Haemodynamic Instability and Brain Injury in Neonates Exposed to Hypoxia–Ischaemia

 , ,
, ,  ,
, {kind=link}
{kind=link}
Abstract
:1. The Problem
2. A Window for Reducing Further Brain Injury
3. Physiological Changes During Asphyxia
3.1. Myocardial Function
3.2. Cerebral Circulation
4. Failure of Oxygen Delivery and the Provision of Supplementary Oxygen
5. A Physiology-Based Resuscitation Approach
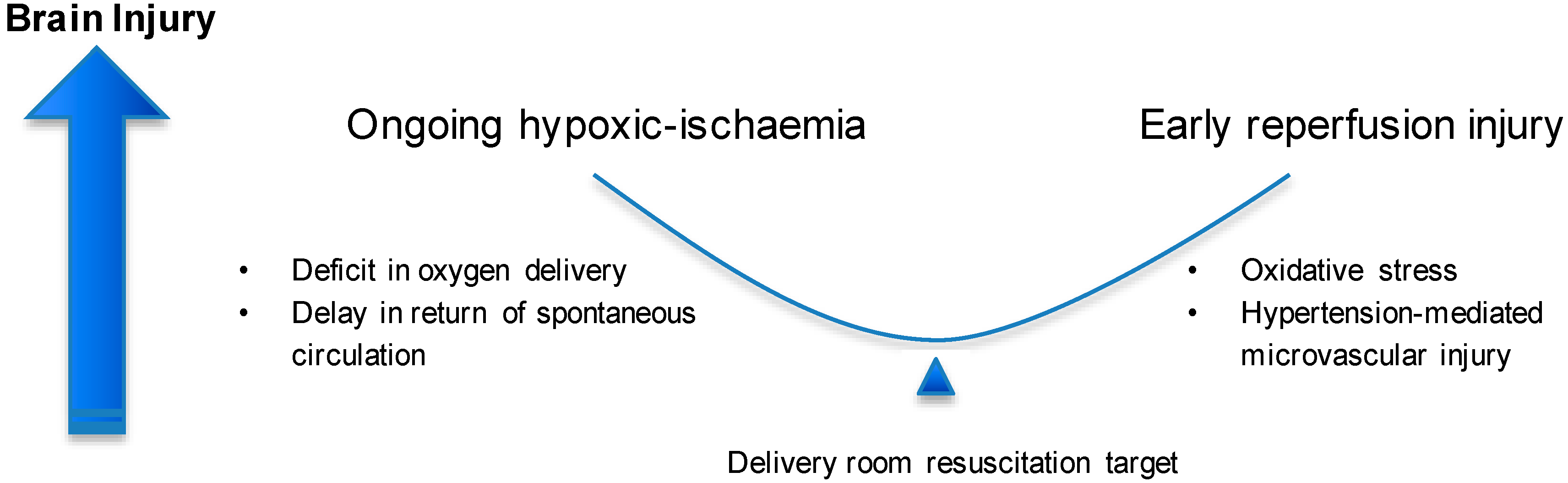
- Minimise ischaemic time by maintaining cardiac output and oxygenation until lung aeration is established;
- Avoid reperfusion injury by targeting a graded normalisation of cerebral perfusion pressure and oxygen kinetics (Figure 2).
Placental Transfusion
6. Personalised Resuscitation
7. Limitations and Practical Considerations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO | Disease Burden and Mortality Estimates. Available online: http://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html (accessed on 3 May 2018).
- Shankaran, S.; Laptook, A.R.; Ehrenkranz, R.A.; Tyson, J.E.; McDonald, S.A.; Donovan, E.F.; Fanaroff, A.A.; Poole, W.K.; Wright, L.L.; Higgins, R.D.; et al. Whole-Body Hypothermia for Neonates with Hypoxic–Ischemic Encephalopathy. N. Engl. J. Med. 2005, 353, 1574–1584. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, D.V.; Strohm, B.; Edwards, A.D.; Dyet, L.; Halliday, H.L.; Juszczak, E.; Kapellou, O.; Levene, M.; Marlow, N.; Porter, E.; et al. Moderate Hypothermia to Treat Perinatal Asphyxial Encephalopathy. N. Engl. J. Med. 2009, 361, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Wyatt, J.S.; Azzopardi, D.; Ballard, R.; Edwards, A.D.; Ferriero, D.M.; Polin, R.A.; Robertson, C.M.; Thoresen, M.; Whitelaw, A.; et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: Multicentre randomised trial. Lancet 2005, 365, 663–670. [Google Scholar] [CrossRef]
- Jacobs, S.E.; Berg, M.; Hunt, R.; Tarnow-Mordi, W.O.; Inder, T.E.; Davis, P.G. Cooling for newborns with hypoxic ischaemic encephalopathy. In Cochrane Database of Systematic Reviews; Jacobs, S.E., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2013; p. CD003311. [Google Scholar]
- Davis, P.G.; Tan, A.; O’Donnell, C.P.; Schulze, A. Resuscitation of newborn infants with 100% oxygen or air: A systematic review and meta-analysis. Lancet 2004, 364, 1329–1333. [Google Scholar] [CrossRef]
- Wyllie, J.; Bruinenberg, J.; Roehr, C.C.; Rüdiger, M.; Trevisanuto, D.; Urlesberger, B. European Resuscitation Council Guidelines for Resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation 2015, 95, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; Kim, H.-S.; Liley, H.G.; Mildenhall, L.; Simon, W.M.; et al. Part 7: Neonatal Resuscitation. Circulation 2015, 132, S204–S241. [Google Scholar] [CrossRef] [PubMed]
- Kamath-Rayne, B.D.; Jobe, A.H. Birth Asphyxia; Elsevier: Philadelphia, PA, USA, 2016; ISBN 9780323462846. [Google Scholar]
- Bocking, A.D.; Gagnon, R.; White, S.E.; Homan, J.; Milne, K.M.; Richardson, B.S. Circulatory responses to prolonged hypoxemia in fetal sheep. Am. J. Obstet. Gynecol. 1988, 159, 1418–1424. [Google Scholar] [CrossRef]
- Hooper, S.B. Fetal metabolic responses to hypoxia. Reprod. Fertil. Dev. 1995, 7, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Zaichkin, J.; Kattwinkel, J.; McGowan, J. NRP Neonatal Resuscitation Textbook, 6th ed.; American Academy of Pediatrics: Itasca, IL, USA; American Heart Association: Dallas, TX, USA, 2011; ISBN 9781581106305. [Google Scholar]
- Polglase, G.R.; Ong, T.; Hillman, N.H. Cardiovascular Alterations and Multiorgan Dysfunction after Birth Asphyxia. Clin. Perinatol. 2016, 43, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Sobotka, K.S.; Polglase, G.R.; Schmölzer, G.M.; Davis, P.G.; Klingenberg, C.; Hooper, S.B. Effects of chest compressions on cardiovascular and cerebral hemodynamics in asphyxiated near-term lambs. Pediatr. Res. 2015, 78, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Polglase, G.R.; Blank, D.A.; Barton, S.K.; Miller, S.L.; Stojanovska, V.; Kluckow, M.; Gill, A.W.; LaRosa, D.; te Pas, A.B.; Hooper, S.B. Physiologically based cord clamping stabilises cardiac output and reduces cerebrovascular injury in asphyxiated near-term lambs. Arch. Dis. Child.-Fetal Neonatal Ed. 2018, 103, F530–F538. [Google Scholar] [CrossRef] [PubMed]
- Sobotka, K.S.; Ong, T.; Polglase, G.R.; Crossley, K.J.; Moss, T.J.M.; Hooper, S.B. The effect of oxygen content during an initial sustained inflation on heart rate in asphyxiated near-term lambs. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F337–F343. [Google Scholar] [CrossRef] [PubMed]
- Vutskits, L. Cerebral blood flow in the neonate. Pediatr. Anesth. 2014, 24, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Chalak, L.F.; Tarumi, T.; Zhang, R. The “neurovascular unit approach” to evaluate mechanisms of dysfunctional autoregulation in asphyxiated newborns in the era of hypothermia therapy. Early Hum. Dev. 2014, 90, 687–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Toro, J.; Louis, P.T.; Goddard-Finegold, J. Cerebrovascular regulation and neonatal brain injury. Pediatr. Neurol. 1991, 7, 3–12. [Google Scholar] [CrossRef]
- Herrera-Marschitz, M.; Neira-Peña, T.; Leyton, L.; Gebicke-Haerter, P.; Rojas-Mancilla, E.; Morales, P.; Bustamante, D. Short- and Long-Term Consequences of Perinatal Asphyxia: Looking for Neuroprotective Strategies. Adv. Neurobiol. 2015, 10, 169–198. [Google Scholar] [PubMed]
- Smolich, J.J.; Kenna, K.R.; Cheung, M.M. Onset of asphyxial state in nonrespiring interval between cord clamping and ventilation increases hemodynamic lability of birth transition in preterm lambs. J. Appl. Physiol. 2015, 118, 675–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polglase, G.R.; Dawson, J.A.; Kluckow, M.; Gill, A.W.; Davis, P.G.; te Pas, A.B.; Crossley, K.J.; McDougall, A.; Wallace, E.M.; Hooper, S.B. Ventilation Onset Prior to Umbilical Cord Clamping (Physiological-Based Cord Clamping) Improves Systemic and Cerebral Oxygenation in Preterm Lambs. PLoS ONE 2015, 10, e0117504. [Google Scholar] [CrossRef] [PubMed]
- Lio, A.; Aurilia, C.; Zahra, V.; Moss, T.J.; LaRosa, D.A.; Hooper, S.B.; Gill, A.W.; Kluckow, M.; Nitsos, I.; Vento, G.; et al. Ventilation Prior to Umbilical Cord Clamping Improves Cardiovascular Stability and Oxygenation in Preterm Lambs After Exposure to Intrauterine Inflammation. Front. Pediatr. 2018, 6, 286. [Google Scholar] [CrossRef] [PubMed]
- Smolich, J.J.; Kenna, K.R.; Esler, M.D.; Phillips, S.E.; Lambert, G.W. Greater sympathoadrenal activation with longer preventilation intervals after immediate cord clamping increases hemodynamic lability at birth in preterm lambs. Am. J. Physiol. Integr. Comp. Physiol. 2017, 312, R903–R911. [Google Scholar] [CrossRef] [PubMed]
- Dawes, G.S.; Mott, J.C.; Widdicombe, J.G. The foetal circulation in the lamb. J. Physiol. 1954, 126, 563–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dildy, G.A.; van den Berg, P.P.; Katz, M.; Clark, S.L.; Jongsma, H.W.; Nijhuis, J.G.; Loucks, C.A. Intrapartum fetal pulse oximetry: Fetal oxygen saturation trends during labor and relation to delivery outcome. Am. J. Obstet. Gynecol. 1994, 171, 679–684. [Google Scholar] [CrossRef]
- Luttkus, A.; Fengler, T.; Friedmann, W.; Dudenhausen, J. Continuous monitoring of fetal oxygen saturation by pulse oximetry. Obstet. Gynecol. 1995, 85, 183–186. [Google Scholar] [CrossRef]
- Luttkus, A.K.; Callsen, T.-A.; Stupin, J.H.; Dudenhausen, J.W. Pulse oximetry during labour—Does it give rise to hope? Value of saturation monitoring in comparison to fetal blood gas status. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 110 (Suppl. 1), S132–S138. [Google Scholar] [CrossRef]
- Dawson, J.A.; Kamlin, C.O.F.; Vento, M.; Wong, C.; Cole, T.J.; Donath, S.M.; Davis, P.G.; Morley, C.J. Defining the Reference Range for Oxygen Saturation for Infants After Birth. Pediatrics 2010, 125, e1340–e1347. [Google Scholar] [CrossRef] [PubMed]
- Murphy, P.J. The fetal circulation. Contin. Educ. Anaesth. Crit. Care Pain 2005, 5, 107–112. [Google Scholar] [CrossRef]
- Lang, J.A.R.; Pearson, J.T.; Binder-Heschl, C.; Wallace, M.J.; Siew, M.L.; Kitchen, M.J.; te Pas, A.B.; Fouras, A.; Lewis, R.A.; Polglase, G.R.; et al. Increase in pulmonary blood flow at birth: Role of oxygen and lung aeration. J. Physiol. 2016, 594, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Smit, E.; Liu, X.; Gill, H.; Jary, S.; Wood, T.; Thoresen, M. The effect of resuscitation in 100% oxygen on brain injury in a newborn rat model of severe hypoxic-ischaemic encephalopathy. Resuscitation 2015, 96, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Te Pas, A.B.; Sobotka, K.; Hooper, S.B. Novel Approaches to Neonatal Resuscitation and the Impact on Birth Asphyxia. Clin. Perinatol. 2016, 43, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Fellman, V.; Raivio, K.O. Reperfusion injury as the mechanism of brain damage after perinatal asphyxia. Pediatr. Res. 1997, 41, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, E.P.; Ekici, B.; Tatlı, B. Neonatal hypoxic ischemic encephalopathy: An update on disease pathogenesis and treatment. Expert Rev. Neurother. 2017, 17, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Alison, B.J.; Wallace, E.M.; Crossley, K.J.; Gill, A.W.; Kluckow, M.; te Pas, A.B.; Morley, C.J.; Polglase, G.R.; Hooper, S.B. Delaying cord clamping until ventilation onset improves cardiovascular function at birth in preterm lambs. J. Physiol. 2013, 591, 2113–2126. [Google Scholar] [CrossRef] [PubMed]
- Crossley, K.J.; Allison, B.J.; Polglase, G.R.; Morley, C.J.; Davis, P.G.; Hooper, S.B. Dynamic changes in the direction of blood flow through the ductus arteriosus at birth. J. Physiol. 2009, 587, 4695–4704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, S.B.; Binder-Heschl, C.; Polglase, G.R.; Gill, A.W.; Kluckow, M.; Wallace, E.M.; Blank, D.; te Pas, A.B. The timing of umbilical cord clamping at birth: Physiological considerations. Matern. Health Neonatol. Perinatol. 2016, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Ersdal, H.; Linde, J.; Auestad, B.; Mduma, E.; Lyanga, S.; Svensen, E.; Perlman, J. Timing of cord clamping in relation to start of breathing or ventilation among depressed neonates-an observational study. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Ersdal, H.L.; Mduma, E.; Svensen, E.; Perlman, J.M. Early initiation of basic resuscitation interventions including face mask ventilation may reduce birth asphyxia related mortality in low-income countries. Resuscitation 2012, 83, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs early umbilical cord clamping for preterm infants: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.J.; Middleton, P.; Dowswell, T.; Morris, P.S. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst. Rev. 2013, CD004074. [Google Scholar] [CrossRef] [PubMed]
- Brace, R.A. Fetal blood volume responses to acute fetal hypoxia. Am. J. Obstet. Gynecol. 1986, 155, 889–893. [Google Scholar] [CrossRef]
- Linderkamp, O.; Versmold, H.T.; Messow-Zahn, K.; Müller-Holve, W.; Riegel, K.P.; Betke, K. The effect of intra-partum and intra-uterine asphyxia on placental transfusion in premature and full-term infants. Eur. J. Pediatr. 1978, 127, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Brucknerová, I.; Ujházy, E.; Dubovický, M.; Mach, M. Early assessment of the severity of asphyxia in term newborns using parameters of blood count. Interdiscip. Toxicol. 2008, 1, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Naumann, D.N.; Hazeldine, J.; Bishop, J.; Midwinter, M.J.; Harrison, P.; Nash, G.; Hutchings, S.D. Impact of plasma viscosity on microcirculatory flow after traumatic haemorrhagic shock: A prospective observational study. Clin. Hemorheol. Microcirc. 2019, 71, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Kalteren, W.S.; Ter Horst, H.J.; den Heijer, A.E.; de Vetten, L.; Kooi, E.M.W.; Bos, A.F. Perinatal Anemia is Associated with Neonatal and Neurodevelopmental Outcomes in Infants with Moderate to Severe Perinatal Asphyxia. Neonatology 2018, 114, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Phillipos, E.; Solevåg, A.L.; Pichler, G.; Aziz, K.; van Os, S.; O’Reilly, M.; Cheung, P.-Y.; Schmölzer, G.M. Heart Rate Assessment Immediately after Birth. Neonatology 2016, 109, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Nolan, J.P.; Böttiger, B.W.; Perkins, G.D.; Lott, C.; Carli, P.; Pellis, T.; Sandroni, C.; Skrifvars, M.B.; Smith, G.B.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015, 95, 100–147. [Google Scholar] [CrossRef] [PubMed]
- Hamrick, J.T.; Hamrick, J.L.; Bhalala, U.; Armstrong, J.S.; Lee, J.-H.; Kulikowicz, E.; Lee, J.K.; Kudchadkar, S.R.; Koehler, R.C.; Hunt, E.A.; et al. End-Tidal CO2–Guided Chest Compression Delivery Improves Survival in a Neonatal Asphyxial Cardiac Arrest Model. Pediatr. Crit. Care Med. 2017, 18, e575–e584. [Google Scholar] [CrossRef] [PubMed]
- Witcombe, N.B.; Yiallourou, S.R.; Sands, S.A.; Walker, A.M.; Horne, R.S.C. Preterm Birth Alters the Maturation of Baroreflex Sensitivity in Sleeping Infants. Pediatrics 2012, 129, e89–e96. [Google Scholar] [CrossRef] [PubMed]
- Kroese, J.K.; van Vonderen, J.J.; Narayen, I.C.; Walther, F.J.; Hooper, S.; te Pas, A.B. The perfusion index of healthy term infants during transition at birth. Eur. J. Pediatr. 2016, 175, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Dix, L.M.L.; van Bel, F.; Lemmers, P.M.A. Monitoring Cerebral Oxygenation in Neonates: An Update. Front. Pediatr. 2017, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Cheung, P.-Y.; Aziz, K.; Urlesberger, B.; Schmölzer, G.M. How to monitor the brain during immediate neonatal transition and resuscitation? A systematic qualitative review of the literature. Neonatology 2014, 105, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Urlesberger, B.; Baik, N.; Schwaberger, B.; Binder-Heschl, C.; Avian, A.; Pansy, J.; Cheung, P.-Y.; Schmölzer, G.M. Cerebral Oxygen Saturation to Guide Oxygen Delivery in Preterm Neonates for the Immediate Transition after Birth: A 2-Center Randomized Controlled Pilot Feasibility Trial. J. Pediatr. 2016, 170, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Baik, N.; Urlesberger, B.; Cheung, P.-Y.; Aziz, K.; Avian, A.; Schmölzer, G.M. Cord clamping time in spontaneously breathing preterm neonates in the first minutes after birth: Impact on cerebral oxygenation—A prospective observational study. J. Matern.-Fetal Neonatal Med. 2016, 29, 1570–1572. [Google Scholar] [CrossRef] [PubMed]
- Baik, N.; Urlesberger, B.; Schwaberger, B.; Schmölzer, G.M.; Mileder, L.; Avian, A.; Pichler, G. Reference Ranges for Cerebral Tissue Oxygen Saturation Index in Term Neonates during Immediate Neonatal Transition after Birth. Neonatology 2015, 108, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Montaldo, P.; De Leonibus, C.; Giordano, L.; De Vivo, M.; Giliberti, P. Cerebral, renal and mesenteric regional oxygen saturation of term infants during transition. J. Pediatr. Surg. 2015, 50, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Kooi, E.M.W.; Verhagen, E.A.; Elting, J.W.J.; Czosnyka, M.; Austin, T.; Wong, F.Y.; Aries, M.J.H. Measuring cerebrovascular autoregulation in preterm infants using near-infrared spectroscopy: An overview of the literature. Expert Rev. Neurother. 2017, 17, 801–818. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.Y.; Nakamura, M.; Alexiou, T.; Brodecky, V.; Walker, A.M. Tissue oxygenation index measured using spatially resolved spectroscopy correlates with changes in cerebral blood flow in newborn lambs. Intensive Care Med. 2009, 35, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Urlesberger, B.; Brandner, A.; Pocivalnik, M.; Koestenberger, M.; Morris, N.; Pichler, G. A Left-to-Right Shunt via the Ductus Arteriosus Is Associated with Increased Regional Cerebral Oxygen Saturation during Neonatal Transition. Neonatology 2013, 103, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.Y.; Alexiou, T.; Samarasinghe, T.; Brodecky, V.; Walker, A.M. Cerebral arterial and venous contributions to tissue oxygenation index measured using spatially resolved spectroscopy in newborn lambs. Anesthesiology 2010, 113, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Tamussino, A.; Urlesberger, B.; Baik, N.; Schwaberger, B.; Binder-Heschl, C.; Schmölzer, G.M.; Avian, A.; Pichler, G. Low cerebral activity and cerebral oxygenation during immediate transition in term neonates-A prospective observational study. Resuscitation 2016, 103, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, J.; Cheung, P.-Y.; Aziz, K.; Rajani, V.; O’Reilly, M.; Pichler, G.; Schmölzer, G.M. Exhaled Carbon Dioxide and Neonatal Breathing Patterns in Preterm Infants after Birth. J. Pediatr. 2015, 167, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Fierstra, J.; Winter, J.D.; Machina, M.; Lukovic, J.; Duffin, J.; Kassner, A.; Fisher, J.A. Non-invasive accurate measurement of arterial PCO2 in a pediatric animal model. J. Clin. Monit. Comput. 2013, 27, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Hütten, M.C.; Goos, T.G.; Ophelders, D.; Nikiforou, M.; Kuypers, E.; Willems, M.; Niemarkt, H.J.; Dankelman, J.; Andriessen, P.; Mohns, T.; et al. Fully automated predictive intelligent control of oxygenation (PRICO) in resuscitation and ventilation of preterm lambs. Pediatr. Res. 2015, 78, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummler, H.; Fuchs, H.; Schmid, M. Automated adjustments of inspired fraction of oxygen to avoid hypoxemia and hyperoxemia in neonates—A systematic review on clinical studies. Klin. Padiatr. 2014, 226, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, M.; Moroz, T.; Hapuarachchi, T.; Bainbridge, A.; Robertson, N.J.; Cooper, C.E.; Tachtsidis, I. Modelling Blood Flow and Metabolism in the Preclinical Neonatal Brain during and Following Hypoxic-Ischaemia. PLoS ONE 2015, 10, e0140171. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Poretti, A.; Perin, J.; Huisman, T.A.G.M.; Parkinson, C.; Chavez-Valdez, R.; O’Connor, M.; Reyes, M.; Armstrong, J.; Jennings, J.M.; et al. Optimizing Cerebral Autoregulation May Decrease Neonatal Regional Hypoxic-Ischemic Brain Injury. Dev. Neurosci. 2017, 39, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, E.; Knol, R.; Vernooij, A.S.N.; van den Akker, T.; Vlasman, P.E.; Klumper, F.J.C.M.; DeKoninck, P.; Polglase, G.R.; Hooper, S.B.; Te Pas, A.B. Physiological-based cord clamping in preterm infants using a new purpose-built resuscitation table: A feasibility study. Arch. Dis. Child.-Fetal Neonatal Ed. 2018. [Google Scholar] [CrossRef] [PubMed]
- Duley, L.; Dorling, J.; Pushpa-Rajah, A.; Oddie, S.J.; Yoxall, C.W.; Schoonakker, B.; Bradshaw, L.; Mitchell, E.J.; Fawke, J.A. Cord Pilot Trial Collaborative Group. Randomised trial of cord clamping and initial stabilisation at very preterm birth. Arch. Dis. Child.-Fetal Neonatal Ed. 2018, 103, F6–F14. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.; Kattwinkel, J.; Chisholm, C.; Blackman, A.; Wilson, S.; Fairchild, K. Ventilation of Preterm Infants during Delayed Cord Clamping (VentFirst): A Pilot Study of Feasibility and Safety. Am. J. Perinatol. 2016, 34, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, D.A.; Badurdeen, S.; Kamlin, C.O.F.; Jacobs, S.E.; Thio, M.; Dawson, J.A.; Kane, S.C.; Dennis, A.T.; Polglase, G.R.; Hooper, S.B.; et al. Baby-directed umbilical cord clamping: A feasibility study. Resuscitation 2018, 131, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liverpool Invention Could Help Save Babies’ Lives. Available online: https://www.rlbuht.nhs.uk/news/liverpool-invention-could-help-save-babies-lives/ (accessed on 10 January 2019).


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badurdeen, S.; Roberts, C.; Blank, D.; Miller, S.; Stojanovska, V.; Davis, P.; Hooper, S.; Polglase, G. Haemodynamic Instability and Brain Injury in Neonates Exposed to Hypoxia–Ischaemia. Brain Sci. 2019, 9, 49. https://doi.org/10.3390/brainsci9030049
Badurdeen S, Roberts C, Blank D, Miller S, Stojanovska V, Davis P, Hooper S, Polglase G. Haemodynamic Instability and Brain Injury in Neonates Exposed to Hypoxia–Ischaemia. Brain Sciences. 2019; 9(3):49. https://doi.org/10.3390/brainsci9030049
Chicago/Turabian StyleBadurdeen, Shiraz, Calum Roberts, Douglas Blank, Suzanne Miller, Vanesa Stojanovska, Peter Davis, Stuart Hooper, and Graeme Polglase. 2019. "Haemodynamic Instability and Brain Injury in Neonates Exposed to Hypoxia–Ischaemia" Brain Sciences 9, no. 3: 49. https://doi.org/10.3390/brainsci9030049
APA StyleBadurdeen, S., Roberts, C., Blank, D., Miller, S., Stojanovska, V., Davis, P., Hooper, S., & Polglase, G. (2019). Haemodynamic Instability and Brain Injury in Neonates Exposed to Hypoxia–Ischaemia. Brain Sciences, 9(3), 49. https://doi.org/10.3390/brainsci9030049