
Renoprotective Effects of DPP-4 Inhibitors


Abstract
:1. Introduction
2. DPP-4 in Kidney
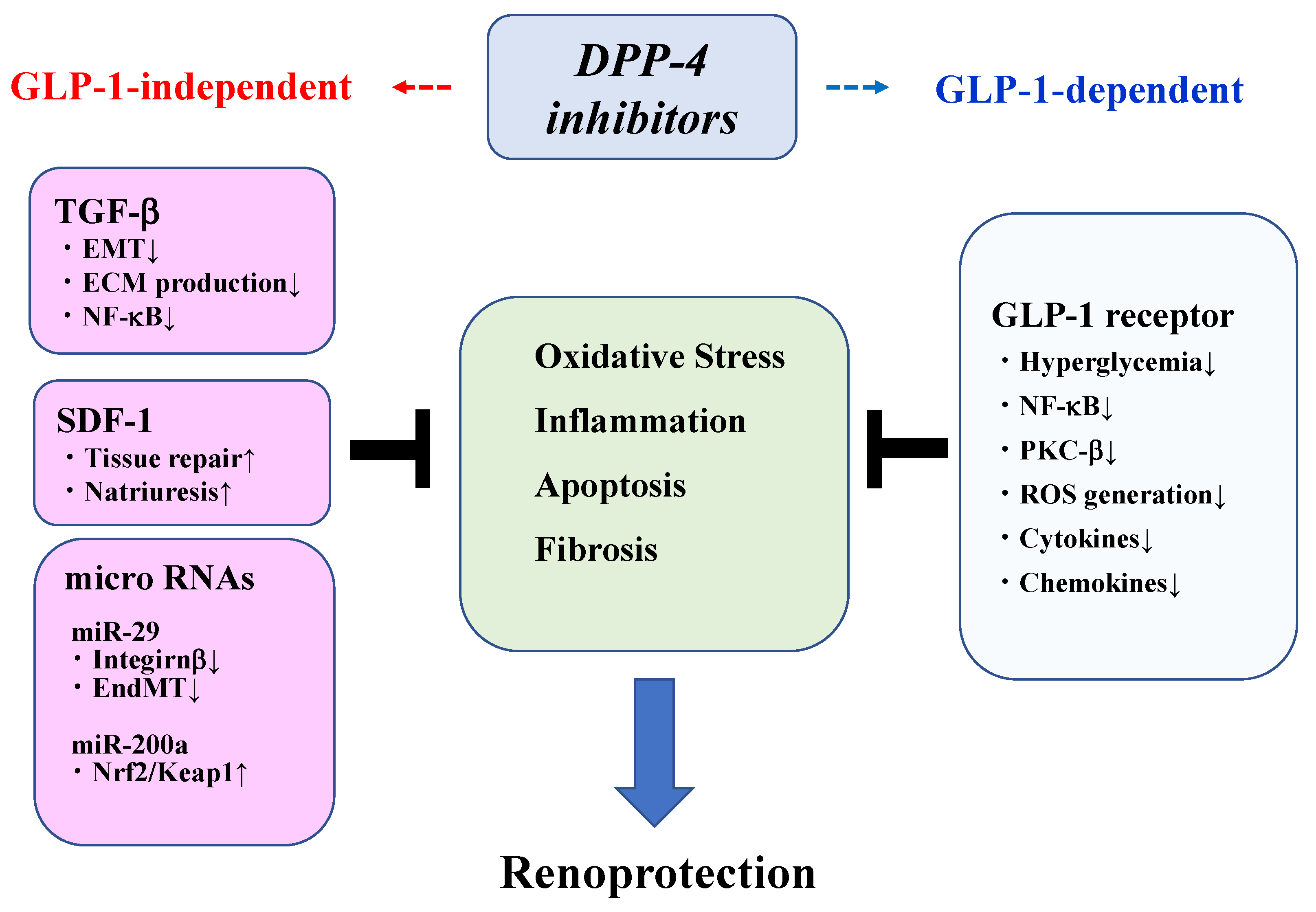
3. Mechanisms Underlying Renoprotection by DPP-4 Inhibitors
3.1. Oxidative Stress/Inflammation
3.2. Natriuresis
3.3. Fibrosis
4. DPP-4 Substrates
4.1. BNP
4.2. Erythropoietin
4.3. NPY
4.4. SDF-1
5. Preclinical Studies
5.1. Diabetic Animal Models
5.2. Non-Diabetic CKD Models
5.3. GLP-1R-Deficient Mice
6. Clinical Trials on Renal Outcomes
6.1. Linagliptin
6.2. Saxagliptin
6.3. Sitagliptin
6.4. Alogliptin
6.5. Vildagliptin
6.6. Anagliptin
6.7. Teneligliptin
7. Meta-Analysis of DPP-4 Inhibitors on Renal Outcomes
8. Safety and Efficacy of DPP-4 Inhibitors in Patients with an Impaired Renal Function
9. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Waldrop, G.; Zhong, J.; Peters, M.; Rajagopalan, S. Incretin-Based Therapy for Diabetes: What a Cardiologist Needs to Know. J. Am. Coll. Cardiol. 2016, 67, 1488–1496. [Google Scholar] [CrossRef]
- Mulvihill, E.E.; Drucker, D.J. Pharmacology, physiology, and mechanisms of action of dipeptidyl peptidase-4 inhibitors. Endocr. Rev. 2014, 35, 992–1019. [Google Scholar] [CrossRef] [Green Version]
- Enz, N.; Vliegen, G.; De Meester, I.; Jungraithmayr, W. CD26/DPP4—A potential biomarker and target for cancer therapy. Pharmacol. Ther. 2019, 198, 135–159. [Google Scholar] [CrossRef]
- Deacon, C.F. Physiology and Pharmacology of DPP-4 in Glucose Homeostasis and the Treatment of Type 2 Diabetes. Front. Endocrinol. 2019, 10, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seino, Y.; Fukushima, M.; Yabe, D. GIP and GLP-1, the two incretin hormones: Similarities and differences. J. Diabetes Investig. 2010, 1, 8–23. [Google Scholar] [CrossRef] [Green Version]
- Seino, Y.; Yabe, D. Glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1: Incretin actions beyond the pancreas. J. Diabetes Investig. 2013, 4, 108–130. [Google Scholar] [CrossRef] [Green Version]
- Zhuge, F.; Ni, Y.; Nagashimada, M.; Nagata, N.; Xu, L.; Mukaida, N.; Kaneko, S.; Ota, T. DPP-4 Inhibition by Linagliptin Attenuates Obesity-Related Inflammation and Insulin Resistance by Regulating M1/M2 Macrophage Polarization. Diabetes 2016, 65, 2966–2979. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.; Fukuhara, A.; Onodera, T.; Yokoyama, C.; Otsuki, M.; Shimomura, I. Regulation of Dipeptidyl Peptidase-4, its Substrate Chemokines, and Their Receptors in Adipose Tissue of ob/ob Mice. Horm. Metab. Res. 2017, 49, 380–387. [Google Scholar] [CrossRef]
- Varin, E.M.; Mulvihill, E.E.; Beaudry, J.L.; Pujadas, G.; Fuchs, S.; Tanti, J.F.; Fazio, S.; Kaur, K.; Cao, X.; Baggio, L.L.; et al. Circulating Levels of Soluble Dipeptidyl Peptidase-4 Are Dissociated from Inflammation and Induced by Enzymatic DPP4 Inhibition. Cell Metab. 2019, 29, 320–334.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppolino, G.; Leporini, C.; Rivoli, L.; Ursini, F.; di Paola, E.D.; Cernaro, V.; Arturi, F.; Bolignano, D.; Russo, E.; De Sarro, G.; et al. Exploring the effects of DPP-4 inhibitors on the kidney from the bench to clinical trials. Pharmacol. Res. 2018, 129, 274–294. [Google Scholar] [CrossRef] [PubMed]
- Girardi, A.C.; Degray, B.C.; Nagy, T.; Biemesderfer, D.; Aronson, P.S. Association of Na(+)-H(+) exchanger isoform NHE3 and dipeptidyl peptidase IV in the renal proximal tubule. J. Biol. Chem. 2001, 276, 46671–46677. [Google Scholar] [CrossRef] [Green Version]
- Tiruppathi, C.; Miyamoto, Y.; Ganapathy, V.; Roesel, R.A.; Whitford, G.M.; Leibach, F.H. Hydrolysis and transport of proline-containing peptides in renal brush-border membrane vesicles from dipeptidyl peptidase IV-positive and dipeptidyl peptidase IV-negative rat strains. J. Biol. Chem. 1990, 265, 1476–1483. [Google Scholar] [CrossRef]
- Carraro-Lacroix, L.R.; Malnic, G.; Girardi, A.C. Regulation of Na+/H+ exchanger NHE3 by glucagon-like peptide 1 receptor agonist exendin-4 in renal proximal tubule cells. Am. J. Physiol. Ren. Physiol. 2009, 297, F1647–F1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlatter, P.; Beglinger, C.; Drewe, J.; Gutmann, H. Glucagon-like peptide 1 receptor expression in primary porcine proximal tubular cells. Regul. Pept. 2007, 141, 120–128. [Google Scholar] [CrossRef]
- Pyke, C.; Heller, R.S.; Kirk, R.K.; Orskov, C.; Reedtz-Runge, S.; Kaastrup, P.; Hvelplund, A.; Bardram, L.; Calatayud, D.; Knudsen, L.B. GLP-1 receptor localization in monkey and human tissue: Novel distribution revealed with extensively validated monoclonal antibody. Endocrinology 2014, 155, 1280–1290. [Google Scholar] [CrossRef] [PubMed]
- Ronn, J.; Jensen, E.P.; Wewer Albrechtsen, N.J.; Holst, J.J.; Sorensen, C.M. Glucagon-like peptide-1 acutely affects renal blood flow and urinary flow rate in spontaneously hypertensive rats despite significantly reduced renal expression of GLP-1 receptors. Physiol. Rep. 2017, 5, e13503. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Chou, C.L.; Knepper, M.A. Deep Sequencing in Microdissected Renal Tubules Identifies Nephron Segment-Specific Transcriptomes. J. Am. Soc. Nephrol. 2015, 26, 2669–2677. [Google Scholar] [CrossRef]
- Jensen, E.P.; Poulsen, S.S.; Kissow, H.; Holstein-Rathlou, N.H.; Deacon, C.F.; Jensen, B.L.; Holst, J.J.; Sorensen, C.M. Activation of GLP-1 receptors on vascular smooth muscle cells reduces the autoregulatory response in afferent arterioles and increases renal blood flow. Am. J. Physiol. Ren. Physiol. 2015, 308, F867–F877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hviid, A.V.R.; Sorensen, C.M. Glucagon-like peptide-1 receptors in the kidney: Impact on renal autoregulation. Am. J. Physiol. Ren. Physiol. 2020, 318, F443–F454. [Google Scholar] [CrossRef] [PubMed]
- Duvnjak, L.; Perkovic, M.N.; Blaslov, K. Dipeptidyl peptidase-4 activity is associated with urine albumin excretion in type 1 diabetes. J. Diabetes Complicat. 2017, 31, 218–222. [Google Scholar] [CrossRef] [Green Version]
- Zheng, T.; Liu, Y.; Qin, S.; Liu, H.; Zhang, X.; Zhao, H. Increased plasma dipeptidyl peptidase-4 activities are associated with high prevalence of diabetic nephropathy in Chinese patients with newly diagnosed type 2 diabetes: A cross-sectional study. Diabetes Vasc. Dis. Res. 2016, 13, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Zheng, T.; Baskota, A.; Gao, Y.; Tian, H.; Yang, F. Increased plasma dipeptidyl peptidase 4 activities predict new-onset microalbuminuria in association with its proinflammatory effects in Chinese without diabetes: A four-year prospective study. Nephrol. Dial. Transplant. 2015, 30, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Cho, E.H.; Kim, S.W. Soluble Dipeptidyl Peptidase-4 Levels Are Associated with Decreased Renal Function in Patients with Type 2 Diabetes Mellitus. Diabetes Metab. J. 2019, 43, 97–104. [Google Scholar] [CrossRef]
- Baggio, L.L.; Varin, E.M.; Koehler, J.A.; Cao, X.; Lokhnygina, Y.; Stevens, S.R.; Holman, R.R.; Drucker, D.J. Plasma levels of DPP4 activity and sDPP4 are dissociated from inflammation in mice and humans. Nat. Commun. 2020, 11, 3766. [Google Scholar] [CrossRef] [PubMed]
- Kawanami, D.; Matoba, K.; Utsunomiya, K. Signaling pathways in diabetic nephropathy. Histol. Histopathol. 2016, 11777. [Google Scholar] [CrossRef]
- Kawanami, D.; Matoba, K.; Takeda, Y.; Nagai, Y.; Akamine, T.; Yokota, T.; Sango, K.; Utsunomiya, K. SGLT2 Inhibitors as a Therapeutic Option for Diabetic Nephropathy. Int. J. Mol. Sci. 2017, 18, 1083. [Google Scholar] [CrossRef] [PubMed]
- Opazo-Rios, L.; Mas, S.; Marin-Royo, G.; Mezzano, S.; Gomez-Guerrero, C.; Moreno, J.A.; Egido, J. Lipotoxicity and Diabetic Nephropathy: Novel Mechanistic Insights and Therapeutic Opportunities. Int. J. Mol. Sci. 2020, 21, 2632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, Y.; Matoba, K.; Kawanami, D.; Takeda, Y.; Akamine, T.; Ishizawa, S.; Kanazawa, Y.; Yokota, T.; Utsunomiya, K.; Nishimura, R. ROCK2 regulates TGF-beta-induced expression of CTGF and profibrotic genes via NF-kappaB and cytoskeleton dynamics in mesangial cells. Am. J. Physiol. Ren. Physiol. 2019, 317, F839–F851. [Google Scholar] [CrossRef]
- Matoba, K.; Takeda, Y.; Nagai, Y.; Kawanami, D.; Utsunomiya, K.; Nishimura, R. Unraveling the Role of Inflammation in the Pathogenesis of Diabetic Kidney Disease. Int. J. Mol. Sci. 2019, 20, 3393. [Google Scholar] [CrossRef] [Green Version]
- Loeffler, I.; Wolf, G. Epithelial-to-Mesenchymal Transition in Diabetic Nephropathy: Fact or Fiction? Cells 2015, 4, 631–652. [Google Scholar] [CrossRef]
- Kumar Pasupulati, A.; Chitra, P.S.; Reddy, G.B. Advanced glycation end products mediated cellular and molecular events in the pathology of diabetic nephropathy. Biomol. Concepts 2016, 7, 293–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ram, C.; Jha, A.K.; Ghosh, A.; Gairola, S.; Syed, A.M.; Murty, U.S.; Naidu, V.G.M.; Sahu, B.D. Targeting NLRP3 inflammasome as a promising approach for treatment of diabetic nephropathy: Preclinical evidences with therapeutic approaches. Eur. J. Pharmacol. 2020, 885, 173503. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Lee, K.; Chuang, P.Y.; Liu, Z.; He, J.C. Glomerular endothelial cell injury and cross talk in diabetic kidney disease. Am. J. Physiol. Ren. Physiol. 2015, 308, F287–F297. [Google Scholar] [CrossRef] [Green Version]
- Kanasaki, K. The pathological significance of dipeptidyl peptidase-4 in endothelial cell homeostasis and kidney fibrosis. Diabetol Int. 2016, 7, 212–220. [Google Scholar] [CrossRef]
- Takagaki, Y.; Koya, D.; Kanasaki, K. Dipeptidyl peptidase-4 inhibition and renoprotection: The role of antifibrotic effects. Curr. Opin. Nephrol. Hypertens. 2017, 26, 56–66. [Google Scholar] [CrossRef]
- Muskiet, M.H.A.; Tonneijck, L.; Smits, M.M.; van Baar, M.J.B.; Kramer, M.H.H.; Hoorn, E.J.; Joles, J.A.; van Raalte, D.H. GLP-1 and the kidney: From physiology to pharmacology and outcomes in diabetes. Nat. Rev. Nephrol. 2017, 13, 605–628. [Google Scholar] [CrossRef] [PubMed]
- Alicic, R.Z.; Cox, E.J.; Neumiller, J.J.; Tuttle, K.R. Incretin drugs in diabetic kidney disease: Biological mechanisms and clinical evidence. Nat. Rev. Nephrol. 2020, 1–18. [Google Scholar] [CrossRef]
- Kawanami, D.; Takashi, Y. GLP-1 Receptor Agonists in Diabetic Kidney Disease: From Clinical Outcomes to Mechanisms. Front. Pharmacol. 2020, 11, 967. [Google Scholar] [CrossRef]
- Yin, W.; Jiang, Y.; Xu, S.; Wang, Z.; Peng, L.; Fang, Q.; Deng, T.; Zhao, W.; Zhang, W.; Lou, J. Protein kinase C and protein kinase A are involved in the protection of recombinant human glucagon-like peptide-1 on glomeruli and tubules in diabetic rats. J. Diabetes Investig. 2019, 10, 613–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Luo, P.; Wang, Y.; Li, W.; Wang, C.; Sun, D.; Zhang, R.; Su, T.; Ma, X.; Zeng, C.; et al. Glucagon-like peptide-1 protects against cardiac microvascular injury in diabetes via a cAMP/PKA/Rho-dependent mechanism. Diabetes 2013, 62, 1697–1708. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Park, M.S.; Choung, J.S.; Kim, S.S.; Oh, H.H.; Choi, C.S.; Ha, S.Y.; Kang, Y.; Kim, Y.; Jun, H.S. Glucagon-like peptide-1 inhibits adipose tissue macrophage infiltration and inflammation in an obese mouse model of diabetes. Diabetologia 2012, 55, 2456–2468. [Google Scholar] [CrossRef] [Green Version]
- Kodera, R.; Shikata, K.; Kataoka, H.U.; Takatsuka, T.; Miyamoto, S.; Sasaki, M.; Kajitani, N.; Nishishita, S.; Sarai, K.; Hirota, D.; et al. Glucagon-like peptide-1 receptor agonist ameliorates renal injury through its anti-inflammatory action without lowering blood glucose level in a rat model of type 1 diabetes. Diabetologia 2011, 54, 965–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishibashi, Y.; Nishino, Y.; Matsui, T.; Takeuchi, M.; Yamagishi, S. Glucagon-like peptide-1 suppresses advanced glycation end product-induced monocyte chemoattractant protein-1 expression in mesangial cells by reducing advanced glycation end product receptor level. Metabolism 2011, 60, 1271–1277. [Google Scholar] [CrossRef]
- Saha, S.; Buttari, B.; Panieri, E.; Profumo, E.; Saso, L. An Overview of Nrf2 Signaling Pathway and Its Role in Inflammation. Molecules 2020, 25, 5474. [Google Scholar] [CrossRef]
- Guo, K.; Jin, F. Dipeptidyl peptidase-4 (DPP-4) inhibitor saxagliptin alleviates lipopolysaccharide-induced acute lung injury via regulating the Nrf-2/HO-1 and NF-kappaB pathways. J. Invest. Surg. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Gaber, S.A.; Geddawy, A.; Moussa, R.A. The hepatoprotective effect of sitagliptin against hepatic ischemia reperfusion-induced injury in rats involves Nrf-2/HO-1 pathway. Pharmacol. Rep. 2019, 71, 1044–1049. [Google Scholar] [CrossRef]
- Si, J.; Meng, R.; Gao, P.; Hui, F.; Li, Y.; Liu, X.; Yang, B. Linagliptin protects rat carotid artery from balloon injury and activates the NRF2 antioxidant pathway. Exp. Anim. 2019, 68, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Li, C.; Peng, H.; Ye, Z.; Zhang, J.; Liu, X.; Lou, T. Activation of the Nrf2-ARE pathway attenuates hyperglycemia-mediated injuries in mouse podocytes. Cell Physiol. Biochem. 2014, 34, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Civantos, E.; Bosch, E.; Ramirez, E.; Zhenyukh, O.; Egido, J.; Lorenzo, O.; Mas, S. Sitagliptin ameliorates oxidative stress in experimental diabetic nephropathy by diminishing the miR-200a/Keap-1/Nrf2 antioxidant pathway. Diabetes Metab. Syndr. Obes. 2017, 10, 207–222. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Liu, D.; Lu, Y.; Liu, Z. The Interplay of Renin-Angiotensin System and Toll-Like Receptor 4 in the Inflammation of Diabetic Nephropathy. J. Immunol. Res. 2020, 2020, 6193407. [Google Scholar] [CrossRef]
- Ibrahim, S.S.A.; Salama, M.A.; Selima, E.; Shehata, R.R. Sitagliptin and tofacitinib ameliorate adjuvant induced arthritis via modulating the cross talk between JAK/STAT and TLR-4/NF-kappaB signaling pathways. Life Sci. 2020, 260, 118261. [Google Scholar] [CrossRef]
- Helal, M.G.; Megahed, N.A.; Abd Elhameed, A.G. Saxagliptin mitigates airway inflammation in a mouse model of acute asthma via modulation of NF-kB and TLR4. Life Sci. 2019, 239, 117017. [Google Scholar] [CrossRef]
- El-Kashef, D.H.; Serrya, M.S. Sitagliptin ameliorates thioacetamide-induced acute liver injury via modulating TLR4/NF-KB signaling pathway in mice. Life Sci. 2019, 228, 266–273. [Google Scholar] [CrossRef]
- Schultheis, P.J.; Clarke, L.L.; Meneton, P.; Miller, M.L.; Soleimani, M.; Gawenis, L.R.; Riddle, T.M.; Duffy, J.J.; Doetschman, T.; Wang, T.; et al. Renal and intestinal absorptive defects in mice lacking the NHE3 Na+/H+ exchanger. Nat. Genet. 1998, 19, 282–285. [Google Scholar] [CrossRef]
- Rieg, T.; Gerasimova, M.; Murray, F.; Masuda, T.; Tang, T.; Rose, M.; Drucker, D.J.; Vallon, V. Natriuretic effect by exendin-4, but not the DPP-4 inhibitor alogliptin, is mediated via the GLP-1 receptor and preserved in obese type 2 diabetic mice. Am. J. Physiol. Ren. Physiol. 2012, 303, F963–F971. [Google Scholar] [CrossRef] [Green Version]
- Vallon, V.; Docherty, N.G. Intestinal regulation of urinary sodium excretion and the pathophysiology of diabetic kidney disease: A focus on glucagon-like peptide 1 and dipeptidyl peptidase 4. Exp. Physiol. 2014, 99, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Moroi, M.; Kubota, T. Diuretic and Natriuretic Effects of Dipeptidyl Peptidase-4 Inhibitor Teneligliptin: The Contribution of Glucagon-like Peptide-1. J. Cardiovasc. Pharmacol. 2015, 66, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Lovshin, J.A.; Rajasekeran, H.; Lytvyn, Y.; Lovblom, L.E.; Khan, S.; Alemu, R.; Locke, A.; Lai, V.; He, H.; Hittle, L.; et al. Dipeptidyl Peptidase 4 Inhibition Stimulates Distal Tubular Natriuresis and Increases in Circulating SDF-1alpha(1-67) in Patients With Type 2 Diabetes. Diabetes Care 2017, 40, 1073–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanasaki, K. The role of renal dipeptidyl peptidase-4 in kidney disease: Renal effects of dipeptidyl peptidase-4 inhibitors with a focus on linagliptin. Clin. Sci. 2018, 132, 489–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, S.; Srivastava, S.P.; Kanasaki, M.; He, J.; Kitada, M.; Nagai, T.; Nitta, K.; Takagi, S.; Kanasaki, K.; Koya, D. Interactions of DPP-4 and integrin beta1 influences endothelial-to-mesenchymal transition. Kidney Int. 2015, 88, 479–489. [Google Scholar] [CrossRef] [Green Version]
- Khalil, R.; Shata, A.; Abd El-Kader, E.M.; Sharaf, H.; Abdo, W.S.; Amin, N.A.; Saber, S. Vildagliptin, a DPP-4 inhibitor, attenuates carbon tetrachloride-induced liver fibrosis by targeting ERK1/2, p38alpha, and NF-kappaB signaling. Toxicol. Appl. Pharmacol. 2020, 407, 115246. [Google Scholar] [CrossRef] [PubMed]
- Aboulmagd, Y.M.; El-Bahy, A.A.Z.; Menze, E.T.; Azab, S.S.; El-Demerdash, E. Role of linagliptin in preventing the pathological progression of hepatic fibrosis in high fat diet and streptozotocin-induced diabetic obese rats. Eur. J. Pharmacol. 2020, 881, 173224. [Google Scholar] [CrossRef]
- Srivastava, S.P.; Goodwin, J.E.; Kanasaki, K.; Koya, D. Inhibition of Angiotensin-Converting Enzyme Ameliorates Renal Fibrosis by Mitigating DPP-4 Level and Restoring Antifibrotic MicroRNAs. Genes 2020, 11, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahba, N.S.; Ghareib, S.A.; Abdelghany, R.H.; Abdel-Aal, M.; Alsemeh, A.E. Vitamin D3 potentiates the nephroprotective effects of metformin in a rat model of metabolic syndrome: Role of AMPK/SIRT1 activation and DPP-4 inhibition. Can. J. Physiol. Pharmacol. 2020. [Google Scholar] [CrossRef]
- Kawakubo, M.; Tanaka, M.; Ochi, K.; Watanabe, A.; Saka-Tanaka, M.; Kanamori, Y.; Yoshioka, N.; Yamashita, S.; Goto, M.; Itoh, M.; et al. Dipeptidyl peptidase-4 inhibition prevents nonalcoholic steatohepatitis-associated liver fibrosis and tumor development in mice independently of its anti-diabetic effects. Sci. Rep. 2020, 10, 983. [Google Scholar] [CrossRef]
- Soare, A.; Gyorfi, H.A.; Matei, A.E.; Dees, C.; Rauber, S.; Wohlfahrt, T.; Chen, C.W.; Ludolph, I.; Horch, R.E.; Bauerle, T.; et al. Dipeptidylpeptidase 4 as a Marker of Activated Fibroblasts and a Potential Target for the Treatment of Fibrosis in Systemic Sclerosis. Arthritis Rheumatol. 2020, 72, 137–149. [Google Scholar] [CrossRef]
- Hirose, M.; Takano, H.; Hasegawa, H.; Tadokoro, H.; Hashimoto, N.; Takemura, G.; Kobayashi, Y. The effects of dipeptidyl peptidase-4 on cardiac fibrosis in pressure overload-induced heart failure. J. Pharmacol. Sci. 2017, 135, 164–173. [Google Scholar] [CrossRef]
- Brown, S.M.; Smith, C.E.; Meuth, A.I.; Khan, M.; Aroor, A.R.; Cleeton, H.M.; Meininger, G.A.; Sowers, J.R.; DeMarco, V.G.; Chandrasekar, B.; et al. Dipeptidyl Peptidase-4 Inhibition With Saxagliptin Ameliorates Angiotensin II-Induced Cardiac Diastolic Dysfunction in Male Mice. Endocrinology 2017, 158, 3592–3604. [Google Scholar] [CrossRef]
- Zhao, J.; Pei, L. Cardiac Endocrinology: Heart-Derived Hormones in Physiology and Disease. JACC Basic Transl. Sci. 2020, 5, 949–960. [Google Scholar] [CrossRef] [PubMed]
- Seki, N.; Matsumoto, T.; Fukazawa, M. Relationship Between the Brain Natriuretic Peptide (BNP) Level and Prognosis of Diabetic Nephropathy with Microalbuminuria: A 7-Year Follow-Up Study. Horm. Metab. Res. 2018, 50, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Sakai, T.; Niiya, T.; Miyaoka, H.; Miyake, T.; Yamamoto, S.; Tanaka, K.; Ueda, T.; Senba, H.; Torisu, M.; et al. B-type natriuretic peptide and renal function in Japanese patients with type 2 diabetes mellitus: The Dogo Study. Endocr. J. 2017, 64, 1131–1136. [Google Scholar] [CrossRef] [Green Version]
- Seki, N.; Matsumoto, T.; Fukazawa, M. Relationship between the brain natriuretic peptide (BNP) level and remission of diabetic nephropathy with microalbuminuria: A 3-year follow-up study. Horm. Metab. Res. 2015, 47, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Regulation of erythropoietin production. New insights into molecular mechanisms of oxygen homeostasis. Hematol. Oncol. Clin. North. Am. 1994, 8, 863–884. [Google Scholar] [CrossRef]
- Tsuruya, K.; Yoshida, H.; Suehiro, T.; Fujisaki, K.; Masutani, K.; Kitazono, T. Erythropoiesis-stimulating agent slows the progression of chronic kidney disease: A possibility of a direct action of erythropoietin. Ren. Fail. 2016, 38, 390–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, M.; Takei, M.; Shiraishi, Y.; Suzuki, Y. Increased Hematocrit During Sodium-Glucose Cotransporter 2 Inhibitor Therapy Indicates Recovery of Tubulointerstitial Function in Diabetic Kidneys. J. Clin. Med. Res. 2016, 8, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broxmeyer, H.E.; Hoggatt, J.; O’Leary, H.A.; Mantel, C.; Chitteti, B.R.; Cooper, S.; Messina-Graham, S.; Hangoc, G.; Farag, S.; Rohrabaugh, S.L.; et al. Dipeptidylpeptidase 4 negatively regulates colony-stimulating factor activity and stress hematopoiesis. Nat. Med. 2012, 18, 1786–1796. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.C.; Liu, Y.B.; Liu, W.F.; Zhou, Y.Y.; He, H.F.; Lin, S. Neuropeptide Y Is an Immunomodulatory Factor: Direct and Indirect. Front. Immunol. 2020, 11, 580378. [Google Scholar] [CrossRef]
- Lay, A.C.; Barrington, A.F.; Hurcombe, J.A.; Ramnath, R.D.; Graham, M.; Lewis, P.A.; Wilson, M.C.; Heesom, K.J.; Butler, M.J.; Perrett, R.M.; et al. A role for NPY-NPY2R signaling in albuminuric kidney disease. Proc. Natl. Acad. Sci. USA 2020, 117, 15862–15873. [Google Scholar] [CrossRef]
- Hasan, A.A.; Hocher, B. Role of soluble and membrane-bound dipeptidyl peptidase-4 in diabetic nephropathy. J. Mol. Endocrinol. 2017, 59, R1–R10. [Google Scholar] [CrossRef]
- Sayyed, S.G.; Hagele, H.; Kulkarni, O.P.; Endlich, K.; Segerer, S.; Eulberg, D.; Klussmann, S.; Anders, H.J. Podocytes produce homeostatic chemokine stromal cell-derived factor-1/CXCL12, which contributes to glomerulosclerosis, podocyte loss and albuminuria in a mouse model of type 2 diabetes. Diabetologia 2009, 52, 2445–2454. [Google Scholar] [CrossRef] [Green Version]
- Nistala, R.; Habibi, J.; Aroor, A.; Sowers, J.R.; Hayden, M.R.; Meuth, A.; Knight, W.; Hancock, T.; Klein, T.; DeMarco, V.G.; et al. DPP4 inhibition attenuates filtration barrier injury and oxidant stress in the zucker obese rat. Obesity 2014, 22, 2172–2179. [Google Scholar] [CrossRef] [Green Version]
- Takashima, S.; Fujita, H.; Fujishima, H.; Shimizu, T.; Sato, T.; Morii, T.; Tsukiyama, K.; Narita, T.; Takahashi, T.; Drucker, D.J.; et al. Stromal cell-derived factor-1 is upregulated by dipeptidyl peptidase-4 inhibition and has protective roles in progressive diabetic nephropathy. Kidney Int. 2016, 90, 783–796. [Google Scholar] [CrossRef]
- Liu, W.J.; Xie, S.H.; Liu, Y.N.; Kim, W.; Jin, H.Y.; Park, S.K.; Shao, Y.M.; Park, T.S. Dipeptidyl peptidase IV inhibitor attenuates kidney injury in streptozotocin-induced diabetic rats. J. Pharmacol. Exp. Ther. 2012, 340, 248–255. [Google Scholar] [CrossRef]
- Kodera, R.; Shikata, K.; Takatsuka, T.; Oda, K.; Miyamoto, S.; Kajitani, N.; Hirota, D.; Ono, T.; Usui, H.K.; Makino, H. Dipeptidyl peptidase-4 inhibitor ameliorates early renal injury through its anti-inflammatory action in a rat model of type 1 diabetes. Biochem. Biophys. Res. Commun. 2014, 443, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Vavrinec, P.; Henning, R.H.; Landheer, S.W.; Wang, Y.; Deelman, L.E.; Dokkum, R.P.; Buikema, H. Vildagliptin restores renal myogenic function and attenuates renal sclerosis independently of effects on blood glucose or proteinuria in zucker diabetic fatty rat. Curr. Vasc. Pharmacol. 2014, 12, 836–844. [Google Scholar] [CrossRef]
- Birnbaum, Y.; Bajaj, M.; Qian, J.; Ye, Y. Dipeptidyl peptidase-4 inhibition by Saxagliptin prevents inflammation and renal injury by targeting the Nlrp3/ASC inflammasome. BMJ Open Diabetes Res. Care. 2016, 4, e000227. [Google Scholar] [CrossRef]
- Nakashima, S.; Matsui, T.; Takeuchi, M.; Yamagishi, S.I. Linagliptin blocks renal damage in type 1 diabetic rats by suppressing advanced glycation end products-receptor axis. Horm. Metab. Res. 2014, 46, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Oraby, M.A.; El-Yamany, M.F.; Safar, M.M.; Assaf, N.; Ghoneim, H.A. Amelioration of Early Markers of Diabetic Nephropathy by Linagliptin in Fructose-Streptozotocin-Induced Type 2 Diabetic Rats. Nephron 2019, 141, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Spencer, N.Y.; Yang, Z.; Sullivan, J.C.; Klein, T.; Stanton, R.C. Linagliptin unmasks specific antioxidant pathways protective against albuminuria and kidney hypertrophy in a mouse model of diabetes. PLoS ONE 2018, 13, e0200249. [Google Scholar] [CrossRef]
- Takagaki, Y.; Shi, S.; Katoh, M.; Kitada, M.; Kanasaki, K.; Koya, D. Dipeptidyl peptidase-4 plays a pathogenic role in BSA-induced kidney injury in diabetic mice. Sci. Rep. 2019, 9, 7519. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Lian, X.; Wang, Z.; Zheng, J.; Liu, J.; Chu, Y.; Teng, Y.; Zhang, Z. The dipeptidyl peptidase-4 inhibitor sitagliptin ameliorates renal injury in type 1 diabetic mice via inhibiting the TGF-beta/Smad signal pathway. Pharmazie 2019, 74, 239–242. [Google Scholar] [PubMed]
- Ren, X.; Zhu, R.; Liu, G.; Xue, F.; Wang, Y.; Xu, J.; Zhang, W.; Yu, W.; Li, R. Effect of sitagliptin on tubulointerstitial Wnt/beta-catenin signalling in diabetic nephropathy. Nephrology 2019, 24, 1189–1197. [Google Scholar] [CrossRef]
- Gangadharan Komala, M.; Gross, S.; Zaky, A.; Pollock, C.; Panchapakesan, U. Saxagliptin reduces renal tubulointerstitial inflammation, hypertrophy and fibrosis in diabetes. Nephrology 2016, 21, 423–431. [Google Scholar] [CrossRef]
- Kanasaki, K.; Shi, S.; Kanasaki, M.; He, J.; Nagai, T.; Nakamura, Y.; Ishigaki, Y.; Kitada, M.; Srivastava, S.P.; Koya, D. Linagliptin-mediated DPP-4 inhibition ameliorates kidney fibrosis in streptozotocin-induced diabetic mice by inhibiting endothelial-to-mesenchymal transition in a therapeutic regimen. Diabetes 2014, 63, 2120–2131. [Google Scholar] [CrossRef] [Green Version]
- Shi, S.; Kanasaki, K.; Koya, D. Linagliptin but not Sitagliptin inhibited transforming growth factor-beta2-induced endothelial DPP-4 activity and the endothelial-mesenchymal transition. Biochem. Biophys. Res. Commun. 2016, 471, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Gavrilova, Y.S.; Bgatova, N.P.; Klimontov, V.V.; Ischenko, I.Y.; Michurina, S.V.; Myakina, N.E.; Zavyalov, E.L. Effect of Linagliptin on Structural Changes in the Kidney in Experimental Type 2 Diabetes Mellitus. Bull. Exp. Biol. Med. 2016, 161, 501–504. [Google Scholar] [CrossRef]
- Kubo, A.; Hidaka, T.; Nakayama, M.; Sasaki, Y.; Takagi, M.; Suzuki, H.; Suzuki, Y. Protective effects of DPP-4 inhibitor on podocyte injury in glomerular diseases. BMC Nephrol. 2020, 21, 402. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Mega, C.; Goncalves, A.; Rodrigues-Santos, P.; Teixeira-Lemos, E.; Teixeira, F.; Fontes-Ribeiro, C.; Reis, F.; Fernandes, R. Sitagliptin prevents inflammation and apoptotic cell death in the kidney of type 2 diabetic animals. Mediat. Inflamm. 2014, 2014, 538737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuprykov, O.; Ando, R.; Reichetzeder, C.; von Websky, K.; Antonenko, V.; Sharkovska, Y.; Chaykovska, L.; Rahnenfuhrer, J.; Hasan, A.A.; Tammen, H.; et al. The dipeptidyl peptidase inhibitor linagliptin and the angiotensin II receptor blocker telmisartan show renal benefit by different pathways in rats with 5/6 nephrectomy. Kidney Int. 2016, 89, 1049–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmy, M.M.; Mouneir, S.M. Reno-protective effect of linagliptin against gentamycin nephrotoxicity in rats. Pharmacol. Rep. 2019, 71, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Cappetta, D.; Ciuffreda, L.P.; Cozzolino, A.; Esposito, G.; Scavone, C.; Sapio, L.; Naviglio, S.; D’Amario, D.; Crea, F.; Rossi, F.; et al. Dipeptidyl Peptidase 4 Inhibition Ameliorates Chronic Kidney Disease in a Model of Salt-Dependent Hypertension. Oxid. Med. Cell. Longev. 2019, 2019, 8912768. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Kume, S.; Chin-Kanasaki, M.; Araki, H.; Araki, S.I.; Ugi, S.; Sugaya, T.; Uzu, T.; Maegawa, H. Renoprotective effect of DPP-4 inhibitors against free fatty acid-bound albumin-induced renal proximal tubular cell injury. Biochem. Biophys. Res. Commun. 2016, 470, 539–545. [Google Scholar] [CrossRef]
- Delic, D.; Wiech, F.; Urquhart, R.; Gabrielyan, O.; Rieber, K.; Rolser, M.; Tsuprykov, O.; Hasan, A.A.; Kramer, B.K.; Baum, P.; et al. Linagliptin and telmisartan induced effects on renal and urinary exosomal miRNA expression in rats with 5/6 nephrectomy. Sci. Rep. 2020, 10, 3373. [Google Scholar] [CrossRef] [Green Version]
- Hasan, A.A.; von Websky, K.; Reichetzeder, C.; Tsuprykov, O.; Gaballa, M.M.S.; Guo, J.; Zeng, S.; Delic, D.; Tammen, H.; Klein, T.; et al. Mechanisms of GLP-1 receptor-independent renoprotective effects of the dipeptidyl peptidase type 4 inhibitor linagliptin in GLP-1 receptor knockout mice with 5/6 nephrectomy. Kidney Int. 2019, 95, 1373–1388. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, J.; Perkovic, V.; Johansen, O.E.; Cooper, M.E.; Kahn, S.E.; Marx, N.; Alexander, J.H.; Pencina, M.; Toto, R.D.; Wanner, C.; et al. Effect of Linagliptin vs Placebo on Major Cardiovascular Events in Adults With Type 2 Diabetes and High Cardiovascular and Renal Risk: The CARMELINA Randomized Clinical Trial. JAMA 2019, 321, 69–79. [Google Scholar] [CrossRef]
- Perkovic, V.; Toto, R.; Cooper, M.E.; Mann, J.F.E.; Rosenstock, J.; McGuire, D.K.; Kahn, S.E.; Marx, N.; Alexander, J.H.; Zinman, B.; et al. Effects of Linagliptin on Cardiovascular and Kidney Outcomes in People With Normal and Reduced Kidney Function: Secondary Analysis of the CARMELINA Randomized Trial. Diabetes Care 2020, 43, 1803–1812. [Google Scholar] [CrossRef]
- Groop, P.H.; Cooper, M.E.; Perkovic, V.; Hocher, B.; Kanasaki, K.; Haneda, M.; Schernthaner, G.; Sharma, K.; Stanton, R.C.; Toto, R.; et al. Linagliptin and its effects on hyperglycaemia and albuminuria in patients with type 2 diabetes and renal dysfunction: The randomized MARLINA-T2D trial. Diabetes Obes. Metab. 2017, 19, 1610–1619. [Google Scholar] [CrossRef] [PubMed]
- Scirica, B.M.; Mosenzon, O.; Bhatt, D.L.; Udell, J.A.; Steg, P.G.; McGuire, D.K.; Im, K.; Kanevsky, E.; Stahre, C.; Sjostrand, M.; et al. Cardiovascular Outcomes According to Urinary Albumin and Kidney Disease in Patients With Type 2 Diabetes at High Cardiovascular Risk: Observations From the SAVOR-TIMI 53 Trial. JAMA Cardiol. 2018, 3, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosenzon, O.; Leibowitz, G.; Bhatt, D.L.; Cahn, A.; Hirshberg, B.; Wei, C.; Im, K.; Rozenberg, A.; Yanuv, I.; Stahre, C.; et al. Effect of Saxagliptin on Renal Outcomes in the SAVOR-TIMI 53 Trial. Diabetes Care 2017, 40, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornel, J.H.; Bakris, G.L.; Stevens, S.R.; Alvarsson, M.; Bax, W.A.; Chuang, L.M.; Engel, S.S.; Lopes, R.D.; McGuire, D.K.; Riefflin, A.; et al. Effect of Sitagliptin on Kidney Function and Respective Cardiovascular Outcomes in Type 2 Diabetes: Outcomes From TECOS. Diabetes Care 2016, 39, 2304–2310. [Google Scholar] [CrossRef] [Green Version]
- Hattori, S. Sitagliptin reduces albuminuria in patients with type 2 diabetes. Endocr. J. 2011, 58, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, I.; Hiura, Y.; Tamai, A.; Yoshida, Y.; Yakusiji, Y.; Ikuno, Y.; Okada, M.; Ueno, H.; Tanaka, N.; Yamagami, K.; et al. Sitagliptin reduces the urine albumin-to-creatinine ratio in type 2 diabetes through decreasing both blood pressure and estimated glomerular filtration rate. J. Diabetes 2015, 7, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Okada, Y.; Arao, T.; Tanaka, Y. Sitagliptin improves albuminuria in patients with type 2 diabetes mellitus. J. Diabetes Investig. 2014, 5, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, W.B.; Cannon, C.P.; Heller, S.R.; Nissen, S.E.; Bergenstal, R.M.; Bakris, G.L.; Perez, A.T.; Fleck, P.R.; Mehta, C.R.; Kupfer, S.; et al. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N. Engl. J. Med. 2013, 369, 1327–1335. [Google Scholar] [CrossRef] [Green Version]
- Fujita, H.; Taniai, H.; Murayama, H.; Ohshiro, H.; Hayashi, H.; Sato, S.; Kikuchi, N.; Komatsu, T.; Komatsu, K.; Komatsu, K.; et al. DPP-4 inhibition with alogliptin on top of angiotensin II type 1 receptor blockade ameliorates albuminuria via up-regulation of SDF-1alpha in type 2 diabetic patients with incipient nephropathy. Endocr. J. 2014, 61, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakata, K.; Hayakawa, M.; Yano, Y.; Tamaki, N.; Yokota, N.; Eto, T.; Watanabe, R.; Hirayama, N.; Matsuo, T.; Kuroki, K.; et al. Efficacy of alogliptin, a dipeptidyl peptidase-4 inhibitor, on glucose parameters, the activity of the advanced glycation end product (AGE)—Receptor for AGE (RAGE) axis and albuminuria in Japanese type 2 diabetes. Diabetes Metab. Res. Rev. 2013, 29, 624–630. [Google Scholar] [CrossRef]
- Tani, S.; Nagao, K.; Hirayama, A. Association between urinary albumin excretion and low-density lipoprotein heterogeneity following treatment of type 2 diabetes patients with the dipeptidyl peptidase-4 inhibitor, vildagliptin: A pilot study. Am. J. Cardiovasc. Drugs 2013, 13, 443–450. [Google Scholar] [CrossRef]
- Mohsen, M.; Elberry, A.A.; Mohamed Rabea, A.; Abdelrahim, M.E.A.; Hussein, R.R.S. Saxagliptin and vildagliptin lowered albuminuria in patients with diabetes and hypertension independent on glycaemic control. Int. J. Clin. Pract. 2020, e13769. [Google Scholar] [CrossRef]
- Kitada, M.; Tsuda, S.I.; Konishi, K.; Takeda-Watanabe, A.; Fujii, M.; Kanasaki, K.; Nishizawa, M.; Nakagawa, A.; Koya, D. Anagliptin ameliorates albuminuria and urinary liver-type fatty acid-binding protein excretion in patients with type 2 diabetes with nephropathy in a glucose-lowering-independent manner. BMJ Open Diabetes Res. Care. 2017, 5, e000391. [Google Scholar] [CrossRef] [Green Version]
- Kitada, M.; Ogura, Y.; Nitta, K.; Fujii, M.; Kanasaki, K.; Konishi, K.; Iida, Y.; Nakagawa, A.; Koya, D. Effect of switching to teneligliptin from other dipeptidyl peptidase-4 inhibitors on glucose control and renoprotection in type 2 diabetes patients with diabetic kidney disease. J. Diabetes Investig. 2019, 10, 706–713. [Google Scholar] [CrossRef]
- O’Hara, D.V.; Parkhill, T.R.; Badve, S.V.; Jun, M.; Jardine, M.J.; Perkovic, V. The effects of dipeptidyl peptidase-4 inhibitors on kidney outcomes. Diabetes Obes. Metab. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.H.; Kim, S.; Park, E.G.; Kim, S.G.; Hahn, S.; Kim, N.H. Effects of Dipeptidyl Peptidase-4 Inhibitors on Renal Outcomes in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Endocrinol. Metab. 2019, 34, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, N.M.; Jandeleit-Dahm, K.A. Dipeptidyl peptidase-4 inhibitors and cardiovascular and renal disease in type 2 diabetes: What have we learned from the CARMELINA trial? Diabetes Vasc. Dis. Res. 2019, 16, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, H. A systematic review of the benefits and harms of dipeptidyl peptidase-4 inhibitor for chronic kidney disease. Hemodial. Int. 2017, 21, 72–83. [Google Scholar] [CrossRef]
- Walker, S.R.; Komenda, P.; Khojah, S.; Al-Tuwaijri, W.; MacDonald, K.; Hiebert, B.; Tangri, N.; Nadurak, S.W.D.; Ferguson, T.W.; Rigatto, C.; et al. Dipeptidyl Peptidase-4 Inhibitors in Chronic Kidney Disease: A Systematic Review of Randomized Clinical Trials. Nephron 2017, 136, 85–94. [Google Scholar] [CrossRef]
- Chacra, A.; Gantz, I.; Mendizabal, G.; Durlach, L.; O’Neill, E.A.; Zimmer, Z.; Suryawanshi, S.; Engel, S.S.; Lai, E. A randomised, double-blind, trial of the safety and efficacy of omarigliptin (a once-weekly DPP-4 inhibitor) in subjects with type 2 diabetes and renal impairment. Int. J. Clin. Pract. 2017, 71, e12955. [Google Scholar] [CrossRef] [Green Version]
- Homma, K.; Yoshizawa, J.; Shiina, Y.; Ozawa, H.; Igarashi, M.; Matsuoka, T.; Sasaki, J.; Yoshizawa, M.; Homma, Y. A Dipeptidyl Peptidase-4 Inhibitor, Teneligliptin, Decreases Plasma Triglyceride-Rich Lipoprotein Remnants in Diabetic Patients with Chronic Kidney Disease Undergoing Hemodialysis. Drugs R&D 2017, 17, 397–402. [Google Scholar]
- Coca, S.G.; Ismail-Beigi, F.; Haq, N.; Krumholz, H.M.; Parikh, C.R. Role of intensive glucose control in development of renal end points in type 2 diabetes mellitus: Systematic review and meta-analysis intensive glucose control in type 2 diabetes. Arch. Intern. Med. 2012, 172, 761–769. [Google Scholar] [CrossRef] [Green Version]
- Ueki, K.; Sasako, T.; Okazaki, Y.; Kato, M.; Okahata, S.; Katsuyama, H.; Haraguchi, M.; Morita, A.; Ohashi, K.; Hara, K.; et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): An open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 951–964. [Google Scholar] [CrossRef]
- Ueki, K.; Sasako, T.; Okazaki, Y.; Miyake, K.; Nangaku, M.; Ohashi, Y.; Noda, M.; Kadowaki, T.; Group, J.D.S. Multifactorial intervention has a significant effect on diabetic kidney disease in patients with type 2 diabetes. Kidney Int. 2020, 99. [Google Scholar] [CrossRef] [PubMed]
- Shikata, K.; Haneda, M.; Ninomiya, T.; Koya, D.; Suzuki, Y.; Suzuki, D.; Ishida, H.; Akai, H.; Tomino, Y.; Uzu, T.; et al. Randomized trial of an intensified, multifactorial intervention in patients with advanced-stage diabetic kidney disease: Diabetic Nephropathy Remission and Regression Team Trial in Japan (DNETT-Japan). J. Diabetes Investig. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yamanouchi, M.; Furuichi, K.; Hoshino, J.; Ubara, Y.; Wada, T. Nonproteinuric diabetic kidney disease. Clin. Exp. Nephrol. 2020, 24, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakris, G.; Oshima, M.; Mahaffey, K.W.; Agarwal, R.; Cannon, C.P.; Capuano, G.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; et al. Effects of Canagliflozin in Patients with Baseline eGFR <30 mL/min per 1.73 m(2): Subgroup Analysis of the Randomized CREDENCE Trial. Clin. J. Am. Soc. Nephrol. 2020, 15, 1705–1714. [Google Scholar] [CrossRef]


{kind=link}
| Trials | Participants | Renal Outcome |
|---|---|---|
| SAVOR-TIMI 53 (saxagliptin 2.5 mg or 5 mg vs. placebo) | T2D with high CV risk (n = 9696), 2 years | UACR↓ (including in normal range) No effect on eGFR |
| TECOS (sitagliptin 50 mg or 100 mg vs. placebo) | T2D with high CV risk (n = 14,671), 3 years | No effect on eGFR |
| MARLINA-T2D (linagliptin 5 mg vs placebo) | T2D with albuminuria (n = 360), 24 weeks | No significant effect on UACR |
| CARMELINA (linagliptin 5 mg vs placebo) | T2D with high CV risk and renal risk defined as reduced eGFR and micro-macro albuminuria (n = 6991), 2.2 years | Progression of Albuminuria↓ No effects on composite renal outcomes (time to first occurrence of adjudicated death due to renal failure, ESRD, or sustained 40% or higher decrease in eGFR from baseline) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawanami, D.; Takashi, Y.; Takahashi, H.; Motonaga, R.; Tanabe, M. Renoprotective Effects of DPP-4 Inhibitors. Antioxidants 2021, 10, 246. https://doi.org/10.3390/antiox10020246
Kawanami D, Takashi Y, Takahashi H, Motonaga R, Tanabe M. Renoprotective Effects of DPP-4 Inhibitors. Antioxidants. 2021; 10(2):246. https://doi.org/10.3390/antiox10020246
Chicago/Turabian StyleKawanami, Daiji, Yuichi Takashi, Hiroyuki Takahashi, Ryoko Motonaga, and Makito Tanabe. 2021. "Renoprotective Effects of DPP-4 Inhibitors" Antioxidants 10, no. 2: 246. https://doi.org/10.3390/antiox10020246
APA StyleKawanami, D., Takashi, Y., Takahashi, H., Motonaga, R., & Tanabe, M. (2021). Renoprotective Effects of DPP-4 Inhibitors. Antioxidants, 10(2), 246. https://doi.org/10.3390/antiox10020246