
Severe Glutathione Deficiency, Oxidative Stress and Oxidant Damage in Adults Hospitalized with COVID-19: Implications for GlyNAC (Glycine and N-Acetylcysteine) Supplementation

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approval
2.2. Participants
2.3. Study Details
2.4. Outcome Measures
2.4.1. Glutathione Concentrations and Oxidative Stress
2.4.2. Plasma Biochemistry
2.5. Statistical Methods
3. Results
3.1. Age
3.2. Plasma Biochemistry
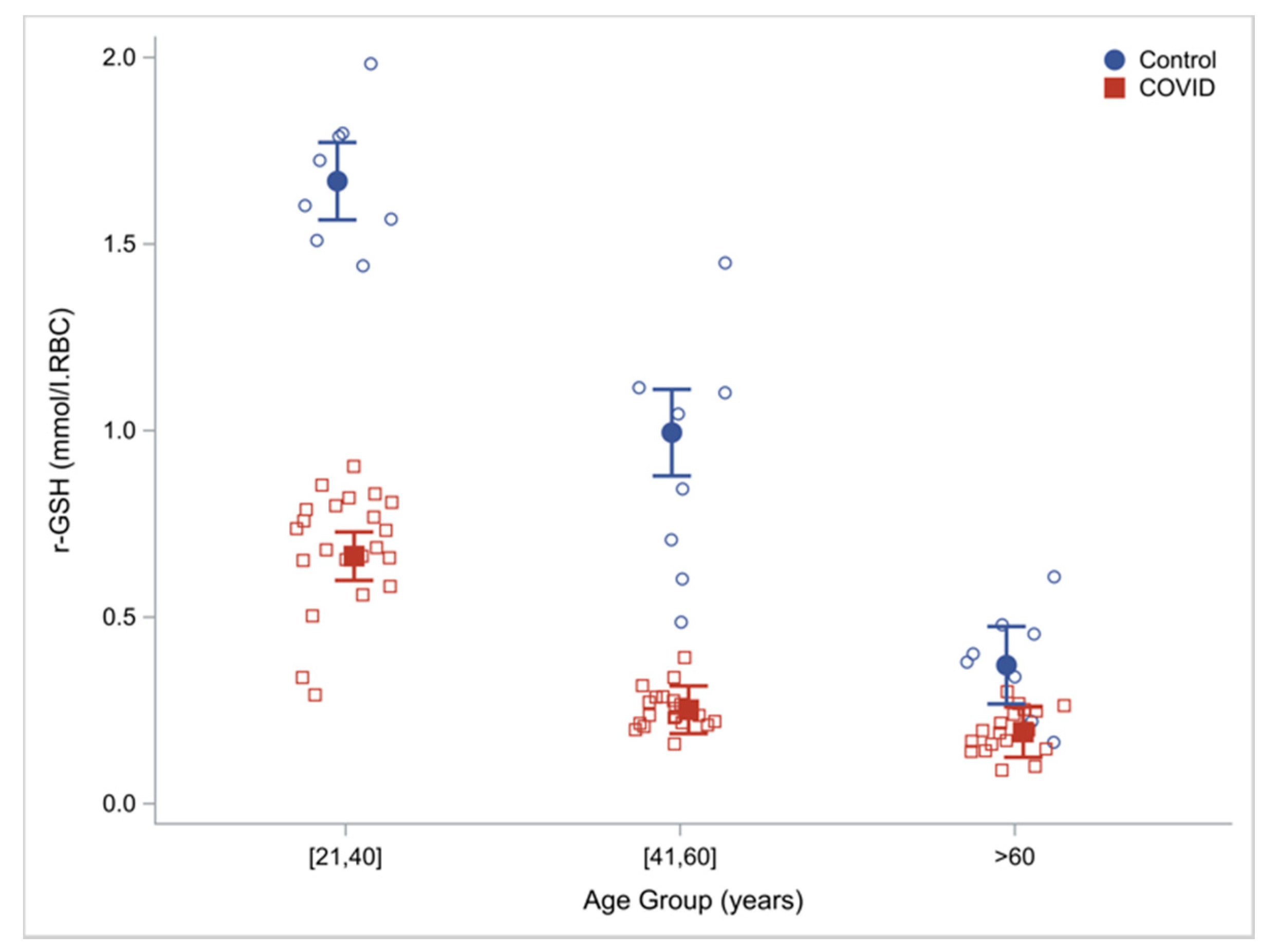
3.3. GSH Adequacy
3.4. Oxidative Stress
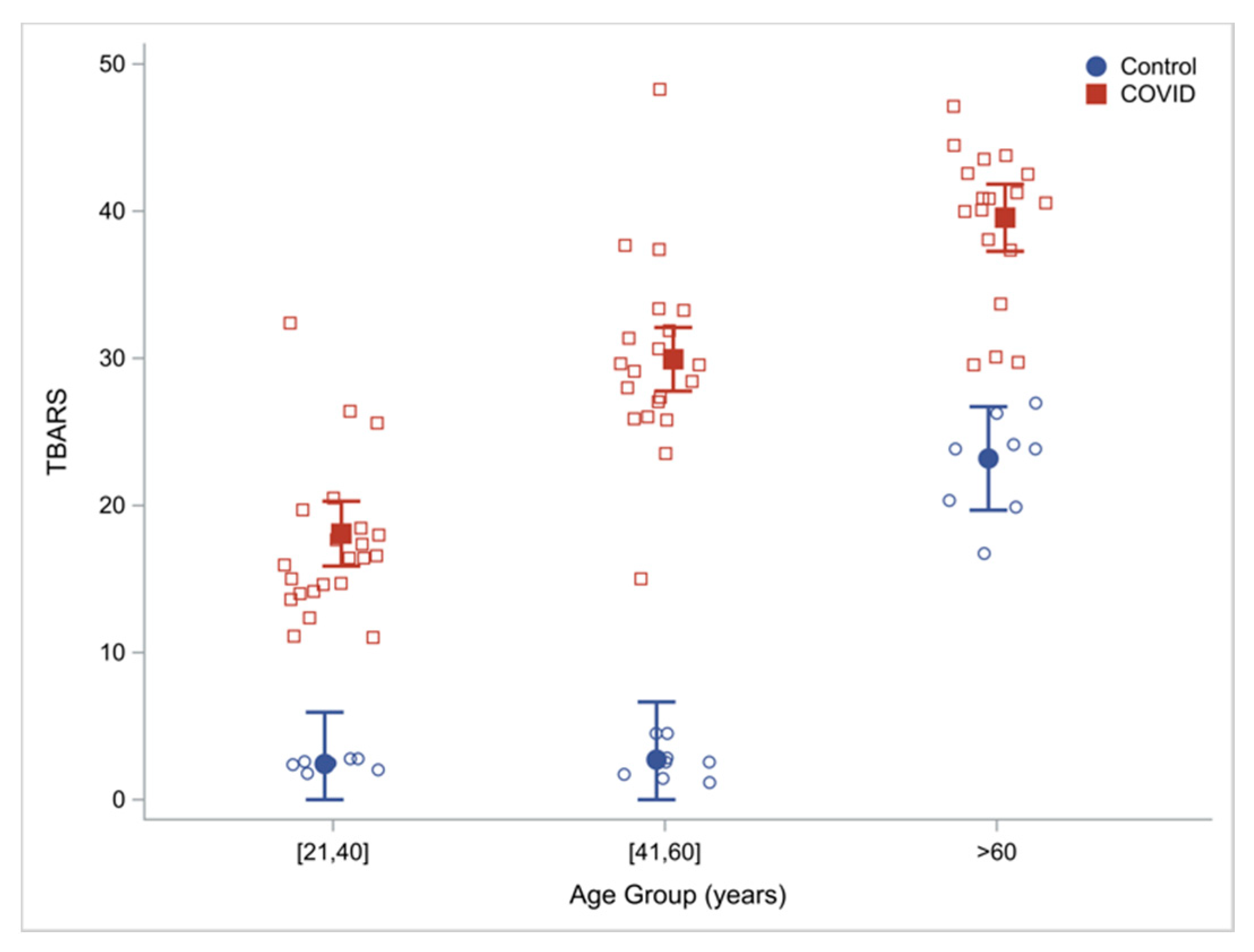
3.4.1. Oxidative Stress
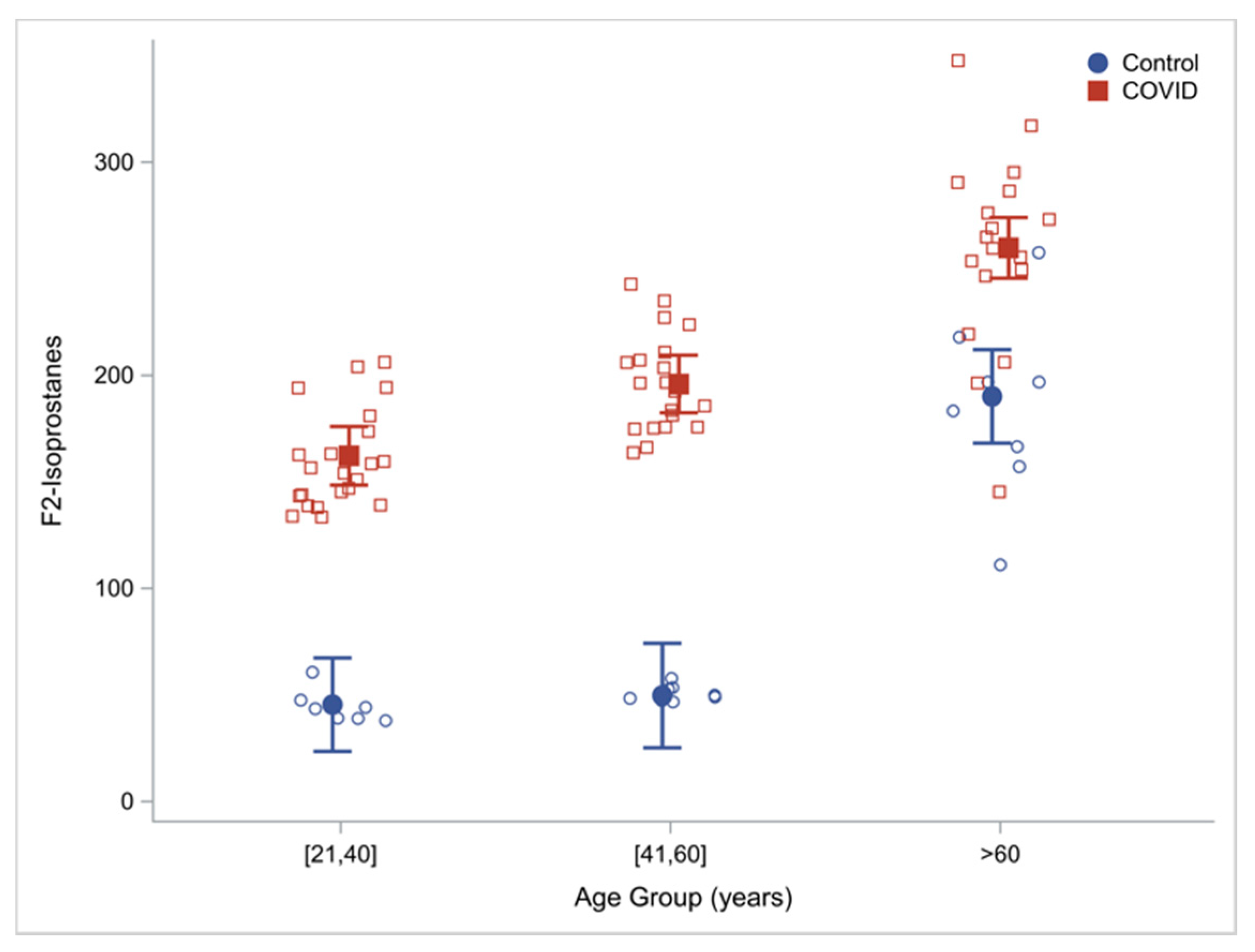
3.4.2. Damage Due to OxS (Oxidant Damage)
4. Discussion
4.1. GSH Deficiency in COVID-19
4.2. Oxidative Stress and Oxidant Damage in COVID-19
4.3. Potential Benefits of GlyNAC Supplementation in COVID-19
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://web.archive.org/web/20211130225803/https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 November 2021).
- Centers for Disease Control and Prevention. Available online: https://web.archive.org/web/20211201200354/https://www.cdc.gov/coronavirus/2019-ncov/ (accessed on 2 December 2021).
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://web.archive.org/web/20211201012905/https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 1 December 2021).
- Mainous, A.G.; Rooks, B.J.; Wu, V.; Orlando, F.A. COVID-19 Post-Acute Sequelae among Adults: 12 Month Mortality Risk. Front. Med. 2021, 8, 2351. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Risk for COVID-19 Infection, Hospitalization, and Death by Age Group. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 1 December 2021).
- Kirkham, P.A.; Barnes, P.J. Oxidative stress in COPD. Chest 2013, 144, 266–273. [Google Scholar] [CrossRef]
- Van der Vliet, A.; Janssen-Heininger, Y.M.W.; Anathy, V. Oxidative stress in chronic lung disease: From mitochondrial dysfunction to dysregulated redox signaling. Mol. Asp. Med. 2018, 63, 59–69. [Google Scholar] [CrossRef]
- Kibel, A.; Lukinac, A.M.; Dambic, V.; Juric, I.; Selthofer-Relatic, K. Oxidative Stress in Ischemic Heart Disease. Oxid. Med. Cell Longev. 2020, 2020, 6627144. [Google Scholar] [CrossRef]
- Peoples, J.N.; Saraf, A.; Ghazal, N.; Pham, T.T.; Kwong, J.Q. Mitochondrial dysfunction and oxidative stress in heart disease. Exp. Mol. Med. 2019, 51, 1–13. [Google Scholar] [CrossRef]
- Jiang, T.; Sun, Q.; Chen, S. Oxidative stress: A major pathogenesis and potential therapeutic target of antioxidative agents in Parkinson’s disease and Alzheimer’s disease. Prog. Neurobiol. 2016, 147, 1–19. [Google Scholar] [CrossRef]
- Giacco, F.; Brownlee, M. Oxidative stress and diabetic complications. Circ Res. 2010, 107, 1058–1070. [Google Scholar] [CrossRef] [Green Version]
- Ashraf, N.U.; Sheikh, T.A. Endoplasmic reticulum stress and Oxidative stress in the pathogenesis of Non-alcoholic fatty liver disease. Free Radic. Res. 2015, 49, 1405–1418. [Google Scholar] [CrossRef]
- Daenen, K.; Andries, A.; Mekahli, D.; Van Schepdael, A.; Jouret, F.; Bammens, B. Oxidative stress in chronic kidney disease. Pediatr. Nephrol. 2019, 34, 975–991. [Google Scholar] [CrossRef] [Green Version]
- Harman, D. Aging: A theory based on free radical and radiation chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Mills, K.; Le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res Rev. 2020, 57, 100982. [Google Scholar] [CrossRef]
- Ballatori, N.; Krance, S.M.; Notenboom, S.; Shi, S.; Tieu, K.; Hammond, C.L. Glutathione dysregulation and the etiology and progression of human diseases. Biol. Chem. 2009, 390, 191–214. [Google Scholar] [CrossRef] [Green Version]
- Teskey, G.; Abrahem, R.; Cao, R.; Gyurjian, K.; Islamoglu, H.; Lucero, M.; Martinez, A.; Paredes, E.; Salaiz, O.; Robinson, B.; et al. Glutathione as a Marker for Human Disease. Adv. Clin. Chem. 2018, 87, 141–159. [Google Scholar] [CrossRef]
- Wu, G.; Fang, Y.Z.; Yang, S.; Lupton, J.R.; Turner, N.D. Glutathione metabolism and its implications for health. J. Nutr. 2004, 134, 489–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, A.; Vura, N.V.R.K.; Gravenstein, S. COVID-19 in older adults. Aging Clin. Exp. Res. 2020, 32, 1199–1202. [Google Scholar] [CrossRef]
- Powell, T.; Bellin, E.; Ehrlich, A.R. Older Adults and Covid-19: The Most Vulnerable, the Hardest Hit. Hastings Cent. Rep. 2020, 50, 61–63. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lu, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid-19). Diabetes Metab. Res. Rev. 2021, 37, e3377. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Yang, Y.; Wang, F.; Ren, H.; Zhang, S.; Shi, X.; Yu, X.; Dong, K. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001343. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2021, 8, e24–e32. [Google Scholar] [CrossRef]
- Sekhar, R.V.; Patel, S.G.; Guthikonda, A.P.; Reid, M.; Balasubramanyam, A.; Taffet, G.E.; Jahoor, F. Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. Am. J. Clin. Nutr. 2011, 94, 847–853. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, R.V.; McKay, S.V.; Patel, S.G.; Guthikonda, A.P.; Reddy, V.T.; Balasubramanyam, A.; Jahoor, F. Glutathione synthesis is diminished in patients with uncontrolled diabetes and restored by dietary supplementation with cysteine and glycine. Diabetes Care 2011, 34, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.; Hsu, J.W.; Jahoor, F.; Sekhar, R.V. Effect of increasing glutathione with cysteine and glycine supplementation on mitochondrial fuel oxidation, insulin sensitivity, and body composition in older HIV-infected patients. J. Clin. Endocrinol. Metab. 2014, 99, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, D.; Samson, S.L.; Reddy, V.T.; Gonzalez, E.V.; Sekhar, R.V. Impaired mitochondrial fatty acid oxidation and insulin resistance in aging: Novel protective role of glutathione. Aging Cell. 2013, 12, 415–425. [Google Scholar] [CrossRef]
- Kumar, P.; Liu, C.; Hsu, J.W.; Chacko, S.; Minard, C.; Jahoor, F.; Sekhar, R.V. Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition: Results of a pilot clinical trial. Clin. Transl. Med. 2021, 11, e372. [Google Scholar] [CrossRef]
- Kumar, P.; Liu, C.; Suliburk, J.W.; Minard, C.G.; Muthupillai, R.; Chacko, S.; Hsu, J.W.; Jahoor, F.; Sekhar, R.V. Supplementing Glycine and N-acetylcysteine (GlyNAC) in Aging HIV Patients Improves Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Endothelial Dysfunction, Insulin Resistance, Genotoxicity, Strength, and Cognition: Results of an Open-Label Clinical Trial. Biomedicines 2020, 8, 390. [Google Scholar] [CrossRef]
- Sekhar, R.V. GlyNAC Supplementation Improves Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Aging Hallmarks, Metabolic Defects, Muscle Strength, Cognitive Decline, and Body Composition: Implications for Healthy Aging. J. Nutr. 2021, 29, nxab309. [Google Scholar] [CrossRef] [PubMed]
- Polonikov, A. Endogenous Deficiency of Glutathione as the Most Likely Cause of Serious Manifestations and Death in COVID-19 Patients. ACS Infect. Dis. 2020, 6, 1558–1562. [Google Scholar] [CrossRef]
- Scirè, A.; Cianfruglia, L.; Minnelli, C.; Bartolini, D.; Torquato, P.; Principato, G.; Galli, F.; Armeni, T. Glutathione compartmentalization and its role in glutathionylation and other regulatory processes of cellular pathways. Biofactors 2019, 45, 152–168. [Google Scholar] [CrossRef]
- Pérez, L.M.; Hooshmand, B.; Mangialasche, F.; Mecocci, P.; Smith, A.D.; Refsum, H.; Inzitari, M.; Fratiglioni, L.; Rizzuto, D.; Calderón-Larrañaga, A. Glutathione Serum Levels and Rate of Multimorbidity Development in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Liu, Y.; Yang, Y.; Zhang, P.; Zhong, W.; Wang, Y.; Wang, Q.; Xu, Y.; Li, M.; Li, X.; et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharm. Sin. B 2020, 10, 766–788. [Google Scholar] [CrossRef]
- Amatore, D.; Celestino, I.; Brundu, S.; Galluzzi, L.; Coluccio, P.; Checconi, P.; Magnani, M.; Palamara, A.T.; Fraternale, A.; Nencioni, L. Glutathione increase by the n-butanoyl glutathione derivative (GSH-C4) inhibits viral replication and induces a predominant Th1 immune profile in old mice infected with influenza virus. FASEB Bioadv. 2019, 1, 296–305. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, R.I.; Freeman, P.R.; Bruzzese, J. Efficacy of glutathione therapy in relieving dyspnea associated with COVID-19 pneumonia: A report of 2 cases. Respir. Med. Case Rep. 2020, 30, 101063. [Google Scholar] [CrossRef] [PubMed]
- Assimakopoulos, S.F.; Aretha, D.; Komninos, D.; Dimitropoulou, D.; Lagadinou, M.; Leonidou, L.; Oikonomou, I.; Mouzaki, A.; Marangos, M. N-acetyl-cysteine reduces the risk for mechanical ventilation and mortality in patients with COVID-19 pneumonia: A two-center retrospective cohort study. Infect. Dis. Lond. 2021, 53, 847–854. [Google Scholar] [CrossRef]
- McCaddon, A.; Regland, B. COVID-19: A methyl-group assault? Med. Hypotheses 2021, 149, 110543. [Google Scholar] [CrossRef]
- Pedersen, S.F.; Ho, Y.C. SARS-CoV-2: A storm is raging. J. Clin. Investig. 2020, 130, 2202–2205. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef]
- Pietrobon, A.J.; Teixeira, F.M.E.; Sato, M.N. Immunosenescence and Inflammaging: Risk Factors of Severe COVID-19 in Older People. Front. Immunol. 2020, 11, 579220. [Google Scholar] [CrossRef]
- Moreno Fernández-Ayala, D.J.; Navas, P.; López-Lluch, G. Age-related mitochondrial dysfunction as a key factor in COVID-19 disease. Exp. Gerontol. 2020, 142, 111147. [Google Scholar] [CrossRef] [PubMed]
- Gangadharan, C.; Ahluwalia, R.; Sigamani, A. Diabetes and COVID-19: Role of insulin resistance as a risk factor for COVID-19 severity. World J. Diabetes 2021, 12, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Bello-Perez, M.; Sola, I.; Novoa, B.; Klionsky, D.J.; Falco, A. Canonical and Noncanonical Autophagy as Potential Targets for COVID-19. Cells 2020, 9, 1619. [Google Scholar] [CrossRef] [PubMed]
- Tuzun, S.; Keles, A.; Okutan, D.; Yildiran, T.; Palamar, D. Assessment of musculoskeletal pain, fatigue and grip strength in hospitalized patients with COVID-19. Eur. J. Phys. Rehabil. Med. 2021, 57, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.M.; Zheng, Y.; Yu, Y.; Wang, Y.; Huang, Q.; Qian, F.; Sun, L.; Song, Z.G.; Chen, Z.; Feng, J.; et al. Blood molecular markers associated with COVID-19 immunopathology and multi-organ damage. EMBO J. 2020, 39, e105896. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Uninfected Controls | Hospitalized COVID-19 Patients |
|---|---|---|
| Hemoglobin (g/L) | 13.9 ± 0.8 n = 24 | 14.0 ± 4.3 p = 0.9 n = 59 |
| Total protein (g/dL) | 7.2 ± 0.4 n = 24 | 6.6 ± 0.5 p < 0.0001 n = 55 |
| Total bilirubin (mg/dL) | 0.7 ± 0.2 n = 24 | 0.6 ± 0.3 p = 0.08 n = 55 |
| Alanine transaminase (U/L) | 22.2 ± 7.3 n = 24 | 54.2 ± 45.5 p = 0.001 n = 55 |
| Aspartate transaminase (U/L) | 20.0 ± 8.2 n = 24 | 51.5 ± 56.3 p = 0.008 n = 55 |
| Alkaline phosphatase (U/L) | 70.2 ± 26.2 n = 24 | 78.4 ± 38.3 p = 0.3 n = 55 |
| BUN (mmol/L) | 13.4 ± 3.6 n = 24 | 17.2 ± 8.2 p = 0.03 n = 58 |
| Creatinine (mg/dL) | 0.9 ± 0.2 n = 24 | 0.7 ± 0.2 p = 0.0006 n = 58 |
| Outcome Measure | Controls N = 24 | Hospitalized COVID-19 Patients N = 60 |
|---|---|---|
| RBC-total GSH (mmol/L.RBC) | 1.2 ± 0.5 | 0.5 ± 0.2 p < 0.0001 |
| RBC-reduced GSH (mmol/L.RBC) | 1.0 ± 0.6 | 0.4 ± 0.2 p < 0.0001 |
| RBC-GSSG (mmol/L.RBC) | 0.2 ± 0.2 | 0.1 ± 0.0 p > 0.99 |
| RBC GSH/GSSG | 9.4 ± 10.1 | 8.0 ± 9.2 p = 0.5 |
| Plasma TBARS (μM/L) | 9.3 ± 9.9 | 28.2 ± 10.6 p < 0.0001 |
| Plasma F2-isoprostane (pg/mL) | 93.7 ± 71.0 | 201.6 ± 51.0 p < 0.0001 |
| Physical Function | Young Adults (21–40 years) | Young COVID-19 Patients (21–40 years) YA vs. YA-C YA-C vs. OA-C | Middle-Aged Adults (41–60 years) | Middle-Aged COVID-19 Patients (41–60 years) MA vs. MA-C MA-C vs. YA-C | Older Adults (≥60 years) | Older COVID-19 Patients (≥60 years) OA vs. OA-C OA-C vs. MA-C |
|---|---|---|---|---|---|---|
| RBC-total GSH (mmol/L.RBC) | 1.8 (1.7, 1.9) | 0.7 (0.7, 0.8) p < 0.0001 p < 0.0001 | 1.1 (1.0, 1.3) | 0.3 (0.3, 0.4) p < 0.0001 p < 0.0001 | 0.8 (0.6, 0.9) | 0.3 (0.2, 0.4) p < 0.0001 p > 0.99 |
| RBC-reduced GSH (mmol/L.RBC) | 1.7 (1.6, 1.8) | 0.7 (0.6, 0.7) p < 0.0001 p < 0.0001 | 1.0 (0.9, 1.1) | 0.3 (0.2, 0.3) p < 0.0001 p < 0.0001 | 0.4 (0.3, 0.5) | 0.2 (0.1, 0.3) p = 0.036 p > 0.99 |
| RBC-GSSG (mmol/L.RBC) | 0.2 (0.1, 0.2) | 0.1 (0.0, 0.1) p = 0.09 p > 0.99 | 0.1 (0.0, 0.2) | 0.1 (0.0, 0.1) p > 0.99 p > 0.99 | 0.4 (0.3, 0.5) | 0.1 (0.0, 0.1) p < 0.0001 p > 0.99 |
| RBC GSH/GSSG ratio | 10.0 (4.9, 15.0) | 14.7 (11.5, 17.8) p = 0.8 p < 0.0001 | 16.7 (11.0, 22.3) | 3.7 (0.6, 6.8) p = 0.001 p < 0.0001 | 1.9 (0, 7.0) | 2.5 (0, 5.7) p > 0.99 p > 0.99 |
| Plasma TBARS (μM/L) | 2.4 (0, 5.9) | 18.1 (15.9, 20.3) p < 0.0001 p < 0.0001 | 2.7 (0, 6.6) | 29.9 (27.8, 32.1) p < 0.0001 p < 0.0001 | 23.2 (19.7, 26.7) | 39.6 (37.3, 41.8) p < 0.0001 p < 0.0001 |
| Plasma F2-isoprostane (pg/mL) | 45.4 (23.5, 67.4) | 162.3 (148.5, 176.0) p < 0.0001 p < 0.0001 | 49.7 (25.2, 74.3) | 195.9 (182.4, 209.4) p < 0.0001 p = 0.006 | 190.1 (168.2, 212.1) | 259.8 (245.6, 274.1) p < 0.0001 p < 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, P.; Osahon, O.; Vides, D.B.; Hanania, N.; Minard, C.G.; Sekhar, R.V. Severe Glutathione Deficiency, Oxidative Stress and Oxidant Damage in Adults Hospitalized with COVID-19: Implications for GlyNAC (Glycine and N-Acetylcysteine) Supplementation. Antioxidants 2022, 11, 50. https://doi.org/10.3390/antiox11010050
Kumar P, Osahon O, Vides DB, Hanania N, Minard CG, Sekhar RV. Severe Glutathione Deficiency, Oxidative Stress and Oxidant Damage in Adults Hospitalized with COVID-19: Implications for GlyNAC (Glycine and N-Acetylcysteine) Supplementation. Antioxidants. 2022; 11(1):50. https://doi.org/10.3390/antiox11010050
Chicago/Turabian StyleKumar, Premranjan, Ob Osahon, David B. Vides, Nicola Hanania, Charles G. Minard, and Rajagopal V. Sekhar. 2022. "Severe Glutathione Deficiency, Oxidative Stress and Oxidant Damage in Adults Hospitalized with COVID-19: Implications for GlyNAC (Glycine and N-Acetylcysteine) Supplementation" Antioxidants 11, no. 1: 50. https://doi.org/10.3390/antiox11010050
APA StyleKumar, P., Osahon, O., Vides, D. B., Hanania, N., Minard, C. G., & Sekhar, R. V. (2022). Severe Glutathione Deficiency, Oxidative Stress and Oxidant Damage in Adults Hospitalized with COVID-19: Implications for GlyNAC (Glycine and N-Acetylcysteine) Supplementation. Antioxidants, 11(1), 50. https://doi.org/10.3390/antiox11010050