
Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord

 ,
,  , , , ,
, , , , 

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Tissue Samples
2.3. Genetic and Molecular Studies
2.4. Immunohistochemical Studies
2.5. Lipid Peroxidation Assay
2.6. Statistical Analysis
3. Results
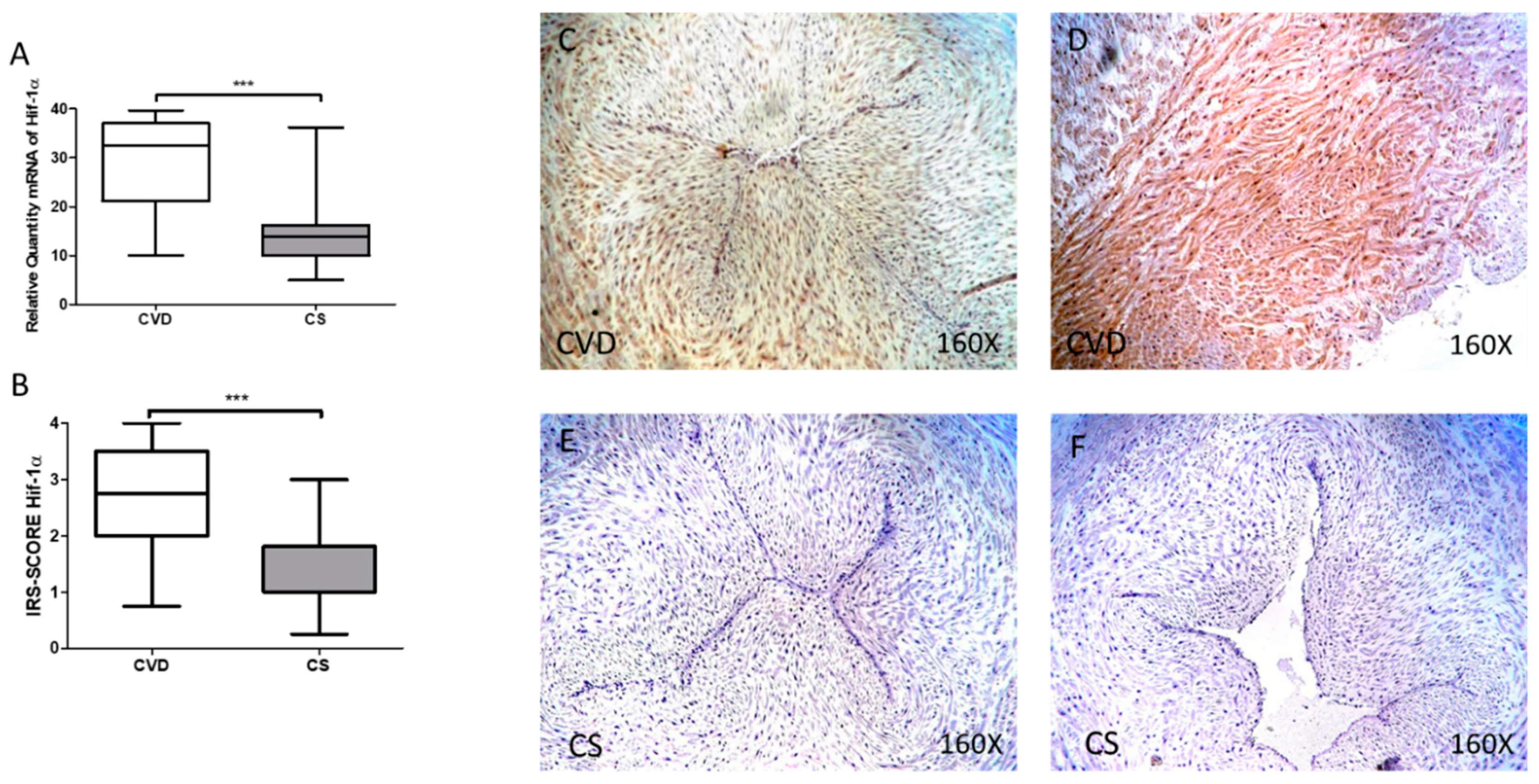
3.1. The Umbilical Cords of Newborns of Mothers Who Had CVD during Pregnancy Show an Increase in Tissue Markers of Hypoxia
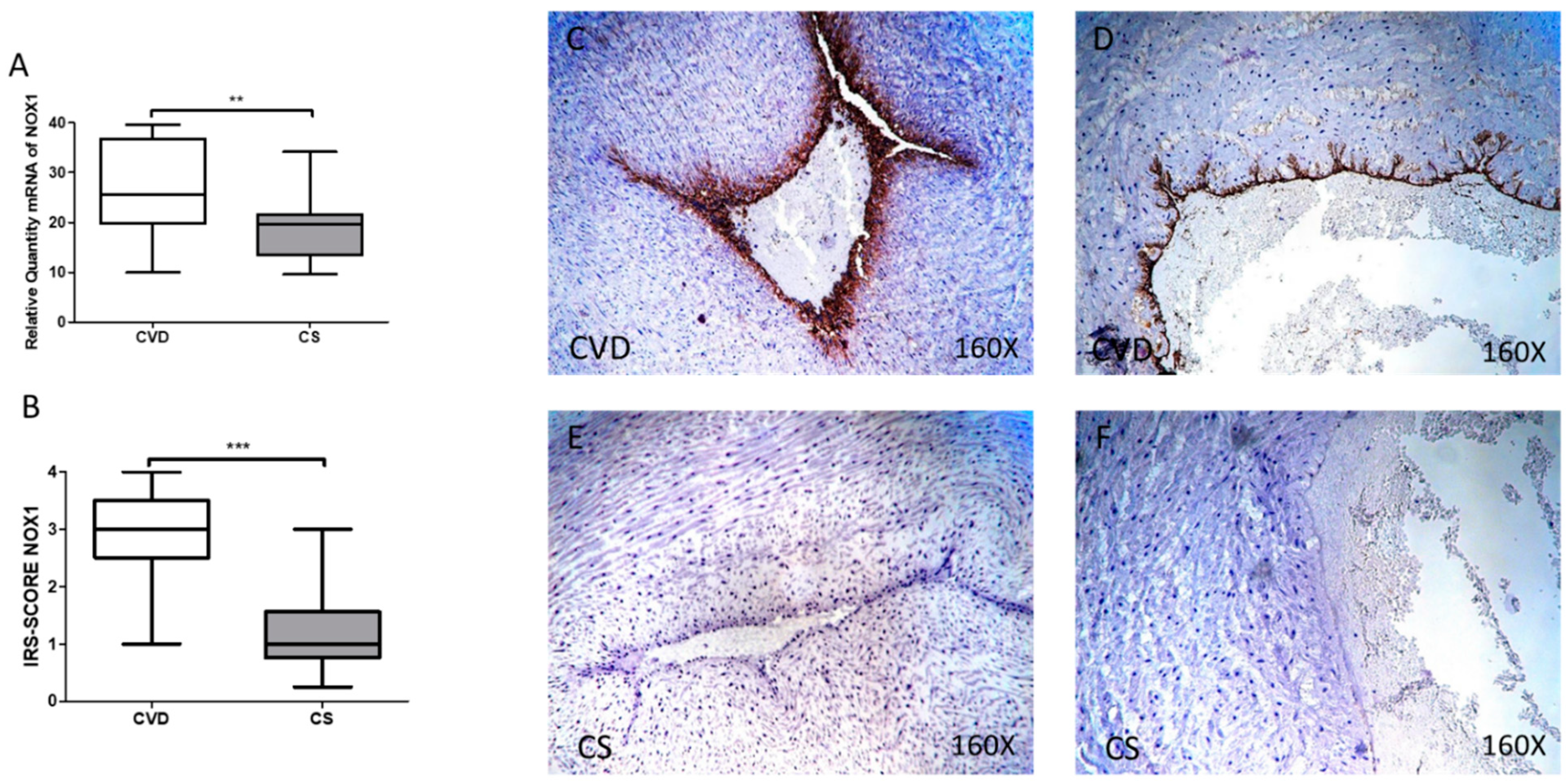
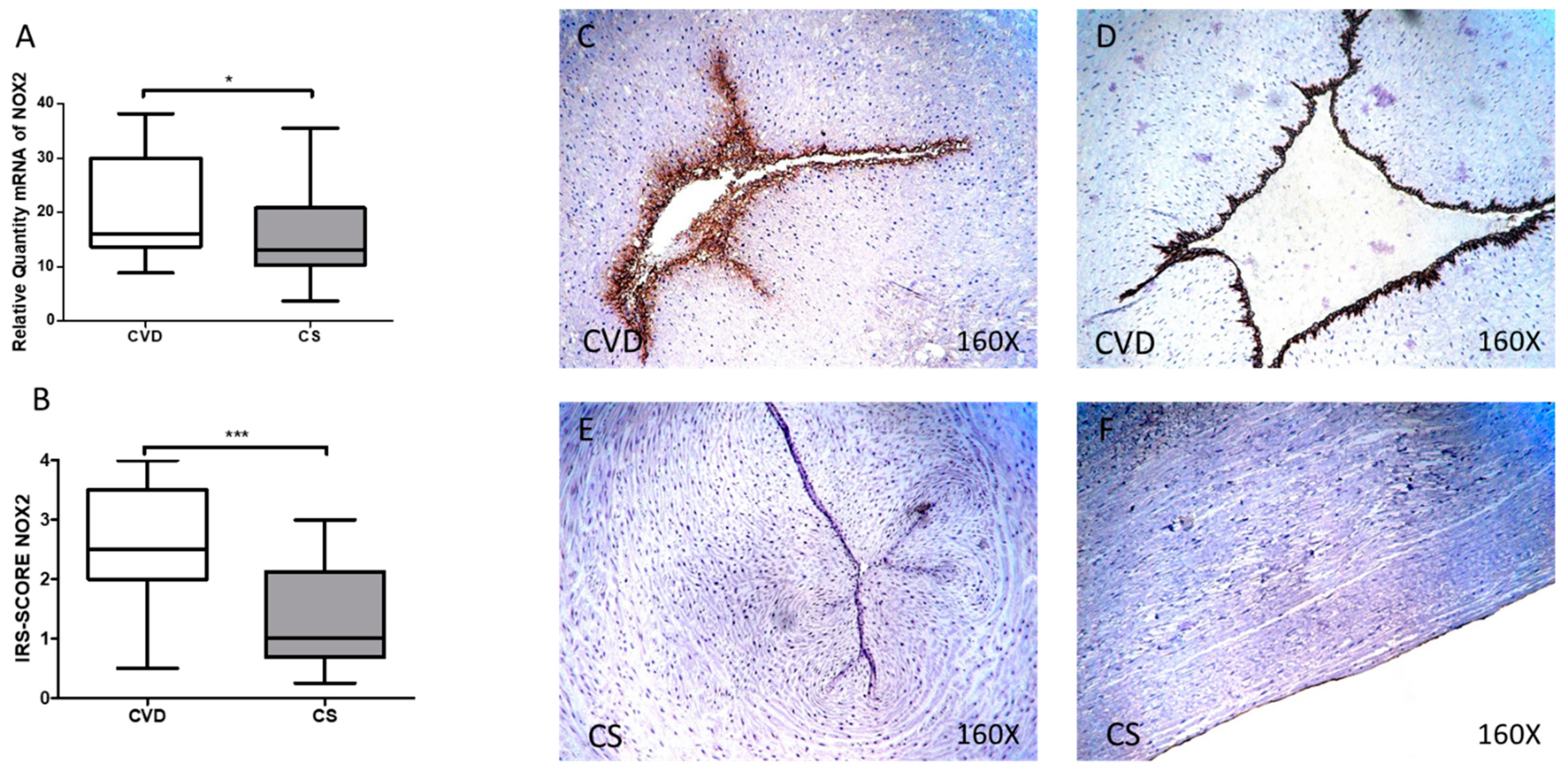
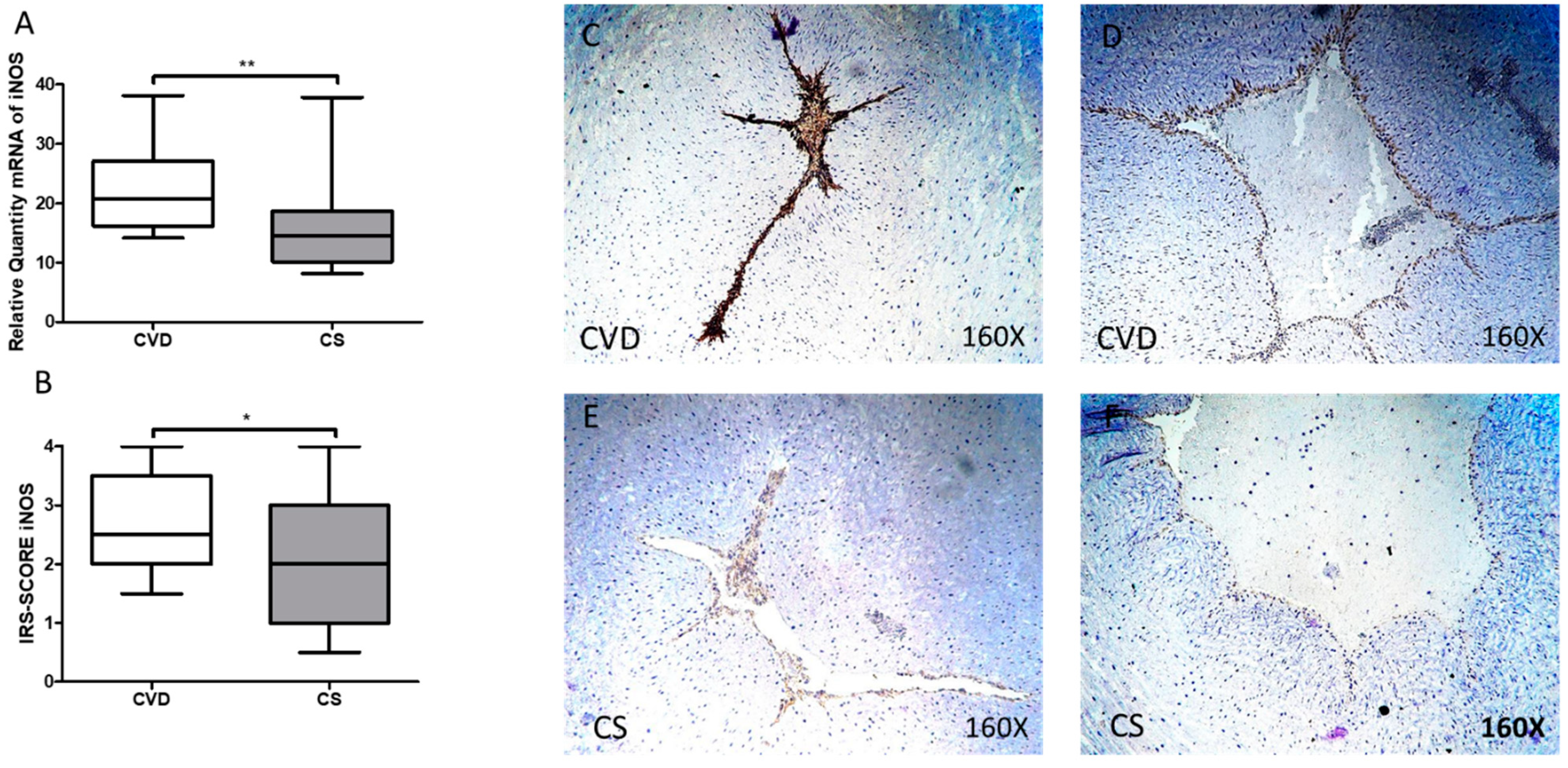
3.2. The Umbilical Cords of Newborns Whose Mothers had CVD during Pregnancy Show an Increase in Tissue Markers of Oxidative Stress
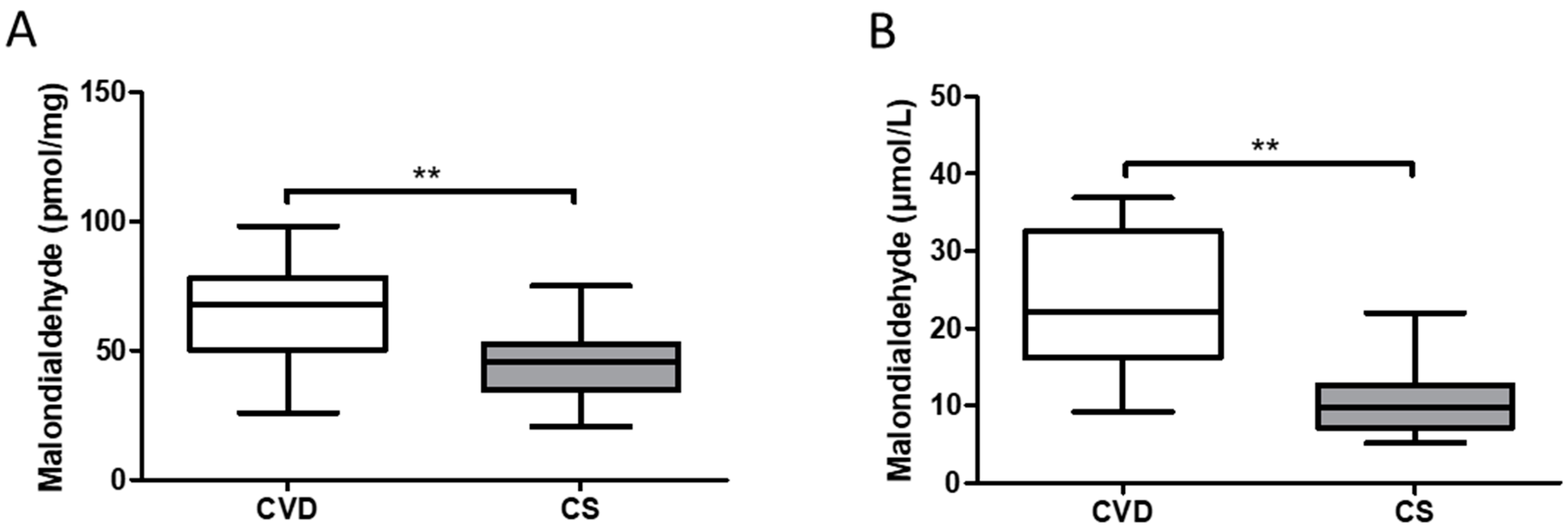
3.3. Newborns Whose Mothers had CVD during Pregnancy Show Increased Levels of Malondialdehyde at the Tissue and Plasma Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tan, E.K.; Tan, E.L. Alterations in physiology and anatomy during pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 791–802. [Google Scholar] [CrossRef]
- Morton, A. Physiological Changes and Cardiovascular Investigations in Pregnancy. Hear. Lung Circ. 2021, 30, e6–e15. [Google Scholar] [CrossRef]
- Al-Sulttan, S.; Achary, C.; Odor, P.M.; Bampoe, S. Obstetric anaesthesia 1: Physiological changes in pregnancy. Br. J. Hosp. Med. 2019, 80, C107–C111. [Google Scholar] [CrossRef] [PubMed]
- Troiano, N.H. Physiologic and hemodynamic changes during pregnancy. AACN Adv. Crit. Care 2018, 29, 273–283. [Google Scholar] [CrossRef]
- Mahendru, A.A.; Everett, T.R.; Wilkinson, I.B.; Lees, C.C.; McEniery, C.M. Maternal cardiovascular changes from pre-pregnancy to very early pregnancy. J. Hypertens. 2012, 30, 2168–2172. [Google Scholar] [CrossRef]
- Aleksenko, L.; Quaye, I.K. Pregnancy-induced Cardiovascular Pathologies: Importance of Structural Components and Lipids. Am. J. Med. Sci. 2020, 360, 447–466. [Google Scholar] [CrossRef]
- Raffetto, J.D.; Mannello, F. Pathophysiology of chronic venous disease. Int. Angiol. 2014, 33, 212–221. [Google Scholar]
- Eberhardt, R.T.; Raffetto, J.D. Chronic venous insufficiency. Circulation 2014, 130, 333–346. [Google Scholar] [CrossRef]
- Labropoulos, N. How Does Chronic Venous Disease Progress from the First Symptoms to the Advanced Stages? A Review. Adv. Ther. 2019, 36, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Ismail, L.; Normahani, P.; Standfield, N.J.; Jaffer, U. A systematic review and meta-analysis of the risk for development of varicose veins in women with a history of pregnancy. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 518–524.e1. [Google Scholar] [CrossRef]
- Taylor, J.; Hicks, C.W.; Heller, J.A. The hemodynamic effects of pregnancy on the lower extremity venous system. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 246–255. [Google Scholar] [CrossRef]
- García-Honduvilla, N.; Ortega, M.A.; Asúnsolo, Á.; Álvarez-Rocha, M.J.; Romero, B.; De León-Luis, J.; Álvarez-Mon, M.; Buján, J. Placentas from women with pregnancy-associated venous insufficiency show villi damage with evidence of hypoxic cellular stress. Hum. Pathol. 2018, 77, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, K.; Morikage, N.; Harada, T.; Samura, M.; Nagase, T.; Takeuchi, Y.; Mizoguchi, T.; Nakamura, K.; Hamano, K. Extracellular Fluid Content in the Legs of Patients with Chronic Venous Disease. Ann. Vasc. Surg. 2021, 71, 215–219. [Google Scholar] [CrossRef]
- Gifre-Renom, L.; Jones, E.A.V. Vessel Enlargement in Development and Pathophysiology. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Saez, M.A.; Fraile-Martínez, O.; Asúnsolo, Á.; Pekarek, L.; Bravo, C.; Coca, S.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; et al. Increased angiogenesis and lymphangiogenesis in the placental villi of women with chronic venous disease during pregnancy. Int. J. Mol. Sci. 2020, 21, 2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, M.A.; Saez, M.Á.; Asúnsolo, Á.; Romero, B.; Bravo, C.; Coca, S.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Upregulation of VEGF and PEDF in Placentas of Women with Lower Extremity Venous Insufficiency during Pregnancy and Its Implication in Villous Calcification. BioMed Res. Int. 2019, 2019. [Google Scholar] [CrossRef]
- Ortega, M.A.; Saez, M.A.; Sainz, F.; Fraile-Martínez, O.; García-Gallego, S.; Pekarek, L.; Bravo, C.; Coca, S.; Álvarez-Mon, M.; Buján, J.; et al. Lipidomic profiling of chorionic villi in the placentas of women with chronic venous disease. Int. J. Med. Sci. 2020, 17, 2790–2798. [Google Scholar] [CrossRef]
- Ortega, M.A.; Romero, B.; Asúnsolo, Á.; Sola, M.; Álavrez-Rocha, M.J.; Sainz, F.; Álavrez-Mon, M.; Buján, J.; García-Honduvilla, N. Patients with incompetent valves in chronic venous insufficiency show increased systematic lipid peroxidation and cellular oxidative stress markers. Oxid. Med. Cell. Longev. 2019, 2019. [Google Scholar] [CrossRef]
- Krzyściak, W.; Kózka, M. Generation of reactive oxygen species by a sufficient, insufficient and varicose vein wall. Acta Biochim. Pol. 2011, 58, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017. [Google Scholar] [CrossRef]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [Green Version]
- Dubois-deruy, E.; Peugnet, V.; Turkieh, A.; Pinet, F. Oxidative stress in cardiovascular diseases. Antioxidants 2020, 9, 864. [Google Scholar] [CrossRef]
- Pereira, R.D.; De Long, N.E.; Wang, R.C.; Yazdi, F.T.; Holloway, A.C.; Raha, S. Angiogenesis in the placenta: The role of reactive oxygen species signaling. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoots, M.H.; Gordijn, S.J.; Scherjon, S.A.; van Goor, H.; Hillebrands, J.L. Oxidative stress in placental pathology. Placenta 2018, 69, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Bedard, K.; Krause, K.H. The NOX family of ROS-generating NADPH oxidases: Physiology and pathophysiology. Physiol. Rev. 2007, 87, 245–313. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Romero, B.; Asúnsolo, Á.; Martínez-Vivero, C.; Sainz, F.; Bravo, C.; De León-Luis, J.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Pregnancy-associated venous insufficiency course with placental and systemic oxidative stress. J. Cell. Mol. Med. 2020, 24, 4157–4170. [Google Scholar] [CrossRef] [Green Version]
- Sarikabadayi, Y.U.; Aydemir, O.; Aydemir, C.; Uras, N.; Oguz, S.S.; Erdeve, O.; Dilmen, U. Umbilical cord oxidative stress in infants of diabetic mothers and its relation to maternal hyperglycemia. J. Pediatr. Endocrinol. Metab. 2011, 24, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Echeverri, I.; Ortega-Ávila, J.G.; Mosquera, M.; Castillo, A.; Jiménez, E.; Suárez-Ortegon, M.F.; Mateus, J.C.; Aguilar-de Plata, C. Relationship between maternal and newborn endothelial function and oxidative stress. Am. J. Hum. Biol. 2015, 27, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Perrone, S.; Laschi, E.; Buonocore, G. Biomarkers of oxidative stress in the fetus and in the newborn. Free Radic. Biol. Med. 2019, 142, 23–31. [Google Scholar] [CrossRef]
- Perrone, S.; Laschi, E.; Buonocore, G. Oxidative stress biomarkers in the perinatal period: Diagnostic and prognostic value. Semin. Fetal Neonatal Med. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Draganovic, D.; Lucic, N.; Jojic, D.; Milicevic, S. Correlation of oxidative stress markers with ultrasound and cardiotocography parameters with hypertension induced pregnancy. Acta Inform. Med. 2017, 25, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; De Maeseneer, M.; et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Sanmartín-Salinas, P.; Guijarro, L.G. Overexpression of IRS-4 Correlates with Procaspase 3 Levels in Tumoural Tissue of Patients with Colorectal Cancer. J. Oncol. 2018, 2018, 3812581. [Google Scholar] [CrossRef]
- Furness, D.L.F.; Dekker, G.A.; Roberts, C.T. DNA damage and health in pregnancy. J. Reprod. Immunol. 2011, 89, 153–162. [Google Scholar] [CrossRef]
- Al-Gubory, K.H.; Fowler, P.A.; Garrel, C. The roles of cellular reactive oxygen species, oxidative stress and antioxidants in pregnancy outcomes. Int. J. Biochem. Cell Biol. 2010, 42, 1634–1650. [Google Scholar] [CrossRef]
- Burtenshaw, D.; Hakimjavadi, R.; Redmond, E.M.; Cahill, P.A. Nox, reactive oxygen species and regulation of vascular cell fate. Antioxidants 2017, 6, 90. [Google Scholar] [CrossRef] [Green Version]
- Manea, S.A.; Constantin, A.; Manda, G.; Sasson, S.; Manea, A. Regulation of Nox enzymes expression in vascular pathophysiology: Focusing on transcription factors and epigenetic mechanisms. Redox Biol. 2015, 5, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.L.; Brockman, D.; Campos, B.; Myatt, L. Expression of NADPH oxidase isoform 1 (Nox1) in human placenta: Involvement in preeclampsia. Placenta 2006, 27, 422–431. [Google Scholar] [CrossRef] [Green Version]
- Aouache, R.; Biquard, L.; Vaiman, D.; Miralles, F. Oxidative stress in preeclampsia and placental diseases. Int. J. Mol. Sci. 2018, 19, 1496. [Google Scholar] [CrossRef] [Green Version]
- Guerby, P.; Tasta, O.; Swiader, A.; Pont, F.; Bujold, E.; Parant, O.; Vayssiere, C.; Salvayre, R.; Negre-Salvayre, A. Role of oxidative stress in the dysfunction of the placental endothelial nitric oxide synthase in preeclampsia. Redox Biol. 2021, 40. [Google Scholar] [CrossRef]
- Choi, S.; Kim, J.A.; Na, H.Y.; Kim, J.E.; Park, S.; Han, K.H.; Kim, Y.J.; Suh, S.H. NADPH oxidase 2-derived superoxide downregulates endothelial K Ca3.1 in preeclampsia. Free Radic. Biol. Med. 2013, 57, 10–21. [Google Scholar] [CrossRef]
- Brandes, R.P.; Weissmann, N.; Schröder, K. Nox family NADPH oxidases: Molecular mechanisms of activation. Free Radic. Biol. Med. 2014, 76, 208–226. [Google Scholar] [CrossRef]
- Salvolini, E.; Vignini, A.; Sabbatinelli, J.; Lucarini, G.; Pompei, V.; Sartini, D.; Cester, A.M.; Ciavattini, A.; Mazzanti, L.; Emanuelli, M. Nitric oxide synthase and VEGF expression in full-term placentas of obese women. Histochem. Cell Biol. 2019, 152, 415–422. [Google Scholar] [CrossRef]
- Du, L.; He, F.; Kuang, L.; Tang, W.; Li, Y.; Chen, D. ENOS/iNOS and endoplasmic reticulum stress-induced apoptosis in the placentas of patients with preeclampsia. J. Hum. Hypertens. 2017, 31, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Chruściel, M.; Andronowska, A.; Postek, A. Expression patterns of endothelial and inducible nitric oxide isoforms in the porcine umbilical cord. Reprod. Domest. Anim. 2009, 44, 621–630. [Google Scholar] [CrossRef]
- Mauro, A.; Buscemi, M.; Provenzano, S.; Gerbino, A. Human umbilical cord expresses several vasoactive peptides involved in the local regulation of vascular tone: Protein and gene expression of Orphanin, Oxytocin, ANP, eNOS and iNOS. Folia Histochem. Cytobiol. 2011, 49, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Sezer, S.D.; Küçük, M.; Nergiz Avcioʇlu, S.; Zafer, E.; Altinkaya, S.Ö.; Biçakçi, B.; Yenisey, Ç.; Yüksel, H.; Kurt Ömürlü, I. Comparison of maternal and umbilical cord blood HIF-1 α and nitric oxide levels in early and late onset preeclamptic pregnancies. Gynecol. Endocrinol. 2015, 31, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Movafagh, S.; Crook, S.; Vo, K. Regulation of hypoxia-inducible Factor-1a by reactive oxygen species: New developments in an old debate. J. Cell. Biochem. 2015, 116, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, B.; Novakov-Mikic, A.; Brkic, S.; Bogavac, M.A.; Tomic, S.; Miler, V. Lipid peroxidation in the first trimester of pregnancy. J. Matern. Neonatal Med. 2012, 25, 1316–1318. [Google Scholar] [CrossRef]
- Ozsurekci, Y.; Aykac, K. Oxidative Stress Related Diseases in Newborns. Oxid. Med. Cell. Longev. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CVD (n = 62) | CS (n = 52) | |
|---|---|---|
| Median age [IQR] | 33 [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] | 34 [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] |
| Gestational age (wk) median [IQR] | 40.5 [39–41.5] | 41 [39,40,41,42] |
| Previous pregnancies | 33 (53.2%) | 19 (36.5%) |
| C-section delivery | 12 (19.4%) | 9 (17.3%) |
| CEAP | ||
| C1 | 37 (59.7%) | 0 (0%) |
| C2 | 21 (33.8%) | 0 (0%) |
| C3 | 4 (6.5%) | 0 (0%) |
| Newborn body weigh (gr) | 3190.00 [2069.00–3890.00] | 3250.00 [4050.00–2055.00] |
| Newborn size (cm) | 48.00 [41.00–50.00] | 49.00 [42.00–53.00] |
| Apgar score (1 min) ** | 7.00 [5.00–10.00] | 9.00 [6.00–10.00] |
| Apgar score (5 min) * | 8.00 [5.00–10.00] | 9.00 [8.00–10.00] |
| GENE | SEQUENCE Fwd (5′→3′) | SEQUENCE Rev (5′→3′) | Temp |
|---|---|---|---|
| TBP | TGC ACA GGA GCC AAG AGT GAA | CAC ATC ACA GCT CCC CAC CA | 60 °C |
| Hif-1α | ACGTGTTATCTGTCGCTTTGAG | ATCGTCTGGCTGCTGTAATAATG | 59 °C |
| iNOS | CCT TAC GAG GCG AAG AAG GAC AG | CAG TTT GAG AGA GGA GGC TCC G | 61 °C |
| NOX1 | GTT TTA CCG CTC CCA GCA GAA | GGA TGC CAT TCC AGG AGA GAG | 55 °C |
| NOX2 | TCC GCA TCG TTG GGG ACT GGA | CCA AAG GGC CCA TCA ACC GCT | 60 °C |
| (A) | ||||
| Antigen | Species | Dilution | Provider | Protocol Specifications |
| NOX 1 | Rabbit | 1:250 | Abcam (ab78016) | 10 mM Sodium citrate pH = 6 before incubation with blocking solution |
| NOX 2 | Goat | 1:500 | Abcam (ab111175) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| iNOS | Rabbit | 1:350 | Abcam (ab95866) | 10 mM Sodium citrate pH = 6 before incubation with blocking solution |
| Hif-1α | Mouse | 1:800 | Abcam (ab16066) | EDTA at pH 9 before incubation with blocking solution |
| (B) | ||||
| Antigen | Species | Dilution | Provider | Protocol Specifications |
| IgG (Mouse) | Goat | 1:300 | Sigma-Aldrich (F2012/045K6072) | -------------------- |
| IgG (Rabbit) | Mouse | 1:1000 | Sigma-Aldrich (RG-96/B5283) | -------------------- |
| IgG (Goat) | Mouse | 1:100 | Sigma-Aldrich (A5420) | -------------------- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, M.A.; Sánchez-Trujillo, L.; Bravo, C.; Fraile-Martinez, O.; García-Montero, C.; Saez, M.A.; Alvarez-Mon, M.A.; Sainz, F.; Alvarez-Mon, M.; Bujan, J.; et al. Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord. Antioxidants 2021, 10, 980. https://doi.org/10.3390/antiox10060980
Ortega MA, Sánchez-Trujillo L, Bravo C, Fraile-Martinez O, García-Montero C, Saez MA, Alvarez-Mon MA, Sainz F, Alvarez-Mon M, Bujan J, et al. Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord. Antioxidants. 2021; 10(6):980. https://doi.org/10.3390/antiox10060980
Chicago/Turabian StyleOrtega, Miguel A., Lara Sánchez-Trujillo, Coral Bravo, Oscar Fraile-Martinez, Cielo García-Montero, Miguel A. Saez, Miguel A. Alvarez-Mon, Felipe Sainz, Melchor Alvarez-Mon, Julia Bujan, and et al. 2021. "Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord" Antioxidants 10, no. 6: 980. https://doi.org/10.3390/antiox10060980
APA StyleOrtega, M. A., Sánchez-Trujillo, L., Bravo, C., Fraile-Martinez, O., García-Montero, C., Saez, M. A., Alvarez-Mon, M. A., Sainz, F., Alvarez-Mon, M., Bujan, J., De Leon-Luis, J. A., & García-Honduvilla, N. (2021). Newborns of Mothers with Venous Disease during Pregnancy Show Increased Levels of Lipid Peroxidation and Markers of Oxidative Stress and Hypoxia in the Umbilical Cord. Antioxidants, 10(6), 980. https://doi.org/10.3390/antiox10060980