Anodal Transcranial Direct Current Stimulation over the Vertex Enhances Leg Motor Cortex Excitability Bilaterally


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Transcanial Direct Current Stimulation
2.4. Electromyography
2.5. Transcranial Magnetic Stimulation
2.6. Statistical Analysis
3. Results
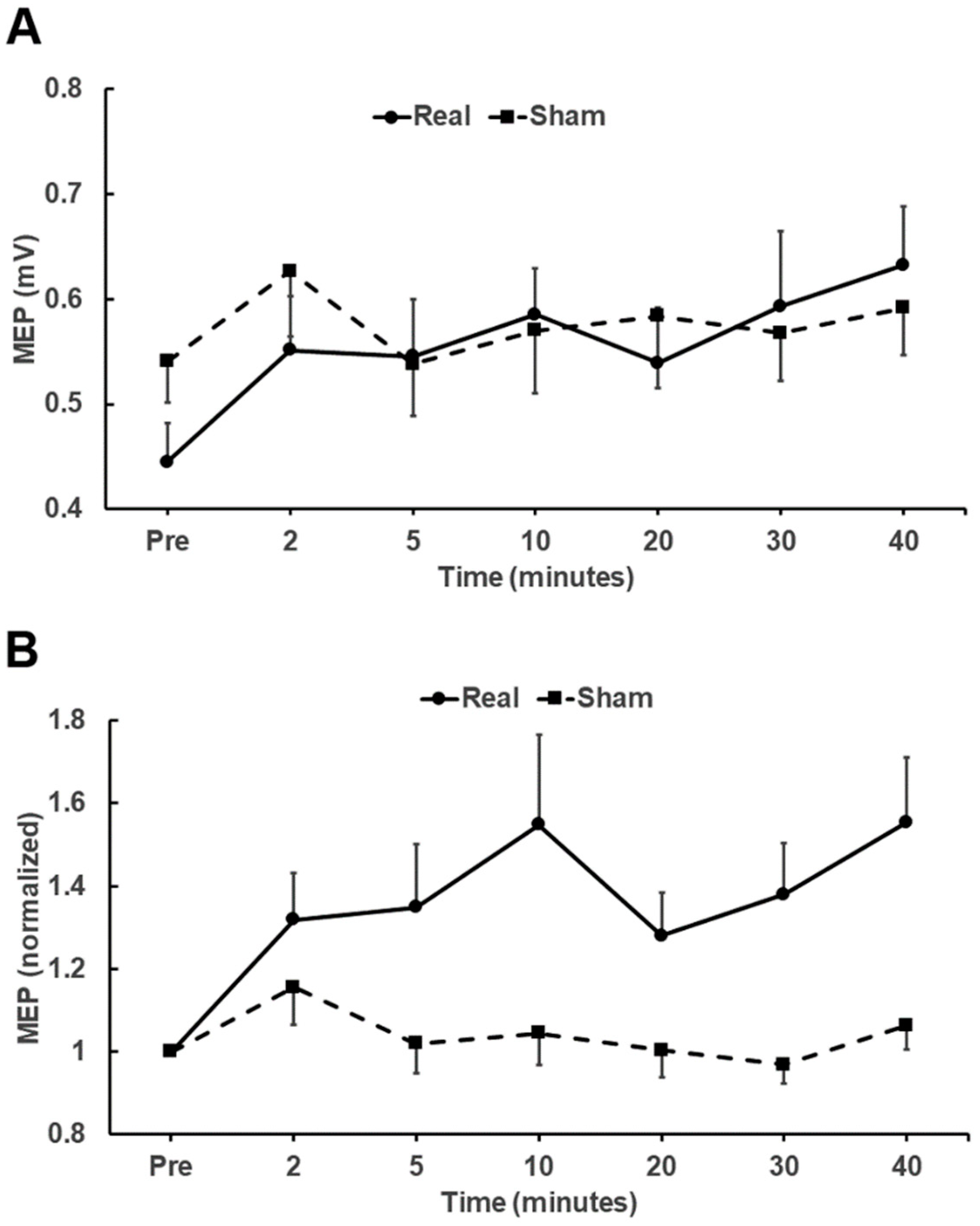
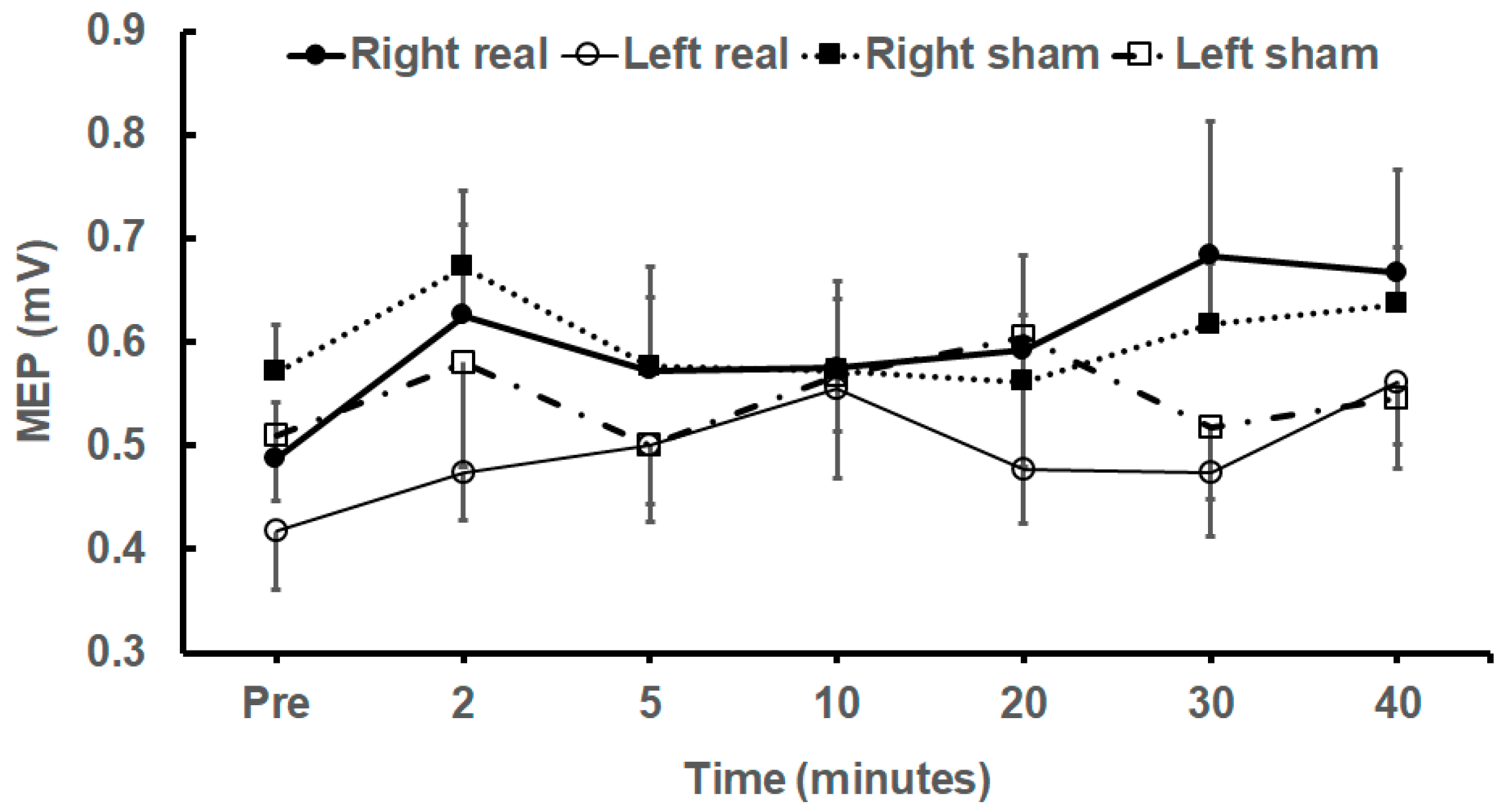
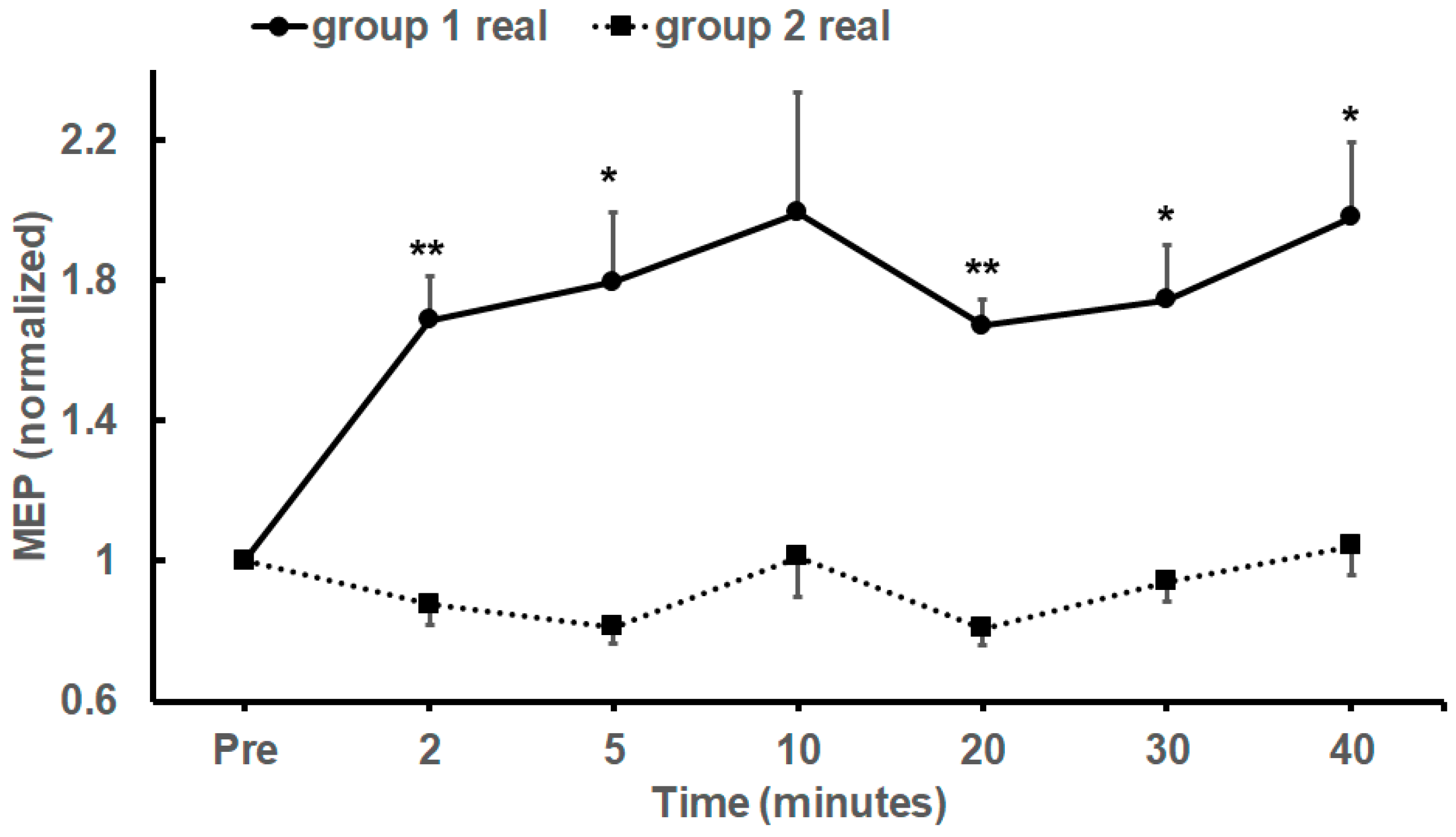
Comparison of Real and Sham tDCS Stimulation for 20 min
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| M1 | Motor cortex |
| MEP | Motor Evoked Potential |
| MSO | Maximum Stimulator Output |
| RMT | Resting Motor Threshold |
| TA | Tibialis Anterior |
| tDCS | Transcranial Direct Current Stimulation |
| TS | Test Stimulus |
References
- Prior, M.M.; Stinear, J.W. Phasic spike-timing-dependent plasticity of human motor cortex during walking. Brain Res. 2006, 1110, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, G.; Stinear, J.W. The Effects of Transcranial Stimulation on Paretic Lower Limb Motor Excitability During Walking. J. Clin. Neurophysiol. 2009, 26, 272–279. [Google Scholar] [CrossRef]
- Kaski, D.; Bronstein, A.M. Treatments for Neurological Gait and Balance Disturbance: The use of non-invasive electrical brain stimulation. Adv. Neurosci. 2014, 2014. [Google Scholar] [CrossRef]
- Kaski, D.; Quadir, S.; Patel, M.; Yousif, N.; Bronstein, A.M. Enhanced locomotor adaptation after effect in the “broken escalator” phenomenon using anodal tDCS. J. Neurophysiol. 2012, 107, 2493–2505. [Google Scholar] [CrossRef]
- Kaski, D.; Dominguez, R.; Allum, J.; Islam, A.; Bronstein, A. Combining physical training with transcranial direct current stimulation to improve gait in Parkinson’s disease: A pilot randomized controlled study. Clin. Rehabil. 2014, 28, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, E.; Steele, C.J.; Hoff, M.; Gundlach, C.; Rjosk, V.; Sehm, B.; Villringer, A.; Ragert, P. Transcranial direct current stimulation (tDCS) over primary motor cortex leg area promotes dynamic balance task performance. Clin. Neurophysiol. 2016, 127, 2455–2462. [Google Scholar] [CrossRef]
- Grecco, L.A.C.; Oliveira, C.S.; Galli, M.; Cosmo, C.; Duarte, N.D.A.C.; Zanon, N.; Edwards, D.J.; Fregni, F. Spared Primary Motor Cortex and The Presence of MEP in Cerebral Palsy Dictate the Responsiveness to tDCS during Gait Training. Front. Hum. Neurosci. 2016, 10, 265. [Google Scholar] [CrossRef]
- Bastani, A.; Jaberzadeh, S. Does anodal transcranial direct current stimulation enhance excitability of the motor cortex and motor function in healthy individuals and subjects with stroke: A systematic review and meta-analysis. Clin. Neurophysiol. 2012, 123, 644–657. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Galea, J.M.; Celnik, P. Brain polarization enhances the formation and retrntion of motor memories. J. Neurophysiol. 2009, 102, 294–301. [Google Scholar] [CrossRef]
- Nair, D.G.; Renga, V.; Lindenberg, R.; Zhu, L.; Schlaug, G. Optimizing recovery potential through simultaneous occupational therapy and non-invasive brain-stimulation using tDCS. Restor. Neurol. Neurosci. 2011, 29, 411–420. [Google Scholar] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Wiethoff, S.; Hamada, M.; Rothwell, J.C. Variability in Response to Transcranial Direct Current Stimulation of the Motor Cortex. Brain Stimul. 2014, 7, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Alonso, V.; Cheeran, B.; Rio-Rodriguez, D.; Fernandez-del-Olmo, M. Inter-individual Variability in Response to Non-invasive Brain Stimulation Paradigms. Brain Stimul. 2014, 7, 372–380. [Google Scholar] [CrossRef]
- Madhavan, S.; Sriraman, A.; Freels, S. Reliability and Variability of tDCS Induced Changes in the Lower Limb Motor Cortex. Brain Sci. 2016, 6, 26. [Google Scholar]
- Laakso, I.; Mikkonen, M.; Koyama, S.; Hirata, A.; Tanaka, S. Can electric fields explain inter-individual variability in transcranial direct current stimulation of the motor cortex? Sci. Rep. 2019, 9, 626. [Google Scholar] [CrossRef] [PubMed]
- Filmer, H.L.; Ehrhardt, S.E.; Bollmann, S.; Mattingley, J.B.; Dux, P.E. Accounting for individual differences in the response to tDCS with baseline levels of neurochemical excitability. Cortex 2019, 115, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Labruna, L.; Stark-Inbar, A.; Breska, A.; Dabit, M.; Vanderschelden, B.; Nitsche, M.A.; Ivry, R.B. Individual differences in TMS sensitivity influence the efficacy of tDCS in facilitating sensorimotor adaptation. Brain Stimul. 2019. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Tergau, F.; Liebetanz, D.; Paulus, W. Pharmacological approach to the mechanisms of transcranial DC-stimulation-induced after-effects of human motor cortex excitability. Brain 2002, 125, 2238–2247. [Google Scholar]
- Ardolino, G.; Bossi, B.; Barbieri, S.; Priori, A. Non-synaptic mechanisms underlie the after-effects of cathodal transcutaneous direct current stimulation of the human brain. J. Physiol. 2005, 568, 653–663. [Google Scholar] [CrossRef]
- Roche, N.; Lackmy, A.; Achache, V.; Bussel, B.; Katz, R. Effect of anodal transcranial direct current stimulation over the leg motor area on lumbar spinal network excitability in healthy subjects. J. Physiol. 2009, 589, 2813–2826. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, D.T.; Norton, J.A.; Roy, F.D.; Gorassini, M.A. Effects of transcranial direct current stimulation on the excitability of the leg motor cortex. Exp. Brain 2007, 182, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, S.; Stinear, J.W. Focal and bi-directional modulation of lower limb motor cortex using anodal transcranial direct current stimulation. Brain Stimul. 2010, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Batsikadze, G.; Moliadze, V.; Paulus, W.; Kuo, M.-F.; Nitsche, M.A. Partially non-linear stimulation intensity-dependent effects of direct current stimulation on motor cortex excitability in humans. J. Physiol. 2013, 591, 1987–2000. [Google Scholar] [CrossRef] [PubMed]
- Lacz’o, B.; Antal, A.; Rothkegel, H.; Paulus, W. Increasing human leg motor cortex excitability by transcranial high frequency random noise stimulation. Restor. Neurol. Neurosci. 2014, 32, 403–410. [Google Scholar] [CrossRef]
- Miranda, P.C.; Lomarev, M.; Hallett, M. Modeling the current distribution during transcranial direct current stimulation. Clin. Neurophysiol. 2006, 117, 1623–1629. [Google Scholar] [CrossRef]
- Purpura, D.P.; McMurtry, J.G. INTRACELLULAR ACTIVITIES AND EVOKED POTENTIAL CHANGES DURING POLARIZATION OF MOTOR CORTEX. J. Neurophysiol. 1965, 28, 166–185. [Google Scholar] [CrossRef]
- Opitz, A.; Paulus, W.; Will, S.; Antunes, A.; Thielscher, A. Determinants of the electric field during transcranial direct current stimulation. NeuroImage 2015, 109, 140–150. [Google Scholar] [CrossRef]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Screening questionnaire before TMS: An update. Clin. Neurophysiol. 2011, 122, 1686. [Google Scholar] [CrossRef]
- Borckardt, J.J.; Nahas, Z.; Koola, J.; George, M.S. Estimating resting motor thresholds in transcranial magnetic stimulation research and practice: A computer simulation evaluation of best methods. J. ECT 2006, 22, 169–175. [Google Scholar] [CrossRef]
- Awiszus, F.; Borckardt, J.J. TMS Motor Threshold Assessment Tool (MTAT 2.0). 2011. Available online: https://www.clinicalresearcher.org/software.htm (accessed on 17 October 2014).
- Müller-Dahlhaus, J.F.M.; Orekhov, Y.; Liu, Y.; Ziemann, U. Interindividual variability and age-dependency of motor cortical plasticity induced by paired associative stimulation. Exp. Brain 2008, 187, 467–475. [Google Scholar] [CrossRef]
- Jamil, A.; Batsikadze, G.; Kuo, H.-I.; Labruna, L.; Hasan, A.; Paulus, W.; Nitsche, M.A. Systematic evaluation of the impact of stimulationintensity on neuroplastic after-effects induced bytranscranial direct current stimulation. J. Physiol. 2017, 595, 1273–1288. [Google Scholar] [CrossRef]
- Ridding, M.C.; Ziemann, U. Determinants of the induction of cortical plasticity by non-invasive brain stimulation in healthy subjects. J. Physiol. 2010, 588, 2291–2304. [Google Scholar] [CrossRef]
- Antal, A.; Terney, D.; Poreisz, C.; Paulus, W. Towards unravelling task-related modulations of neuroplastic changes induced in the human motor cortex. Eur. J. Neurosci. 2007, 26, 2687–2691. [Google Scholar] [CrossRef]
- Antonenko, D.; Thielscher, A.; Saturnino, G.B.; Aydin, S.; Ittermann, B.; Grittner, U.; Flöel, A. Towards precise brain stimulation: Is electric field simulation related to neuromodulation? Brain Stimul. 2019. [Google Scholar] [CrossRef]
- Foerster, A.S.; Rezaee, Z.; Paulus, W.; Nitsche, M.A.; Dutta, A. Effects of Cathode Location and the Size of Anode on Anodal Transcranial Direct Current Stimulation Over the Leg Motor Area in Healthy Humans. Front. Neurosci. 2018, 12, 443. [Google Scholar] [CrossRef]
- Seidel, O.; Ragert, P. Effects of Transcranial Direct Current Stimulation of Primary Motor Cortex on Reaction Time and Tapping Performance: A Comparison Between Athletes and Non-athletes. Front. Hum. Neurosci. 2019, 13, 103. [Google Scholar] [CrossRef]
- Ho, K.-A.; Taylor, J.L.; Chew, T.; Gálvez, V.; Alonzo, A.; Bai, S.; Dokos, S.; Loo, C.K.; Information, P.E.K.F.C. The Effect of Transcranial Direct Current Stimulation (tDCS) Electrode Size and Current Intensity on Motor Cortical Excitability: Evidence from Single and Repeated Sessions. Brain Stimul. 2016, 9, 1–7. [Google Scholar] [CrossRef]
- Iyer, M.B.; Mattu, U.; Grafman, J.; Lomarev, M.; Sato, S.; Wassermann, E.M. Safety and cognitive effect of frontal DC brain polarization in healthy individuals. Neurology 2005, 64, 872–875. [Google Scholar] [CrossRef]
- Madhavan, S.; Weber, K.A.; Stinear, J.W. Non-invasive brain stimulation enhances fine motor control of the hemiparetic ankle: Implications for rehabilitation. Exp. Brain Res. 2011, 209, 9–17. [Google Scholar] [CrossRef]
- Sriraman, A.; Oishi, T.; Madhavan, S. Timing-dependent priming effects of tDCS on ankle motor skill learning. Brain Res. 2014, 581, 23–29. [Google Scholar] [CrossRef]
- Biabani, M.; Farrell, M.; Zoghi, M.; Egan, G.; Jaberzadeh, S. The minimal number of TMS trials required for the reliable assessment of corticospinal excitability, short interval intracortical inhibition, and intracortical facilitation. Neurosci. Lett. 2018, 674, 94–100. [Google Scholar] [CrossRef]
- Fonteneau, C.; Mondino, M.; Arns, M.; Baeken, C.; Bikson, M.; Brunoni, A.R.; Burke, M.J.; Neuvonen, T.; Padberg, F.; Pascual-Leone, A.; et al. Sham tDCS: A hidden source of variability? Reflections for further blinded, controlled trials. Brain Stimul. 2019, 12, 668–673. [Google Scholar] [CrossRef]
- Fregni, F.; Boggio, P.S.; Mansur, C.G.; Wagner, T.; Ferreira, M.J.L.; Lima, M.C.; Rigonatti, S.P.; Marcolin, M.A.; Freedman, S.D.; Nitsche, M.A.; et al. Transcranial direct current stimulation of the unaffected hemisphere in stroke patients. NeuroReport 2005, 16, 1551–1555. [Google Scholar] [CrossRef]
- Mansur, C.G.; Fregni, F.; Boggio, P.S.; Riberto, M.; Gallucci-Neto, J.; Santos, C.M.; Wagner, T.; Rigonatti, S.P.; Marcolin, M.A.; Pascual-Leone, A. A sham stimulation controlled trial of rTMS of the unaffected hemiphere in stroke patients. Neurology 2005, 64, 1802–1804. [Google Scholar] [CrossRef]
- Bashir, S.; Varnet, M.; Najib, U.; Perez, J.; Alonso-Alonso, M.; Knobel, M.; Yoo, W.-K.; Edwards, D.; Pascual-Leone, A.; Vernet, M. Enhanced motor function and its neurophysiological correlates after navigated low-frequency repetitive transcranial magnetic stimulation over the contralesional motor cortex in stroke. Restor. Neurol. Neurosci. 2016, 34, 677–689. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Real Stimulation | Sham Stimulation | |||
|---|---|---|---|---|
| Left Hemisphere | Right Hemisphere | Left Hemisphere | Right Hemisphere | |
| Number | 11 | 11 | 11 | 11 |
| RMT (%MSO, Mean ± SEM) | 43 ± 3.1 | 42 ± 2.7 | 43 ± 2.2 | 42 ± 2.7 |
| Test Stim (%MSO, Mean ± SEM) | 52 ± 3.2 | 52 ± 3.3 | 52 ± 3.1 | 51 ± 4 |
| Baseline TA MEP (mV, Mean ± SEM) | 0.49 ± 0.05 | 0.42 ± 0.06 | 0.57 ± 0.05 | 0.51 ± 0.06 |
| Participant | Real tDCS | |
|---|---|---|
| Right TA | Left TA | |
| 1 | 0.99 | 0.94 |
| 2 | 1.80 † | 1.29 † |
| 3 | 1.89 † | 0.89 |
| 4 | 1.88 † | 2.13 † |
| 5 | 1.36 † | 1.50 † |
| 6 | 0.88 | 1.83 † |
| 7 | 0.97 | 0.86 |
| 8 | 0.88 | 0.87 |
| 9 | 0.96 | 1.31 † |
| 10 | 2.29 † | 1.72 † |
| 11 | 0.92 | 2.75 † |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghosh, S.; Hathorn, D.; Eisenhauer, J.; Dixon, J.; Cooper, I.D. Anodal Transcranial Direct Current Stimulation over the Vertex Enhances Leg Motor Cortex Excitability Bilaterally. Brain Sci. 2019, 9, 98. https://doi.org/10.3390/brainsci9050098
Ghosh S, Hathorn D, Eisenhauer J, Dixon J, Cooper ID. Anodal Transcranial Direct Current Stimulation over the Vertex Enhances Leg Motor Cortex Excitability Bilaterally. Brain Sciences. 2019; 9(5):98. https://doi.org/10.3390/brainsci9050098
Chicago/Turabian StyleGhosh, Soumya, David Hathorn, Jennifer Eisenhauer, Jesse Dixon, and Ian D. Cooper. 2019. "Anodal Transcranial Direct Current Stimulation over the Vertex Enhances Leg Motor Cortex Excitability Bilaterally" Brain Sciences 9, no. 5: 98. https://doi.org/10.3390/brainsci9050098
APA StyleGhosh, S., Hathorn, D., Eisenhauer, J., Dixon, J., & Cooper, I. D. (2019). Anodal Transcranial Direct Current Stimulation over the Vertex Enhances Leg Motor Cortex Excitability Bilaterally. Brain Sciences, 9(5), 98. https://doi.org/10.3390/brainsci9050098