Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. MRI Acquisition
2.2.1. Preparation for Non-Sedated MRI
2.2.2. MRI Sequences
2.3. Qualitative MRI Analysis
2.4. Quantitative MRI Analysis
2.4.1. T2-Weighted Brain MRI Tissue Segmentation
- Preprocessing: (i) Intracranial space segmentation: T2 images were skull-stripped using the unvalidated ‘Simple Watershed Scalping’ module in the MANTiS toolbox, followed by manual editing in FSLview; (ii) Bias field correction was performed using FMRIB’s Automated Segmentation Tool (FAST) [34]; (iii) Setting the image origin employed the ‘Origin to the Center of Mass’ module in the MANTiS toolbox;
- MANTiS Segmentation: Preprocessed images underwent MANTiS segmentation pipeline [33]. Automated CSF segmentations were visually inspected and subsequently edited to correct for any tissue misclassifications as described below;
- Post-Segmentation Editing: Automated CSF segmentations were (i) masked to zero voxels outside of intracranial space, (ii) thresholded at 40% to eliminate voxels with <40% probability of representing CSF, and (iii) converted to binary masks. Additional complex editing was undertaken due to the frequent exclusion of CSF spaces and inclusion of brain tissue. Specifically, the partial volume estimate map of CSF generated by FAST [34] was (i) thresholded at 50% to eliminate voxels with <50% of their volume comprising CSF, (ii) converted to a binary mask, and (iii) combined with subject’s thresholded/binarized MANTiS CSF mask for each case. Consequently, FAST’s CSF map effectively filled in spaces missing in MANTiS’ CSF segmentation (e.g., cisterns, 4th ventricle, and sulcal spaces), resulting in a ‘comprehensive’ CSF image. Additional minor manual editing was performed to erase misclassified brain tissue. A single individual performed all manual editing to ensure consistent tissue delineation. This final total CSF segmentation was further divided into extra-axial and ventricular spaces by manually erasing ventricular CSF from the total CSF segmentation to produce extra-axial space segmentation.
2.4.2. T1-Weighted Brain MRI Tissue Segmentation
- Whole Brain Segmentation. Semi-automated brain tissue segmentation was achieved as follows: (i) Skull-stripping of T1 images by manually tracing the brain outline (includes ventricles); and (ii) Partial volume segmentation of CSF using FAST [34]. Using tools in FSL, CSF partial volume estimate maps were (a) thresholded at 99% to eliminate voxels with <99% of their volume comprising CSF, (b) converted to binary masks, and (c) subtracted from the masks of brain outline (includes ventricles) in order to generate masks of brain tissue that exclude the ventricles. The latter brain-only masks subsequently underwent additional (d) minor manual editing to draw in any missing brain tissue.
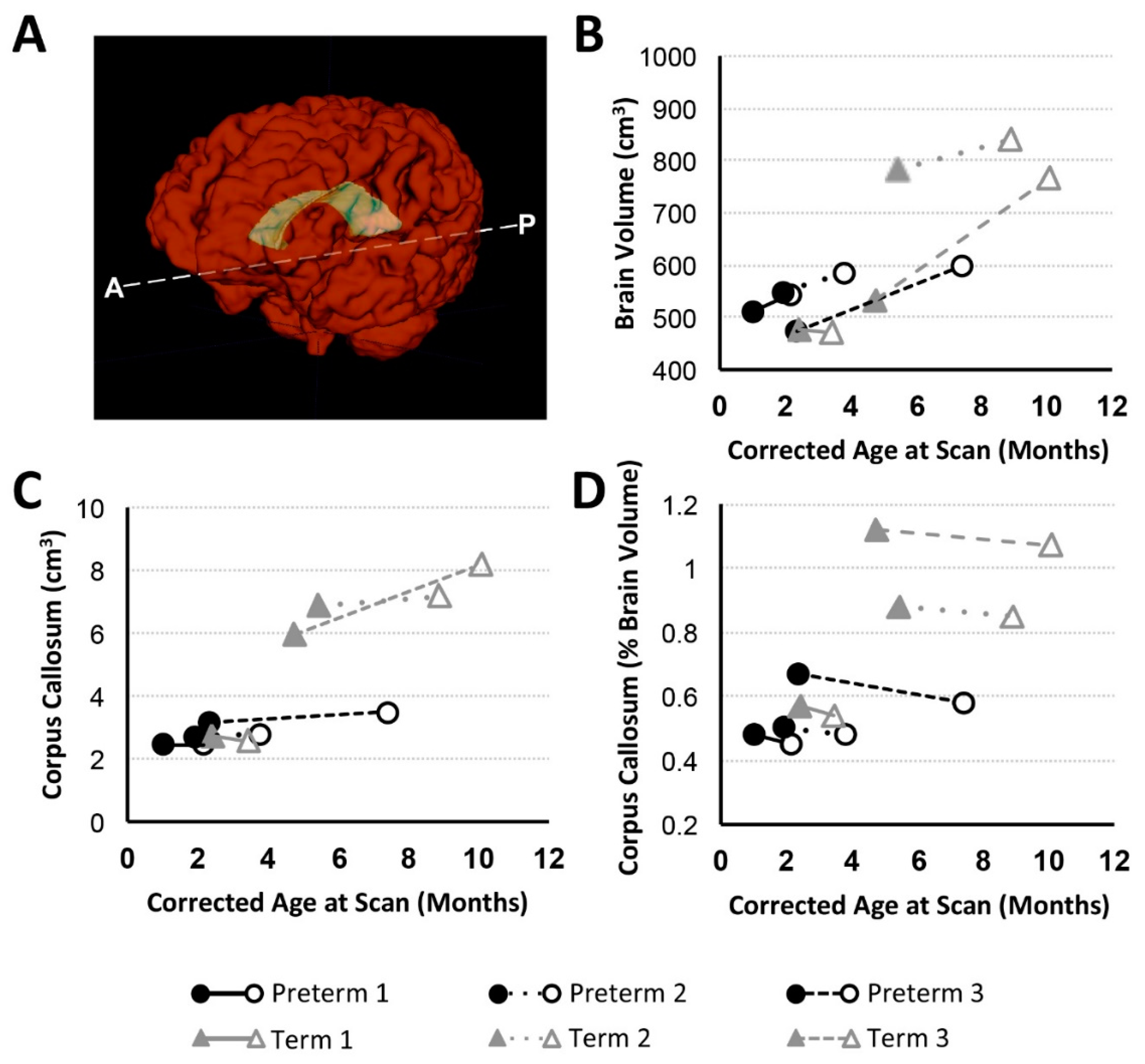
- Manual CC Segmentation. We extended available protocol for CC segmentation by Yu et al. [36], as previously described by our group [32]. Effectively, CC was traced as an arching line from the tips of the lateral ventricles to the in-folding of the cingulate gyrus. We used both a neuroanatomical atlas [37] and a fiber tract-based atlas of human white matter [38] for anatomical referencing to guide total CC segmentation.
2.4.3. MRI Data Volumetry
2.5. Quantification of Pharmacological Treatment
3. Results
3.1. Perioperative Critical Care for LGEA
3.1.1. Pre-Foker Management
3.1.2. Anesthesia Management for the Foker Process.
3.1.3. Complex Critical Care Management
- Postoperative Intubation. Postoperative sedation in combination with immobilization served to preserve the temporary placement of surgical devices, facilitate proper tissue expansion, and allow for safe healing following both Foker I and Foker II thoracotomies. Length of intubation served as a proxy of length of sedation. Combinations of opioids (viz. morphine) and benzodiazepines (viz. midazolam) were used for primary sedation management and were administered as both infusions and intermittent boluses per institutional guidelines [12]. Preterms 1, 2, 3, and Term 1 additionally received fentanyl boluses, and lorazepam was administered to Preterm 2 and Term 1 during this sedation period.
- Weaning from Opioid and Benzodiazepine Sedation. Because each infant received prolonged sedation (≥5 days), which is associated with the development of physical dependence [12,24,25], weaning of sedation was required following extubation. Morphine, midazolam, and lorazepam were used to facilitate this process, though Term 1 did not receive lorazepam and Term 2 did not receive midazolam. Preterm 3 also received oxycodone during weaning. The administration of α-2 adrenergic agonists (clonidine and/or dexmedetomidine), initiated during primary sedation, was continued into the weaning period in all patients except Term 1 and Term 3. Only Preterm 2 did not have complete drug evaluation for sedation weaning, due to transfer to another hospital before completion of treatment.
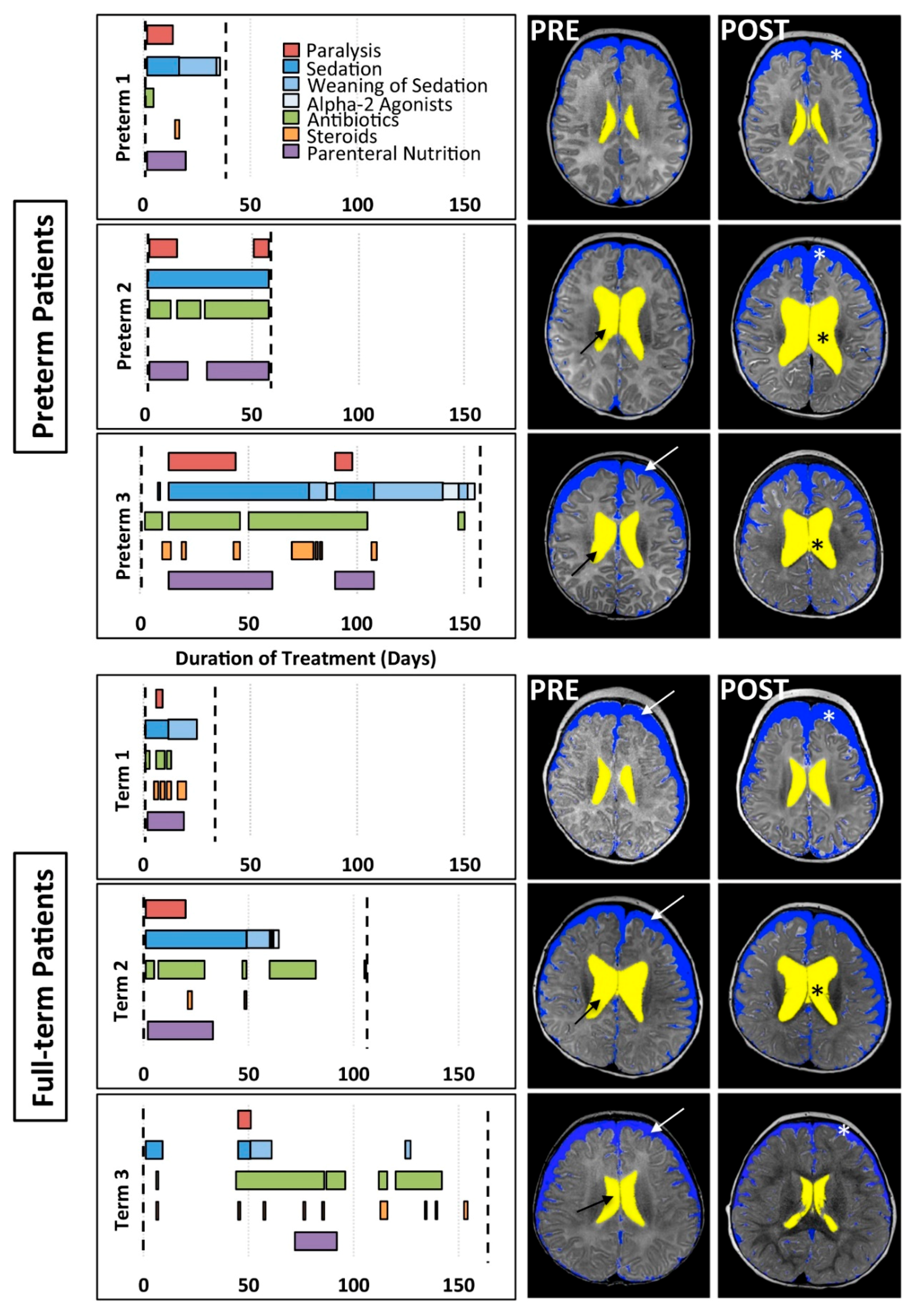
- Other. As graphically illustrated in Figure 1, in addition to muscle relaxants (red bars), sedative medications for intubation (dark blue bars), and weaning of sedation medications (lighter blue bars), a variety of antibiotics were prescribed to each patient to prevent/treat infection throughout the clinical course (green bars). All patients except Preterm 2 also periodically received steroids (orange bars). Due to the nature of the illness, nutritional resources were supplied by parenteral route (purple bars).
3.2. Qualitative Clinical Brain MRI Reports
3.2.1. PRE-Foker Process Brain MRI
3.2.2. POST-Foker Process Brain MRI
3.3. Quantitative Brain MRI Analysis
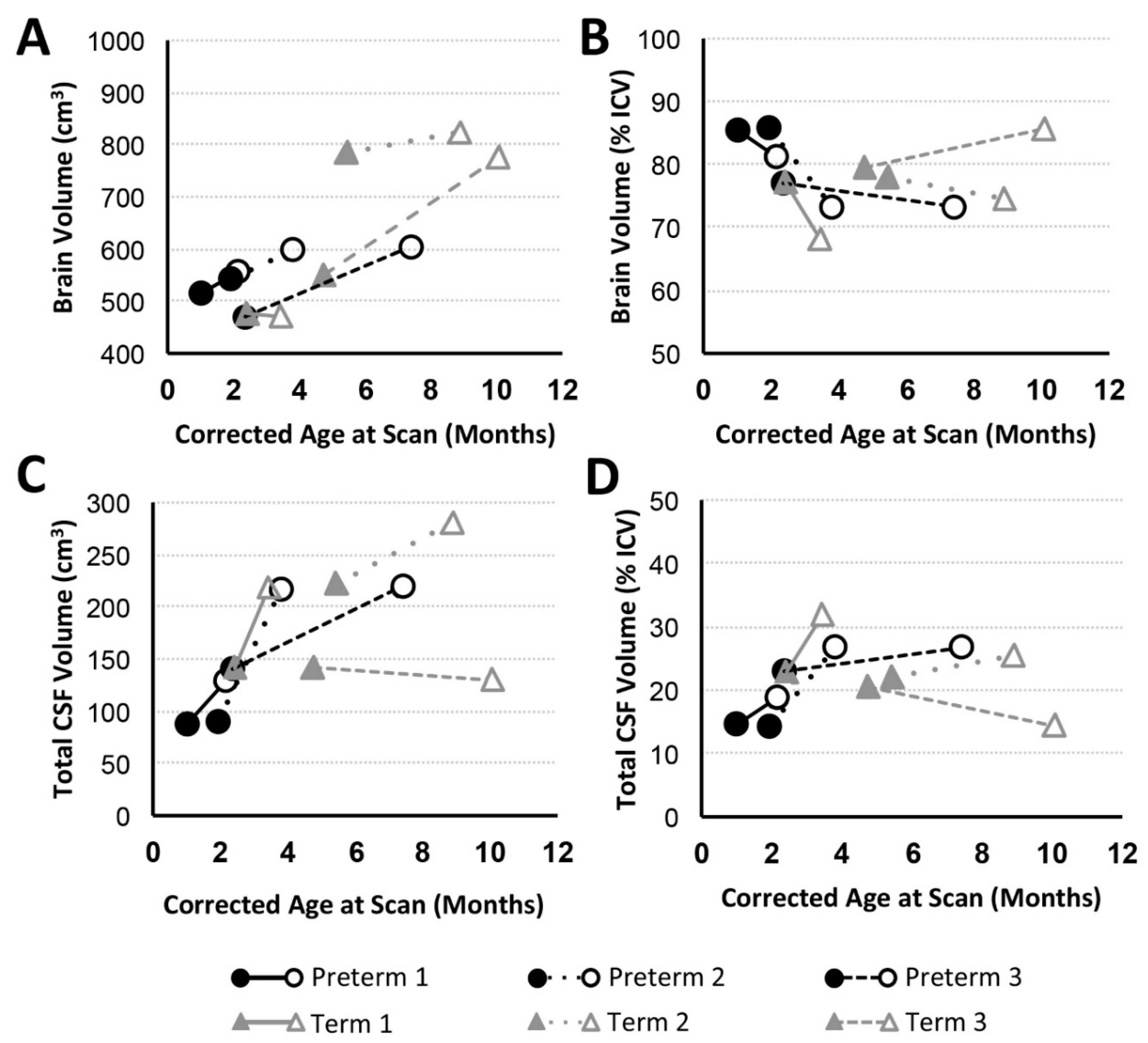
3.3.1. Brain and Total CSF Volume Change
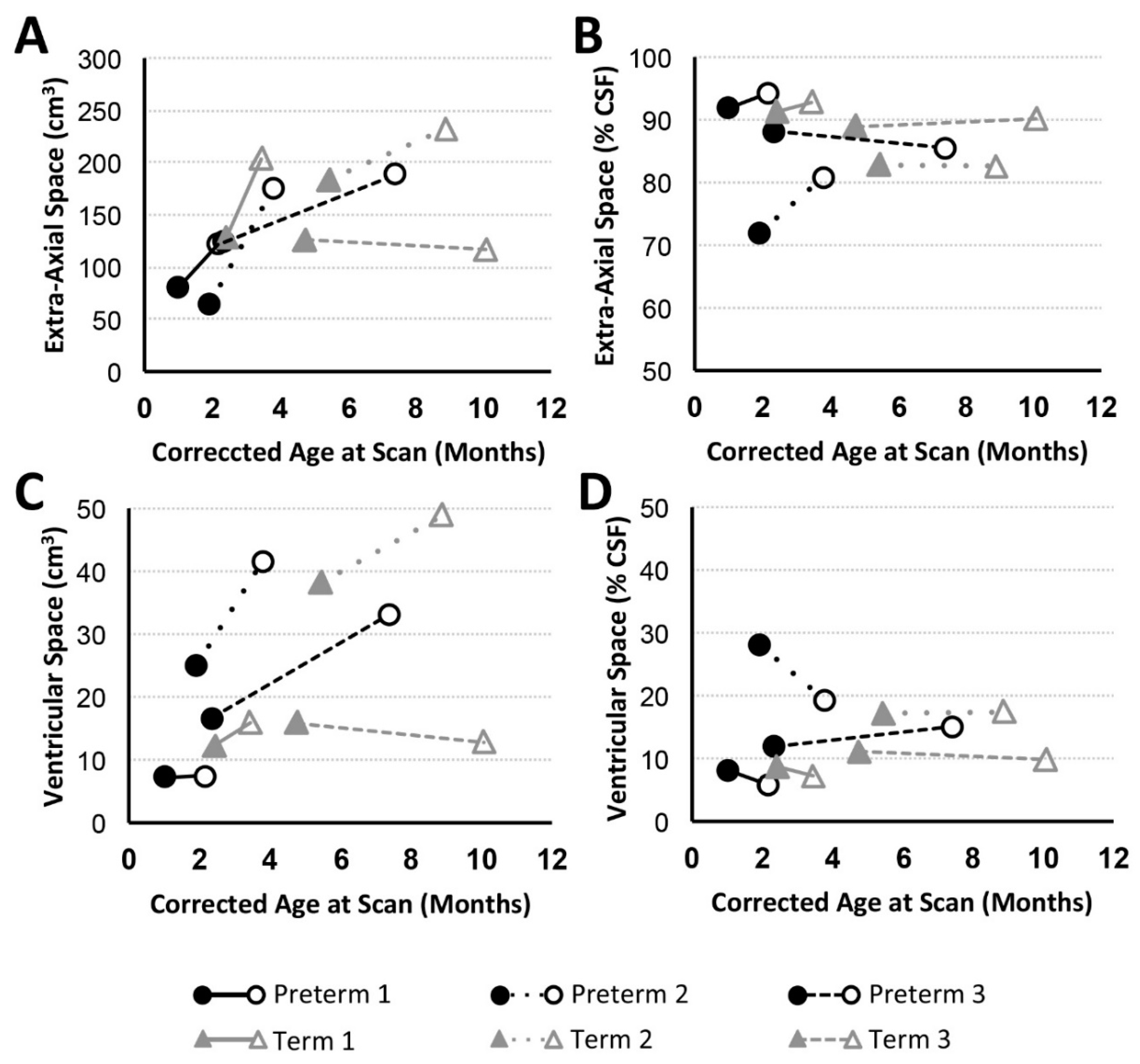
3.3.2. CSF Compartments Volume Change
3.3.3. Corpus Callosum Volume Change
4. Discussion
4.1. PRE-Foker Process Brain MRI Findings in Infants Born with LGEA
4.2. Impact of Complex Perioperative Critical Care for the Foker Process in Infants with LGEA
4.2.1. Qualitative Brain MRI Findings
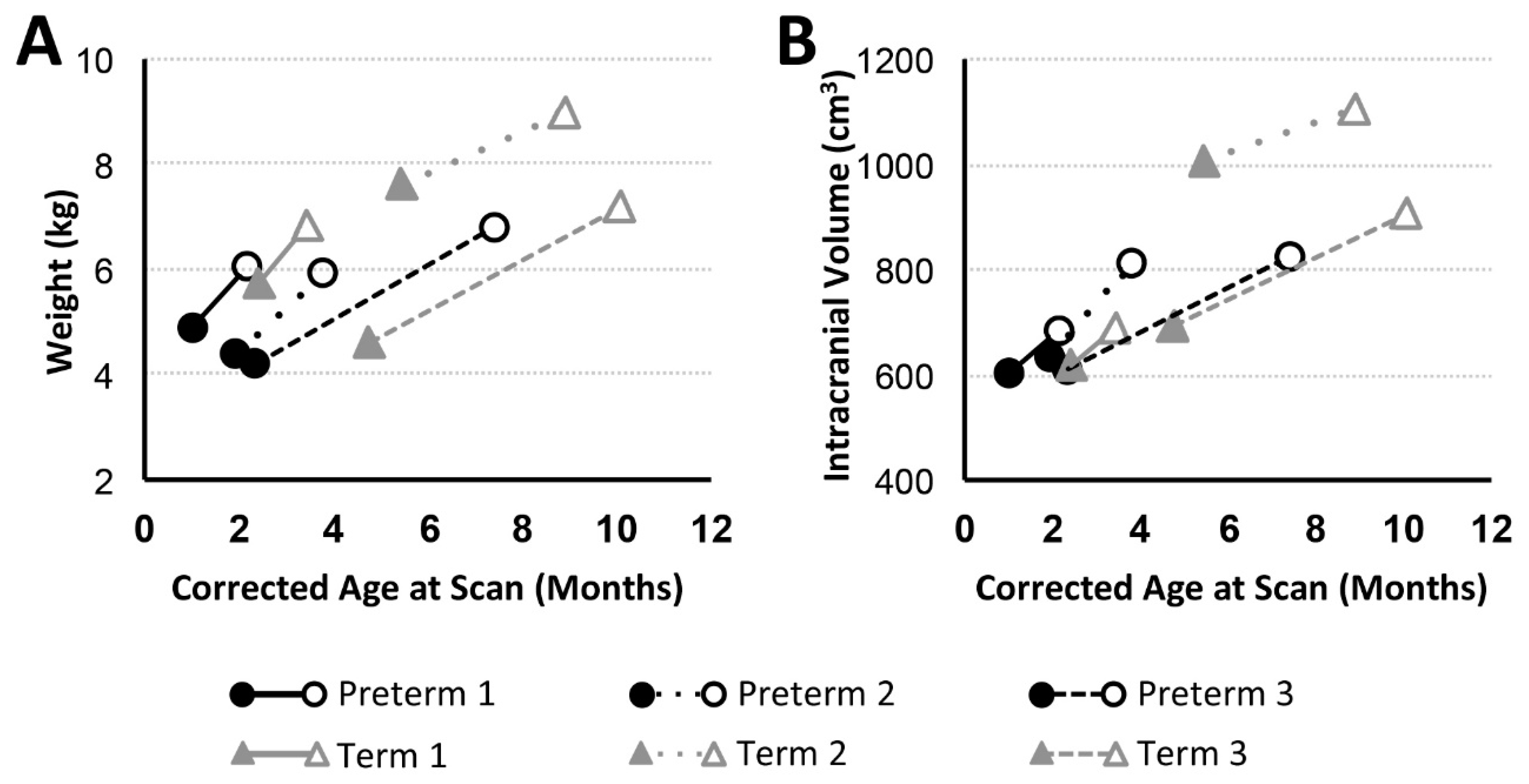
4.2.2. Brain Growth in Infancy
4.2.3. Increased CSF Volume in Infancy
4.2.4. Corpus Callosum Maturation in Infancy
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | atrial septal defect |
| CC | corpus callosum |
| CSF | cerebrospinal fluid |
| CT | computerized tomography |
| EA | esophageal atresia |
| ECMO | extracorporeal membrane oxygenation |
| EGD | esophagoduodenoscopy |
| F | female |
| FAST | FMRIB’s Automated Segmentation Tool |
| FSL | FMRIB Software Library |
| FTT | failure to thrive |
| G-tube | gastrostomy tube |
| GA | gestational age |
| ICV | intracranial volume |
| IUGR | intrauterine growth restriction |
| LGEA | long-gap esophageal atresia |
| M | male |
| MAC | minimum alveolar concentration |
| MANTiS | morphologically adaptive neonatal tissue segmentation |
| MRI | magnetic resonance imaging |
| MSICU | medical-surgical intensive care unit |
| NICU | neonatal intensive care unit |
| PDA | patent ductus arteriosus |
| pHTN | pulmonary hypertension |
| PICC | peripherally inserted central catheter |
| Rx | treatment/therapy |
| SDH | subdural hematoma |
| TEE | transesophageal echocardiography |
| TEF | tracheoesophageal fistula |
| TOF | tetralogy of Fallot |
| TPN | total parenteral nutrition |
| VACTERL | Referring to vertebral, anorectal, cardiac, TEF and/or EA, renal, and limb malformations |
| VSD | ventricular septal defect |
References
- Vohr, B. Long-term outcomes of moderately preterm, late preterm, and early term infants. Clin. Perinatol. 2013, 40, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W.; Anderson, P.J. Adult outcome of extremely preterm infants. Pediatrics 2010, 126, 342–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunau, R.E.; Holsti, L.; Peters, J.W. Long-term consequences of pain in human neonates. Semin. Fetal Neonatal Med. 2006, 11, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.; Barone, S., Jr. Critical periods of vulnerability for the developing nervous system: Evidence from humans and animal models. Environ. Health Perspect. 2000, 108 (Suppl. 3), 511–533. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.L.; Sleeper, L.A.; Volpe, J.J.; Kinney, H.C. Neuropathologic studies of the encephalopathy of prematurity in the late preterm infant. Clin. Perinatol. 2013, 40, 707–722. [Google Scholar] [CrossRef] [PubMed]
- Wernovsky, G.; Licht, D.J. Neurodevelopmental Outcomes in Children With Congenital Heart Disease-What Can We Impact? Pediatr. Crit. Care Med. 2016, 17, S232–S242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolwijk, L.J.; Keunen, K.; de Vries, L.S.; Groenendaal, F.; van der Zee, D.C.; van Herwaarden, M.Y.A.; Lemmers, P.M.A.; Benders, M. Neonatal Surgery for Noncardiac Congenital Anomalies: Neonates at Risk of Brain Injury. J. Pediatr. 2017, 182, 335–341. [Google Scholar] [CrossRef]
- Stolwijk, L.J.; Lemmers, P.M.; Harmsen, M.; Groenendaal, F.; de Vries, L.S.; van der Zee, D.C.; Benders, M.J.; van Herwaarden-Lindeboom, M.Y. Neurodevelopmental Outcomes After Neonatal Surgery for Major Noncardiac Anomalies. Pediatrics 2016, 137, e20151728. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.J. Anesthesia and neurotoxicity to the developing brain: The clinical relevance. Paediatr. Anaesth. 2011, 21, 716–721. [Google Scholar] [CrossRef]
- Johnston, C.C.; Stevens, B.J. Experience in a neonatal intensive care unit affects pain response. Pediatrics 1996, 98, 925–930. [Google Scholar]
- Anand, K.J.; Willson, D.F.; Berger, J.; Harrison, R.; Meert, K.L.; Zimmerman, J.; Carcillo, J.; Newth, C.J.; Prodhan, P.; Dean, J.M.; et al. Tolerance and withdrawal from prolonged opioid use in critically ill children. Pediatrics 2010, 125, e1208–e1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solodiuk, J.C.; Jennings, R.W.; Bajic, D. Evaluation of Postnatal Sedation in Full-Term Infants. Brain Sci. 2019, 9, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, V.; Brant, R.; Poskitt, K.J.; Tam, E.W.; Synnes, A.; Miller, S.P. Postnatal infection is associated with widespread abnormalities of brain development in premature newborns. Pediatr. Res. 2012, 71, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vohr, B.R.; Poindexter, B.B.; Dusick, A.M.; McKinley, L.T.; Wright, L.L.; Langer, J.C.; Poole, W.K.; Network, N.N.R. Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. Pediatrics 2006, 118, e115–e123. [Google Scholar] [CrossRef] [Green Version]
- Lucas, A.; Morley, R.; Cole, T.J.; Gore, S.M. A randomised multicentre study of human milk versus formula and later development in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 1994, 70, F141–F146. [Google Scholar] [CrossRef] [Green Version]
- Mongerson, C.R.L.; Wilcox, S.L.; Goins, S.M.; Pier, D.B.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Infant brain structural MRI analysis in the context of thoracic noncardiac surgery and critical care. Front. Pediatr. 2019, 7, 315. [Google Scholar] [CrossRef] [Green Version]
- Hodkinson, D.J.; Mongerson, C.R.L.; Jennings, R.W.; Bajic, D. Neonatal functional brain maturation in the context of perioperative critical care and pain management: A case report. Heliyon 2019, 5, e02350. [Google Scholar] [CrossRef] [Green Version]
- Mongerson, C.R.L.; Jennings, R.W.; Zurakowski, D.; Bajic, D. Quantitative MRI study of infant regional brain size following surgery for long-gap esophageal atresia requiring prolonged critical care. Int. J. Dev. Neurosci. 2019, 79, 11–20. [Google Scholar] [CrossRef]
- Bairdain, S.; Hamilton, T.E.; Smithers, C.J.; Manfredi, M.; Ngo, P.; Gallagher, D.; Zurakowski, D.; Foker, J.E.; Jennings, R.W. Foker process for the correction of long gap esophageal atresia: Primary treatment versus secondary treatment after prior esophageal surgery. J. Pediatr. Surg. 2015, 50, 933–937. [Google Scholar] [CrossRef]
- Kunisaki, S.M.; Foker, J.E. Surgical advances in the fetus and neonate: Esophageal atresia. Clin. Perinatol. 2012, 39, 349–361. [Google Scholar] [CrossRef]
- Foker, J.E.; Kendall Krosch, T.C.; Catton, K.; Munro, F.; Khan, K.M. Long-gap esophageal atresia treated by growth induction: The biological potential and early follow-up results. Semin. Pediatr. Surg. 2009, 18, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Bairdain, S.; Zurakowski, D.; Vargas, S.O.; Stenquist, N.; McDonald, M.; Towne, M.C.; Miller, D.T.; Jennings, R.W.; Kantor, D.B.; Agrawal, P.B. Long-Gap Esophageal Atresia Is a Unique Entity within the Esophageal Atresia Defect Spectrum. Neonatology 2017, 111, 140–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liszewski, M.C.; Bairdain, S.; Buonomo, C.; Jennings, R.W.; Taylor, G.A. Imaging of long gap esophageal atresia and the Foker process: Expected findings and complications. Pediatr. Radiol. 2014, 44, 467–475. [Google Scholar] [CrossRef]
- Anand, K.J.; Barton, B.A.; McIntosh, N.; Lagercrantz, H.; Pelausa, E.; Young, T.E.; Vasa, R. Analgesia and sedation in preterm neonates who require ventilatory support: Results from the NOPAIN trial. Neonatal Outcome and Prolonged Analgesia in Neonates. Arch. Pediatr. Adolesc. Med. 1999, 153, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Dewey, W.L. Various factors which affect the rate of development of tolerance and physical dependence to abused drugs. Nida Res. Monogr. 1984, 54, 39–49. [Google Scholar] [PubMed]
- Vet, N.J.; Kleiber, N.; Ista, E.; de Hoog, M.; de Wildt, S.N. Sedation in Critically Ill Children with Respiratory Failure. Front. Pediatr. 2016, 4, 89. [Google Scholar] [CrossRef] [PubMed]
- Paterson, S.J.; Badridze, N.; Flax, J.F.; Liu, W.C.; Benasich, A.A. A Method for Structural MRI Scanning of Non-Sedated Infants; International conference on infancy studies: Chicago, IL, USA, 2004. [Google Scholar]
- Almli, C.R.; Rivkin, M.J.; McKinstry, R.C.; Brain Development Cooperative Group. The NIH MRI study of normal brain development (Objective-2): Newborns, infants, toddlers, and preschoolers. Neuroimage 2007, 35, 308–325. [Google Scholar] [CrossRef]
- Raschle, N.; Zuk, J.; Ortiz-Mantilla, S.; Sliva, D.D.; Franceschi, A.; Grant, P.E.; Benasich, A.A.; Gaab, N. Pediatric neuroimaging in early childhood and infancy: Challenges and practical guidelines. Ann. N. Y. Acad. Sci. 2012, 1252, 43–50. [Google Scholar] [CrossRef]
- Tocchio, S.; Kline-Fath, B.; Kanal, E.; Schmithorst, V.J.; Panigrahy, A. MRI evaluation and safety in the developing brain. Semin. Perinatol. 2015, 39, 73–104. [Google Scholar] [CrossRef] [Green Version]
- Mongerson, C.R.L.; Jennings, R.W.; Main, S.A.; Jois, M.S.; Zurakowski, D.; Bajic, D. Infant corpus callosum volumes following thoracic noncardiac surgery for long-gap esophageal atresia. In Proceedings of the 2019 American Society of Anesthesiology Annual Meeting, Orlando, FL, USA, 19–23 October 2019. [Google Scholar]
- Mongerson, C.R.L.; Jaimes, C.; Zurakowski, D.; Jennings, R.W.; Bajic, D. Qualitative and qualitative study of infant corpus callosum following surgery and critical care for long-gap esophageal atresia. Sci. Rep. 2019. in review. [Google Scholar]
- Beare, R.J.; Chen, J.; Kelly, C.E.; Alexopoulos, D.; Smyser, C.D.; Rogers, C.E.; Loh, W.Y.; Matthews, L.G.; Cheong, J.L.; Spittle, A.J.; et al. Neonatal Brain Tissue Classification with Morphological Adaptation and Unified Segmentation. Front. Neuroinform. 2016, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Brady, M.; Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans. Med. Imaging 2001, 20, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Zhang, Y.; Lasky, R.E.; Datta, S.; Parikh, N.A.; Narayana, P.A. Comprehensive brain MRI segmentation in high risk preterm newborns. PLoS ONE 2010, 5, e13874. [Google Scholar] [CrossRef] [PubMed]
- Mai, J.K.; Assheuer, J.; Paxinos, G. Atlas of the Human Brain, 4th ed.; Academic Press: San Diego, CA, USA, 2015; p. 456. [Google Scholar]
- Wakana, S.; Jiang, H.; Nagae-Poetscher, L.M.; van Zijl, P.C.; Mori, S. Fiber tract-based atlas of human white matter anatomy. Radiology 2004, 230, 77–87. [Google Scholar] [CrossRef]
- Whitwell, J.L.; Crum, W.R.; Watt, H.C.; Fox, N.C. Normalization of cerebral volumes by use of intracranial volume: Implications for longitudinal quantitative MR imaging. Am. J. Neuroradiol. 2001, 22, 1483–1489. [Google Scholar]
- Matthews, L.G.; Walsh, B.H.; Knutsen, C.; Neil, J.J.; Smyser, C.D.; Rogers, C.E.; Inder, T.E. Brain growth in the NICU: Critical periods of tissue-specific expansion. Pediatr. Res. 2018, 83, 976–981. [Google Scholar] [CrossRef] [Green Version]
- Lee, S. Basic Knowledge of Tracheoesophageal Fistula and Esophageal Atresia. Adv. Neonatal Care 2018, 18, 14–21. [Google Scholar] [CrossRef]
- Volpe, J.J. Brain injury in premature infants: A complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009, 8, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Inder, T.E.; Wells, S.J.; Mogridge, N.B.; Spencer, C.; Volpe, J.J. Defining the nature of the cerebral abnormalities in the premature infant: A qualitative magnetic resonance imaging study. J. Pediatr. 2003, 143, 171–179. [Google Scholar] [CrossRef]
- Kapellou, O.; Counsell, S.J.; Kennea, N.; Dyet, L.; Saeed, N.; Stark, J.; Maalouf, E.; Duggan, P.; Ajayi-Obe, M.; Hajnal, J.; et al. Abnormal cortical development after premature birth shown by altered allometric scaling of brain growth. PLoS Med. 2006, 3, e265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortinau, C.; Neil, J. The neuroanatomy of prematurity: Normal brain development and the impact of preterm birth. Clin. Anat. 2015, 28, 168–183. [Google Scholar] [CrossRef] [PubMed]
- von Rhein, M.; Buchmann, A.; Hagmann, C.; Dave, H.; Bernet, V.; Scheer, I.; Knirsch, W.; Latal, B.; Bürki, C.; Prêtre, R.; et al. Severe Congenital Heart Defects Are Associated with Global Reduction of Neonatal Brain Volumes. J. Pediatr. 2015, 167, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Bertholdt, S.; Latal, B.; Liamlahi, R.; Pretre, R.; Scheer, I.; Goetti, R.; Dave, H.; Bernet, V.; Schmitz, A.; von Rhein, M.; et al. Cerebral lesions on magnetic resonance imaging correlate with preoperative neurological status in neonates undergoing cardiopulmonary bypass surgery. Eur. J. Cardiothorac. Surg. 2014, 45, 625–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitropoulos, A.; McQuillen, P.S.; Sethi, V.; Moosa, A.; Chau, V.; Xu, D.; Brant, R.; Azakie, A.; Campbell, A.; Barkovich, A.J.; et al. Brain injury and development in newborns with critical congenital heart disease. Neurology 2013, 81, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Yin, S.; Fang, J.; Hua, Y.; Wang, C.; Mu, D.; Zhou, K. Neurodevelopmental delay with critical congenital heart disease is mainly from prenatal injury not infant cardiac surgery: Current evidence based on a meta-analysis of functional magnetic resonance imaging. Ultrasound Obs. Gynecol. 2015, 45, 639–648. [Google Scholar] [CrossRef]
- Smith, G.C.; Gutovich, J.; Smyser, C.; Pineda, R.; Newnham, C.; Tjoeng, T.H.; Vavasseur, C.; Wallendorf, M.; Neil, J.; Inder, T. Neonatal intensive care unit stress is associated with brain development in preterm infants. Ann. Neurol. 2011, 70, 541–549. [Google Scholar] [CrossRef]
- Pierro, A.; Eaton, S. Metabolism and nutrition in the surgical neonate. Semin. Pediatr. Surg. 2008, 17, 276–284. [Google Scholar] [CrossRef]
- De Cunto, A.; Paviotti, G.; Travan, L.; Bua, J.; Cont, G.; Demarini, S. Impact of Surgery for Neonatal Gastrointestinal Diseases on Weight and Fat Mass. J. Pediatr. 2015, 167, 568–571. [Google Scholar] [CrossRef]
- Schwarzenberg, S.J.; Georgieff, M.K.; Committee On, N. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [Green Version]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Ramel, S.E.; Gray, H.L.; Christiansen, E.; Boys, C.; Georgieff, M.K.; Demerath, E.W. Greater Early Gains in Fat-Free Mass, but Not Fat Mass, Are Associated with Improved Neurodevelopment at 1 Year Corrected Age for Prematurity in Very Low Birth Weight Preterm Infants. J. Pediatr. 2016, 173, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Cheong, J.L.; Thompson, D.K.; Spittle, A.J.; Potter, C.R.; Walsh, J.M.; Burnett, A.C.; Lee, K.J.; Chen, J.; Beare, R.; Matthews, L.G.; et al. Brain Volumes at Term-Equivalent Age Are Associated with 2-Year Neurodevelopment in Moderate and Late Preterm Children. J. Pediatr. 2016, 174, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.; Cahill-Rowley, K.; Vassar, R.; Yeom, K.W.; Stecher, X.; Stevenson, D.K.; Hintz, S.R.; Barnea-Goraly, N. Neonatal brain microstructure correlates of neurodevelopment and gait in preterm children 18–22 mo of age: An MRI and DTI study. Pediatr. Res. 2015, 78, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Narberhaus, A.; Segarra, D.; Caldu, X.; Gimenez, M.; Junque, C.; Pueyo, R.; Botet, F. Gestational age at preterm birth in relation to corpus callosum and general cognitive outcome in adolescents. J. Child Neurol. 2007, 22, 761–765. [Google Scholar] [CrossRef]
- Miller, S.P.; McQuillen, P.S.; Hamrick, S.; Xu, D.; Glidden, D.V.; Charlton, N.; Karl, T.; Azakie, A.; Ferriero, D.M.; Barkovich, A.J.; et al. Abnormal brain development in newborns with congenital heart disease. N. Engl. J. Med. 2007, 357, 1928–1938. [Google Scholar] [CrossRef] [Green Version]
- Laing, S.; Walker, K.; Ungerer, J.; Badawi, N.; Spence, K. Early development of children with major birth defects requiring newborn surgery. J. Paediatr. Child Health 2011, 47, 140–147. [Google Scholar] [CrossRef]
- Walker, K.; Badawi, N.; Holland, A.J.; Halliday, R. Developmental outcomes following major surgery: What does the literature say? J. Paediatr. Child Health 2011, 47, 766–770. [Google Scholar] [CrossRef]
- Filan, P.M.; Hunt, R.W.; Anderson, P.J.; Doyle, L.W.; Inder, T.E. Neurologic outcomes in very preterm infants undergoing surgery. J. Pediatr. 2012, 160, 409–414. [Google Scholar] [CrossRef]
- Walker, K.; Holland, A.J.; Winlaw, D.; Sherwood, M.; Badawi, N. Neurodevelopmental outcomes and surgery in neonates. J. Paediatr. Child Health 2006, 42, 749–751. [Google Scholar] [CrossRef]
- Surgery and the tiny baby: Sensorineural outcome at 5 years of age. The Victorian Infant Collaborative Study Group. J. Paediatr. Child Health 1996, 32, 167–172. [CrossRef]
- Wilder, R.T.; Flick, R.P.; Sprung, J.; Katusic, S.K.; Barbaresi, W.J.; Mickelson, C.; Gleich, S.J.; Schroeder, D.R.; Weaver, A.L.; Warner, D.O. Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology 2009, 110, 796–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andropoulos, D.B. Effect of Anesthesia on the Developing Brain: Infant and Fetus. Fetal Diagn. Ther. 2018, 43, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Aslanabadi, S.; Ghabili, K.; Rouzrokh, M.; Hosseini, M.B.; Jamshidi, M.; Adl, F.H.; Shoja, M.M. Associated congenital anomalies between neonates with short-gap and long-gap esophageal atresia: A comparative study. Int. J. Gen. Med. 2011, 4, 487–491. [Google Scholar] [CrossRef] [Green Version]
- Pettit, R.E.; Kilroy, A.W.; Allen, J.H. Macrocephaly with head growth parallel to normal growth pattern: Neurological, developmental, and computerized tomography findings in full-term infants. Arch. Neurol. 1980, 37, 518–521. [Google Scholar] [CrossRef]
- Ment, L.R.; Duncan, C.C.; Geehr, R. Benign enlargement of the subarachnoid spaces in the infant. J. Neurosurg. 1981, 54, 504–508. [Google Scholar] [CrossRef]
- Carolan, P.L.; McLaurin, R.L.; Towbin, R.B.; Towbin, J.A.; Egelhoff, J.C. Benign extra-axial collections of infancy. Pediatr. Neurosci. 1985, 12, 140–144. [Google Scholar] [CrossRef]
- Alvarez, L.A.; Maytal, J.; Shinnar, S. Idiopathic external hydrocephalus: Natural history and relationship to benign familial macrocephaly. Pediatrics 1986, 77, 901–907. [Google Scholar]
- Maytal, J.; Alvarez, L.A.; Elkin, C.M.; Shinnar, S. External hydrocephalus: Radiologic spectrum and differentiation from cerebral atrophy. Am. J. Roentgenol. 1987, 148, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Iafolla, A.K.; McConkie-Rosell, A.; Chen, Y.T. VATER and hydrocephalus: Distinct syndrome? Am. J. Med. Genet. 1991, 38, 46–51. [Google Scholar] [CrossRef]
- Corsello, G.; Giuffre, L. VACTERL with hydrocephalus: A further case with probable autosomal recessive inheritance. Am. J. Med. Genet. 1994, 49, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Genuardi, M.; Chiurazzi, P.; Capelli, A.; Neri, G. X-linked VACTERL with hydrocephalus: The VACTERL-H syndrome. Birth Defects Orig. Artic. Ser. 1993, 29, 235–241. [Google Scholar] [PubMed]
- Chung, B.; Shaffer, L.G.; Keating, S.; Johnson, J.; Casey, B.; Chitayat, D. From VACTERL-H to heterotaxy: Variable expressivity of ZIC3-related disorders. Am. J. Med. Genet. A 2011, 155A, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Lago, P.; Rebsamen, S.; Clancy, R.R.; Pinto-Martin, J.; Kessler, A.; Zimmerman, R.; Schmelling, D.; Bernbaum, J.; Gerdes, M.; D’Agostino, J.A.; et al. MRI, MRA, and neurodevelopmental outcome following neonatal ECMO. Pediatr. Neurol. 1995, 12, 294–304. [Google Scholar] [CrossRef]
- Iwata, S.; Katayama, R.; Kinoshita, M.; Saikusa, M.; Araki, Y.; Takashima, S.; Abe, T.; Iwata, O. Region-specific growth restriction of brain following preterm birth. Sci. Rep. 2016, 6, 33995. [Google Scholar] [CrossRef] [Green Version]
- Inder, T.E.; Warfield, S.K.; Wang, H.; Huppi, P.S.; Volpe, J.J. Abnormal cerebral structure is present at term in premature infants. Pediatrics 2005, 115, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Shen, M.D.; Kim, S.H.; McKinstry, R.C.; Gu, H.; Hazlett, H.C.; Nordahl, C.W.; Emerson, R.W.; Shaw, D.; Elison, J.T.; Swanson, M.R.; et al. Increased Extra-axial Cerebrospinal Fluid in High-Risk Infants Who Later Develop Autism. Biol. Psychiatry 2017, 82, 186–193. [Google Scholar] [CrossRef]
- Keunen, K.; Isgum, I.; van Kooij, B.J.; Anbeek, P.; van Haastert, I.C.; Koopman-Esseboom, C.; Fieret-van Stam, P.C.; Nievelstein, R.A.; Viergever, M.A.; de Vries, L.S.; et al. Brain Volumes at Term-Equivalent Age in Preterm Infants: Imaging Biomarkers for Neurodevelopmental Outcome through Early School Age. J. Pediatr. 2016, 172, 88–95. [Google Scholar] [CrossRef]
- Barkovich, A.J.; Norman, D. Anomalies of the corpus callosum: Correlation with further anomalies of the brain. Am. J. Roentgenol. 1988, 151, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.G.; Laurent, I.; Woodward, L.J.; Inder, T.E. Detection of impaired growth of the corpus callosum in premature infants. Pediatrics 2006, 118, 951–960. [Google Scholar] [CrossRef]
- Thompson, D.K.; Inder, T.E.; Faggian, N.; Johnston, L.; Warfield, S.K.; Anderson, P.J.; Doyle, L.W.; Egan, G.F. Characterization of the corpus callosum in very preterm and full-term infants utilizing MRI. Neuroimage 2011, 55, 479–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beca, J.; Gunn, J.K.; Coleman, L.; Hope, A.; Reed, P.W.; Hunt, R.W.; Finucane, K.; Brizard, C.; Dance, B.; Shekerdemian, L.S. New white matter brain injury after infant heart surgery is associated with diagnostic group and the use of circulatory arrest. Circulation 2013, 127, 971–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rademaker, K.J.; Lam, J.N.; Van Haastert, I.C.; Uiterwaal, C.S.; Lieftink, A.F.; Groenendaal, F.; Grobbee, D.E.; de Vries, L.S. Larger corpus callosum size with better motor performance in prematurely born children. Semin. Perinatol. 2004, 28, 279–287. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Demographics | Preterm 1 | Preterm 2 | Preterm 3 | Term 1 | Term 2 | Term 3 |
|---|---|---|---|---|---|---|
| Sex | F | M | F | F | M | M |
| Race | White | White | AA | AA | Hispanic | Other |
| Gestational age (weeks) | 33 | 34 | 28 | 37 | 39 | 37 |
| Birth weight (kg) | 2.64 | 1.87 | 0.55 | 2.8 | 3.03 | Unknown |
| Birth by cesarean section | No | No | Yes | Yes | Yes | Unknown |
| Clinical Information | ||||||
| Initial Admission Service | NICU | NICU | MSICU | NICU | MSICU | MSICU |
| Main Diagnosis | LGEA | LGEA/TEF | LGEA | LGEA | LGEA/TEF | LGEA/TEF |
| Secondary Diagnoses | - | - | pHTN, IUGR, FTT | - | - | TOF |
| Prior to PRE- Foker MRI Scan | ||||||
| Total number of Surgical Events | 4 | 2 | 4 | 1 | 4 | 5 |
| MAC Equivalent Anesthesia (h) | 2.25 | 8.00 | 2.50 | 0.62 | 14.12 | 19.18 |
| Between PRE- and POST-Foker Scans | ||||||
| Total number of Surgical Events | 3 | 8 | 13 | 3 | 8 | 17 |
| MAC Equivalent Anesthesia (h) | 15.90 | 34.30 | 56.38 | 17.53 | 30.55 | 27.80 |
| Length of Muscle Relaxation (days) | 12 | 20 | 39 | 3 | 19 | 6 |
| Length of Intubation/Sedation (days) | 15 | 57 | 83 | 11 | 48 | 14 |
| Length of Weaning of Sedation (days) | 17 | * | 44 | 13 | 16 | 12 |
| Length of Antibiotic Treatment (days) | 4 | 51 | 99 | 8 | 51 | 78 |
| Length of Steroid Administration (days) | 2 | 0 | 23 | 10 | 3 | 11 |
| Length of TPN (days) | 18 | 47 | 66 | 17 | 31 | 20 |
| Patient | Event | Age at Event (months) | Anesthesia Exposure (h) | Notable Clinical Events/Procedures Performed |
|---|---|---|---|---|
| Preterm 1 | 1 | 0 | 0.25 | Endotracheal Intubation |
| 2 | 0 | 0.50 | PICC Insertion | |
| 3 | 0.03 | 1.00 | Laparoscopic Assisted G-tube Placement | |
| 4 | 2.57 | 0.50 | PICC Insertion | |
| Preterm 2 | 1 | 0.07 | 4.00 | Bronchoscopy, Thoracotomy, TEF Repair, Esophageal Immobilization |
| 2 | 2.43 | 4.00 | Inguinal Hernia Repair with Diagnostic Laparoscopy, Circumcision, Tongue Tie Release, EGD | |
| Preterm 3 | 1 | 1.93 | 1.00 | Open Gastrostomy with Contrast Study via G-tube |
| 2 | 1.97 | 0.25 | Endotracheal Intubation | |
| 3 | 2.20 | 0.50 | PICC Insertion | |
| 4 | 3.50 | 0.75 | Gastrostomy Revision with Fluoroscopy and G-tube Exchange | |
| Term 1 | 1 | 3.07 | 0.62 | Airway CT Scan |
| Term 2 | 1 | 0.03 | 6.00 | Thoracotomy, TEF Repair, Chest Tube and G-tube Placement |
| 2 | 0.90 | 1.00 | PICC Insertion | |
| 3 | 3.07 | 6.00 | Patch Repair of VSD, Suture Closure of ASD, PDA Ligation | |
| 4 | 5.57 | 1.12 | CT Scan | |
| Term 3 | 1 | 0 | 1.00 | Emergent Tracheostomy due to Cardiac Arrest following birth |
| 2 | 0.10 | 6.00 | Thoracotomy for EA/TEF Repair, Tracheostomy Replacement, Gastrostomy | |
| 3 | 5.10 | 7.70 | TOF Repair, EGD, TEE, Direct Laryngoscopy and Bronchoscopy | |
| 4 | 5.30 | 0 | Cardiac Arrest due to clogged tracheostomy; Post-arrest Cooling | |
| 5 | 5.47 | 1.70 | Direct Laryngoscopy and Bronchoscopy | |
| 6 | 5.50 | 2.78 | Airway MRI |
| PREMATURE PATIENTS | Preterm 1 | Preterm 2 | Preterm 3 | |||
| MRI Scan | Pre-Rx | Post-Rx | Pre-Rx | Post-Rx | Pre-Rx | Post-Rx |
| Corrected Age at Scan (months) | 1.02 | 2.16 | 1.93 | 3.80 | 2.36 | 7.41 |
| Weight at Scan (kg) | 4.910 | 6.040 | 4.380 | 5.920 | 4.200 | 6.810 |
| MRI Findings | 1. Increased Extra-Axial Space 2. Widened Sylvian Fissures | 1. Increased Extra-Axial Space 2. Widened Sylvian Fissures 3. SDH | 1. Enlarged Ventricles 2. IVH | 1. Enlarged Ventricles 2. IVH 3. Increased Extra-Axial Space 4. Arterial Ischemic/Hemorrhagic Stroke | 1. Increased Extra-Axial Space 2. Abnormality of CC 3. Enlarged Ventricles 4. Vascular Anomaly | 1. Increased Extra-Axial Space 2. Abnormality of CC 3. Enlarged Ventricles 4. Vascular Anomaly |
| FULL-TERM PATIENTS | Term 1 | Term 2 | Term 3 | |||
| MRI Scan | Pre-Rx | Post-Rx | Pre-Rx | Post-Rx | Pre-Rx | Post-Rx |
| Corrected Age at Scan (months) | 2.43 | 3.44 | 5.44 | 8.89 | 4.75 | 10.07 |
| Weight at Scan (kg) | 5.750 | 6.845 | 7.600 | 8.964 | 4.600 | 7.175 |
| MRI Findings | 1. Enlarged Ventricles 2. CC Thinning 3. Chronic Subdural Collection | 1. Progressive Enlargement of CSF Spaces | 1. Enlarged Ventricles 2. CC Thinning | 1. Enlarged Ventricles 2. CC Thinning 3. Increased Extra-Axial Space | 1. Prominent Extra-Axial Space | 1. Increased Extra-Axial Space 2. Brachycephaly 3. Under Operculation of Sylvian Fissures |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudisill, S.S.; Wang, J.T.; Jaimes, C.; Mongerson, C.R.L.; Hansen, A.R.; Jennings, R.W.; Bajic, D. Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study. Brain Sci. 2019, 9, 383. https://doi.org/10.3390/brainsci9120383
Rudisill SS, Wang JT, Jaimes C, Mongerson CRL, Hansen AR, Jennings RW, Bajic D. Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study. Brain Sciences. 2019; 9(12):383. https://doi.org/10.3390/brainsci9120383
Chicago/Turabian StyleRudisill, Samuel S., Jue T. Wang, Camilo Jaimes, Chandler R. L. Mongerson, Anne R. Hansen, Russell W. Jennings, and Dusica Bajic. 2019. "Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study" Brain Sciences 9, no. 12: 383. https://doi.org/10.3390/brainsci9120383
APA StyleRudisill, S. S., Wang, J. T., Jaimes, C., Mongerson, C. R. L., Hansen, A. R., Jennings, R. W., & Bajic, D. (2019). Neurologic Injury and Brain Growth in the Setting of Long-Gap Esophageal Atresia Perioperative Critical Care: A Pilot Study. Brain Sciences, 9(12), 383. https://doi.org/10.3390/brainsci9120383