Maternal Urinary Metal and Metalloid Concentrations in Association with Oxidative Stress Biomarkers


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
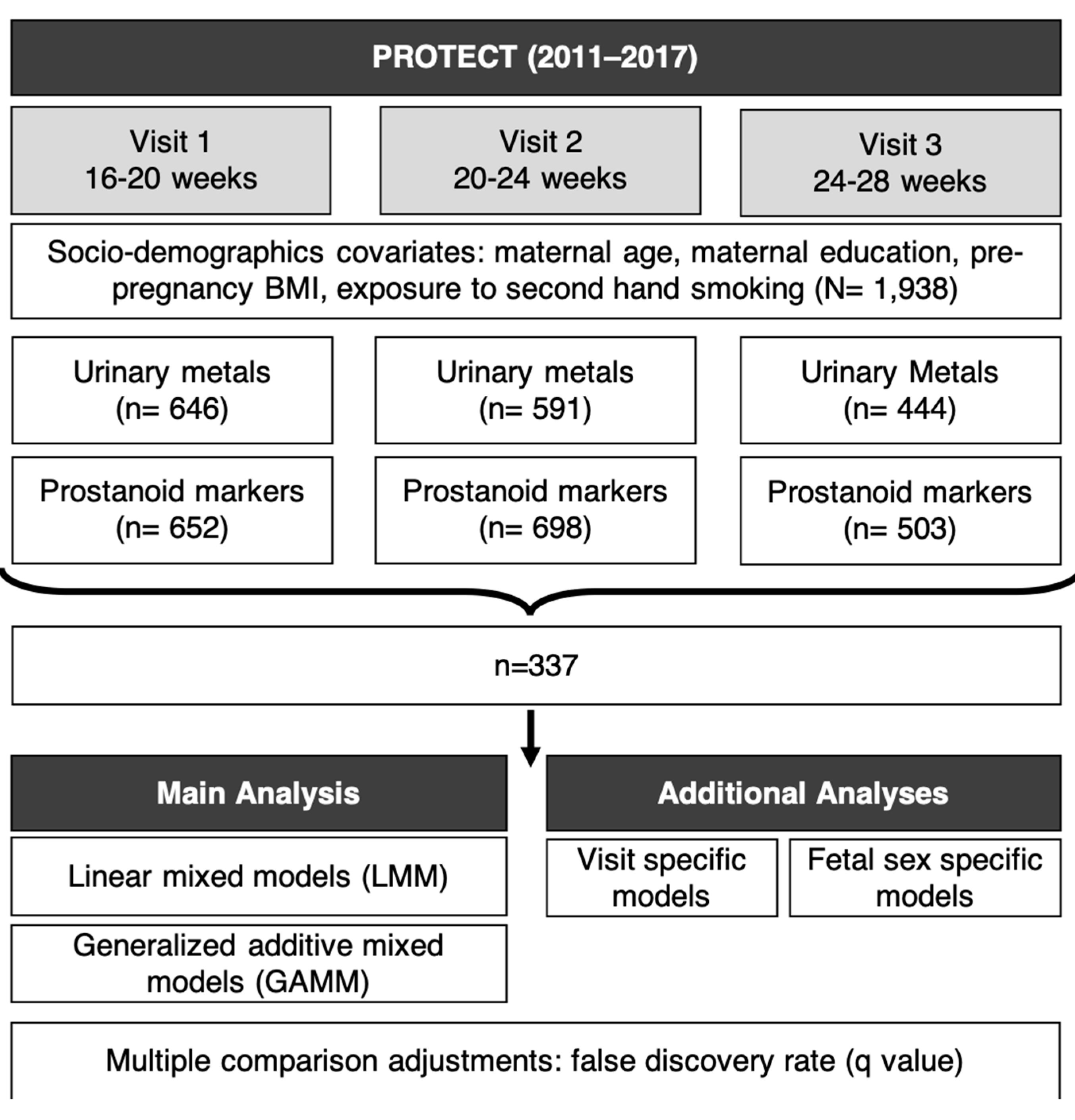
2.1. Study Population
2.2. Measurement of Metals
2.3. Measurement of Oxidative Stress Biomarkers
2.4. Statistical Methods
3. Results
3.1. Demographics
3.2. Descriptive Statistics
3.3. Urinary Metals and Prostanoids
3.4. Windows of Vulnerability Analysis
3.5. Sex-Specific Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, R.; Gautam, N.; Mishra, A.; Gupta, R. Heavy metals and living systems: An overview. Indian J. Pharmacol. 2011, 43, 246–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti-Kandarakis, E.; Bourguignon, J.P.; Giudice, L.C.; Hauser, R.; Prins, G.S.; Soto, A.M.; Zoeller, R.T.; Gore, A.C. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocr. Rev. 2009, 30, 293–342. [Google Scholar] [CrossRef] [PubMed]
- De Coster, S.; van Larebeke, N. Endocrine-disrupting chemicals: Associated disorders and mechanisms of action. J. Environ. Public Health 2012, 2012, 713696. [Google Scholar] [CrossRef] [PubMed]
- Mendiola, J.; Moreno, J.M.; Roca, M.; Vergara-Juarez, N.; Martinez-Garcia, M.J.; Garcia-Sanchez, A.; Elvira-Rendueles, B.; Moreno-Grau, S.; Lopez-Espin, J.J.; Ten, J.; et al. Relationships between heavy metal concentrations in three different body fluids and male reproductive parameters: A pilot study. Environ. Health 2011, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Bloom, M.S.; Parsons, P.J.; Steuerwald, A.J.; Schisterman, E.F.; Browne, R.W.; Kim, K.; Coccaro, G.A.; Conti, G.C.; Narayan, N.; Fujimoto, V.Y. Toxic trace metals and human oocytes during in vitro fertilization (IVF). Reprod. Toxicol. 2010, 29, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.P. Redefining oxidative stress. Antioxid. Redox Signal. 2006, 8, 1865–1879. [Google Scholar] [CrossRef]
- Moore, T.A.; Ahmad, I.M.; Zimmerman, M.C. Oxidative Stress and Preterm Birth: An Integrative Review. Biol. Res. Nurs. 2018, 20, 497–512. [Google Scholar] [CrossRef]
- Menon, R. Oxidative stress damage as a detrimental factor in preterm birth pathology. Front. Immunol. 2014, 5, 567. [Google Scholar] [CrossRef]
- Peter Stein, T.; Scholl, T.O.; Schluter, M.D.; Leskiw, M.J.; Chen, X.; Spur, B.W.; Rodriguez, A. Oxidative stress early in pregnancy and pregnancy outcome. Free Radic. Res. 2008, 42, 841–848. [Google Scholar] [CrossRef]
- Sharma, J.; Sharma, A.; Bahadur, A.; Vimala, N.; Satyam, A.; Mittal, S. Oxidative stress markers and antioxidant levels in normal pregnancy and pre-eclampsia. Int. J. Gynecol. Obstet. 2006, 94, 23–27. [Google Scholar] [CrossRef]
- Mert, I.; Oruc, A.S.; Yuksel, S.; Cakar, E.S.; Buyukkagnici, U.; Karaer, A.; Danisman, N. Role of oxidative stress in preeclampsia and intrauterine growth restriction. J. Obstet. Gynaecol. Res. 2012, 38, 658–664. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Oxidative stress. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 287–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, K.K.; Cantonwine, D.E.; McElrath, T.F.; Mukherjee, B.; Meeker, J.D. Repeated measures analysis of associations between urinary bisphenol-A concentrations and biomarkers of inflammation and oxidative stress in pregnancy. Reprod. Toxicol. 2016, 66, 93–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, K.K.; Chen, Y.H.; VanderWeele, T.J.; McElrath, T.F.; Meeker, J.D.; Mukherjee, B. Mediation of the Relationship between Maternal Phthalate Exposure and Preterm Birth by Oxidative Stress with Repeated Measurements across Pregnancy. Environ. Health Perspect. 2017, 125, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.M.; van ’t Erve, T.J.; Boss, J.; Sathyanarayana, S.; Barrett, E.S.; Nguyen, R.H.N.; Bush, N.R.; Milne, G.L.; McElrath, T.F.; Swan, S.H.; et al. Urinary oxidative stress biomarkers and accelerated time to spontaneous delivery. Free Radic. Biol. Med. 2019, 130, 419–425. [Google Scholar] [CrossRef]
- Longini, M.; Perrone, S.; Vezzosi, P.; Marzocchi, B.; Kenanidis, A.; Centini, G.; Rosignoli, L.; Buonocore, G. Association between oxidative stress in pregnancy and preterm premature rupture of membranes. Clin. Biochem. 2007, 40, 793–797. [Google Scholar] [CrossRef]
- Mestan, K.; Matoba, N.; Arguelles, L.; Harvey, C.; Ernst, L.M.; Farrow, K.; Wang, X. Cord blood 8-isoprostane in the preterm infant. Early Hum. Dev. 2012, 88, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Eick, S.M.; Ferguson, K.K.; Milne, G.L.; Rios-McConnell, R.; Velez-Vega, C.; Rosario, Z.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Repeated measures of urinary oxidative stress biomarkers and preterm birth in Puerto Rico. Free Radic. Biol. Med. 2020, 146, 299–305. [Google Scholar] [CrossRef]
- Valko, M.; Morris, H.; Cronin, M.T. Metals, toxicity and oxidative stress. Curr. Med. Chem. 2005, 12, 1161–1208. [Google Scholar] [CrossRef] [Green Version]
- Alfanie, I.; Muhyi, R.; Suhartono, E. Effect of Heavy Metal on Malondialdehyde and Advanced Oxidation Protein Products Cencentration A Focus on Arsenic, Cadmium, and Mercury. J. Med. Bioeng. 2015, 4, 1–6. [Google Scholar]
- Betteridge, D.J. What is oxidative stress? Metabolism 2000, 49, 3–8. [Google Scholar] [CrossRef]
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M.S.H. Prevalence of exposure of heavy metals and their impact on health consequences. J. Cell. Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef] [PubMed]
- Singh, L.; Agarwal, P.; Anand, M.; Taneja, A. Toxic and essential metals in placenta and its relation with lipid peroxides/glutathione status in pre-term and full-term deliveries. Asian J. Med. Sci. 2015, 7, 34–39. [Google Scholar] [CrossRef] [Green Version]
- Ahamed, M.; Mehrotra, P.K.; Kumar, P.; Siddiqui, M.K. Placental lead-induced oxidative stress and preterm delivery. Environ. Toxicol. Pharmacol. 2009, 27, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Quig, D. Cysteine metabolism and metal toxicity. Altern. Med. Rev. 1998, 3, 262–270. [Google Scholar] [PubMed]
- Dashner-Titus, E.J.; Hoover, J.; Li, L.; Lee, J.H.; Du, R.; Liu, K.J.; Traber, M.G.; Ho, E.; Lewis, J.; Hudson, L.G. Metal exposure and oxidative stress markers in pregnant Navajo Birth Cohort Study participants. Free Radic. Biol. Med. 2018, 124, 484–492. [Google Scholar] [CrossRef]
- Jan, A.T.; Azam, M.; Siddiqui, K.; Ali, A.; Choi, I.; Haq, Q.M. Heavy Metals and Human Health: Mechanistic Insight into Toxicity and Counter Defense System of Antioxidants. Int. J. Mol. Sci. 2015, 16, 29592–29630. [Google Scholar] [CrossRef] [Green Version]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, mechanism and health effects of some heavy metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar] [CrossRef] [Green Version]
- Andrews, K.W.; Savitz, D.A.; Hertz-Picciotto, I. Prenatal lead exposure in relation to gestational age and birth weight: A review of epidemiologic studies. Am. J. Ind. Med. 1994, 26, 13–32. [Google Scholar] [CrossRef]
- Stodden, R.A.; Ianacone, R.N. Career/vocational assessment of the special needs individual: A conceptual model. Except. Child. 1981, 47, 600–608. [Google Scholar] [CrossRef]
- Perkins, M.; Wright, R.O.; Amarasiriwardena, C.J.; Jayawardene, I.; Rifas-Shiman, S.L.; Oken, E. Very low maternal lead level in pregnancy and birth outcomes in an eastern Massachusetts population. Ann. Epidemiol. 2014, 24, 915–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Sanchez, L.E.; Berkowitz, G.; Lopez-Carrillo, L.; Torres-Arreola, L.; Rios, C.; Lopez-Cervantes, M. Intrauterine lead exposure and preterm birth. Environ. Res. 1999, 81, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Cantonwine, D.; Hu, H.; Sanchez, B.N.; Lamadrid-Figueroa, H.; Smith, D.; Ettinger, A.S.; Mercado-Garcia, A.; Hernandez-Avila, M.; Wright, R.O.; Tellez-Rojo, M.M. Critical windows of fetal lead exposure: Adverse impacts on length of gestation and risk of premature delivery. J. Occup. Environ. Med. 2010, 52, 1106–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Zhang, B.; Huo, W.; Cao, Z.; Liu, W.; Liao, J.; Xia, W.; Xu, S.; Li, Y. Fetal exposure to lead during pregnancy and the risk of preterm and early-term deliveries. Int. J. Hyg. Environ. Health 2017, 220, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Huo, W.; Zhang, B.; Zheng, T.; Li, Y.; Pan, X.; Liu, W.; Chang, H.; Jiang, M.; Zhou, A.; et al. Maternal urinary cadmium concentrations in relation to preterm birth in the Healthy Baby Cohort Study in China. Environ. Int. 2016, 94, 300–306. [Google Scholar] [CrossRef]
- Wang, H.; Liu, L.; Hu, Y.F.; Hao, J.H.; Chen, Y.H.; Su, P.Y.; Yu, Z.; Fu, L.; Tao, F.B.; Xu, D.X. Association of maternal serum cadmium level during pregnancy with risk of preterm birth in a Chinese population. Environ. Pollut. 2016, 216, 851–857. [Google Scholar] [CrossRef]
- Tsuji, M.; Shibata, E.; Morokuma, S.; Tanaka, R.; Senju, A.; Araki, S.; Sanefuji, M.; Koriyama, C.; Yamamoto, M.; Ishihara, Y.; et al. The association between whole blood concentrations of heavy metals in pregnant women and premature births: The Japan Environment and Children’s Study (JECS). Environ. Res. 2018, 166, 562–569. [Google Scholar] [CrossRef]
- Ashrap, P.; Watkins, D.J.; Mukherjee, B.; Boss, J.; Richards, M.J.; Rosario, Z.; Velez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Maternal blood metal and metalloid concentrations in association with birth outcomes in Northern Puerto Rico. Environ. Int. 2020, 138, 105606. [Google Scholar] [CrossRef]
- Zoroddu, M.A.; Aaseth, J.; Crisponi, G.; Medici, S.; Peana, M.; Nurchi, V.M. The essential metals for humans: A brief overview. J. Inorg. Biochem. 2019, 195, 120–129. [Google Scholar] [CrossRef]
- Lewicka, I.; Kocylowski, R.; Grzesiak, M.; Gaj, Z.; Oszukowski, P.; Suliburska, J. Selected trace elements concentrations in pregnancy and their possible role - literature review. Ginekol. Pol. 2017, 88, 509–514. [Google Scholar] [CrossRef]
- Jablonska, E.; Vinceti, M. Selenium and human health: Witnessing a Copernican revolution? J. Environ. Sci. Health Part C 2015, 33, 328–368. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Jomova, K.; Rhodes, C.J.; Kuča, K.; Musílek, K. Redox-and non-redox-metal-induced formation of free radicals and their role in human disease. Arch. Toxicol. 2016, 90, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Meeker, J.D.; Keil, A.P.; Aung, M.T.; Bommarito, P.A.; Cantonwine, D.E.; McElrath, T.F.; Ferguson, K.K. Exposure to 17 trace metals in pregnancy and associations with urinary oxidative stress biomarkers. Environ. Res. 2019, 179, 108854. [Google Scholar] [CrossRef] [PubMed]
- Cantonwine, D.E.; Cordero, J.F.; Rivera-Gonzalez, L.O.; Anzalota Del Toro, L.V.; Ferguson, K.K.; Mukherjee, B.; Calafat, A.M.; Crespo, N.; Jimenez-Velez, B.; Padilla, I.Y.; et al. Urinary phthalate metabolite concentrations among pregnant women in Northern Puerto Rico: Distribution, temporal variability, and predictors. Environ. Int. 2014, 62, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Meeker, J.D.; Cantonwine, D.E.; Rivera-Gonzalez, L.O.; Ferguson, K.K.; Mukherjee, B.; Calafat, A.M.; Ye, X.; Anzalota Del Toro, L.V.; Crespo-Hernandez, N.; Jimenez-Velez, B.; et al. Distribution, variability, and predictors of urinary concentrations of phenols and parabens among pregnant women in Puerto Rico. Environ. Sci. Technol. 2013, 47, 3439–3447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashrap, P.; Watkins, D.J.; Calafat, A.M.; Ye, X.; Rosario, Z.; Brown, P.; Velez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Elevated concentrations of urinary triclocarban, phenol and paraben among pregnant women in Northern Puerto Rico: Predictors and trends. Environ. Int. 2018, 121, 990–1002. [Google Scholar] [CrossRef] [PubMed]
- Watkins, D.J.; Ferguson, K.K.; Anzalota Del Toro, L.V.; Alshawabkeh, A.N.; Cordero, J.F.; Meeker, J.D. Associations between urinary phenol and paraben concentrations and markers of oxidative stress and inflammation among pregnant women in Puerto Rico. Int. J. Hyg. Environ. Health 2015, 218, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.S.; Meeker, J.D.; Carroll, R.; Zhao, S.; Mourgas, M.J.; Richards, M.J.; Aung, M.; Cantonwine, D.E.; McElrath, T.F.; Ferguson, K.K. Urinary trace metals individually and in mixtures in association with preterm birth. Environ. Int. 2018, 121, 582–590. [Google Scholar] [CrossRef]
- Morales, C.R.; Terry, E.S.; Zackert, W.E.; Montine, T.J.; Morrow, J.D. Improved assay for the quantification of the major urinary metabolite of the isoprostane 15-F(2t)-Isoprostane (8-iso-PGF(2alpha)) by a stable isotope dilution mass spectrometric assay. Clin. Chim. Acta 2001, 314, 93–99. [Google Scholar] [CrossRef]
- Morrow, J.D.; Roberts, L.J., 2nd. Mass spectrometric quantification of F2-isoprostanes in biological fluids and tissues as measure of oxidant stress. Methods Enzymol. 1999, 300, 3–12. [Google Scholar]
- Milne, G.L.; Sanchez, S.C.; Musiek, E.S.; Morrow, J.D. Quantification of F2-isoprostanes as a biomarker of oxidative stress. Nat. Protoc. 2007, 2, 221–226. [Google Scholar] [CrossRef]
- Roberts, L.J.; Morrow, J.D. Measurement of F(2)-isoprostanes as an index of oxidative stress in vivo. Free Radic. Biol. Med. 2000, 28, 505–513. [Google Scholar] [CrossRef]
- Awad, J.A.; Morrow, J.D.; Takahashi, K.; Roberts, L.J., 2nd. Identification of non-cyclooxygenase-derived prostanoid (F2-isoprostane) metabolites in human urine and plasma. J. Biol. Chem. 1993, 268, 4161–4169. [Google Scholar] [CrossRef]
- van ’t Erve, T.J.; Lih, F.B.; Kadiiska, M.B.; Deterding, L.J.; Eling, T.E.; Mason, R.P. Reinterpreting the best biomarker of oxidative stress: The 8-iso-PGF(2alpha)/PGF(2alpha) ratio distinguishes chemical from enzymatic lipid peroxidation. Free Radic. Biol. Med. 2015, 83, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van’t Erve, T.J.; Lih, F.B.; Jelsema, C.; Deterding, L.J.; Eling, T.E.; Mason, R.P.; Kadiiska, M.B. Reinterpreting the best biomarker of oxidative stress: The 8-iso-prostaglandin F2alpha/prostaglandin F2alpha ratio shows complex origins of lipid peroxidation biomarkers in animal models. Free Radic. Biol. Med. 2016, 95, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Eriksson, M. Lipid peroxidation induced by an early inflammatory response in endotoxaemia. Acta Anaesthesiol. Scand. 2000, 44, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K. Does the interdependence between oxidative stress and inflammation explain the antioxidant paradox? Oxidative Med. Cell. Longev. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van ’t Erve, T.J.; Lih, F.B.; Kadiiska, M.B.; Deterding, L.J.; Mason, R.P. Elevated plasma 8-iso-prostaglandin F2alpha levels in human smokers originate primarily from enzymatic instead of non-enzymatic lipid peroxidation. Free Radic. Biol. Med. 2018, 115, 105–112. [Google Scholar] [CrossRef]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the U.S. population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Ingle, M.E.; Watkins, D.; Rosario, Z.; VelezVega, C.M.; Calafat, A.M.; Ospina, M.; Ferguson, K.K.; Cordero, J.F.; Alshawabkeh, A.; Meeker, J.D. An exploratory analysis of urinary organophosphate ester metabolites and oxidative stress among pregnant women in Puerto Rico. Sci. Total Environ. 2020, 703, 134798. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Aker, A.M.; Ferguson, K.K.; Rosario, Z.Y.; Mukherjee, B.; Alshawabkeh, A.N.; Cordero, J.F.; Meeker, J.D. The associations between prenatal exposure to triclocarban, phenols and parabens with gestational age and birth weight in northern Puerto Rico. Environ. Res. 2019, 169, 41–51. [Google Scholar] [CrossRef]
- Ashrap, P.; Watkins, D.J.; Mukherjee, B.; Boss, J.; Richards, M.J.; Rosario, Z.; Velez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Predictors of urinary and blood Metal(loid) concentrations among pregnant women in Northern Puerto Rico. Environ. Res. 2020, 183, 109178. [Google Scholar] [CrossRef]
- Chang, K.L.; Hung, T.C.; Hsieh, B.S.; Chen, Y.H.; Chen, T.F.; Cheng, H.L. Zinc at pharmacologic concentrations affects cytokine expression and induces apoptosis of human peripheral blood mononuclear cells. Nutrition 2006, 22, 465–474. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Manganese; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2012.
- CDC. Guidelines for the Identification and Management of Lead Exposure in Pregnant and Lactating Women; National Center for Environmental Health: Washington, DC, USA, 2010.
- Ye, B.-J.; Kim, B.-G.; Jeon, M.-J.; Kim, S.-Y.; Kim, H.-C.; Jang, T.-W.; Chae, H.-J.; Choi, W.-J.; Ha, M.-N.; Hong, Y.-S. Evaluation of mercury exposure level, clinical diagnosis and treatment for mercury intoxication. Ann. Occup. Environ. Med. 2016, 28. [Google Scholar] [CrossRef] [Green Version]
- Basu, S.; Eriksson, M. Oxidative injury and survival during endotoxemia. FEBS Lett. 1998, 438, 159–160. [Google Scholar] [CrossRef] [Green Version]
- Basu, S. Oxidative injury induced cyclooxygenase activation in experimental hepatotoxicity. Biochem. Biophys. Res. Commun. 1999, 254, 764–767. [Google Scholar] [CrossRef]
- Fort, M.; Cosin-Tomas, M.; Grimalt, J.O.; Querol, X.; Casas, M.; Sunyer, J. Assessment of exposure to trace metals in a cohort of pregnant women from an urban center by urine analysis in the first and third trimesters of pregnancy. Environ. Sci. Pollut. Res. Int. 2014, 21, 9234–9241. [Google Scholar] [CrossRef] [Green Version]
- Hinwood, A.L.; Stasinska, A.; Callan, A.C.; Heyworth, J.; Ramalingam, M.; Boyce, M.; McCafferty, P.; Odland, J.O. Maternal exposure to alkali, alkali earth, transition and other metals: Concentrations and predictors of exposure. Environ. Pollut. 2015, 204, 256–263. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Cesium; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2004.
- Atapaththu, K.S.; Rashid, M.H.; Asaeda, T. Growth and Oxidative Stress of Brittlewort (Nitella pseudoflabellata) in Response to Cesium Exposure. Bull. Environ. Contam. Toxicol. 2016, 96, 347–353. [Google Scholar] [CrossRef]
- Sahr, T.; Voigt, G.; Paretzke, H.G.; Schramel, P.; Ernst, D. Caesium-affected gene expression in Arabidopsis thaliana. New Phytol. 2005, 165, 747–754. [Google Scholar] [CrossRef]
- Callan, A.C.; Hinwood, A.L.; Ramalingam, M.; Boyce, M.; Heyworth, J.; McCafferty, P.; Odland, J.O. Maternal exposure to metals—concentrations and predictors of exposure. Environ. Res. 2013, 126, 111–117. [Google Scholar] [CrossRef]
- Shirai, S.; Suzuki, Y.; Yoshinaga, J.; Mizumoto, Y. Maternal exposure to low-level heavy metals during pregnancy and birth size. J. Environ. Sci. Health Part A 2010, 45, 1468–1474. [Google Scholar] [CrossRef]
- Uauy, R.; Olivares, M.; Gonzalez, M. Essentiality of copper in humans. Am. J. Clin. Nutr. 1998, 67, 952S–959S. [Google Scholar] [CrossRef]
- Turnlund, J. Copper nutriture, bioavailability, and the influence of dietary factors. J. Am. Diet. Assoc. 1988, 88, 303–308. [Google Scholar]
- Gaetke, L.M.; Chow, C.K. Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology 2003, 189, 147–163. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Copper; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2004.
- Thounaojam, T.C.; Panda, P.; Mazumdar, P.; Kumar, D.; Sharma, G.; Sahoo, L.; Sanjib, P. Excess copper induced oxidative stress and response of antioxidants in rice. Plant Physiol. Biochem. 2012, 53, 33–39. [Google Scholar] [CrossRef]
- Bremner, I. Manifestations of copper excess. Am. J. Clin. Nutr. 1998, 67, 1069S–1073S. [Google Scholar] [CrossRef]
- Kadiiska, M.B.; Hanna, P.M.; Jordan, S.J.; Mason, R.P. Electron spin resonance evidence for free radical generation in copper-treated vitamin E-and selenium-deficient rats: In vivo spin-trapping investigation. Mol. Pharmacol. 1993, 44, 222–227. [Google Scholar]
- Jomova, K.; Baros, S.; Valko, M. Redox active metal-induced oxidative stress in biological systems. Transit. Met. Chem. 2012, 37, 127–134. [Google Scholar] [CrossRef]
- King, J.C. Physiology of pregnancy and nutrient metabolism. Am. J. Clin. Nutr. 2000, 71, 1218S–1225S. [Google Scholar] [CrossRef] [Green Version]
- Weaver, V.M.; Vargas, G.G.; Silbergeld, E.K.; Rothenberg, S.J.; Fadrowski, J.J.; Rubio-Andrade, M.; Parsons, P.J.; Steuerwald, A.J.; Navas-Acien, A.; Guallar, E. Impact of urine concentration adjustment method on associations between urine metals and estimated glomerular filtration rates (eGFR) in adolescents. Environ. Res. 2014, 132, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Cheung, K.L.; Lafayette, R.A. Renal physiology of pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Hytten, F.E.; Paintin, D.B. Increase in plasma volume during normal pregnancy. J. Obstet. Gynaecol. Br. Emp. 1963, 70, 402–407. [Google Scholar] [CrossRef]
- Al-Qaraghouli, M.; Fang, Y.M.V. Effect of Fetal Sex on Maternal and Obstetric Outcomes. Front. Pediatr. 2017, 5, 144. [Google Scholar] [CrossRef] [Green Version]
- DiPietro, J.A.; Voegtline, K.M. The gestational foundation of sex differences in development and vulnerability. Neuroscience 2017, 342, 4–20. [Google Scholar] [CrossRef] [Green Version]
- Fontaine, C.J.; Patten, A.R.; Sickmann, H.M.; Helfer, J.L.; Christie, B.R. Effects of pre-natal alcohol exposure on hippocampal synaptic plasticity: Sex, age and methodological considerations. Neurosci. Biobehav. Rev. 2016, 64, 12–34. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Perera, F.; Mrozek-Budzyn, D.; Mroz, E.; Flak, E.; Spengler, J.D.; Edwards, S.; Jacek, R.; Kaim, I.; Skolicki, Z. Gender differences in fetal growth of newborns exposed prenatally to airborne fine particulate matter. Environ. Res. 2009, 109, 447–456. [Google Scholar] [CrossRef] [Green Version]
- Wolff, M.S.; Engel, S.M.; Berkowitz, G.S.; Ye, X.; Silva, M.J.; Zhu, C.; Wetmur, J.; Calafat, A.M. Prenatal phenol and phthalate exposures and birth outcomes. Environ. Health Perspect. 2008, 116, 1092–1097. [Google Scholar] [CrossRef]
- Cowell, W.J.; Wright, R.J. Sex-specific effects of combined exposure to chemical and non-chemical stressors on neuroendocrine development: A review of recent findings and putative mechanisms. Curr. Environ. Health Rep. 2017, 4, 415–425. [Google Scholar] [CrossRef]
- Aiken, C.E.; Ozanne, S.E. Sex differences in developmental programming models. Reproduction 2013, 145, R1–R13. [Google Scholar] [CrossRef] [Green Version]
- Murphy, V.E.; Smith, R.; Giles, W.B.; Clifton, V.L. Endocrine regulation of human fetal growth: The role of the mother, placenta, and fetus. Endocr. Rev. 2006, 27, 141–169. [Google Scholar] [CrossRef]
- Clifton, V.L. Review: Sex and the human placenta: Mediating differential strategies of fetal growth and survival. Placenta 2010, 31, S33–S39. [Google Scholar] [CrossRef]
- Basu, S. Review isoprostanes: Novel bioactive products of lipid peroxidation. Free Radic. Res. 2004, 38, 105–122. [Google Scholar] [CrossRef]
- Morris, J.M.; Gopaul, N.K.; Endresen, M.J.; Knight, M.; Linton, E.A.; Dhir, S.; Ängård, E.E.; Redman, C.W. Circulating markers of oxidative stress are raised in normal pregnancy and pre-eclampsia. BJOG Int. J. Obstet. Gynaecol. 1998, 105, 1195–1199. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) | |
|---|---|---|
| maternal age | 26.7 (5.5) | |
| Characteristic | Category | Count (Percent) |
| Insurance type | private | 124 (57.7%) |
| public (mi salud) | 80 (37.2%) | |
| missing | 11 (5.1%) | |
| maternal education | ≤high school/ged | 50 (23.3%) |
| some college or technical school | 73 (34%) | |
| college degree | 64 (29.8%) | |
| master’s degree or higher | 26 (12.1%) | |
| missing | 2 (0.9%) | |
| household income | <$10,000 | 59 (27.4%) |
| ≥$10,000 to <$30,000 | 60 (27.9%) | |
| ≥$30,000 to <$50,000 | 42 (19.5%) | |
| ≥$50,000 | 25 (11.6%) | |
| missing | 29 (13.5%) | |
| marital status | single | 51 (23.7%) |
| married or living together | 162 (75.3%) | |
| missing | 2 (0.9%) | |
| parity (# birth) | 0 | 84 (39.1%) |
| 1 | 77 (35.8%) | |
| >1 | 52 (24.2%) | |
| missing | 2 (0.9%) | |
| infant sex | female | 88 (40.9%) |
| male | 114 (53%) | |
| missing | 13 (6%) | |
| prepregnancy BMI (kg m−2) | ≤25 | 105 (48.8%) |
| >25 to ≤30 | 66 (30.7%) | |
| >30 | 33 (15.3%) | |
| missing | 11 (5.1%) | |
| employment status | employed | 123 (57.2%) |
| unemployed | 90 (41.9%) | |
| missing | 2 (0.9%) | |
| smoking | never | 174 (80.9%) |
| ever | 36 (16.7%) | |
| current | 3 (1.4%) | |
| missing | 2 (0.9%) | |
| exposure to secondhand smoking | none | 186 (86.5%) |
| up to 1 h | 8 (3.7%) | |
| more than 1 h | 14 (6.5%) | |
| missing | 7 (3.3%) | |
| alcohol consumption | none | 92 (42.8%) |
| before pregnancy | 109 (50.7%) | |
| within the last few months | 12 (5.6%) | |
| missing | 2 (0.9%) | |
| Metal(loid) 2 | LOD | % >LOD | GM | GSD | 25% | 50% | 75% | 95% | Max |
|---|---|---|---|---|---|---|---|---|---|
| Co | 0.05 | 100 | 1.1 | 1.6 | 0.80 | 1.0 | 1.4 | 2.6 | 8.2 |
| Cs | 0.01 | 100 | 5.4 | 1.4 | 4.3 | 5.3 | 6.6 | 10.0 | 18.4 |
| Cu | 2.5 | 99.3 | 15.3 | 1.5 | 11.9 | 14.9 | 18.7 | 32.0 | 149 |
| Mn | 0.08 | 100 | 1.4 | 1.6 | 1.08 | 1.4 | 1.7 | 3.1 | 31.6 |
| Mo | 0.3 | 100 | 61.9 | 1.7 | 44.7 | 63.3 | 84.3 | 147.6 | 307 |
| Sb | 0.04 | 90 | 0.09 | 1.8 | 0.07 | 0.09 | 0.13 | 0.23 | 1.2 |
| Sn | 0.1 | 100 | 2.0 | 2.6 | 1.0 | 1.7 | 3.2 | 11.2 | 81.4 |
| Zn | 2 | 100 | 301 | 1.9 | 203 | 327 | 481 | 798 | 2136 |
| As | 0.3 | 100 | 11.3 | 2.2 | 6.6 | 10.9 | 17.8 | 43.1 | 128 |
| Ba | 0.1 | 99.3 | 2.4 | 2.4 | 1.4 | 2.4 | 4.4 | 10.2 | 35 |
| Cd | 0.06 | 74.5 | 0.13 | 2.3 | 0.07 | 0.12 | 0.20 | 0.59 | 7.6 |
| Hg | 0.05 | 98.6 | 0.56 | 2.7 | 0.30 | 0.58 | 1.1 | 2.8 | 13.6 |
| Ni | 0.8 | 98.9 | 5.1 | 1.7 | 3.8 | 5.2 | 7.1 | 12.3 | 32 |
| Pb | 0.1 | 72.1 | 0.24 | 2.4 | 0.1 | 0.26 | 0.41 | 1.0 | 4.6 |
| Oxidative stress Biomarkers 2 | % >LOD | GM | GSD | 25% | 50% | 75% | 95% | Max | |
| 8-iso-PGF2α | 100 | 1.8 | 1.9 | 1.3 | 2.0 | 2.9 | 4.6 | 11.7 | |
| 8-iso-PGF2α metabolite | 100 | 0.91 | 1.8 | 0.62 | 0.93 | 1.4 | 2.2 | 7.1 | |
| PGF2α | 100 | 2.8 | 2.1 | 1.9 | 2.9 | 4.5 | 8.3 | 40.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashrap, P.; Watkins, D.J.; Milne, G.L.; Ferguson, K.K.; Loch-Caruso, R.; Fernandez, J.; Rosario, Z.; Vélez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; et al. Maternal Urinary Metal and Metalloid Concentrations in Association with Oxidative Stress Biomarkers. Antioxidants 2021, 10, 114. https://doi.org/10.3390/antiox10010114
Ashrap P, Watkins DJ, Milne GL, Ferguson KK, Loch-Caruso R, Fernandez J, Rosario Z, Vélez-Vega CM, Alshawabkeh A, Cordero JF, et al. Maternal Urinary Metal and Metalloid Concentrations in Association with Oxidative Stress Biomarkers. Antioxidants. 2021; 10(1):114. https://doi.org/10.3390/antiox10010114
Chicago/Turabian StyleAshrap, Pahriya, Deborah J. Watkins, Ginger L. Milne, Kelly K. Ferguson, Rita Loch-Caruso, Jennifer Fernandez, Zaira Rosario, Carmen M. Vélez-Vega, Akram Alshawabkeh, José F. Cordero, and et al. 2021. "Maternal Urinary Metal and Metalloid Concentrations in Association with Oxidative Stress Biomarkers" Antioxidants 10, no. 1: 114. https://doi.org/10.3390/antiox10010114
APA StyleAshrap, P., Watkins, D. J., Milne, G. L., Ferguson, K. K., Loch-Caruso, R., Fernandez, J., Rosario, Z., Vélez-Vega, C. M., Alshawabkeh, A., Cordero, J. F., & Meeker, J. D. (2021). Maternal Urinary Metal and Metalloid Concentrations in Association with Oxidative Stress Biomarkers. Antioxidants, 10(1), 114. https://doi.org/10.3390/antiox10010114