J. Neurosurg. 2010, 112, 479–490. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Implanted with X-ray Control | X | Y | Z | Patients Implanted without X-ray Control | Difference in the Depth of Right and Left Electrode | X | Y | Z |
|---|---|---|---|---|---|---|---|---|
| 1 | 0.9 | 0.5 | 0.5 | 1 | 4 | 1.5 | 2.1 | 3.5 |
| 2 | 0.9 | 2.4 | 0.2 | 2 | 1 | 1.0 | 2.3 | 3.0 |
| 3 | 1.5 | 3.3 | 0.5 | 3 | 2 | 0.5 | 3.4 | 2.0 |
| 4 | 0.4 | 3.2 | 0.7 | 4 | 1 | 1.6 | 2.2 | 3.1 |
| 5 | 0.2 | 1.1 | 0.6 | 5 | 3 | 1.5 | 2.5 | 3.2 |
| 6 | 2.2 | 1.3 | 0.3 | 6 | 3 | 0.7 | 3.1 | 2.8 |
| 7 | 1.0 | 0.5 | 0.6 | Mean ± S.D (mm) | 2.3 ± 1.2 | 1.1 ± 0.5 | 2.6 ± 0.5 | 2.9 ± 0.5 |
| 8 | 0.5 | 1.3 | 0.5 | |||||
| Mean ± SD (mm) | 0.95 ± 0.76 | 1.87 ± 1.0 * | 0.48 ± 0.1 * |
| Preoperative UPDRS III DBS ON | Postoperative UPDRS III DBS ON | Preoperative LIDs DBS ON | Postoperative LIDs DBS ON | Preoperative L- Dopa mg/die | Postoperative L-Dopa mg/die | Days Required in Programming DBS Setup | |
|---|---|---|---|---|---|---|---|
| Patients implanted with intraoperative X-ray control | 25 ± 6.1 | 14 ± 4.5 * | 3.3 ± 0.9 | 1.8 ± 0.8 ** | 1.150 ± 227 | 895 ± 165 | 4 ± 3 *** |
| Patients implanted without intraoperative X-ray control | 26 ± 3.6 | 16 ± 3.9 * | 3.6 ± 0.5 | 2.3 ± 0.5 ** | 1.240 ± 461 | 1.040 ± 270 | 10 ± 3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzone, P.; Stefani, A.; Viselli, F.; Scarnati, E. Frameless Stereotaxis for Subthalamic Nucleus Deep Brain Stimulation: An Innovative Method for the Direct Visualization of Electrode Implantation by Intraoperative X-ray Control. Brain Sci. 2018, 8, 90. https://doi.org/10.3390/brainsci8050090
Mazzone P, Stefani A, Viselli F, Scarnati E. Frameless Stereotaxis for Subthalamic Nucleus Deep Brain Stimulation: An Innovative Method for the Direct Visualization of Electrode Implantation by Intraoperative X-ray Control. Brain Sciences. 2018; 8(5):90. https://doi.org/10.3390/brainsci8050090
Chicago/Turabian StyleMazzone, Paolo, Alessandro Stefani, Fabio Viselli, and Eugenio Scarnati. 2018. "Frameless Stereotaxis for Subthalamic Nucleus Deep Brain Stimulation: An Innovative Method for the Direct Visualization of Electrode Implantation by Intraoperative X-ray Control" Brain Sciences 8, no. 5: 90. https://doi.org/10.3390/brainsci8050090
APA StyleMazzone, P., Stefani, A., Viselli, F., & Scarnati, E. (2018). Frameless Stereotaxis for Subthalamic Nucleus Deep Brain Stimulation: An Innovative Method for the Direct Visualization of Electrode Implantation by Intraoperative X-ray Control. Brain Sciences, 8(5), 90. https://doi.org/10.3390/brainsci8050090