
Association between Changes in Total Antioxidant Levels and Clinical Symptom Improvement in Patients with Antipsychotic-Naïve First-Episode Schizophrenia after 3 Months of Risperidone Monotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment of Psychiatric Symptoms and Clinical Outcomes
2.3. Determination of TAS in the Patients and Controls
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data of ANFE Patients at Baseline
3.2. Comparisons of TAS before and after Risperidone Treatment
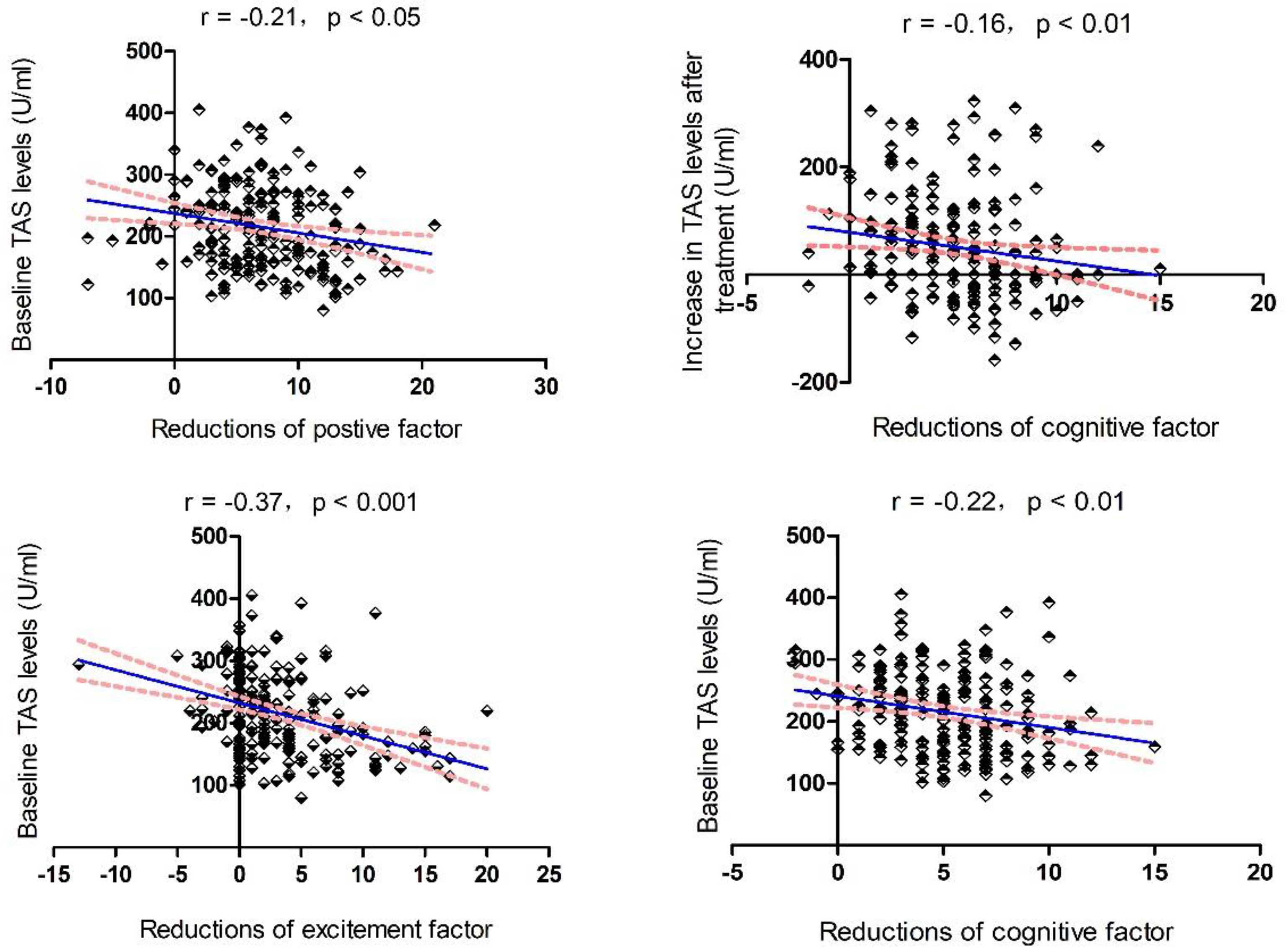
3.3. Relationship between Baseline TAS, Changes in TAS, and Improvement in Clinical Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barnett, R. Schizophrenia. Lancet 2018, 391, 648. [Google Scholar] [CrossRef]
- Orlovska-Waast, S.; Kohler-Forsberg, O.; Brix, S.W.; Nordentoft, M.; Kondziella, D.; Krogh, J.; Benros, M.E. Cerebrospinal fluid markers of inflammation and infections in schizophrenia and affective disorders: A systematic review and meta-analysis. Mol. Psychiatry 2019, 24, 869–887. [Google Scholar] [CrossRef] [Green Version]
- Möller, H.J.; Czobor, P. Pharmacological treatment of negative symptoms in schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 567–578. [Google Scholar] [CrossRef]
- Xie, T.; Li, Q.; Luo, X.; Tian, L.; Wang, Z.; Tan, S.; Chen, S.; Yang, G.; An, H.; Yang, F.; et al. Plasma total antioxidant status and cognitive impairments in first-episode drug-naïve patients with schizophrenia. Cogn. Neurodyn. 2019, 13, 357–365. [Google Scholar] [CrossRef]
- Virit, O.; Altindag, A.; Yumru, M.; Dalkilic, A.; Savas, H.A.; Selek, S.; Erel, O.; Herken, H. A defect in the antioxidant defense system in schizophrenia. Neuropsychobiology 2009, 60, 87–93. [Google Scholar] [CrossRef]
- Wu, J.Q.; Kosten, T.R.; Zhang, X.Y. Free radicals, antioxidant defense systems, and schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 46, 200–206. [Google Scholar] [CrossRef]
- Şenyurt, M.; Aybek, H.; Herken, H.; Kaptanoglu, B.; Korkmaz, A. Evaluation of Oxidative Status in Patients Treated with Electroconvulsive Therapy. Clin. Psychopharmacol. Neurosci. 2017, 15, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Al-Chalabi, B.M.; Thanoon, I.A.; Ahmed, F.A. Potential effect of olanzapine on total antioxidant status and lipid peroxidation in schizophrenic patients. Neuropsychobiology 2009, 59, 8–11. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Zhou, D.F.; Shen, Y.C.; Zhang, P.Y.; Zhang, W.F.; Liang, J.; Chen, D.C.; Xiu, M.H.; Kosten, T.A.; Kosten, T.R. Effects of risperidone and haloperidol on superoxide dismutase and nitric oxide in schizophrenia. Neuropharmacology 2012, 62, 1928–1934. [Google Scholar] [CrossRef]
- Aringhieri, S.; Carli, M.; Kolachalam, S.; Verdesca, V.; Cini, E.; Rossi, M.; McCormick, P.J.; Corsini, G.U.; Maggio, R.; Scarselli, M. Molecular targets of atypical antipsychotics: From mechanism of action to clinical differences. Pharmacol. Ther. 2018, 192, 20–41. [Google Scholar] [CrossRef]
- Li, X.R.; Xiu, M.H.; Guan, X.N.; Wang, Y.C.; Wang, J.; Leung, E.; Zhang, X.Y. Altered Antioxidant Defenses in Drug-Naive First Episode Patients with Schizophrenia Are Associated with Poor Treatment Response to Risperidone: 12-Week Results from a Prospective Longitudinal Study. Neurotherapeutics 2021, 18, 1316–1324. [Google Scholar] [CrossRef]
- Wallwork, R.S.; Fortgang, R.; Hashimoto, R.; Weinberger, D.R.; Dickinson, D. Searching for a consensus five-factor model of the Positive and Negative Syndrome Scale for schizophrenia. Schizophr. Res. 2012, 137, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Koga, M.; Serritella, A.V.; Sawa, A.; Sedlak, T.W. Implications for reactive oxygen species in schizophrenia pathogenesis. Schizophr. Res. 2016, 176, 52–71. [Google Scholar] [CrossRef]
- Bulbul, F.; Virit, O.; Alpak, G.; Unal, A.; Bulut, M.; Kaya, M.C.; Altindag, A.; Celik, H.; Savas, H.A. Are oxidative stress markers useful to distinguish schizoaffective disorder from schizophrenia and bipolar disorder? Acta Neuropsychiatr. 2014, 26, 120–124. [Google Scholar] [CrossRef]
- Wang, D.F.; Cao, B.; Xu, M.Y.; Liu, Y.Q.; Yan, L.L.; Liu, R.; Wang, J.Y.; Lu, Q.B. Meta-Analyses of Manganese Superoxide Dismutase Activity, Gene Ala-9Val Polymorphism, and the Risk of Schizophrenia. Medicine 2015, 94, e1507. [Google Scholar] [CrossRef]
- Dadheech, G.; Mishra, S.; Gautam, S.; Sharma, P. Oxidative stress, alpha-tocopherol, ascorbic acid and reduced glutathione status in schizophrenics. Indian J. Clin. Biochem. 2006, 21, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Micó, J.A.; Rojas-Corrales, M.O.; Gibert-Rahola, J.; Parellada, M.; Moreno, D.; Fraguas, D.; Graell, M.; Gil, J.; Irazusta, J.; Castro-Fornieles, J.; et al. Reduced antioxidant defense in early onset first-episode psychosis: A case-control study. BMC Psychiatry 2011, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Lohr, J.B.; Kuczenski, R.; Niculescu, A.B. Oxidative mechanisms and tardive dyskinesia. CNS Drugs 2003, 17, 47–62. [Google Scholar] [CrossRef]
- Cadet, J.L.; Perumal, A.S. Chronic treatment with prolixin causes oxidative stress in rat brain. Biol. Psychiatry 1990, 28, 738–740. [Google Scholar] [CrossRef]
- Nilsson, G. Brain and body oxygen requirements of Gnathonemus petersii, a fish with an exceptionally large brain. J. Exp. Biol. 1996, 199, 603–607. [Google Scholar] [CrossRef]
- Cobley, J.N.; Fiorello, M.L.; Bailey, D.M. 13 reasons why the brain is susceptible to oxidative stress. Redox Biol. 2018, 15, 490–503. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Controls (n = 115) | Patients with TAS (n = 246) | F (p Value) |
|---|---|---|---|
| Sex (male/female) | 64/54 | 138/108 | 0.5 (0.49) |
| Age (years) | 27.7 ± 8.0 | 27.5 ± 9.2 | 0.03 (0.87) |
| Education (years) | 10.4 ± 3.1 | 9.0 ± 3.9 | 12.0 (0.001) |
| BMI (kg/m2) | 23.9 ± 4.5 | 21.3 ± 3.4 | 34.3 (<0.001) |
| Smokers/nonsmokers | 42/73 | 67/170 | 2.5 (0.12) |
| Age of onset (years) | 26.0 ± 9.1 | ||
| Baseline PANSS score | |||
| Positive symptoms | 21.8 ± 6.3 | ||
| Negative symptoms | 18.8 ± 6.8 | ||
| General psychopathology | 35.5 ± 9.6 | ||
| Total score | 75.9 ± 17.2 | ||
| Source | Type III Sum of Squares | df | Mean Square | F | p |
|---|---|---|---|---|---|
| Corrected model | 51,573.8 | 3 | 17,191.3 | 4.3 | 0.006 |
| Intercept | 1,020,459.1 | 1 | 1,020,459.1 | 252.4 | <0.001 |
| Age | 21,984.4 | 1 | 21,984.4 | 5.4 | 0.02 |
| Sex | 2236.4 | 1 | 2236.4 | 0.6 | 0.46 |
| Group | 21,466.8 | 1 | 21,466.8 | 5.3 | 0.02 |
| Error | 1,350,255.0 | 334 | 4042.7 | ||
| Total | 17,474,638.9 | 338 | |||
| Corrected total | 1,401,828.8 | 337 |
| Baseline | Follow-Up | t (p Value) | |
|---|---|---|---|
| PANSS 5-factor score, mean ± SD | |||
| Positive factor | 14.7 ± 4.5 | 7.7 ± 3.4 | 22.0 (<0.001) |
| Negative factor | 14.8 ± 6.1 | 12.5 ± 5.3 | 6.0 (<0.001) |
| Cognitive factor | 10. ± 3.0 | 4.9 ± 2.2 | 25.0 (<0.001) |
| Excitement factor | 8.2 ± 4.6 | 4.9 ± 2.1 | 10.1 (<0.001) |
| Depressive factor | 5.5 ± 2.6 | 4.3 ± 1.8 | 6.8 (<0.001) |
| PANSS score, mean ± SD | |||
| P subscore | 22.1 ± 6.6 | 11.8 ± 4.5 | 23.3 (<0.001) |
| N subscore | 18.8 ± 7.0 | 14.2 ± 5.6 | 10.6 (<0.001) |
| G subscore | 35.8 ± 10.1 | 24.9 ± 6.0 | 16.6 (<0.001) |
| Total score | 76.5 ± 18.1 | 50.8 ± 12.9 | 20.0 (<0.001) |
| Biomarker levels, mean ± SD | |||
| TAS (U/mL) | 216.1 ± 66.3 | 266.3 ± 104.8 | −7.7 (<0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.; Xiu, M.; Su, X.; Wu, F.; Zhang, X. Association between Changes in Total Antioxidant Levels and Clinical Symptom Improvement in Patients with Antipsychotic-Naïve First-Episode Schizophrenia after 3 Months of Risperidone Monotherapy. Antioxidants 2022, 11, 646. https://doi.org/10.3390/antiox11040646
Wang K, Xiu M, Su X, Wu F, Zhang X. Association between Changes in Total Antioxidant Levels and Clinical Symptom Improvement in Patients with Antipsychotic-Naïve First-Episode Schizophrenia after 3 Months of Risperidone Monotherapy. Antioxidants. 2022; 11(4):646. https://doi.org/10.3390/antiox11040646
Chicago/Turabian StyleWang, Keqiang, Meihong Xiu, Xiuru Su, Fengchun Wu, and Xiangyang Zhang. 2022. "Association between Changes in Total Antioxidant Levels and Clinical Symptom Improvement in Patients with Antipsychotic-Naïve First-Episode Schizophrenia after 3 Months of Risperidone Monotherapy" Antioxidants 11, no. 4: 646. https://doi.org/10.3390/antiox11040646
APA StyleWang, K., Xiu, M., Su, X., Wu, F., & Zhang, X. (2022). Association between Changes in Total Antioxidant Levels and Clinical Symptom Improvement in Patients with Antipsychotic-Naïve First-Episode Schizophrenia after 3 Months of Risperidone Monotherapy. Antioxidants, 11(4), 646. https://doi.org/10.3390/antiox11040646