
Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity

 ,
,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Anthropometric and Physical Activity Characterization
2.3. Plasma and PBMCs Isolation
2.4. Biochemical Parameters and Hemogram
2.5. Antioxidant Protein Levels
2.6. Enzymatic Determinations
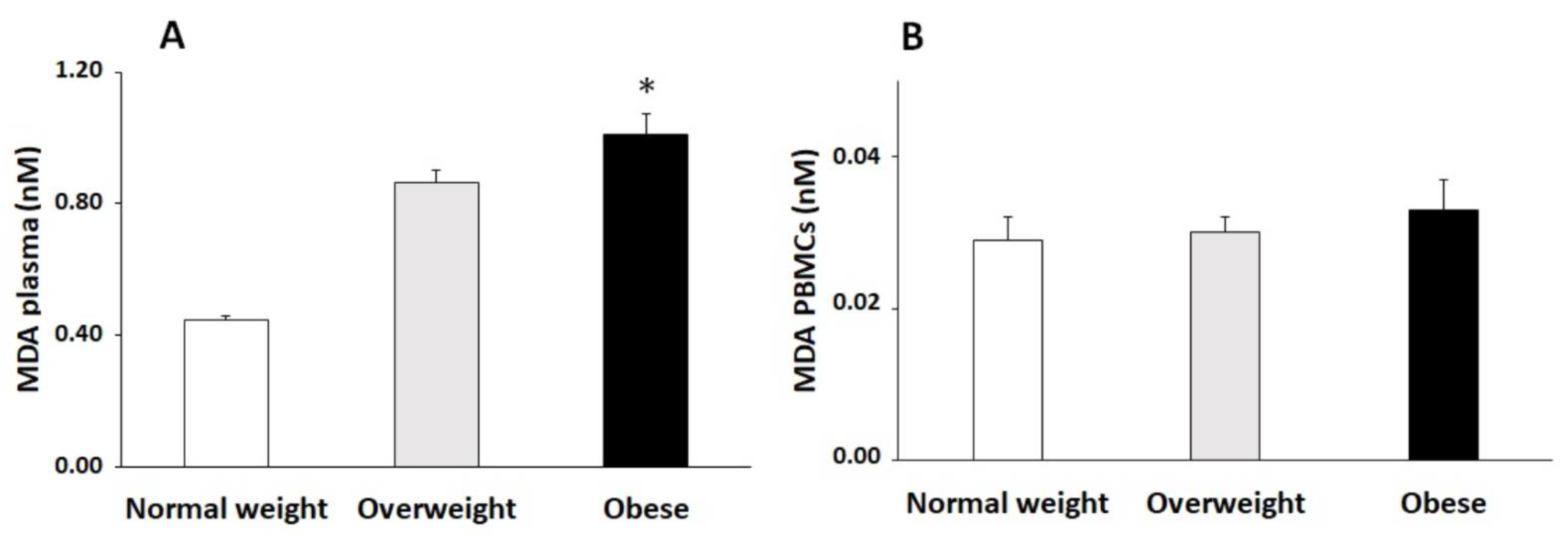
2.7. Malondialdehyde Assay
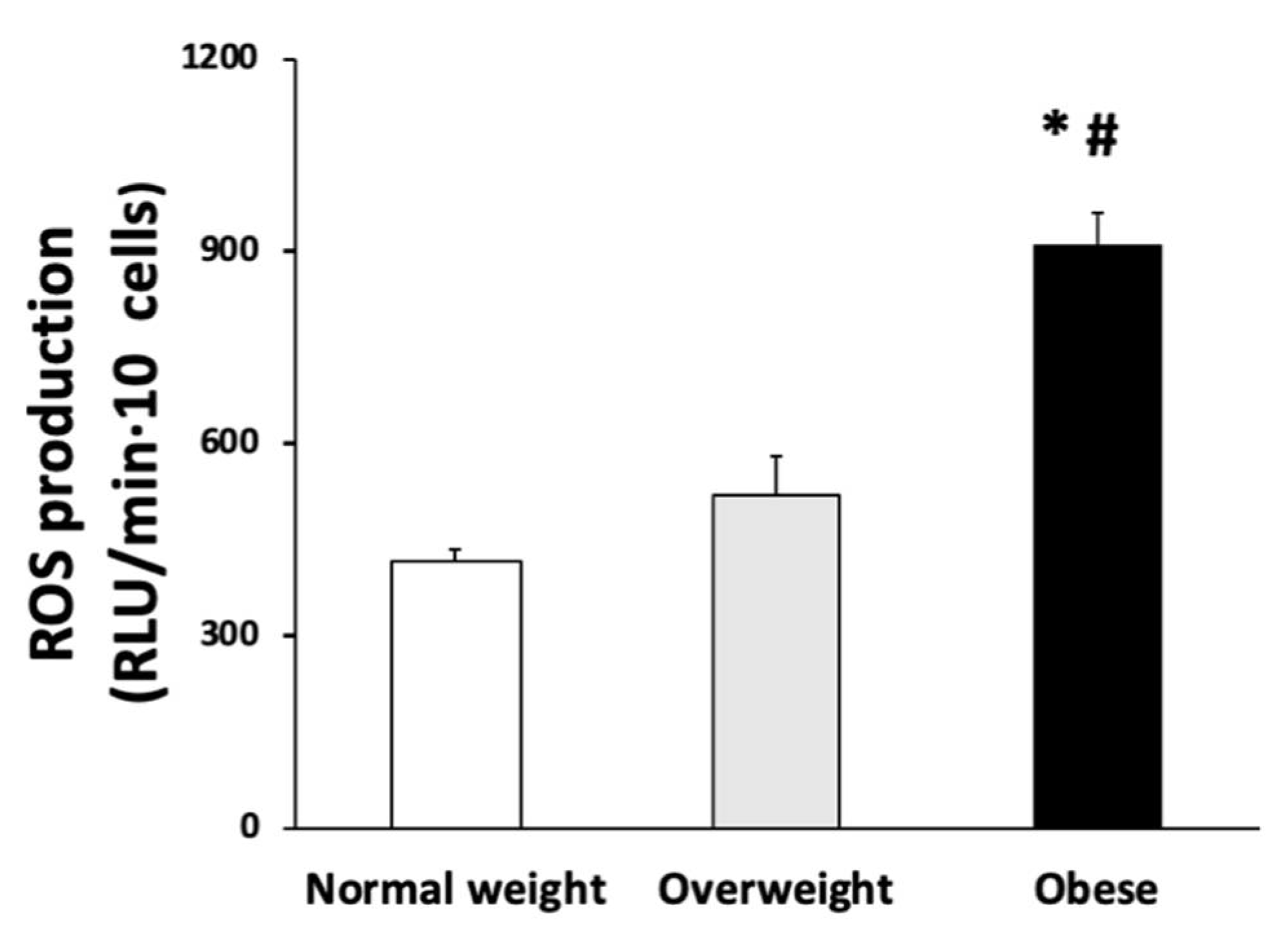
2.8. PBMCs ROS Production
2.9. Cytokine Assays
2.10. Statistics
3. Results
3.1. Anthropometric and Haematological Parameters
3.2. Biomarkers of Oxidative Stress
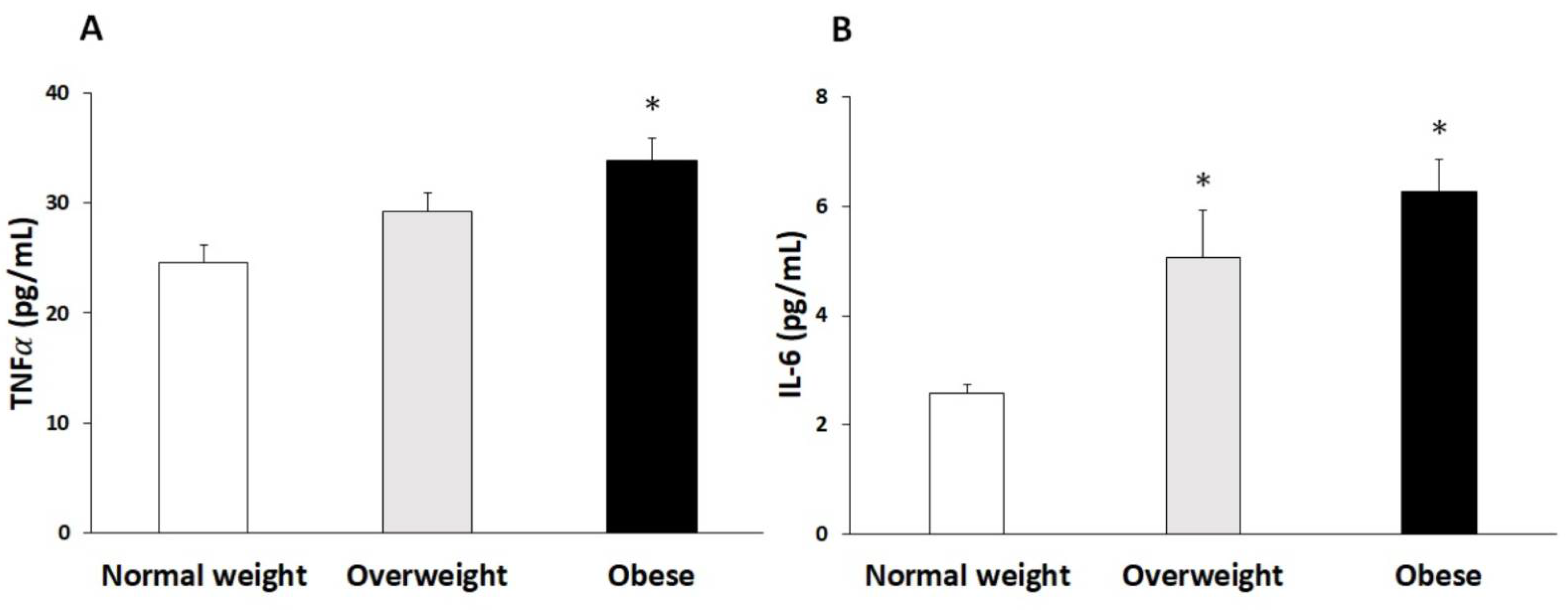
3.3. Cytokine Levels
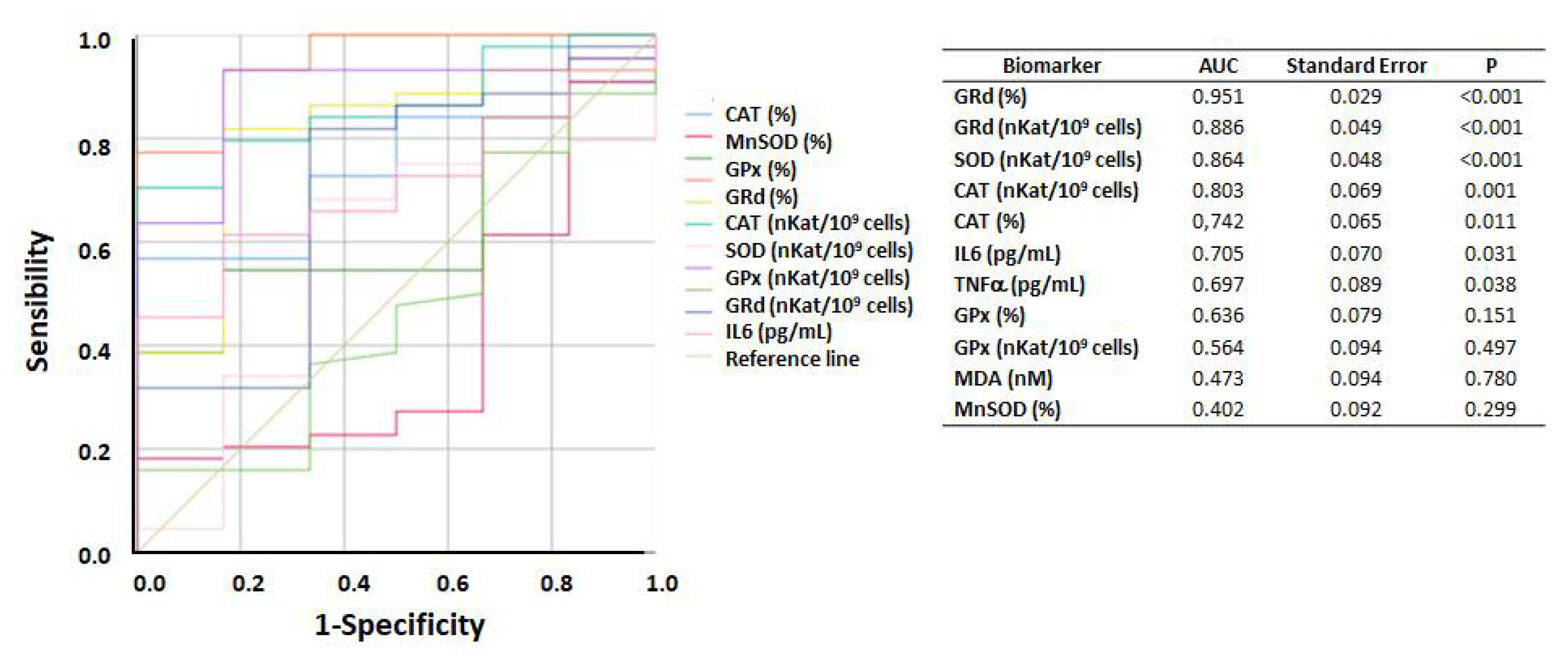
3.4. ROC Curve of Biomarkers According to BMI
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Biswas, T.; Garnett, S.P.; Pervin, S.; Rawal, L.B. The prevalence of underweight, overweight and obesity in Bangladeshi adults: Data from a national survey. PLoS ONE 2017, 12, e0177395. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, R.; Adams-Huet, B.; Jialal, I. The effect of increasing body mass index on cardio-metabolic risk and biomarkers of oxidative stress and inflammation in nascent metabolic syndrome. J. Diabetes Complicat. 2017, 31, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Skalicky, J.; Muzakova, V.; Kandar, R.; Meloun, M.; Rousar, T.; Palicka, V. Evaluation of oxidative stress and inflammation in obese adults with metabolic syndrome. Clin. Chem. Lab. Med. 2008, 46, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Ataey, A.; Jafarvand, E.; Adham, D.; Moradi-Asl, E. The Relationship Between Obesity, Overweight, and the Human Development Index in World Health Organization Eastern Mediterranean Region Countries. J. Prev. Med. Public Health 2020, 53, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Vincent, H.K.; Taylor, A.G. Biomarkers and potential mechanisms of obesity-induced oxidant stress in humans. Int. J. Obes. 2006, 30, 400–418. [Google Scholar] [CrossRef] [Green Version]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Sánchez, A.; Gámez-Nava, J.I.; Díaz-de la Cruz, E.N.; Cardona-Muñoz, E.G.; Becerra-Alvarado, I.N.; Aceves-Aceves, J.A.; Sánchez-Rodríguez, E.N.; Miranda-Díaz, A.G. The Effect of Visceral Abdominal Fat Volume on Oxidative Stress and Proinflammatory Cytokines in Subjects with Normal Weight, Overweight and Obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 1077–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popko, K.; Gorska, E.; Stelmaszczyk-Emmel, A.; Plywaczewski, R.; Stoklosa, A.; Gorecka, D.; Pyrzak, B.; Demkow, U. Proinflammatory cytokines IL-6 and TNF-α and the development of inflammation in obese subjects. Eur. J. Med. Res. 2010, 15, 120–122. [Google Scholar] [CrossRef]
- Cawthorn, W.P.; Sethi, J.K. TNF-α and adipocyte biology. FEBS Lett. 2008, 582, 117–131. [Google Scholar] [CrossRef] [Green Version]
- Jung, U.J.; Seo, Y.R.; Ryu, R.; Choi, M.S. Differences in metabolic biomarkers in the blood and gene expression profiles of peripheral blood mononuclear cells among normal weight, mildly obese and moderately obese subjects. Br. J. Nutr. 2016, 116, 1022–1032. [Google Scholar] [CrossRef] [Green Version]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Capó, X.; Bouzas, C.; Mateos, D.; Pons, A.; Tur, J.A.; Sureda, A. Metabolic Syndrome is Associated with Oxidative Stress and Proinflammatory State. Antioxidants 2020, 9, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bories, G.; Caiazzo, R.; Derudas, B.; Copin, C.; Raverdy, V.; Pigeyre, M.; Pattou, F.; Staels, B.; Chinetti-Gbaguidi, G. Impaired alternative macrophage differentiation of peripheral blood mononuclear cells from obese subjects. Diabetes Vasc. Dis. Res. 2012, 9, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busquets-Cortés, C.; Capó, X.; del Mar Bibiloni, M.; Martorell, M.; Ferrer, M.D.; Argelich, E.; Bouzas, C.; Carreres, S.; Tur, J.A.; Pons, A.; et al. Peripheral blood mononuclear cells antioxidant adaptations to regular physical activity in elderly people. Nutrients 2018, 10, 1555. [Google Scholar] [CrossRef] [Green Version]
- Report of a who Expert Committee. Physical status: The use and interpretation of anthropometry. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S. Compendium of Physical Activities: Classification of energy costs of human physical activities. Med. Sci. Sport. Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef]
- Boyum, A. Separation of White Blood Cells. Nature 1964, 204, 793–794. [Google Scholar] [CrossRef]
- Aebi, H. Catalase in vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar]
- McCord, J.M.; Fridovich, I. Superoxide dismutase. An enzymic function for erythrocuprein (hemocuprein). J. Biol. Chem. 1969, 244, 6049–6055. [Google Scholar] [CrossRef]
- Glohé, L.; Gunzler, W. Assay of glutathione peroxidase. Methods Enzymol. 1984, 105, 114–121. [Google Scholar]
- Bergmayer, H.U. Glutathione reductase. Methods of Enzymatic Analysis. Starch Stärke 1963, 15, 272. [Google Scholar]
- Nihi, M.M.; Manfro, R.C.; Martins, C.; Suliman, M.; Murayama, Y.; Riella, M.C.; Lindholm, B.; Nascimento, M.M. do [Association between body fat, inflammation and oxidative stress in hemodialysis]. J. Bras. Nefrol. 2010, 32, 9–15. [Google Scholar] [PubMed]
- Sureda, A.; Bibiloni, M.; Julibert, A.; Bouzas, C.; Argelich, E.; Llompart, I.; Pons, A.; Tur, J. Adherence to the Mediterranean Diet and Inflammatory Markers. Nutrients 2018, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Ryder, E.; Diez-Ewald, M.; Mosquera, J.; Fernández, E.; Pedreañez, A.; Vargas, R.; Peña, C.; Fernández, N. Association of obesity with leukocyte count in obese individuals without metabolic syndrome. Diabetes Metab. Syndr. Clin. Res. Rev. 2014, 8, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Olefsky, J.M.; Glass, C.K. Macrophages, inflammation, and insulin resistance. Annu. Rev. Physiol. 2009, 72, 219–246. [Google Scholar] [CrossRef] [PubMed]
- Rocha, V.Z.; Folco, E.J.; Sukhova, G.; Shimizu, K.; Gotsman, I.; Vernon, A.H.; Libby, P. Interferon-γ, a Th1 cytokine, regulates fat inflammation: A role for adaptive immunity in obesity. Circ. Res. 2008, 103, 467–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgazar-Carmon, V.; Rudich, A.; Hadad, N.; Levy, R. Neutrophils transiently infiltrate intra-abdominal fat early in the course of high-fat feeding. J. Lipid Res. 2008, 49, 1894–1903. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez-Ruiz, J.; Velázquez-Paniagua, M.; Prieto-Gómez, B. El tejido adiposo como órgano maestro en el metabolismo. Rev. Endocrinol. Nutr. 2011, 19, 154–162. [Google Scholar]
- Adnan, M.T.; Amin, M.N.; Uddin, M.G.; Hussain, M.S.; Sarwar, M.S.; Hossain, M.K.; Uddin, S.M.N.; Islam, M.S. Increased concentration of serum MDA, decreased antioxidants and altered trace elements and macro-minerals are linked to obesity among Bangladeshi population. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 933–938. [Google Scholar] [CrossRef]
- Vincent, H.K.; Innes, K.E.; Vincent, K.R. Oxidative stress and potential interventions to reduce oxidative stress in overweight and obesity. Diabetes Obes. Metab. 2007, 9, 813–839. [Google Scholar] [CrossRef] [PubMed]
- Galan, P.; Viteri, F.E.; Bertrais, S.; Czernichow, S.; Faure, H.; Arnaud, J.; Ruffieux, D.; Chenal, S.; Arnault, N.; Favier, A.; et al. Serum concentrations of β-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur. J. Clin. Nutr. 2005, 59, 1181–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozata, M.; Mergen, M.; Oktenli, C.; Aydin, A.; Sanisoglu, S.Y.; Bolu, E.; Yilmaz, M.I.; Sayal, A.; Isimer, A.; Ozdemir, I.C. Increased oxidative stress and hypozincemia in male obesity. Clin. Biochem. 2002, 35, 627–631. [Google Scholar] [CrossRef]
- Olusi, S.O. Obesity is an independent risk factor for plasma lipid peroxidation and depletion of erythrocyte cytoprotectic enzymes in humans. Int. J. Obes. 2002, 26, 1159–1164. [Google Scholar] [CrossRef] [Green Version]
- Yue, K.K.M.; Chung, W.S.; Leung, A.W.N.; Cheng, C.H.K. Redox changes precede the occurrence of oxidative stress in eyes and aorta, but not in kidneys of diabetic rats. Life Sci. 2003, 73, 2557–2570. [Google Scholar] [CrossRef]
- Ladeiras-Lopes, R.; Teixeira, P.; Azevedo, A.; Leite-Moreira, A.; Bettencourt, N.; Fontes-Carvalho, R. Metabolic syndrome severity score is associated with diastolic dysfunction and low-grade inflammation in a community-based cohort. Eur. J. Prev. Cardiol. 2020, 27, 2330–2333. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, R.W.; Kay, T.; Lyle, E.A.; Traxler, S.A.; Deveney, C.W.; Jobe, B.A.; Roberts, C.T.; Marks, D.; Rosenbaum, J.T. Alterations in peripheral blood lymphocyte cytokine expression in obesity. Clin. Exp. Immunol. 2006, 146, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, H.; Aljada, A.; Hofmeyer, D.; Syed, T.; Mohanty, P.; Dandona, P. Circulating mononuclear cells in the obese are in a proinflammatory state. Circulation 2004, 110, 1564–1571. [Google Scholar] [CrossRef] [Green Version]
- Catalán, V.; Gómez-Ambrosi, J.; Rodríguez, A.; Ramírez, B.; Valentí, V.; Moncada, R.; Silva, C.; Salvador, J.; Frühbeck, G. Peripheral mononuclear blood cells contribute to the obesity-associated inflammatory state independently of glycemic status: Involvement of the novel proinflammatory adipokines chemerin, chitinase-3-like protein 1, lipocalin-2 and osteopontin. Genes Nutr. 2015, 10, 460. [Google Scholar] [CrossRef] [Green Version]
- Dicker, D.; Salook, M.A.; Marcoviciu, D.; Djaldetti, M.; Bessler, H. Role of peripheral blood mononuclear cells in the predisposition of obese individuals to inflammation and infection. Obes. Facts 2013, 6, 146–151. [Google Scholar] [CrossRef]
- Akhter, N.; Madhoun, A.; Arefanian, H.; Wilson, A.; Kochumon, S.; Thomas, R.; Shenouda, S.; Al-Mulla, F.; Ahmad, R.; Sindhu, S. Oxidative Stress Induces Expression of the Toll-Like Receptors (TLRs) 2 and 4 in the Human Peripheral Blood Mononuclear Cells: Implications for Metabolic Inflammation. Cell. Physiol. Biochem. 2019, 53, 1–18. [Google Scholar] [PubMed]
- Bondia-Pons, I.; Ryan, L.; Martinez, J.A. Oxidative stress and inflammation interactions in human obesity. J. Physiol. Biochem. 2012, 68, 701–711. [Google Scholar] [CrossRef]
- Bankoglu, E.E.; Gerber, J.; Kodandaraman, G.; Seyfried, F.; Stopper, H. Influence of bariatric surgery induced weight loss on oxidative DNA damage. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2020, 853, 503194. [Google Scholar] [CrossRef] [PubMed]
- Qaddoumi, M.G.; Alanbaei, M.; Hammad, M.M.; Al Khairi, I.; Cherian, P.; Channanath, A.; Thanaraj, T.A.; Al-Mulla, F.; Abu-Farha, M.; Abubaker, J. Investigating the Role of Myeloperoxidase and Angiopoietin-like Protein 6 in Obesity and Diabetes. Sci. Rep. 2020, 10, 6170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Abbate, M.; Montemayor, S.; Mascaró, C.M.; Casares, M.; Tejada, S.; Abete, I.; Zulet, M.A.; Tur, J.A.; et al. Oxidative stress and pro-inflammatory status in patients with non-alcoholic fatty liver disease. Antioxidants 2020, 9, 759. [Google Scholar] [CrossRef] [PubMed]
- Busquets-Cortés, C.; Capó, X.; Argelich, E.; Ferrer, M.D.; Mateos, D.; Bouzas, C.; Abbate, M.; Tur, J.A.; Sureda, A.; Pons, A. Effects of micromolar steady-state hydrogen peroxide exposure on inflammatory and redox gene expression in immune cells from humans with metabolic syndrome. Nutrients 2018, 10, 1920. [Google Scholar] [CrossRef] [Green Version]
- Djelić, N.; Radaković, M.; Borozan, S.; Dimirijević-Srećković, V.; Pajović, N.; Vejnović, B.; Borozan, N.; Bankoglu, E.E.; Stopper, H.; Stanimirović, Z. Oxidative stress and DNA damage in peripheral blood mononuclear cells from normal, obese, prediabetic and diabetic persons exposed to adrenaline in vitro. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2019, 843, 81–89. [Google Scholar] [CrossRef]
- Crujeiras, A.B.; Parra, D.; Milagro, F.I.; Goyenechea, E.; Larrarte, E.; Margareto, J.; Martínez, J.A. Differential expression of oxidative stress and inflammation related genes in peripheral blood mononuclear cells in response to a low-calorie diet: A nutrigenomics study. OMICS J. Integr. Biol. 2008, 12, 251–261. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Weight (n = 50) | Overweight (n = 50) | Obese (n = 50) | p-Value | |
|---|---|---|---|---|
| Age (years) | 65.6 ± 0.7 | 64.9 ± 0.7 | 64.0 ± 0.6 | 0.246 |
| Weight (kg) | 61.3 ± 1.1 | 74.5 ± 1.4 * | 92.9 ± 1.8 *# | <0.001 |
| Height (cm) | 161.9 ± 1.1 | 163.7 ± 1.4 | 162.3 ± 1.3 | 0.586 |
| BMI (kg/m2) | 23.0 ± 0.2 | 27.6 ± 0.2 * | 35.2 ± 0.4 *# | <0.001 |
| Total physical activity (MET·hour/week) | 66.6 ± 3.2 | 51.9 ± 4.0 | 46.9 ± 5.4 * | 0.007 |
| Systolic blood pressure (mmHg) | 136.8 ± 3.5 | 135.7 ± 2.3 | 135.2 ± 3.7 | 0.941 |
| Diastolic blood pressure (mmHg) | 78.3 ± 1.5 | 77.5 ± 1.3 | 76.9 ± 1.9 | 0.838 |
| Glucose (mg/dL) | 91.3 ± 1.0 | 101.2 ± 2.3 | 118.7 ± 4.8 *# | <0.001 |
| Triglycerides (mg/dL) | 91.6 ± 4.2 | 102.0 ± 5.1 | 154.5 ± 8.9 *# | <0.001 |
| HDL-cholesterol (mg/dL) | 61.5 ± 1.7 | 51.6 ± 1.4 * | 44.4 ± 1.3 *# | <0.001 |
| Abdominal obesity (cm) | 82.1 ± 1.6 | 93.7 ± 1.2 * | 115.3 ± 1.3 *# | <0.001 |
| WHtR | 0.51 ± 0.01 | 0.57 ± 0.01 * | 0.71 ± 0.01 *# | <0.001 |
| Normal Weight (n = 50) | Overweight (n = 50) | Obese (n = 50) | ANOVA | |
|---|---|---|---|---|
| Hematocrit (%) | 43.0 ± 0.5 | 43.7 ± 0.5 | 42.6 ± 0.59 | 0.367 |
| Erythrocytes (106/mm3) | 4.74 ± 0.06 | 4.79 ± 0.06 | 4.71 ± 0.07 | 0.715 |
| Leukocytes (103/mm3) | 6.39 ± 0.21 | 6.57 ± 0.25 | 7.45 ± 0.25 *# | 0.004 |
| Neutrophils (103/mm3) | 3.27 ± 0.16 | 3.57 ± 0.19 | 4.09 ± 0.16 * | 0.004 |
| Lymphocytes (103/mm3) | 2.36 ± 0.10 | 2.23 ± 0.09 | 2.45 ± 0.12 | 0.342 |
| Basophils (103/mm3) | 0.04 ± 0.00 | 0.048 ± 0.00 | 0.050 ± 0.00 * | 0.026 |
| Monocytes (103/mm3) | 0.48 ± 0.02 | 0.545 ± 0.03 | 0.633 ± 0.03 *# | <0.001 |
| Eosinophils (103/mm3) | 0.24 ± 0.03 | 0.18 ± 0.02 | 0.23 ± 0.02 | 0.150 |
| Normal Weight (n = 50) | Overweight (n = 50) | Obese (n = 50) | ANOVA | |
|---|---|---|---|---|
| PBMCs activity | ||||
| CAT (K/109 cells) | 10.8 ± 2.2 | 25.4 ± 3.1 * | 34.9 ± 3.8 * | <0.001 |
| GRd (nkat/109 cells) | 221 ± 46 | 305 ± 37 * | 448 ± 34 * | <0.001 |
| GPx (nkat/109 cells) | 53.4 ± 6.1 | 57.1 ± 5.4 | 73.7 ± 4.7 *# | 0.017 |
| SOD (nkat/109 cells) | 39.3 ± 4.8 | 59.3 ± 5.5 * | 74.7 ± 4.4 * | <0.001 |
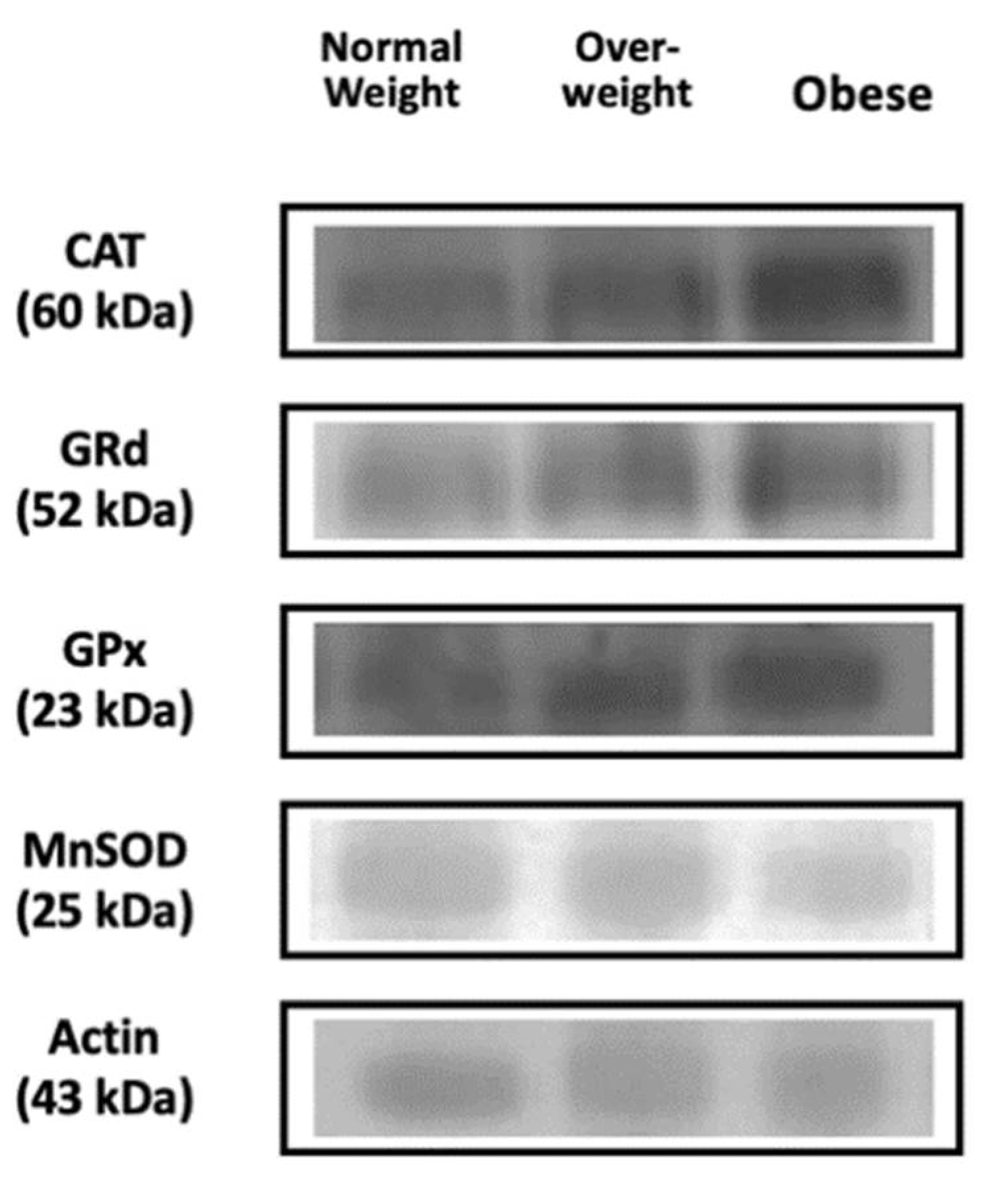
| PBMCs protein levels | ||||
| CAT (%) | 100 ± 12 | 127 ± 8 | 140 ± 8 * | 0.015 |
| GRd (%) | 100 ± 16 | 157 ± 14 * | 169 ± 13 * | 0.009 |
| GPx (%) | 100 ± 8 | 116 ± 6 | 118 ± 8 | 0.307 |
| MnSOD (%) | 100 ± 11 | 84.3 ± 9.8 | 77.7 ± 11.4 | 0.396 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Bouzas, C.; Capó, X.; Mateos, D.; Ugarriza, L.; Tur, J.A.; Sureda, A. Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity. Antioxidants 2021, 10, 813. https://doi.org/10.3390/antiox10050813
Monserrat-Mesquida M, Quetglas-Llabrés M, Bouzas C, Capó X, Mateos D, Ugarriza L, Tur JA, Sureda A. Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity. Antioxidants. 2021; 10(5):813. https://doi.org/10.3390/antiox10050813
Chicago/Turabian StyleMonserrat-Mesquida, Margalida, Magdalena Quetglas-Llabrés, Cristina Bouzas, Xavier Capó, David Mateos, Lucía Ugarriza, Josep A. Tur, and Antoni Sureda. 2021. "Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity" Antioxidants 10, no. 5: 813. https://doi.org/10.3390/antiox10050813
APA StyleMonserrat-Mesquida, M., Quetglas-Llabrés, M., Bouzas, C., Capó, X., Mateos, D., Ugarriza, L., Tur, J. A., & Sureda, A. (2021). Peripheral Blood Mononuclear Cells Oxidative Stress and Plasma Inflammatory Biomarkers in Adults with Normal Weight, Overweight and Obesity. Antioxidants, 10(5), 813. https://doi.org/10.3390/antiox10050813