
Associations between Oxidative/Nitrosative Stress and Thyroid Hormones in Pregnant Women—Tainan Birth Cohort Study (TBCS)

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Analytical Method for Oxidative and Nitrosative Stress Biomarkers
2.3. Analytical Method for Measuring Serum Thyroid Hormones and Urinary Creatinine
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Participants
3.2. Distributions of Oxidative and Nitrosative Stress Biomarkers and Thyroid Hormones
3.3. Correlations between Oxidative and Nitrosative Stress Biomarkers and Thyroid Hormones
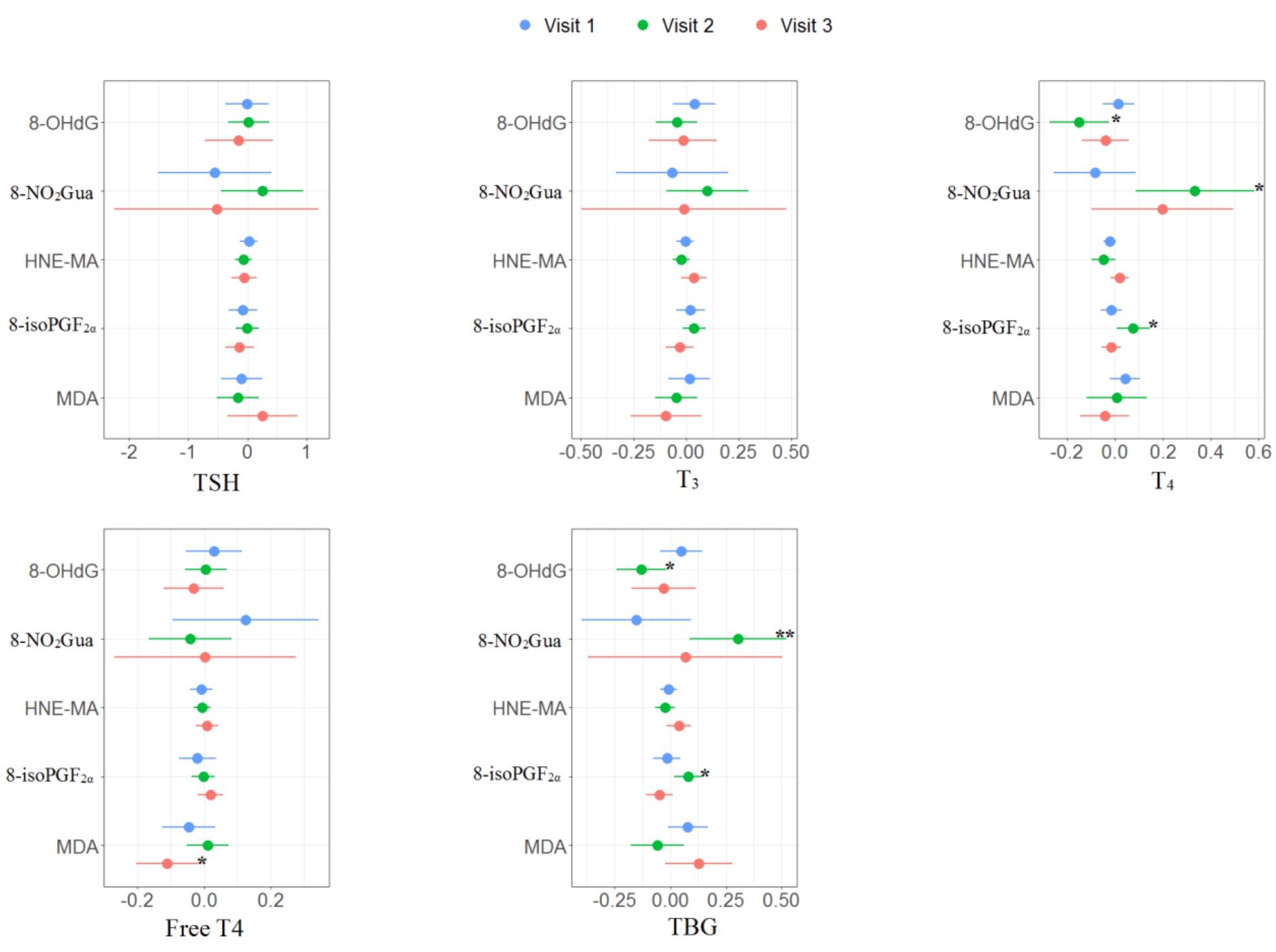
3.4. Associations between Oxidative and Nitrosative Stress Biomarkers and Thyroid Hormones in Multiple Linear Regression and Linear Mixed Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mancini, A.; Di Segni, C.; Raimondo, S.; Olivieri, G.; Silvestrini, A.; Meucci, E.; Currò, D. Thyroid hormones, oxidative stress, and inflammation. Mediat. Inflamm. 2016, 2016, 6757154. [Google Scholar] [CrossRef] [Green Version]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef]
- Silvestri, E.; Schiavo, L.; Lombardi, A.; Goglia, F. Thyroid hormones as molecular determinants of thermogenesis. Acta Physiol. Scand. 2005, 184, 265–283. [Google Scholar] [CrossRef]
- Schriks, M.; Roessig, J.M.; Murk, A.J.; Furlow, J.D. Thyroid hormone receptor isoform selectivity of thyroid hormone disrupting compounds quantified with an in vitro reporter gene assay. Environ. Toxicol. Pharmacol. 2007, 23, 302–307. [Google Scholar] [CrossRef]
- Wu, Y.; Koenig, R.J. Gene regulation by thyroid hormone. Trends Endocrinol. Metab. 2000, 11, 207–211. [Google Scholar] [CrossRef]
- Cheserek, M.J.; Wu, G.R.; Ntazinda, A.; Shi, Y.H.; Shen, L.Y.; Le, G.W. Association between thyroid hormones, lipids and oxidative stress markers in subclinical hypothyroidism. J. Med. Biochem. 2015, 34, 323–331. [Google Scholar] [CrossRef]
- Scholl, T.O.; Stein, T.P. Oxidant damage to DNA and pregnancy outcome. J. Matern. Fetal Neonatal Med. 2001, 10, 182–185. [Google Scholar] [CrossRef]
- Wang, Y.; Walsh, S.W. Increased superoxide generation is associated with decreased superoxide dismutase activity and mRNA expression in placental trophoblast cells in pre-eclampsia. Placenta 2001, 22, 206–212. [Google Scholar] [CrossRef]
- Matsubasa, T.; Uchino, T.; Karashima, S.; Tanimura, M.; Endo, F. Oxidative stress in very low birth weight infants as measured by urinary 8-OHdG. Free Radic. Res. 2002, 36, 189–193. [Google Scholar] [CrossRef]
- Kim, Y.J.; Hong, Y.C.; Lee, K.H.; Park, H.J.; Park, E.A.; Moon, H.S.; Ha, E.H. Oxidative stress in pregnant women and birth weight reduction. Reprod. Toxicol. 2005, 19, 487–492. [Google Scholar] [CrossRef]
- Hartoft-Nielsen, M.L.; Boas, M.; Bliddal, S.; Rasmussen, Å.K.; Main, K.; Feldt-Rasmussen, U. Do thyroid disrupting chemicals influence foetal development during pregnancy? J. Thyroid. Res. 2011, 2011, 342189. [Google Scholar] [CrossRef] [Green Version]
- Aggarawal, N.; Suri, V.; Singla, R.; Chopra, S.; Sikka, P.; Shah, V.N.; Bhansali, A. Pregnancy outcome in hyperthyroidism: A case control study. Gynecol. Obstet. Investig. 2014, 77, 94–99. [Google Scholar] [CrossRef]
- Chen, L.M.; Du, W.J.; Dai, J.; Zhang, Q.; Si, G.X.; Yang, H.; Ye, E.L.; Chen, Q.S.; Yu, L.C.; Zhang, C.; et al. Effects of subclinical hypothyroidism on maternal and perinatal outcomes during pregnancy: A single-center cohort study of a Chinese population. PLoS ONE 2014, 9, e109364. [Google Scholar] [CrossRef] [Green Version]
- Henrichs, J.; Bongers-Schokking, J.J.; Schenk, J.J.; Ghassabian, A.; Schmidt, H.G.; Visser, T.J.; Hooijkaas, H.; de Muinck Keizer-Schrama, S.M.P.F.; Hofman, A.; Jaddoe, V.V.W.; et al. Maternal thyroid function during early pregnancy and cognitive functioning in early childhood: The generation R study. J. Clin. Endocrinol. Metab. 2010, 95, 4227–4234. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Shan, Z.; Teng, W.; Yu, X.; Li, Y.; Fan, C.; Teng, X.; Guo, R.; Wang, H.; Li, J.; et al. Abnormalities of maternal thyroid function during pregnancy affect neuropsychological development of their children at 25–30 months. Clin. Endocrinol. 2010, 72, 825–829. [Google Scholar] [CrossRef]
- Wu, C.; Chen, S.T.; Peng, K.H.; Cheng, T.J.; Wu, K.Y. Concurrent quantification of multiple biomarkers indicative of oxidative stress status using liquid chromatography—Tandem mass spectrometry. Anal. Biochem. 2016, 512, 26–35. [Google Scholar] [CrossRef]
- Peter Stein, T.; Scholl, T.O.; Schluter, M.D.; Leskiw, M.J.; Chen, X.; Spur, B.W.; Rodriguez, A. Oxidative stress early in pregnancy and pregnancy outcome. Free Radic. Res. 2008, 42, 841–848. [Google Scholar] [CrossRef]
- Wang, P.W.; Chen, M.L.; Huang, L.W.; Yang, W.; Wu, K.Y.; Huang, Y.F. Prenatal nonylphenol exposure, oxidative and nitrative stress, and birth outcomes: A cohort study in Taiwan. Environ. Pollut. 2015, 207, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.M.; Ferguson, K.K.; Milne, G.L.; Rios-McConnell, R.; Vélez-Vega, C.; Rosario, Z.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Repeated measures of urinary oxidative stress biomarkers and preterm birth in Puerto Rico. Free. Radic. Biol. Med. 2020, 146, 299–305. [Google Scholar] [CrossRef]
- Waits, A.; Chen, H.C.; Kuo, P.L.; Wang, C.W.; Huang, H.B.; Chang, W.H.; Shih, S.F.; Huang, P.C. Urinary phthalate metabolites are associated with biomarkers of DNA damage and lipid peroxidation in pregnant women—Tainan Birth Cohort Study (TBCS). Environ. Res. 2020, 188, 109863. [Google Scholar] [CrossRef]
- Huang, P.C.; Tsai, C.H.; Liang, W.Y.; Li, S.S.; Huang, H.B.; Kuo, P.L. Early phthalates exposure in pregnant women is associated with alteration of thyroid hormones. PLoS ONE 2016, 11, e0159398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.B.; Kuo, P.L.; Chang, J.W.; Jaakkola, J.J.K.; Liao, K.W.; Huang, P.C. Longitudinal assessment of prenatal phthalate exposure on serum and cord thyroid hormones homeostasis during pregnancy—Tainan birth cohort study (TBCS). Sci. Total Environ. 2018, 619–620, 1058–1065. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.C.; Waits, A.; Chen, H.C.; Chang, W.T.; Jaakkola, J.J.; Huang, H.B. Mediating role of oxidative/nitrosative stress biomarkers in the associations between phthalate exposure and thyroid function in Taiwanese adults. Environ. Int. 2020, 140, 105751. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.B.; Pan, W.H.; Chang, J.W.; Chiang, H.C.; Guo, Y.L.; Jaakkola, J.J.; Huang, P.C. Does exposure to phthalates influence thyroid function and growth hormone homeostasis? The Taiwan Environmental Survey for Toxicants (TEST) 2013. Environ. Res. 2017, 153, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the US population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Carney, L.A.; Quinlan, J.D.; West, J.M. Thyroid disease in pregnancy. Am. Fam. Physician 2014, 89, 273–278. [Google Scholar]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.F.; Wang, P.W.; Huang, L.W.; Lai, C.H.; Yang, W.; Wu, K.Y.; Lu, C.A.; Chen, H.C.; Chen, M.L. Prenatal nonylphenol and bisphenol A exposures and inflammation are determinants of oxidative/nitrative stress: A Taiwanese cohort study. Environ. Sci. Technol. 2017, 51, 6422–6429. [Google Scholar] [CrossRef]
- van’t Erve, T.J.; Rosen, E.M.; Barrett, E.S.; Nguyen, R.H.; Sathyanarayana, S.; Milne, G.L.; Calafat, A.M.; Swan, S.H.; Ferguson, K.K. Phthalates and phthalate alternatives have diverse associations with oxidative stress and inflammation in pregnant women. Environ. Sci. Technol. 2019, 53, 3258–3267. [Google Scholar] [CrossRef]
- Zhang, M.; Deng, Y.L.; Liu, C.; Chen, P.P.; Luo, Q.; Miao, Y.; Cui, F.P.; Wang, L.Q.; Jiang, M.; Zeng, Q. Urinary phthalate metabolite concentrations, oxidative stress and thyroid function biomarkers among patients with thyroid nodules. Environ. Pollut. 2021, 272, 116416. [Google Scholar] [CrossRef]
- Venditti, P.; Di Meo, S. Thyroid hormone-induced oxidative stress. Cell. Mol. Life Sci. CMLS 2006, 63, 414–434. [Google Scholar] [CrossRef] [PubMed]
- Resch, U.; Helsel, G.; Tatzber, F.; Sinzinger, H. Antioxidant Status in Thyroid Dysfunction. Clin. Chem. Lab. Med. 2002, 40, 1132–1134. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.; Raimondo, S.; Di Segni, C.; Persano, M.; Gadotti, G.; Silvestrini, A.; Festa, R.; Tiano, L.; Pontecorvi, A.; Meucci, E. Thyroid hormones and antioxidant systems: Focus on oxidative stress in cardiovascular and pulmonary diseases. Int. J. Mol. Sci. 2013, 14, 23893–23909. [Google Scholar] [CrossRef]
- Asayama, K.; Kato, K. Oxidative muscular injury and its relevance to hyperthyroidism. Free Radic. Biol. Med. 1990, 8, 293–303. [Google Scholar] [CrossRef]
- Dardano, A.; Ghiadoni, L.; Plantinga, Y.; Caraccio, N.; Bemi, A.; Duranti, E.; Taddei, S.; Ferrannini, E.; Salvetti, A.; Monzani, F. Recombinant human thyrotropin reduces endothelium-dependent vasodilation in patients monitored for differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 4175–4178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haribabu, A.; Reddy, V.S.; Pallavi, C.H.; Bitla, A.R.; Sachan, A.; Pullaiah, P.; Suresh, V.; Rao, P.V.L.N.S.; Suchitra, M.M. Evaluation of protein oxidation and its association with lipid peroxidation and thyrotropin levels in overt and subclinical hypothyroidism. Endocrine 2013, 44, 152–157. [Google Scholar] [CrossRef]
- Manti, S.; Marseglia, L.; D’Angelo, G.; Cuppari, C.; Cusumano, E.; Arrigo, T.; Gitto, E.; Salpietro, C. “Cumulative Stress”: The effects of maternal and neonatal oxidative stress and oxidative stress-inducible genes on programming of atopy. Oxid. Med. Cell. Longev. 2016, 2016, 8651820. [Google Scholar] [CrossRef] [Green Version]
- Derouiche, S.; DoudiDalal, A.N. Study of oxidative stress during pregnancy. Glob. J. Pharm. Pharm. Sci. 2018, 4, 555646. [Google Scholar]
- Domínguez-Perles, R.; Gil-Izquierdo, A.; Ferreres, F.; Medina, S. Update on oxidative stress and inflammation in pregnant women, unborn children (nasciturus), and newborns—Nutritional and dietary effects. Free Radic. Biol. Med. 2019, 142, 38–51. [Google Scholar] [CrossRef]
- Yao, Y.; Li, M.; Pan, L.; Duan, Y.; Duan, X.; Li, Y.; Sun, H. Exposure to organophosphate ester flame retardants and plasticizers during pregnancy: Thyroid endocrine disruption and mediation role of oxidative stress. Environ. Int. 2021, 146, 106215. [Google Scholar] [CrossRef]
- Obregón, M.J.; Calvo, R.M.; Del Rey, F.E.; De Escobar, G.M. Ontogenesis of thyroid function and interactions with maternal function. Thyroid Gland Dev. Funct. 2007, 10, 86–98. [Google Scholar]
- Medici, M.; de Rijke, Y.B.; Peeters, R.P.; Visser, W.; de Muinck Keizer-Schrama, S.M.; Jaddoe, V.V.; Hofman, A.; Hooijkaas, H.; Steegers, E.A.; Tiemeier, H.; et al. Maternal early pregnancy and newborn thyroid hormone parameters: The Generation R study. J. Clin. Endocrinol. Metab. 2012, 97, 646–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrzyńska, M.M.; Baumgartner, A.; Anderson, D. Antioxidants modulate thyroid hormone-and noradrenaline-induced DNA damage in human sperm. Mutagenesis 2004, 19, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Il’yasova, D.; Scarbrough, P.; Spasojevic, I. Urinary biomarkers of oxidative status. Clin. Chim. Acta 2012, 413, 1446–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age (years) | 35.09 ± 3.51 |
| Gestational week at enrollment (weeks) | 18.25 ± 1.34 |
| n (%) | |
| Education | |
| High school (or earlier) (≤12 years) | 4 (4.1) |
| University (12–16 years) | 76 (78.4) |
| Postgraduate (≥16 years) | 17 (17.5) |
| Annual household income (USD) a | |
| <15,625 | 17 (17.9) |
| 15,625–31,250 | 50 (52.6) |
| ≥31,250 | 28 (29.5) |
| Primiparas | 42 (43.3) |
| Folic acid consumption b | 36 (55.4) |
| Active cigarette smoking before pregnancy c | 2 (2.1) |
| Passive cigarette smoking before pregnancy d | 16 (16.5) |
| Alcohol consumption before pregnancy e | 1 (1.0) |
| Parameters | Visit 1 (n = 97) | Visit 2 (n = 63) | Visit 3 (n = 58) | P trend b | ICC | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DR a | GM | Median (95% CI) | DR | GM | Median (95% CI) | DR | GM | Median (95% CI) | % | ||
| Oxidative/nitrosative stress | |||||||||||
| 8-OHdG (ng/mL) | 100 | 2.6 | 2.1 (1.8–2.6) | 100 | 2.9 | 2.3 (2.2–3.3) | 100 | 2.6 | 2.6 (2.1–2.9) | 0.818 | 18.8 |
| 8-NO2Gua (ng/mL) | 100 | 1.6 | 1.5 (1.4–1.6) | 100 | 1.5 | 1.4 (1.3–1.5) | 100 | 1.5 c | 1.4 (1.4–1.5) | 0.043 * | 2.0 |
| HNE-MA (ng/mL) | 100 | 52.9 | 59.6 (40.1–81.2) | 100 | 54.3 | 57.7 (29.3–90.5) | 100 | 26.9 c | 30.5 (17.7–42.3) | 0.010 * | 7.5 |
| 8-IsoPGF2α (ng/mL) | 64 | 0.6 | 0.6 (0.5–0.8) | 61 | 0.7 | 0.8 (0.5–1.0) | 77 | 0.9 c | 1.0 (0.8–1.3) | 0.022 * | –2.8 |
| MDA (μmole/L) | 100 | 8.2 | 7.8 (6.6–9.0) | 100 | 10.5 c | 10.6 (8.2–12.5) | 100 | 8.8 | 9.3 (7.4–11.8) | 0.296 | 11.0 |
| Thyroid hormones | |||||||||||
| TSH (μIU/mL) d | 100 | 1.0 | 1.2 (1.0–1.4) | 100 | 1.1 | 1.1 (1.0–1.3) | 100 | 2.4 c | 2.9 (2.3–3.2) | <0.001 *** | 30.2 |
| T3 (ng/dL) d | 100 | 122.3 | 126 (118–130) | 100 | 116.2 c | 115.0 (108.0–122.0) | 100 | 105.6 c | 110.0 (97.0–117.0) | <0.001 *** | 45.9 |
| T4 (μg/dL) d | 100 | 8.9 | 8.8 (8.5–9.2) | 100 | 8.7 | 8.9 (8.6–9.4) | 100 | 8.7 | 8.6 (8.3–9.2) | 0.313 | 44.5 |
| Free T4 (ng/dL) d | 100 | 0.8 | 0.8 (0.7–0.9) | 100 | 0.6 c | 0.6 (0.6–0.7) | 100 | 0.6 c | 0.6 (0.6–0.6) | <0.001 *** | 8.4 |
| TBG (μg/mL) d | 100 | 34.7 | 36.2 (33.7–37.8) | 100 | 37.8 c | 39.4 (38.4–43.4) | 100 | 38.3 c | 40.3 (38.7–42.6) | <0.001 *** | 63.1 |
| Creatinine (mg/dL) | 99 | 49.8 | 49.9 (40.0–61.0) | 100 | 63.5 | 66.0 (44.5–85.7) | 100 | 73.9 c | 81.4 (64.7–101.8) | 0.008 ** | 29.8 |
| Parameters | Visit 1 (n = 97) | Visit 2 (n = 63) | Visit 3 (n = 58) | P trend b | ICC | |||
|---|---|---|---|---|---|---|---|---|
| GM | Median (95% CI) | GM | Median (95% CI) | GM | Median (95% CI) | (%) | ||
| T3/TSH | 123.7 | 96.1 (85.8–127.5) | 108.7 c | 104.3 (80.7–122.5) | 44.7 c | 39.5 (36.0–44.0) | <0.001 *** | 4.4 |
| T3/T4 | 13.7 | 13.6 (12.9–14.3) | 13.4 | 12.9 (11.8–14.6) | 12.1 c | 12.1 (11.2–12.7) | 0.001 ** | 5.5 |
| TSH/T4 | 0.1 | 0.1 (0.1–0.1) | 0.1 c | 0.1 (0.1–0.1) | 0.3 c | 0.3 (0.3–0.4) | <0.001 *** | 35.7 |
| TSH/Free T4 | 1.2 | 1.4 (1.3–1.6) | 1.7 c | 1.8 (1.6–2.0) | 3.7 c | 4.3 (3.2–4.9) | <0.001 *** | 25.4 |
| T4/Free T4 | 11.0 | 10.7 (10.2–11.8) | 13.8 c | 14.3 (13.5–14.9) | 13.7 c | 13.6 (13.2–14.5) | <0.001 *** | 18.4 |
| T3/TBG | 3.5 | 3.6 (3.2–3.8) | 3.1 c | 3.0 (2.8–3.3) | 2.8 c | 2.8 (2.5–2.9) | <0.001 *** | 27.9 |
| T4/TBG | 0.3 | 0.3 (0.2–0.3) | 0.2 c | 0.2 (0.2–0.2) | 0.2 c | 0.2 (0.2–0.2) | <0.001 *** | 47.0 |
| Free T4/TBG | 0.02 | 0.02 (0.02–0.02) | 0.02 c | 0.02 (0.01–0.02) | 0.02 c | 0.02 (0.01–0.02) | <0.001 *** | 40.3 |
| Thyroid Hormones | 8-OHdG | 8-NO2Gua | HNE-MA | 8-isoPGF2α | MDA |
|---|---|---|---|---|---|
| Δ%(95%CI) | Δ%(95%CI) | Δ%(95%CI) | Δ%(95%CI) | Δ%(95%CI) | |
| TSH | −12.1 (−27.5, 3.4) | −14 (−26.9, −1.1) * | −23.0 (−35.9, −10.0) *** | 7.6 (−6.4, 21.6) | −4.1 (−19.1, 10.8) |
| T3 | 1.0 (−3.1, 5.1) | −0.1 (−3.6, 3.3) | 2.3 (−1.3, 5.8) | 0.1 (−3.6, 3.9) | −3.7 (−7.7, 0.3) |
| T4 | −2.2 (−5.7, 1.3) | 3.0 (0.2, 5.8) * | −0.1 (−4.0, 2.0) | −0.4 (−3.4, 2.7) | 2.0 (−1.5, 5.5) |
| Free T4 | −0.04 (−4.1, 4.0) | 4.3 (0.8, 7.8) * | 1.9 (−1.8, 5.6) | −0.8 (−4.6, 3.0) | −2.6 (−6.8, 1.6) |
| TBG | −3.2 (−6.9, 0.5) | −1.9 (−4.8, 1.0) | −0.9 (−3.9, 2.2) | −2.9 (−6.0, 0.2) | 3.4 (−0.1, 6.9) |
| T3/TSH | 12.8 (−3.7, 29.3) | 13.9 (0.1, 27.8) | 25.2 (11.2, 39.2) *** | −6.9 (−22.0, 8.1) | 0.6 (−15.8, 17.0) |
| T3/T4 | 4.4 (−0.7, 9.5) | −3.5 (−7.9, 0.9) | 2.5 (−2.1, 7.0) | 1.3 (−3.5, 6.1) | −5.9 (−11.0, −0.8) * |
| TSH/T4 | −8.2 (−24.1, 7.6) | −17.3 (−30.4, −4.3) ** | −21.2 (−34.5, −7.8) ** | 8.4 (−5.8, 22.5) | −6.7 (−21.9, 8.5) |
| TSH/Free T4 | −13.5 (−30.2, 3.2) | −18.6 (−32.6, −4.6) | −24.0 (−38.3, −9.6) ** | 6.8 (−8.7, 22.2) | 0.6 (−15.8, 17.1) |
| T4/Free T4 | −3.8 (−8.8, 1.2) | −1.8 (−6.2, 2.5) | −3.0 (−7.5, 1.5) | −0.1 (−4.9, 4.7) | 4.9 (−0.2, 10.0) |
| T3/TBG | 3.1 (−1.8, 8.0) | 1.9 (−2.2, 6.0) | 1.7 (−2.6, 6.0) | 2.7 (−1.8, 7.1) | −7.5 (−12.3, −2.6) ** |
| T4/TBG | 1.5 (−2.3, 5.4) | 3.6 (0.5, 6.7) * | 0.3 (−3.0, 3.6) | 1.3 (−2.0, 4.8) | −2.3 (−6.0, 1.5) |
| Free T4/TBG | 3.5 (−3.0, 10.1) | 5.6 (0.2, 11.1) * | 1.8 (−3.9, 7.5) | 1.7 (−4.3, 7.7) | −8.8 (−15.1, −2.4) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, P.-K.; Chen, H.-C.; Kuo, P.-L.; Chang, J.-W.; Chang, W.-T.; Huang, P.-C. Associations between Oxidative/Nitrosative Stress and Thyroid Hormones in Pregnant Women—Tainan Birth Cohort Study (TBCS). Antioxidants 2022, 11, 334. https://doi.org/10.3390/antiox11020334
Cheng P-K, Chen H-C, Kuo P-L, Chang J-W, Chang W-T, Huang P-C. Associations between Oxidative/Nitrosative Stress and Thyroid Hormones in Pregnant Women—Tainan Birth Cohort Study (TBCS). Antioxidants. 2022; 11(2):334. https://doi.org/10.3390/antiox11020334
Chicago/Turabian StyleCheng, Po-Keng, Hsin-Chang Chen, Pao-Lin Kuo, Jung-Wei Chang, Wan-Ting Chang, and Po-Chin Huang. 2022. "Associations between Oxidative/Nitrosative Stress and Thyroid Hormones in Pregnant Women—Tainan Birth Cohort Study (TBCS)" Antioxidants 11, no. 2: 334. https://doi.org/10.3390/antiox11020334
APA StyleCheng, P.-K., Chen, H.-C., Kuo, P.-L., Chang, J.-W., Chang, W.-T., & Huang, P.-C. (2022). Associations between Oxidative/Nitrosative Stress and Thyroid Hormones in Pregnant Women—Tainan Birth Cohort Study (TBCS). Antioxidants, 11(2), 334. https://doi.org/10.3390/antiox11020334