Changes in Retinal OCT and Their Correlations with Neurological Disability in Early ALS Patients, a Follow-Up Study

 ,
, 
 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants: Study Groups and Selection Criteria
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
3.1. ALSFRS-R
3.2. Best-Corrected Visual Acuity (BCVA)
3.3. Visual Field (VF)
3.4. Optical Coherence Tomography (OCT)
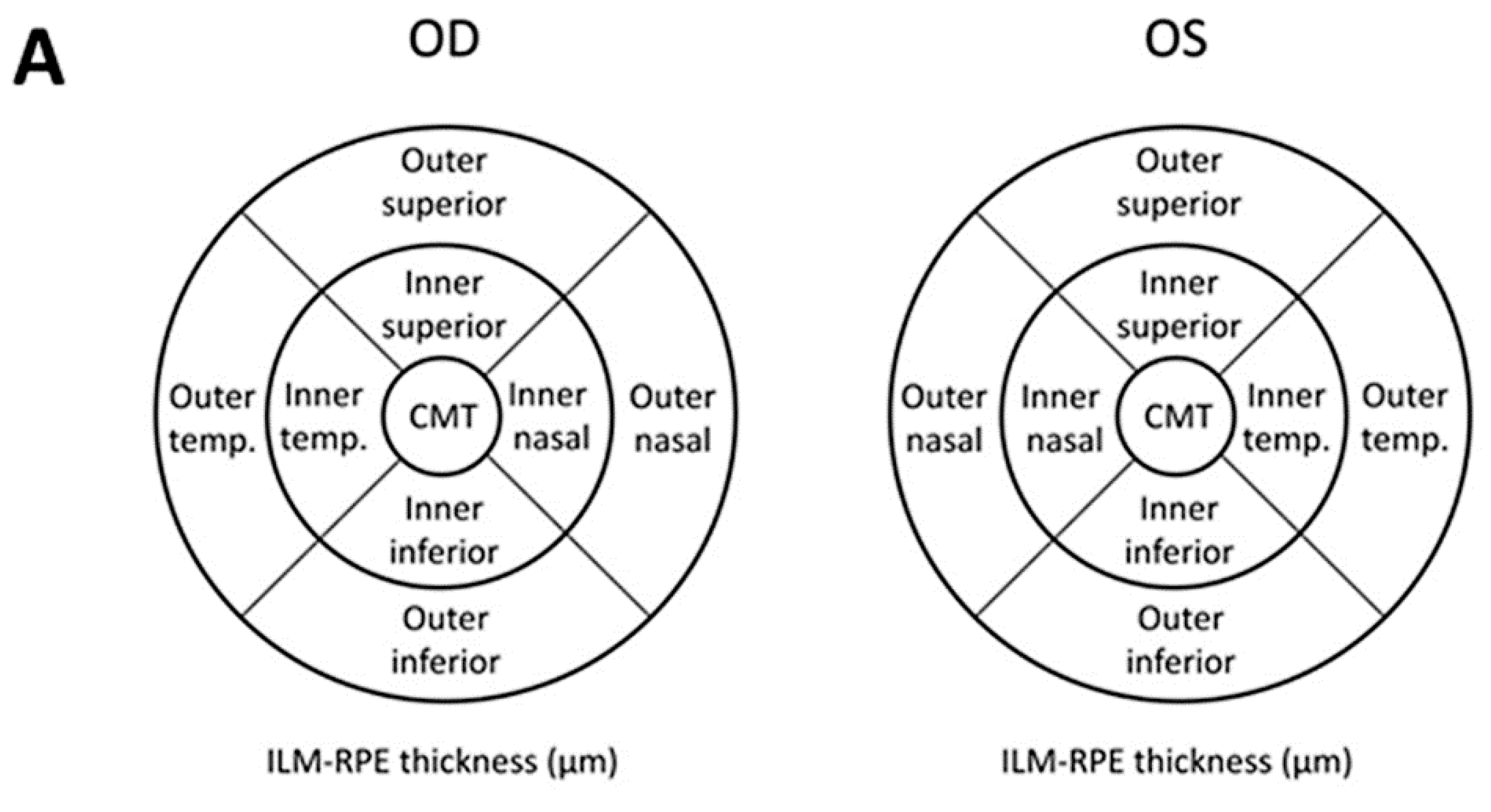
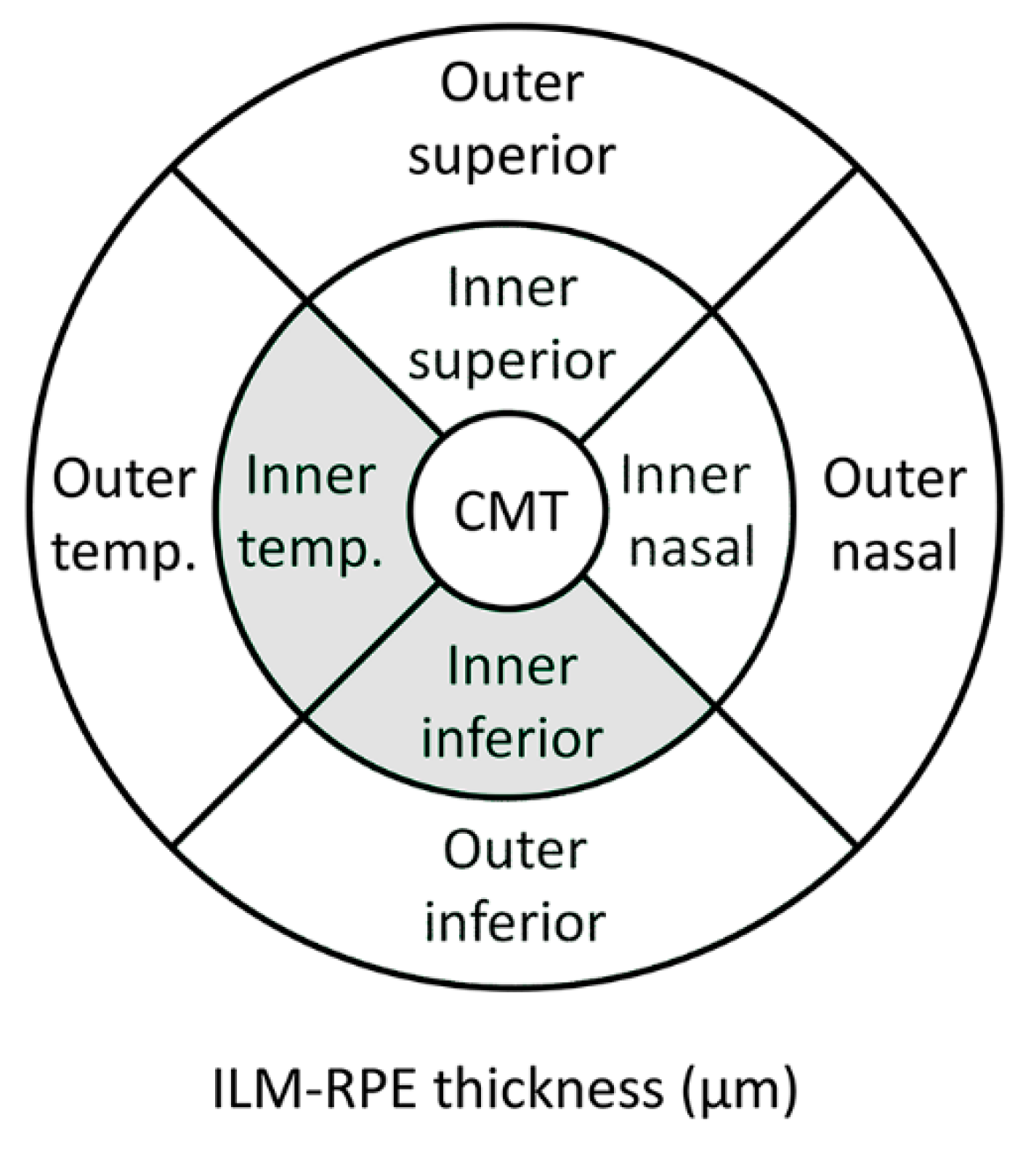
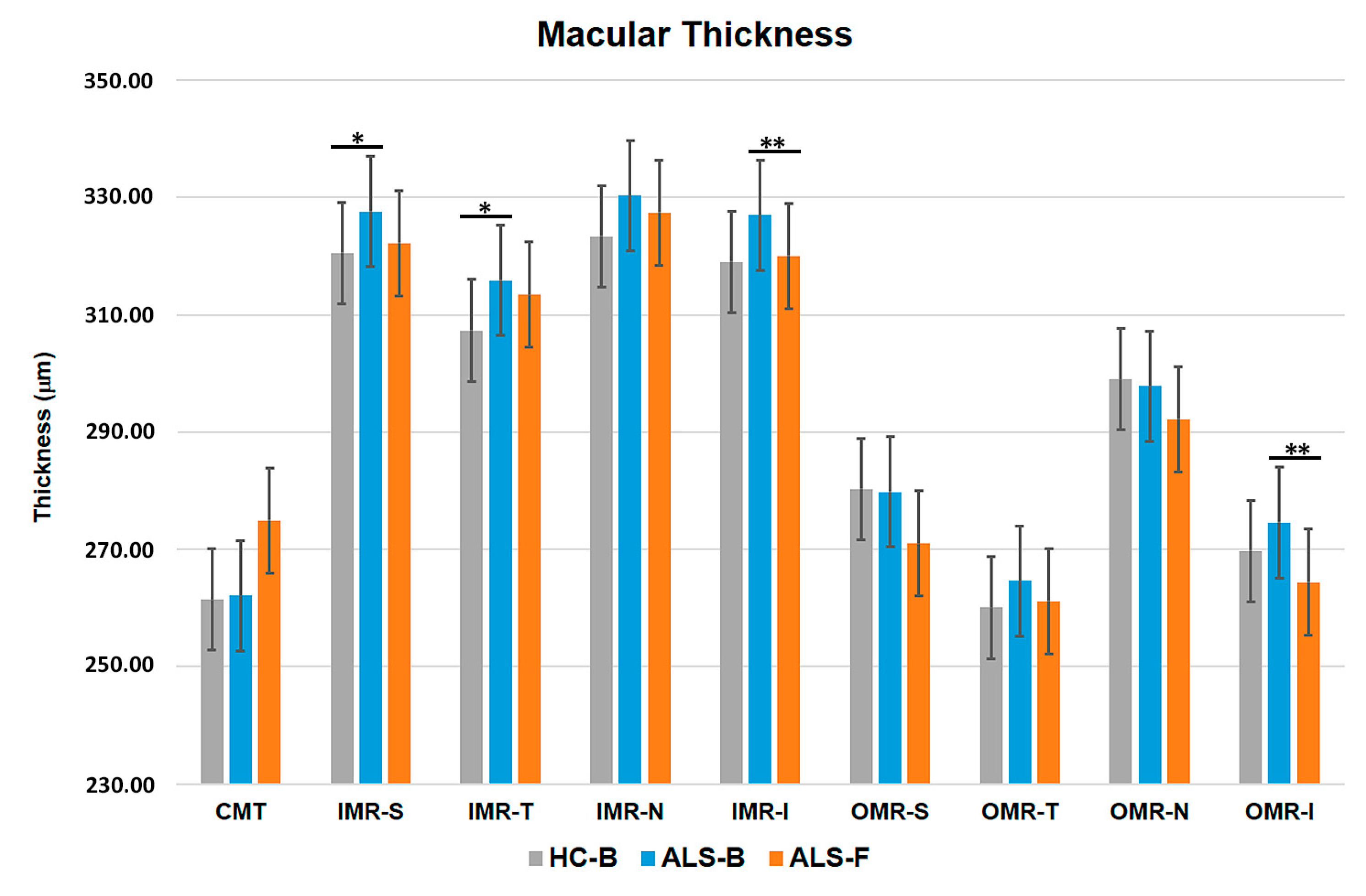
3.5. Macular Thickness (MT)
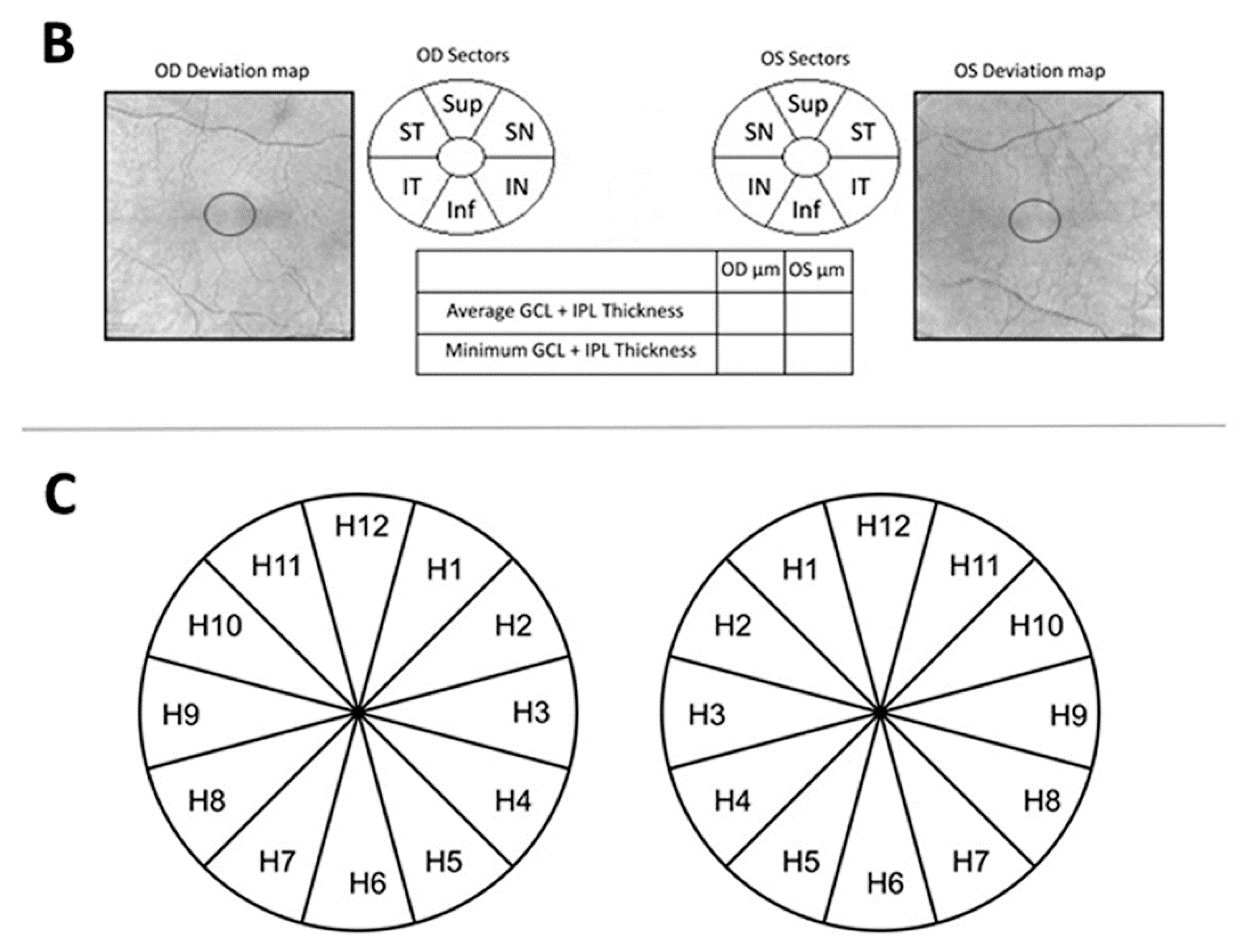
3.6. Ganglion Cell Complex (GCC)
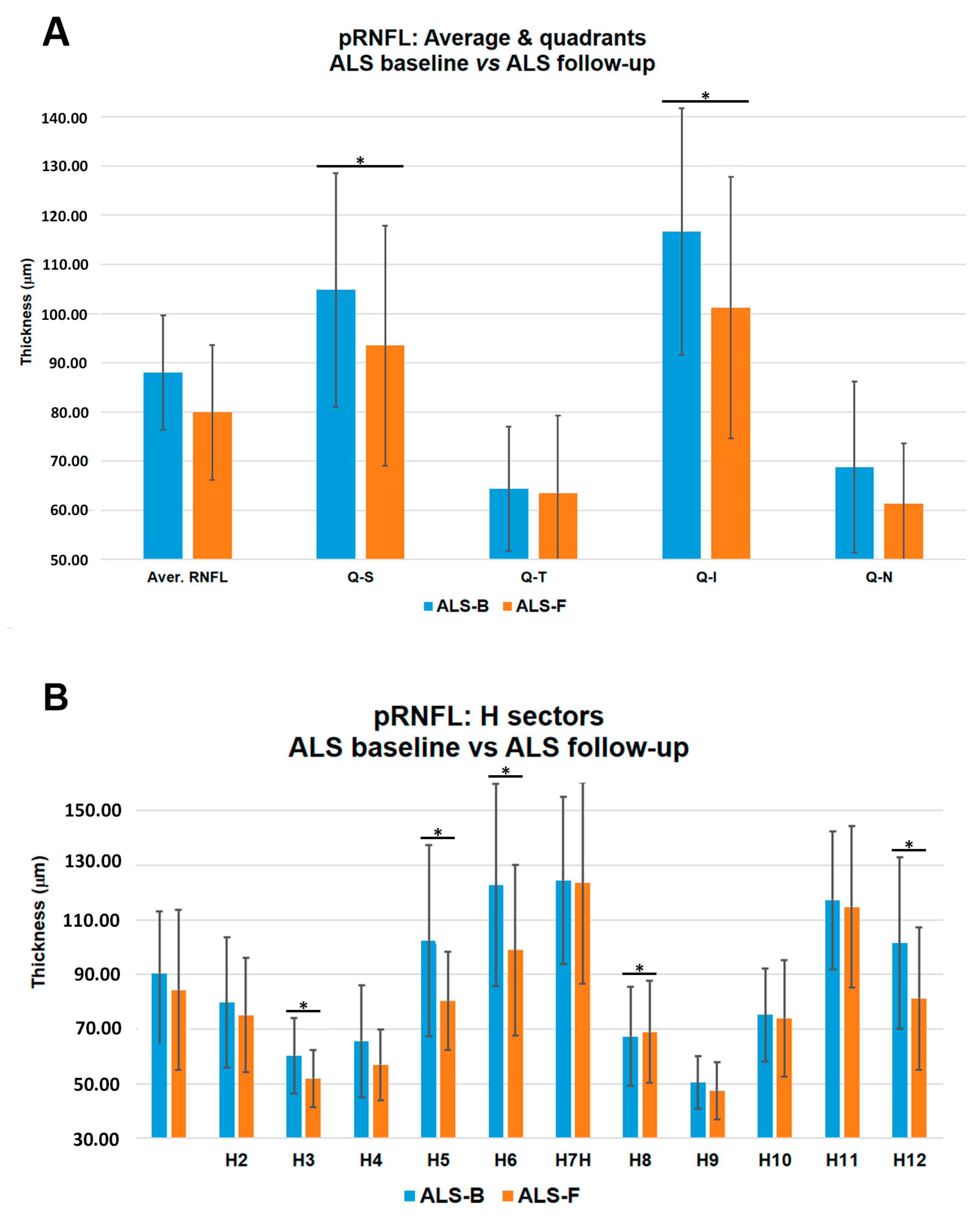
3.7. Peripapillary Retinal Nerve Fiber Layer (pRNFL)
3.8. Interocular Asymmetry
- (1)
- The ALS baseline group in the inferior-nasal area of GCC (RE: 80.60 ± 7.01 and LE: 73.80 ± 13.93 µm, p = 0.042) and in the sectors H7 (RE: 133.00 ± 24.69 and LE: 116.00 ± 34.62 µm, p = 0.022) and H9 (RE: 53.90 ± 11.51 and LE: 47.00 ± 5.93 µm, p = 0.020).
- (2)
- The ALS follow-up group: In the supero-nasal quadrant of the GCC (RE: 79.00 ± 9.27 and LE: 76.00 ± 11.53 µm, p = 0.043), in the temporal quadrant of pRNFL (RE: 68.40 ± 16.04 and LE: 58.60 ± 15.66 µm, p = 0.039), and in sectors H8 (RE: 75.00 ± 18.55 and LE: 63.00 ± 18.87 µm, p = 0.043) and H9 (RE: 50.80 ± 12.40 and LE: 44.20 ± 8.11 µm, p = 0.043).
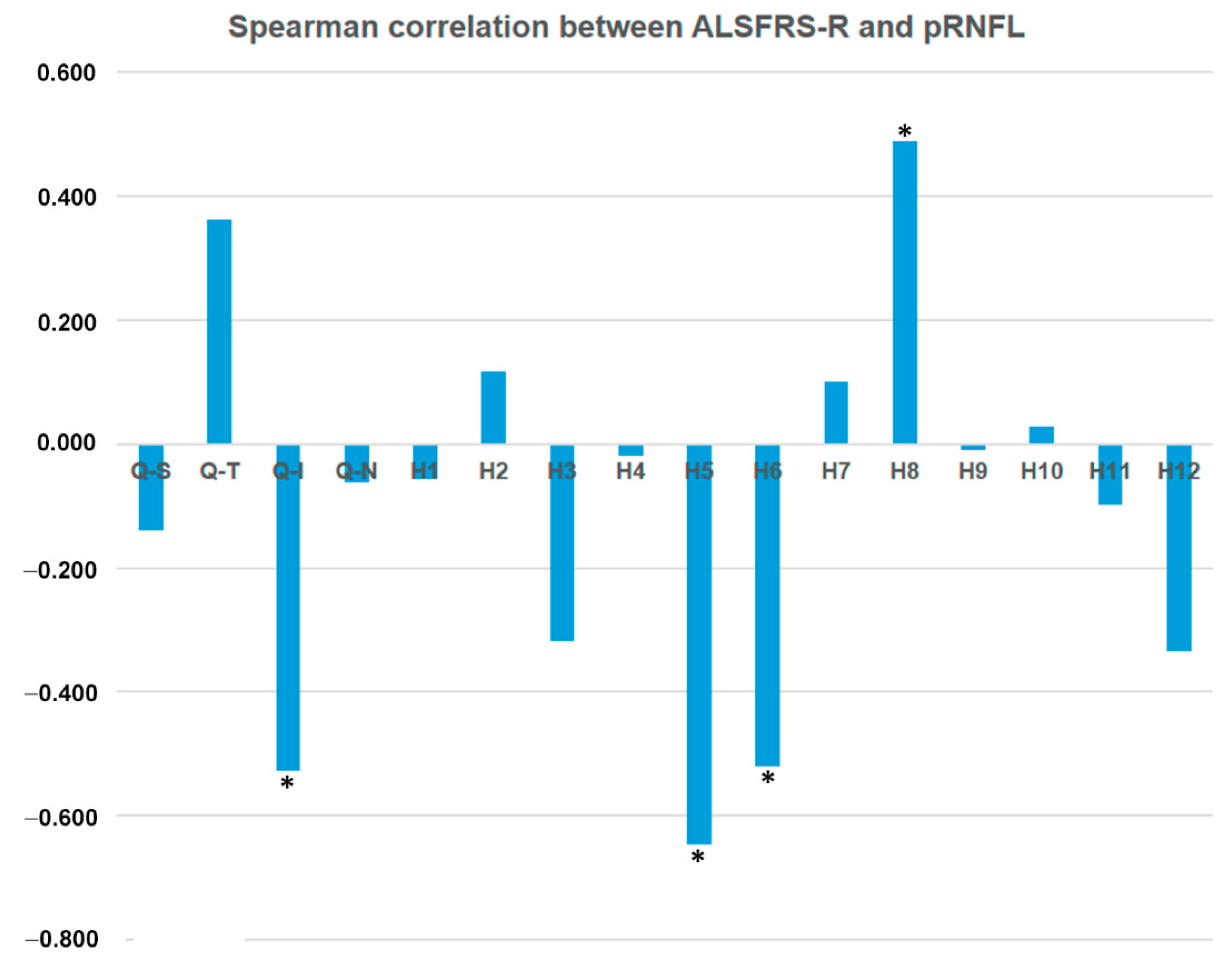
3.9. Spearman Correlations between OCT Measurements and ASLFRS-R Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pratt, A.J.; Getzoff, E.D.; Perry, J.J.P. Amyotrophic lateral sclerosis: Update and new developments. Degener. Neurol. Neuromuscul. Dis. 2012, 2012, 1–14. [Google Scholar] [PubMed]
- Wijesekera, L.C.; Leigh, P.N. Amyotrophic lateral sclerosis. Orphanet J. Rare Dis. 2009, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Averbuch-Heller, L.; Helmchen, C.; Horn, A.K.; Leigh, R.J.; Büttner-Ennerver, J.A. Slow vertical saccades in motor neuron disease: Correlation of structure and function. Ann. Neurol. 1998, 44, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Gizzi, M.; DiRocco, A.; Sivak, M.; Cohen, B. Ocular motor function in motor neuron disease. Neurology 1992, 42, 1037–1046. [Google Scholar] [CrossRef]
- Puligheddu, M.; Congiu, P.; Aricò, D.; Rundo, F.; Borghero, G.; Marrosu, F.; Fantini, M.L.; Ferri, R. Isolated rapid eye movement sleep without atonia in amyotrophic lateral sclerosis. Sleep Med. 2016, 26, 16–22. [Google Scholar] [CrossRef]
- Cedarbaum, J.M.; Stambler, N.; Malta, E.; Fuller, C.; Hilt, D.; Thurmond, B.; Nakanishi, A. The ALSFRS-R: A revised ALS functional rating scale that incorporates assessments of respiratory function. BDNF ALS Study Group (Phase III). J. Neurol. Sci. 1999, 169, 13–21. [Google Scholar] [CrossRef]
- Roth, N.M.; Saidha, S.; Zimmermann, H.; Brandt, A.U.; Oberwahrenbrock, T.; Maragakis, N.J.; Tumani, H.; Ludolph, A.C.; Meyer, T.; Calabresi, P.A.; et al. Optical coherence tomography does not support optic nerve involvement in amyotrophic lateral sclerosis. Eur. J. Neurol. 2013, 20, 1170–1176. [Google Scholar] [CrossRef]
- Ringholz, G.M.; Appel, S.H.; Bradshaw, M.; Cooke, N.A.; Mosnik, D.M.; Schulz, P.E. Prevalence and patterns of cognitive impairment in sporadic ALS. Neurology 2005, 65, 586–590. [Google Scholar] [CrossRef]
- Abrahams, S.; Goldstein, L.H.; Suckling, J.; Ng, V.; Simmons, A.; Chitnis, X.; Atkins, L.; Williams, S.C.R.; Leigh, P.N. Frontotemporal white matter changes in amyotrophic lateral sclerosis. J. Neurol. 2005, 252, 321–331. [Google Scholar] [CrossRef]
- Kassubek, J.; Unrath, A.; Huppertz, H.-J.; Lulé, D.; Ethofer, T.; Sperfeld, A.-D.; Ludolph, A.C. Global brain atrophy and corticospinal tract alterations in ALS, as investigated by voxel-based morphometry of 3-D MRI. Amyotroph. Lateral Scler. Other Motor Neuron Disord. 2005, 6, 213–220. [Google Scholar] [CrossRef]
- Mezzapesa, D.; Ceccarelli, A.; Dicuonzo, F.; Carella, A.; De Caro, M.F.; Lopez, M.; Samarelli, V.; Livrea, P.; Simone, I.L. Whole-Brain and Regional Brain Atrophy in Amyotrophic Lateral Sclerosis. AJNR Am. J. Neuroradiol. 2007, 28, 255–259. [Google Scholar] [PubMed]
- Ellis, C.M.; Suckling, J.; Amaro, E.; Bullmore, E.T.; Simmons, A.; Williams, S.C.; Leigh, P.N. Volumetric analysis reveals corticospinal tract degeneration and extramotor involvement in ALS. Neurology 2001, 57, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Weis, J.; Katona, I.; Müller-Newen, G.; Sommer, C.; Necula, G.; Hendrich, C.; Ludolph, A.C.; Sperfeld, A.-D. Small-fiber neuropathy in patients with ALS. Neurology 2011, 76, 2024–2029. [Google Scholar] [CrossRef] [PubMed]
- Radtke, R.A.; Erwin, A.; Erwin, C.W. Abnormal sensory evoked potentials in amyotrophic lateral sclerosis. Neurology 1986, 36, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Matheson, J.K.; Harrington, H.J.; Hallett, M. Abnormalities of multimodality evoked potentials in amyotrophic lateral sclerosis. Arch. Neurol. 1986, 43, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Münte, T.F.; Tröger, M.C.; Nusser, I.; Wieringa, B.M.; Johannes, S.; Matzke, M.; Dengler, R. Alteration of early components of the visual evoked potential in amyotrophic lateral sclerosis. J. Neurol. 1998, 245, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, J.S.; Yiannikas, C. Multimodality evoked potentials in motor neuron disease. Arch. Neurol. 1990, 47, 989–994. [Google Scholar] [CrossRef]
- Sharma, R.; Hicks, S.; Berna, C.M.; Kennard, C.; Talbot, K.; Turner, M.R. Oculomotor dysfunction in amyotrophic lateral sclerosis: A comprehensive review. Arch. Neurol. 2011, 68, 857–861. [Google Scholar] [CrossRef]
- Shaunak, S.; Orrell, R.W.; O’Sullivan, E.; Hawken, M.B.; Lane, R.J.; Henderson, L.; Kennard, C. Oculomotor function in amyotrophic lateral sclerosis: Evidence for frontal impairment. Ann. Neurol. 1995, 38, 38–44. [Google Scholar] [CrossRef]
- Kang, B.H.; Kim, J.I.; Lim, Y.M.; Kim, K.K. Abnormal Oculomotor Functions in Amyotrophic Lateral Sclerosis. J. Clin. Neurol. 2018, 14, 464–471. [Google Scholar] [CrossRef]
- Kushner, P.D.; Stephenson, D.T.; Wright, S. Reactive astrogliosis is widespread in the subcortical white matter of amyotrophic lateral sclerosis brain. J. Neuropathol. Exp. Neurol. 1991, 50, 263–277. [Google Scholar] [CrossRef] [PubMed]
- Galetta, K.M.; Calabresi, P.A.; Frohman, E.M.; Balcer, L.J. Optical coherence tomography (OCT): Imaging the visual pathway as a model for neurodegeneration. Neurotherapeutics 2011, 8, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Ratchford, J.N.; Quigg, M.E.; Conger, B.A.; Frohman, B.T.; Frohman, B.E.; Balcer, L.J.; Calabresi, P.A.; Kerr, D.A. Optical coherence tomography helps differentiate neuromyelitis optica and MS optic neuropathies. Neurology 2009, 73, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Galetta, S.S.L. MS and NMO: Partners no more. J. Neuro Ophthalmol. 2012, 32, 99–101. [Google Scholar]
- Albrecht, P.; Müller, A.-K.; Ringelstein, M.; Finis, D.; Geerling, G.; Cohn, E.; Aktas, O.; Hartung, H.-P.; Hefter, H.; Methner, A. Retinal neurodegeneration in Wilson’s disease revealed by spectral domain optical coherence tomography. PLoS ONE 2012, 7, e49825. [Google Scholar] [CrossRef]
- Stricker, S.; Oberwahrenbrock, T.; Zimmermann, H.; Schroeter, J.; Endres, M.; Brandt, A.U.; Paul, F. Temporal Retinal Nerve Fiber Loss in Patients with Spinocerebellar Ataxia Type 1. PLoS ONE 2011, 6, e23024. [Google Scholar] [CrossRef]
- Chen, J.J. Optical coherence tomography and Neuro-ophthalmology. J. Neuroophthalmol. 2018, 38, e5–e8. [Google Scholar] [CrossRef]
- Dağ, E.; Örnek, N.; Örnek, K.; Erbahçeci-Timur, I.E. Optical Coherence Tomography and Visual Field Findings in Patients With Friedreich Ataxia. J. Neuro Ophthalmol. 2014, 34, 118–121. [Google Scholar] [CrossRef]
- La Morgia, C.; Barboni, P.; Rizzo, G.; Carbonelli, M.; Savini, G.; Scaglione, C.; Capellari, S.; Bonazza, S.; Giannoccaro, M.P.; Calandra-Buonaura, G.; et al. Loss of temporal retinal nerve fibers in Parkinson disease: A mitochondrial pattern? Eur. J. Neurol. 2013, 20, 198–201. [Google Scholar] [CrossRef]
- Albrecht, P.; Müller, A.-K.; Südmeyer, M.; Ferrea, S.; Ringelstein, M.; Cohn, E.; Aktas, O.; Dietlein, T.; Lappas, A.; Foerster, A.; et al. Optical coherence tomography in parkinsonian syndromes. PLoS ONE 2012, 7, e34891. [Google Scholar] [CrossRef]
- Walpert, M.; Normando, E.M.; Cordeiro, M.F.; Holland, A. Retinal structure in Down’s syndrome; potential markers of Alzheimer’s disease. Acta Ophthalmol. 2016, 94. [Google Scholar] [CrossRef]
- Kesler, A.; Vakhapova, V.; Korczyn, A.D.; Naftaliev, E.; Neudorfer, M. Retinal thickness in patients with mild cognitive impairment and Alzheimer’s disease. Clin. Neurol. Neurosurg. 2011, 113, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Salobrar-Garcia, E.; Hoyas, I.; Leal, M.; de Hoz, R.; Rojas, B.; Ramirez, A.I.; Salazar, J.J.; Yubero, R.; Gil, P.; Triviño, A.; et al. Analysis of retinal peripapillary segmentation in early Alzheimer’s disease patients. Biomed. Res. Int. 2015, 2015, 636548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Martin, E.S.; Rojas, B.; Ramirez, A.I.; de Hoz, R.; Salazar, J.J.; Yubero, R.; Gil, P.; Triviño, A.; Ramirez, J.M. Macular thickness as a potential biomarker of mild Alzheimer’s disease. Ophthalmology 2014, 121, 1149–1151. [Google Scholar] [CrossRef] [Green Version]
- Pfueller, C.F.; Brandt, A.U.; Schubert, F.; Bock, M.; Walaszek, B.; Waiczies, H.; Schwenteck, T.; Dörr, J.; Bellmann-Strobl, J.; Mohr, C.; et al. Metabolic changes in the visual cortex are linked to retinal nerve fiber layer thinning in multiple sclerosis. PLoS ONE 2011, 6, e18019. [Google Scholar] [CrossRef]
- Bock, M.; Paul, F.; Dörr, J. Diagnostik und Verlaufsbeurteilung der Multiplen Sklerose [Diagnosis and monitoring of multiple sclerosis: The value of optical coherence tomography]. Nervenarzt 2013, 84, 483–492. [Google Scholar] [CrossRef]
- Dörr, J.; Wernecke, K.D.; Bock, M.; Gaede, G.; Wuerfel, J.T.; Pfueller, C.F.; Bellmann-Strobl, J.; Freing, A.; Brandt, A.U.; Friedemann, P. Association of retinal and macular damage with brain atrophy in multiple sclerosis. PLoS ONE 2011, 6, e18132. [Google Scholar] [CrossRef] [Green Version]
- Gordon-Lipkin, E.; Chodkowski, B.; Reich, D.S.; Smith, S.A.; Pulicken, M.; Balcer, L.J.; Frohman, E.M.; Cutter, G.; Calabresi, P.A. Retinal nerve fiber layer is associated with brain atrophy in multiple sclerosis. Neurology 2007, 69, 1603–1609. [Google Scholar] [CrossRef]
- Siger, M.; Dziegielewski, K.; Jasek, L.; Bieniek, M.; Nicpan, A.; Nawrocki, J.; Selmaj, K. Optical coherence tomography in multiple sclerosis: Thickness of the retinal nerve fiber layer as a potential measure of axonal loss and brain atrophy. J. Neurol. 2008, 255, 1555–1560. [Google Scholar] [CrossRef]
- Ringelstein, M.; Albrecht, P.; Südmeyer, M.; Harmel, J.; Müller, A.K.; Keser, N.; Finis, D.; Ferrea, S.; Guthoff, R.; Schnitzler, A.; et al. Subtle retinal pathology in amyotrophic lateral sclerosis. Ann. Clin. Transl. Neurol. 2014, 1, 290–297. [Google Scholar] [CrossRef]
- Hübers, A.; Müller, H.P.; Dreyhaupt, J.; Böhm, K.; Lauda, F.; Tumani, H.; Kassubek, J.; Ludolph, A.C.; Pinkhardt, E.H. Retinal involvement in amyotrophic lateral sclerosis: A study with optical coherence tomography and diffusion tensor imaging. J. Neural Transm. 2016, 123, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Volpe, N.J.; Simonett, J.; Fawzi, A.A.; Siddique, T. Opthalmic manifestations of amyotrophic lateral sclerosis (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2015, 113, 1–15. [Google Scholar]
- Simonett, J.M.; Huang, R.; Siddique, N.; Farsiu, S.; Siddique, T.; Volpe, N.J.; Fawzi, A.A. Macular sub-layer thinning and association with pulmonary function tests in Amyotrophic Lateral Sclerosis. Sci. Rep. 2016, 6, 29187. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, N.; McBurney-Lin, S.; Kuo, A.; Bedlack, R.; Tseng, H. Retinal thinning in amyotrophic lateral sclerosis patients without ophthalmic disease. PLoS ONE 2017, 12, e0185242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohani, M.; Meysamie, A.; Zamani, B.; Sowlat, M.M.; Akhoundi, F.H. Reduced retinal nerve fiber layer (RNFL) thickness in ALS patients: A window to disease progression. J. Neurol. 2018, 265, 1557–1562. [Google Scholar] [CrossRef]
- Brooks, B.R.; Miller, R.G.; Swash, M.; Munsat, T.L. El Escorial revisited: Revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2000, 1, 293–299. [Google Scholar] [CrossRef]
- Grading diabetic retinopathy from stereoscopic color fundus photographs—An extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 1991, 98, 786–806. [CrossRef]
- Hee, M.R.; Puliafito, C.A.; Duker, J.S.; Reichel, E.; Coker, J.G.; Wilkins, J.R.; Schuman, J.S.; Swanson, E.A.; Fujimoto, J.G. Topography of diabetic macular edema with optical coherence tomography. Ophthalmology 1998, 105, 360–370. [Google Scholar] [CrossRef] [Green Version]
- Tsironi, E.E.; Dastiridou, A.; Katsanos, A.; Dardiotis, E.; Veliki, S.; Patramani, G.; Zacharaki, F.; Ralli, S.; Hadjigeorgiou, G.M. Perimetric and retinal nerve fiber layer findings in patients with Parkinson’s disease. BMC Ophthalmol. 2012, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Ferreras, A.; Pablo, L.E.; Pajarín, A.B.; Larrosa, J.M.; Polo, V.; Honrubia, F.M. Logistic regression analysis for early glaucoma diagnosis using optical coherence tomography. Arch. Ophthalmol. 2008, 126, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Meier, S.L.; Charleston, A.J.; Tippett, L.J. Cognitive and behavioural deficits associated with the orbitomedial prefrontal cortex in amyotrophic lateral sclerosis. Brain 2010, 133, 3444–3457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fawzi, A.A.; Simonett, J.M.; Purta, P.; Moss, H.E.; Lowry, J.L.; Deng, H.-X.; Siddique, N.; Sufit, R.; Bigio, E.H.; Volpe, N.J.; et al. Clinicopathologic report of ocular involvement in ALS patients with C9orf72 mutation. Amyotroph. Lateral Scler. Frontotemporal Degener. 2014, 15, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Steele, J.C.; Wresch, R.; Hanlon, S.D.; Keystone, J.; Ben-Shlomo, Y. A unique retinal epitheliopathy is associated with amyotrophic lateral sclerosis/Parkinsonism-Dementia complex of Guam. Mov. Disord. 2015, 30, 1271–1275. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, M.; Menke, R.A.L.; Sharma, R.; Berna, C.M.; Hicks, S.L.; Kennard, C.; Talbot, K.; Turner, M.R. Eye-tracking in amyotrophic lateral sclerosis: A longitudinal study of saccadic and cognitive tasks. Amyotroph. Lateral Scler. Front. Degener. 2016, 17, 101–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas Lozano, M.P.; Salobrar-García, E.; Salazar, J.J.; Ramírez, A.; Urcelay Segura, J.L.; Muñoz Blanco, J.L.; Ramírez, J.M. Optical coherence tomography in patients with amyotrophic lateral sclerosis. Acta Ophthalmol. 2016, 94. [Google Scholar] [CrossRef]
- Cooper-Knock, J.; Green, C.; Altschuler, G.; Wei, W.; Bury, J.J.; Heath, P.R.; Wyles, M.; Gelsthorpe, C.; Highley, J.R.; Lorente-Pons, A.; et al. A data-driven approach links microglia to pathology and prognosis in amyotrophic lateral sclerosis. Acta Neuropathol. Commun. 2017, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, A.I.; de Hoz, R.; Salobrar-Garcia, E.; Salazar, J.J.; Rojas, B.; Ajoy, D.; López-Cuenca, I.; Rojas, P.; Triviño, A.; Ramírez, J.M. The role of microglia in retinal neurodegeneration: Alzheimer’s disease, Parkinson, and glaucoma. Front. Aging Neurosci. 2017, 9, 214. [Google Scholar] [CrossRef] [Green Version]
- Geloso, M.C.; Corvino, V.; Marchese, E.; Serrano, A.; Michetti, F.; D’Ambrosi, N. The dual role of microglia in ALS: Mechanisms and therapeutic approaches. Front. Aging Neurosci. 2017, 9, 242. [Google Scholar] [CrossRef] [Green Version]
- Brettschneider, J.; Toledo, J.B.; van Deerlin, V.M.; Elman, L.; McCluskey, L.; Lee, V.M.Y.; Trojanowski, J.Q. Microglial activation correlates with disease progression and upper motor neuron clinical symptoms in amyotrophic lateral sclerosis. PLoS ONE 2012, 7, e39216. [Google Scholar] [CrossRef] [Green Version]
- Brites, D.; Vaz, A.R. Microglia centered pathogenesis in ALS: Insights in cell interconnectivity. Front. Cell. Neurosci. 2014, 8, 1–24. [Google Scholar] [CrossRef]
- Ringer, C.; Weihe, E.; Schütz, B. SOD1 G93A Mutant Mice Develop a Neuroinflammation-Independent Dendropathy in Excitatory Neuronal Subsets of the Olfactory Bulb and Retina. J Neuropathol Exp Neurol 2017, 76, 769–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, K.; Yoon, D.; Yu, M.; Peachey, N.S.; Ferreira, P.A. Microglial activation in an amyotrophic lateral sclerosis-like model caused by Ranbp2 loss and nucleocytoplasmic transport impairment in retinal ganglion neurons. Cell. Mol. Life Sci. 2019, 76, 3407–3432. [Google Scholar] [CrossRef] [PubMed]
- Ikenaka, K.; Katsuno, M.; Kawai, K.; Ishigaki, S.; Tanaka, F.; Sobue, G. Disruption of Axonal Transport in Motor Neuron Diseases. Int. J. Mol. Sci 2012, 13, 1225–1238. [Google Scholar] [CrossRef] [PubMed]
- De Vos, K.J.; Hafezparast, M. Neurobiology of axonal transport defects in motor neuron diseases: Opportunities for translational research? Neurobiol. Dis. 2017, 105, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Devine, M.S.; Kiernan, M.C.; Heggie, S.; McCombe, P.A.; Henderson, R.D. Study of motor asymmetry in ALS indicates an effect of limb dominance on onset and spread of weakness, and an important role for upper motor neurons. Amyotroph. Lateral Scler. Front. Degener. 2014, 15, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Fiori, F.; Sedda, A.; Ferrè, E.R.; Toraldo, A.; Querzola, M.; Pasotti, F.; Ovadia, D.; Piroddi, C.; Dell’aquila, R.; Lunetta, C.; et al. Exploring motor and visual imagery in Amyotrophic Lateral Sclerosis. Exp. Brain Res. 2013, 226, 537–547, Erratum in 2016, 234, 1783–1783. [Google Scholar] [CrossRef]
- D’Ambrosio, A.; Gallo, A.; Trojsi, F.; Corbo, D.; Esposito, F.; Cirillo, M.; Monsurrò, M.R.; Tedeschi, G. Frontotemporal cortical thinning in amyotrophic lateral sclerosis. AJNR. Am. J. Neuroradiol. 2014, 35, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Mao, C.; Jin, J.; Niu, C.; Bai, L.; Dang, J.; Zhang, M. Side of limb-onset predicts laterality of gray matter loss in amyotrophic lateral sclerosis. Biomed Res. Int. 2014, 2014, 473250. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | ALS | p-Value | Spearman Correlation ALSFRS-R | p-Value Spearman Correlation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Control Baseline vs. Control Follow-Up | Control Baseline vs. ALS Baseline | Control Follow-Ip vs. ALS Follow-Up | ALS Baseline vs. ALS Follow-Up | |||
| n = 38 | n = 38 | n = 20 | n = 10 | |||||||
| Gender (Male/Female) | 9/10 | 7/1 | 12/8 | 4/6 | ||||||
| Mean ± SD | ||||||||||
| BCVA ** | 0.98 ± 0.06 | 0.98 ± 0.04 | 0.90 ± 0.16 | 0.91 ± 0.13 | 0.487 | 0.230 | 0.146 | 0.354 | 0.317 | 0.173 |
| AGE | 44.74 ± 11.81 | 45.54 ± 12.47 | 51.10 ± 9.89 | 51.30 ±10.02 | 1.000 | 0.044 | 0.250 | 0.157 | (−0.156) | 0.338 |
| IOP ** | 15.08 ± 2.22 | 15.31 ± 1.89 | 15.75 ± 1.99 | 15.20 ± 1.48 | 0.146 | 0.365 | 0.979 | 0.564 | (−0.407) | 0.075 |
| ALSFRS-R ** | 48.00 ± 0.00 | 48.00 ± 0.00 | 29.50 ± 14.89 | 35.6 ± 14.08 | 1.000 | <0.001 | <0.001 | 0.068 | ------ | ------ |
| VFI ** | 98.63 ± 1.55 | 99.13 ± 1.09 | 95.00 ± 8.51 | 94.63 ± 10.08 | 0.138 | 0.388 | 0.084 | 0.999 | (−0.047) | 0.852 |
| MD ** | (−0.76) ± 1.68 | (−0.05) ± 1.09 | (−1.77) ± 3.74 | (−2.66) ± 4.71 | 0.161 | 0.902 | 0.086 | 0.148 | 0.0854 | 0.736 |
| PSD ** | 1.76 ± 0.75 | 1.68 ± 0.62 | 2.68 ± 2.20 | 2.87 ± 2.96 | 0.877 | 0.297 | 0.257 | 0.896 | (−0.058) | 0.818 |
| % FL ** | 22.87 ± 28.99 | 28.23 ± 31.92 | 28.12 ± 35.06 | 10.21 ± 12.56 | 0.615 | 0.679 | 0.150 | 0.037 | (−0.052) | 0.839 |
| % FN ** | 1.45 ± 2.80 | 2.19 ± 3.04 | 3.06 ± 4.02 | 3.5 ± 3.29 | 0.143 | 0.407 | 0.315 | 0.609 | (0.152) | 0.546 |
| % FP ** | 2.68 ± 3.50 | 3.25 ± 4.07 | 3.44 ± 4.19 | 1.5 ± 2.27 | 0.850 | 0.643 | 0.287 | 0.165 | (−0.131) | 0.605 |
| Control | ALS | p-Value | Spearman Correlation ALSFRS-R | p-Value Spearman Correlation | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Control Baseline vs. Control Follow-Up | Control Baseline vs. ALS Baseline | Control Follow-Up vs. ALS Follow-up | ALS Baseline vs. ALS Follow-Up | ||||
| Macular Analysis (µm) | n = 38 | n = 38 | n = 20 | n = 10 | |||||||
| Mean ± SD | |||||||||||
| Fovea o CMT | 261.42 ± 21.31 | 255.81 ± 23.61 | 262.10 ± 26.29 | 274.90 ± 25.32 | 0.244 | 1.000 | 0.567 | 0.335 | 0.275 | 0.241 | |
| IMR | Superior | 320.55 ± 12.30 | 315.31 ± 12.06 | 327.55 ± 15.31 | 322.20 ± 12.63 | 0.526 | 0.435 | 1.000 | 0.166 | 0.077 | 0.746 |
| Temporal | 307.32 ± 12.49 | 303.06 ± 14.21 | 315.85 ± 15.34 | 313.40 ± 13.38 | 0.705 | 0.049 | 1.000 | 0.160 | 0.079 | 0.741 | |
| Nasal | 323.40 ± 13.99 | 319.13 ± 15.15 | 330.35 ± 16.00 | 327.40 ± 10.93 | 0.794 | 0.510 | 1.000 | 0.397 | 0.159 | 0.502 | |
| Inferior | 319.00 ± 12.54 | 314.88 ± 14.58 | 326.91 ± 15.34 | 320.00 ± 11.88 | 0.660 | 0.029 | 1.000 | 0.002 | 0.000 | 0.852 | |
| OMR | Superior | 280.30 ± 10.95 | 279.06 ± 11.38 | 279.65 ± 14.39 | 271.00 ± 14.73 | 0.444 | 1.000 | 0.418 | 0.161 | (−0.121) | 0.613 |
| Temporal | 260.05 ± 10.04 | 256.63 ± 6.42 | 264.58 ± 13.90 | 261.20 ± 12.54 | 0.937 | 0.912 | 0.872 | 0.327 | (−0.160) | 0.498 | |
| Nasal | 298.97 ± 13.46 | 295.38 ± 14.39 | 297.49 ± 24.05 | 292.20 ± 17.51 | 0.649 | 1.000 | 1.000 | 0.652 | 0.057 | 0.812 | |
| Inferior ** | 269.74 ± 12.84 | 269.31 ± 9.44 | 274.42 ± 14.20 | 264.40 ± 16.34 | 0.183 | 0.819 | 1.000 | 0.031 | (−0.230) | 0.329 | |
| Cube Volume | 10.08 ± 0.41 | 10.04 ± 0.29 | 10.14 ± 0.49 | 10.00 ± 0.41 | 0.309 | 1.000 | 0.292 | 0.120 | (−0.104) | 0.661 | |
| Cube average thickness | 279.58 ± 11.23 | 279.06 ± 7.83 | 281.70 ± 13.79 | 277.70 ± 11.70 | 0.188 | 1.000 | 0.181 | 0.135 | (−0.100) | 0.674 | |
| GCC Analysis (µm) | Control | ALS | p-Value | Spearman Correlation ALSFRS-R | p-Value Spearman Correlation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Control Baseline vs. Control Follow-Up | Control Baseline vs. ALS Baseline | Control Follow-Up vs. ALS Follow-Up | ALS Baseline vs. ALS Follow-Up | ||||
| n = 38 | n = 38 | n = 20 | n = 10 | ||||||||
| Mean ± SD | |||||||||||
| Superior | Central ** | 81.63 ± 6.18 | 80.88 ± 7.62 | 78.70 ± 13.12 | 76.10 ± 10.04 | 0.999 | 1.000 | 1.000 | 0.805 | (−0.179) | 0.450 |
| Temporal ** | 79.08 ± 8.09 | 78.94 ± 4.92 | 77.80 ± 9.36 | 76.00 ± 10.03 | 0.588 | 1.000 | 1.000 | 0.601 | 0.020 | 0.934 | |
| Nasal | 82.68 ± 6.98 | 82.13 ± 5.81 | 80.10 ± 10.80 | 77.50 ± 9.99 | 0.458 | 1.000 | 1.000 | 0.957 | 0.103 | 0.667 | |
| Inferior | Central | 80.53 ± 6.90 | 80.75 ± 4.67 | 80.35 ± 9.69 | 73.70 ± 12.15 | 0.989 | 1.000 | 0.407 | 0.070 | (−0.237) | 0.314 |
| Temporal | 81.40 ± 5.53 | 80.25 ± 4.68 | 81.00 ± 10.05 | 77.30 ± 9.81 | 0.327 | 1.000 | 1.000 | 0.212 | (−0.196) | 0.407 | |
| Nasal | 81.32 ± 7.65 | 80.50 ± 4.90 | 77.20 ± 11.28 | 75.20 ± 12.21 | 0.873 | 1.000 | 0.872 | 0.284 | 0.085 | 0.721 | |
| GCL (µm) thickness | Average | 81.18 ± 6.20 | 80.56 ± 5.20 | 79.15 ± 9.50 | 76.00 ± 10.30 | 0.592 | 1.000 | 1.000 | 0.336 | (−0.011) | 0.962 |
| Minimum ** | 78.90 ± 6.13 | 78.06 ± 5.70 | 72.70 ± 15.04 | 74.00 ± 11.74 | 0.184 | 1.000 | 1.000 | 0.347 | 0.389 | 0.090 | |
| Peripapillary Analysis (µm) | Control | ALS | p-Value | Spearman Correlation ALSFRS-R | p-Value Spearman Correlation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Control Baseline vs. Control Follow-Up | Control Baseline vs. ALS Baseline | Control Follow-Up vs. ALS Follow-Up | ALS Baseline vs. ALS Follow-Up | ||||
| n = 38 | n = 38 | n = 20 | n = 10 | ||||||||
| Mean ± SD | |||||||||||
| Average RNFL Thickness | 94.84 ± 12.88 | 95.69 ± 13.82 | 88.00 ± 2.60 | 79.90 ± 13.75 | 0.572 | 0.659 | 1.000 | 0.073 | (−0.334) | 0.150 | |
| Peripapillary RNFL Quadrants (µm) | Superior | 112.90 ± 18.33 | 117.38 ± 21.54 | 104.80 ± 23.80 | 93.50 ± 24.38 | 0.578 | 0.921 | 0.093 | 0.049 | (−0.140) | 0.555 |
| Temporal | 64.95 ± 10.09 | 65.88 ± 7.21 | 64.35 ± 12.64 | 63.50 ± 15.81 | 0.935 | 1.000 | 0.742 | 0.100 | 0.362 | 0.117 | |
| Inferior | 130.85 ± 22.27 | 129.75 ± 24.70 | 116.65 ± 25.08 | 101.20 ± 26.62 | 0.074 | 0.447 | 1.000 | 0.001 | (−0.527) | 0.017 | |
| Nasal | 71.55 ± 14.87 | 69.94 ± 12.92 | 68.75 ± 17.42 | 61.30 ± 12.29 | 0.986 | 1.000 | 0.659 | 0.060 | (−0.062) | 0.795 | |
| Peripapillary RNFL Sectors (µm) | H1 RE/H11 LE | 100.87 ± 20.30 | 100.94 ± 26.74 | 90.40 ± 22.74 | 84.30 ± 29.35 | 0.070 | 0.567 | 1.000 | 0.781 | (−0.056) | 0.814 |
| H2 RE/H10 LE | 90.11 ± 25.28 | 92.63 ± 25.95 | 79.65 ± 23.86 | 75.10 ± 21.01 | 0.864 | 0.645 | 0.962 | 0.157 | 0.117 | 0.624 | |
| H3 RE/H9 LE | 56.76 ± 10.91 | 55.75 ± 6.59 | 60.30 ± 13.82 | 51.90 ± 10.40 | 0.452 | 1.000 | 0.330 | 0.034 | (−0.318) | 0.172 | |
| H4 RE/H8 LE | 63.82 ± 13.33 | 61.75 ± 10.99 | 65.55 ± 20.61 | 56.90 ± 12.88 | 0.566 | 1.000 | 1.000 | 0.320 | (−0.019) | 0.937 | |
| H5 RE/H7 LE | 111.37 ± 30.21 | 110.38 ± 22.80 | 102.40 ± 35.00 | 80.30 ± 17.93 | 0.635 | 1.000 | 0.126 | 0.038 | (−0.647) | 0.002 | |
| H6 OU | 148.16 ± 32.02 | 149.19 ± 30.94 | 122.75 ± 37.06 | 99.00 ± 31.24 | 0.091 | 0.109 | 0.510 | <0.001 | (−0.521) | 0.018 | |
| H7 RE/H5 LE | 133.42 ± 26.05 | 129.50 ± 34.27 | 124.50 ± 30.54 | 123.50 ± 36.77 | 0.282 | 1.000 | 1.000 | 0.624 | 0.101 | 0.673 | |
| H8 RE/H4 LE | 65.13 ± 12.86 | 65.13 ± 11.04 | 67.35 ± 18.23 | 69.00 ± 18.74 | 0.837 | 1.000 | 1.000 | 0.024 | 0.488 | 0.029 | |
| H9 RE/H3 LE | 51.18 ± 8.79 | 53.38 ± 8.80 | 50.45 ± 9.59 | 47.50 ± 10.47 | 0.369 | 1.000 | 0.366 | 0.286 | (−0.009) | 0.970 | |
| H10 RE/H2 LE | 78.45 ± 16.84 | 79.19 ± 17.05 | 75.20 ± 16.95 | 74.00 ± 21.39 | 0.450 | 1.000 | 1.000 | 0.538 | 0.029 | 0.904 | |
| H11 RE/H1 LE | 129.92 ± 33.30 | 125.50 ± 48.73 | 117.25 ± 25.27 | 114.70 ± 29.59 | 0.307 | 0.629 | 0.924 | 0.747 | (−0.098) | 0.680 | |
| H12 OU | 108.63 ± 23.70 | 119.13 ± 20.47 | 101.50 ± 31.37 | 81.20 ± 26.15 | 0.350 | 1.000 | 0.060 | 0.013 | (−0.335) | 0.149 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas, P.; de Hoz, R.; Ramírez, A.I.; Ferreras, A.; Salobrar-Garcia, E.; Muñoz-Blanco, J.L.; Urcelay-Segura, J.L.; Salazar, J.J.; Ramírez, J.M. Changes in Retinal OCT and Their Correlations with Neurological Disability in Early ALS Patients, a Follow-Up Study. Brain Sci. 2019, 9, 337. https://doi.org/10.3390/brainsci9120337
Rojas P, de Hoz R, Ramírez AI, Ferreras A, Salobrar-Garcia E, Muñoz-Blanco JL, Urcelay-Segura JL, Salazar JJ, Ramírez JM. Changes in Retinal OCT and Their Correlations with Neurological Disability in Early ALS Patients, a Follow-Up Study. Brain Sciences. 2019; 9(12):337. https://doi.org/10.3390/brainsci9120337
Chicago/Turabian StyleRojas, Pilar, Rosa de Hoz, Ana I. Ramírez, Antonio Ferreras, Elena Salobrar-Garcia, José L. Muñoz-Blanco, José L. Urcelay-Segura, Juan J. Salazar, and José M. Ramírez. 2019. "Changes in Retinal OCT and Their Correlations with Neurological Disability in Early ALS Patients, a Follow-Up Study" Brain Sciences 9, no. 12: 337. https://doi.org/10.3390/brainsci9120337
APA StyleRojas, P., de Hoz, R., Ramírez, A. I., Ferreras, A., Salobrar-Garcia, E., Muñoz-Blanco, J. L., Urcelay-Segura, J. L., Salazar, J. J., & Ramírez, J. M. (2019). Changes in Retinal OCT and Their Correlations with Neurological Disability in Early ALS Patients, a Follow-Up Study. Brain Sciences, 9(12), 337. https://doi.org/10.3390/brainsci9120337