
Serum Lutein and Zeaxanthin Are Inversely Associated with High-Sensitivity C-Reactive Protein in Non-Smokers: The Mikkabi Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Mikkabi Study and Participants
2.2. Measurements
2.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
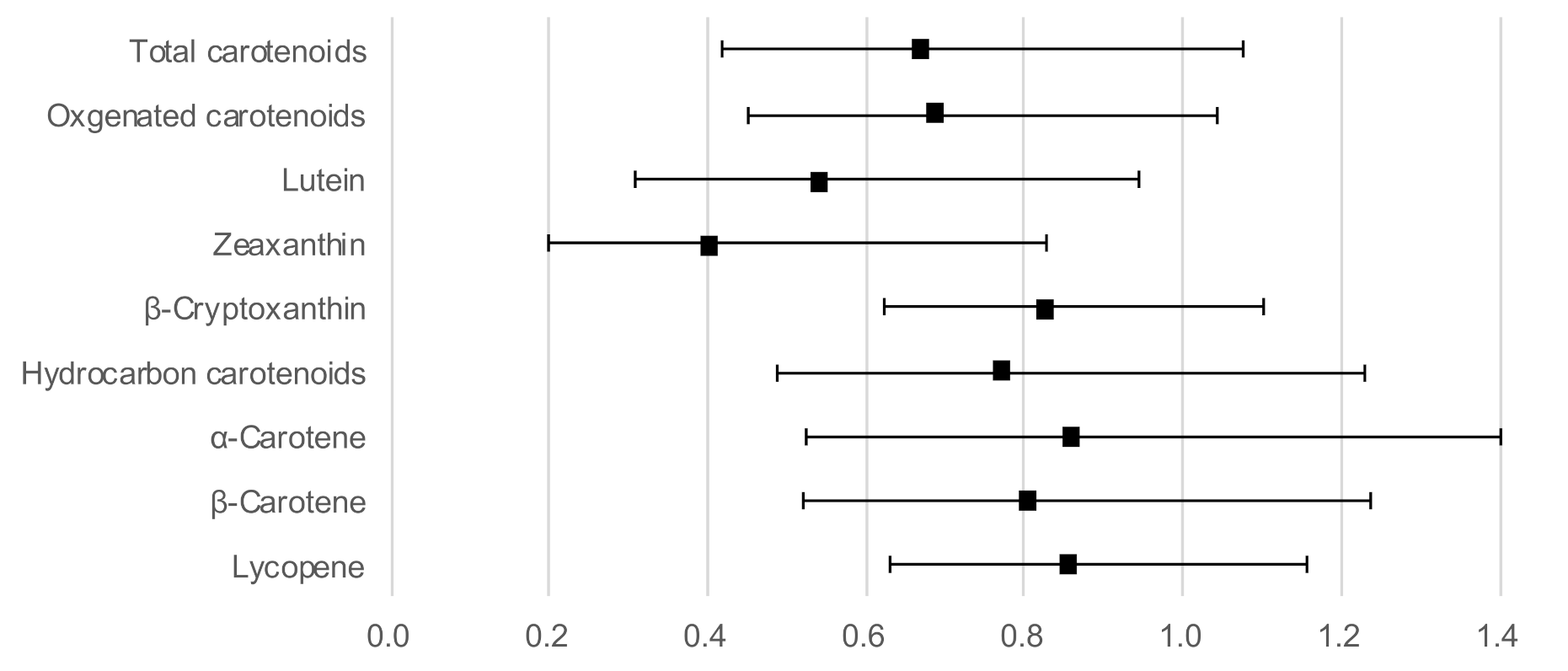
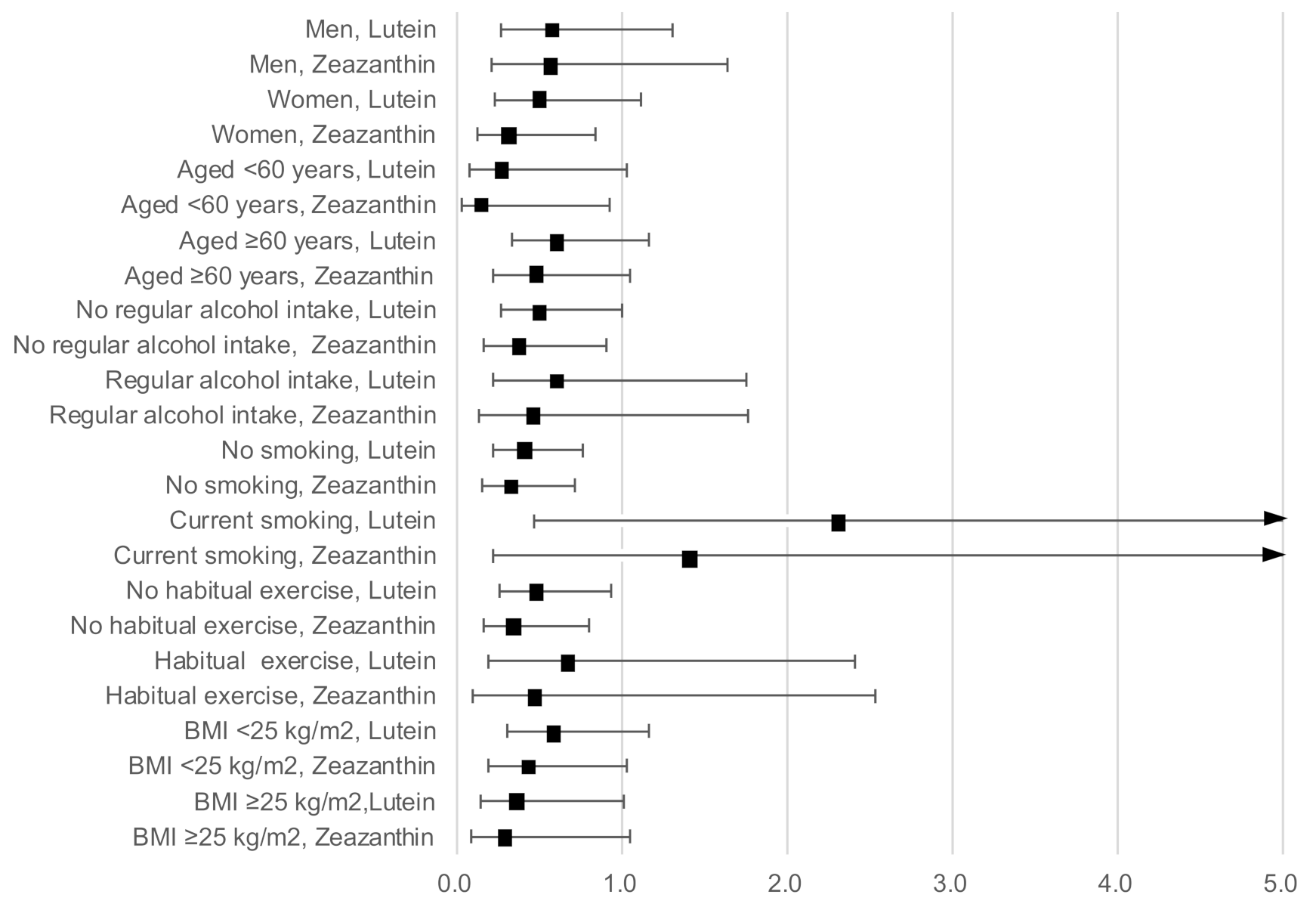
3.2. Association between Serum Carotenoid and High-Sensitivity C-Reactive Protein Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stromsnes, K.; Correas, A.G.; Lehmann, J.; Gambini, J.; Olaso-Gonzalez, G. Anti-Inflammatory Properties of Diet: Role in Healthy Aging. Biomedicines 2021, 9, 922. [Google Scholar] [CrossRef] [PubMed]
- Hayaishi-Okano, R.; Yamasaki, Y.; Katakami, N.; Ohtoshi, K.; Gorogawa, S.; Kuroda, A.; Matsuhisa, M.; Kosugi, K.; Nishikawa, N.; Kajimoto, Y.; et al. Elevated C-reactive protein associates with early-stage carotid atherosclerosisis in young subjects with type 1 diabetes. Diabetes Care 2002, 25, 1432–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Ito, Y.; Ochiai, J.; Kusuhara, Y.; Hashimoto, S.; Tokudome, S.; Kojima, M.; Wakai, K.; Toyoshima, H.; Tamakoshi, K.; et al. Relationship between obesity and serum markers of oxidative stress and inflammation in Japanese. Asian Pac. J. Cancer Prev. 2003, 4, 259–266. [Google Scholar]
- Li, Y.; Zhong, X.; Cheng, G.; Zhao, C.; Zhang, L.; Hong, Y.; Wan, Q.; He, R.; Wang, Z. Hs-CRP and all-cause, cardiovascular, and cancer mortality risk: A meta-analysis. Atherosclerosis 2017, 259, 75–82. [Google Scholar] [CrossRef]
- Ni, P.; Yu, M.; Zhang, R.; Cheng, C.; He, M.; Wang, H.; Chen, S.; Duan, G. Dose-response association between C-reactive protein and risk of all-cause and cause-specific mortality: A systematic review and meta-analysis of cohort studies. Ann. Epidemiol. 2020, 51, 20–27.e11. [Google Scholar] [CrossRef]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef]
- Mailliez, A.; Guilbaud, A.; Puisieux, F.; Dauchet, L.; Boulanger, É. Circulating biomarkers characterizing physical frailty: CRP, hemoglobin, albumin, 25OHD and free testosterone as best biomarkers. Results of a meta-analysis. Exp. Gerontol. 2020, 139, 111014. [Google Scholar] [CrossRef]
- Hozawa, A.; Jacobs, D.R.; Steffes, M.W.; Gross, M.D.; Steffen, L.M.; Lee, D.H. Relationships of circulating carotenoid concentrations with several markers of inflammation, oxidative stress, and endothelial dysfunction: The Coronary Artery Risk Development in Young Adults (CARDIA)/Young Adult Longitudinal Trends in Antioxidants (YALTA) Study. Clin. Chem. 2007, 53, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Demmig-Adams, B.; Lopez-Pozo, M.; Stewart, J.J.; Adams, W.W., 3rd. Zeaxanthin and Lutein: Photoprotectors, Anti-Inflammatories, and Brain Food. Molecules 2020, 25, 3607. [Google Scholar] [CrossRef]
- Ahn, Y.J.; Kim, H. Lutein as a Modulator of Oxidative Stress-Mediated Inflammatory Diseases. Antioxidants 2021, 10, 1448. [Google Scholar] [CrossRef]
- Hajizadeh-Sharafabad, F.; Zahabi, E.S.; Malekahmadi, M.; Zarrin, R.; Alizadeh, M. Carotenoids supplementation and inflammation: A systematic review and meta-analysis of randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2021, 1–17. [Google Scholar] [CrossRef]
- Nakamura, M.; Sugiura, M.; Aoki, N. High beta-carotene and beta-cryptoxanthin are associated with low pulse wave velocity. Atherosclerosis 2006, 184, 363–369. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ikoma, Y.; Yano, M.; Ogawa, K.; Matsumoto, H.; Kato, M.; Ohshima, M.; Nagano, A. The homeostasis model assessment-insulin resistance index is inversely associated with serum carotenoids in non-diabetic subjects. J. Epidemiol. 2006, 16, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, M.; Nakamura, M.; Ikoma, Y.; Yano, M.; Ogawa, K.; Matsumoto, H.; Kato, M.; Ohshima, M.; Nagao, A. Serum carotenoid concentrations are inversely associated with serum aminotransferases in hyperglycemic subjects. Diabetes Res. Clin. Pract. 2006, 71, 82–91. [Google Scholar] [CrossRef]
- Wakai, K.; Egami, I.; Kato, K.; Lin, Y.; Kawamura, T.; Tamakoshi, A.; Aoki, R.; Kojima, M.; Nakayama, T.; Wada, M.; et al. A simple food frequency questionnaire for Japanese diet–Part I. Development of the questionnaire, and reproducibility and validity for food groups. J. Epidemiol. 1999, 9, 216–226. [Google Scholar] [CrossRef]
- Egami, I.; Wakai, K.; Kato, K.; Lin, Y.; Kawamura, T.; Tamakoshi, A.; Aoki, R.; Kojima, M.; Nakayama, T.; Wada, M.; et al. A simple food frequency questionnaire for Japanese diet--Part II. Reproducibility and validity for nutrient intakes. J. Epidemiol. 1999, 9, 227–234. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Matsumoto, H.; Ando, F.; Shimokata, H.; Yano, M. Synergistic interaction of cigarette smoking and alcohol drinking with serum carotenoid concentrations: Findings from a middle-aged Japanese population. Br. J. Nutr. 2009, 102, 1211–1219. [Google Scholar] [CrossRef] [Green Version]
- Kones, R. The Jupiter study, CRP screening, and aggressive statin therapy-implications for the primary prevention of cardiovascular disease. Ther. Adv. Cardiovasc. Dis. 2009, 3, 309–315. [Google Scholar] [CrossRef] [Green Version]
- Van Herpen-Broekmans, W.M.R.; Klopping-Ketelaars, I.A.A.; Bots, M.L.; Kluft, C.; Princen, H.; Hendriks, H.F.J.; Tijburg, L.B.M.; van Poppel, G.; Kardinaal, A.F.M. Serum carotenoids and vitamins in relation to markers of endothelial function and inflammation. Eur. J. Epidemiol. 2004, 19, 915–921. [Google Scholar] [CrossRef]
- Kijlstra, A.; Tian, Y.; Kelly, E.R.; Berendschot, T. Lutein: More than just a filter for blue light. Prog. Retin. Eye Res. 2012, 31, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Watzl, B.; Kulling, S.E.; Moseneder, J.; Barth, S.W.; Bub, A. A 4-wk intervention with high intake of carotenoid-rich vegetables and fruit reduces plasma C-reactive protein in healthy, nonsmoking men. Am. J. Clin. Nutr. 2005, 82, 1052–1058. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.X.; Jiao, J.H.; Li, Z.Y.; Liu, R.R.; Shi, Q.; Ma, L. Lutein supplementation reduces plasma lipid peroxidation and C-reactive protein in healthy nonsmokers. Atherosclerosis 2013, 227, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Graydon, R.; Hogg, R.E.; Chakravarthy, U.; Young, I.S.; Woodside, J.V. The effect of lutein- and zeaxanthin-rich foods v. supplements on macular pigment level and serological markers of endothelial activation, inflammation and oxidation: Pilot studies in healthy volunteers. Br. J. Nutr. 2012, 108, 334–342. [Google Scholar] [CrossRef] [Green Version]
- Estevez-Santiago, R.; Silvan, J.M.; Can-Cauich, C.A.; Veses, A.M.; Alvarez-Acero, I.; Martinez-Bartolome, M.A.; San-Roman, R.; Camara, M.; Olmedilla-Alonso, B.; de Pascual-Teresa, S. Lack of a Synergistic Effect on Cardiometabolic and Redox Markers in a Dietary Supplementation with Anthocyanins and Xanthophylls in Postmenopausal Women. Nutrients 2019, 11, 1533. [Google Scholar] [CrossRef] [Green Version]
- Riso, P.; Vendrame, S.; Del Bo, C.; Martini, D.; Martinetti, A.; Seregni, E.; Visioli, F.; Parolini, M.; Porrini, M. Effect of 10-day broccoli consumption on inflammatory status of young healthy smokers. Int. J. Food Sci. Nutr. 2014, 65, 106–111. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | hs-CRP < 2.0 mg/L | hs-CRP ≥ 2.0 mg/L | p-Value 1 | ||
|---|---|---|---|---|---|
| n = 779 | n = 103 | ||||
| Age, years, mean (SD) | 55.4 | (9.8) | 56.3 | (10.8) | 0.36 |
| Men, n (%) | 255 | (85.3) | 44 | (14.7) | 0.04 |
| Women, n (%) | 524 | (89.9) | 59 | (10.1) | |
| Current smoking: no, n (%) | 690 | (88.5) | 90 | (11.5) | 0.72 |
| Current smoking: yes, n (%) | 89 | (87.3) | 13 | (12.7) | |
| Regular alcohol intake: no, n (%) | 586 | (88.9) | 73 | (11.1) | 0.34 |
| Regular alcohol intake: yes, n (%) | 193 | (86.5) | 30 | (13.5) | |
| Habitual exercise: no, n (%) | 591 | (88.1) | 80 | (11.9) | 0.75 |
| Habitual exercise: yes, n (%) | 184 | (88.9) | 23 | (11.1) | |
| Body mass index, kg/m2, mean (SD) | 22.7 | (2.8) | 24.8 | (4.2) | <0.01 |
| Systolic blood pressure, mmHg, mean (SD) | 130 | (20) | 134 | (18) | 0.10 |
| Diastolic blood pressure, mmHg, mean (SD) | 77 | (12) | 79 | (11) | 0.09 |
| Total cholesterol, mg/dL, mean (SD) | 212 | (34) | 213 | (36) | 0.63 |
| LDL cholesterol, mg/dL, mean (SD) | 126 | (31) | 130 | (31) | 0.21 |
| HDL cholesterol, mg/dL, mean (SD) | 65 | (17) | 60 | (16) | <0.01 |
| Triglycerides, mg/dL, mean 2 | 90 | 102 | 0.04 | ||
| Hemoglobin A1c, %, mean 2 | 5.1 | 5.4 | <0.01 | ||
| White blood cell count, mean 2 | 5287 | 6064 | <0.01 | ||
| Total energy intake, kcal, mean (SD) | 2079 | (589) | 2109 | (543) | 0.62 |
| Total serum carotenoids, µmol/L, mean 2 | 3.48 | 3.11 | 0.03 | ||
| Oxygenated carotenoids, µmol/L, mean 2 | 2.36 | 2.12 | 0.08 | ||
| Lutein, µmol/L, mean 2 | 0.57 | 0.52 | 0.01 | ||
| Zeaxanthin, µmol/L, mean 2 | 0.24 | 0.22 | 0.01 | ||
| β-Cryptoxanthin, µmol/L, mean 2 | 1.37 | 1.23 | 0.23 | ||
| Hydrocarbon carotenoids, µmol/L, mean 2 | 1.03 | 0.89 | 0.01 | ||
| α-Carotene, µmol/L, mean 2 | 0.13 | 0.12 | 0.07 | ||
| β-Carotene, µmol/L, mean 2 | 0.59 | 0.51 | 0.02 | ||
| Lycopene, µmol/L, mean 2 | 0.26 | 0.22 | 0.04 | ||
| Serum Carotenoids | Tertiles of Serum Carotenoid Concentration 1 | |||||
|---|---|---|---|---|---|---|
| T1 (Low) | T2 | T3 (High) | ||||
| OR | OR | 95% CI | OR | 95% CI | ||
| Total serum carotenoids | Model 1 2 | 1.00 | 0.56 | (0.33–0.93) | 0.53 | (0.30–0.91) |
| Model 2 3 | 1.00 | 0.52 | (0.30–0.90) | 0.57 | (0.32–0.9997) | |
| Oxygenated carotenoids | Model 1 2 | 1.00 | 0.58 | (0.35–0.98) | 0.50 | (0.29–0.86) |
| Model 2 3 | 1.00 | 0.58 | (0.34–0.99) | 0.50 | (0.28–0.90) | |
| Lutein | Model 1 2 | 1.00 | 0.78 | (0.49–1.26) | 0.40 | (0.23–0.70) |
| Model 2 3 | 1.00 | 0.81 | (0.50–1.33) | 0.44 | (0.25–0.76) | |
| Zeaxanthin | Model 1 2 | 1.00 | 0.59 | (0.36–0.97) | 0.37 | (0.21–0.64) |
| Model 2 3 | 1.00 | 0.56 | (0.34–0.94) | 0.36 | (0.21–0.64) | |
| β-Cryptoxanthin | Model 1 2 | 1.00 | 1.07 | (0.64–1.81) | 0.79 | (0.45–1.39) |
| Model 2 3 | 1.00 | 0.97 | (0.56–1.68) | 0.74 | (0.41–1.34) | |
| Hydrocarbon carotenoids | Model 12 | 1.00 | 0.80 | (0.49–1.31) | 0.53 | (0.30–0.95) |
| Model 2 3 | 1.00 | 0.87 | (0.52–1.44) | 0.68 | (0.37–1.25) | |
| α-Carotene | Model 1 2 | 1.00 | 0.75 | (0.46–1.22) | 0.56 | (0.31–1.001) |
| Model 2 3 | 1.00 | 0.78 | (0.47–1.30) | 0.64 | (0.35–1.18) | |
| β-Carotene | Model 1 2 | 1.00 | 0.72 | (0.43–1.20) | 0.56 | (0.31–1.005) |
| Model 2 3 | 1.00 | 0.79 | (0.46–1.34) | 0.74 | (0.40–1.37) | |
| Lycopene | Model 1 2 | 1.00 | 0.64 | (0.39–1.06) | 0.59 | (0.34–0.997) |
| Model 2 3 | 1.00 | 0.61 | (0.36–1.02) | 0.63 | (0.36–1.08) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, M.; Sugiura, M. Serum Lutein and Zeaxanthin Are Inversely Associated with High-Sensitivity C-Reactive Protein in Non-Smokers: The Mikkabi Study. Antioxidants 2022, 11, 259. https://doi.org/10.3390/antiox11020259
Nakamura M, Sugiura M. Serum Lutein and Zeaxanthin Are Inversely Associated with High-Sensitivity C-Reactive Protein in Non-Smokers: The Mikkabi Study. Antioxidants. 2022; 11(2):259. https://doi.org/10.3390/antiox11020259
Chicago/Turabian StyleNakamura, Mieko, and Minoru Sugiura. 2022. "Serum Lutein and Zeaxanthin Are Inversely Associated with High-Sensitivity C-Reactive Protein in Non-Smokers: The Mikkabi Study" Antioxidants 11, no. 2: 259. https://doi.org/10.3390/antiox11020259
APA StyleNakamura, M., & Sugiura, M. (2022). Serum Lutein and Zeaxanthin Are Inversely Associated with High-Sensitivity C-Reactive Protein in Non-Smokers: The Mikkabi Study. Antioxidants, 11(2), 259. https://doi.org/10.3390/antiox11020259