

Effect of Particulate Matter 2.5 on Fetal Growth in Male and Preterm Infants through Oxidative Stress
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
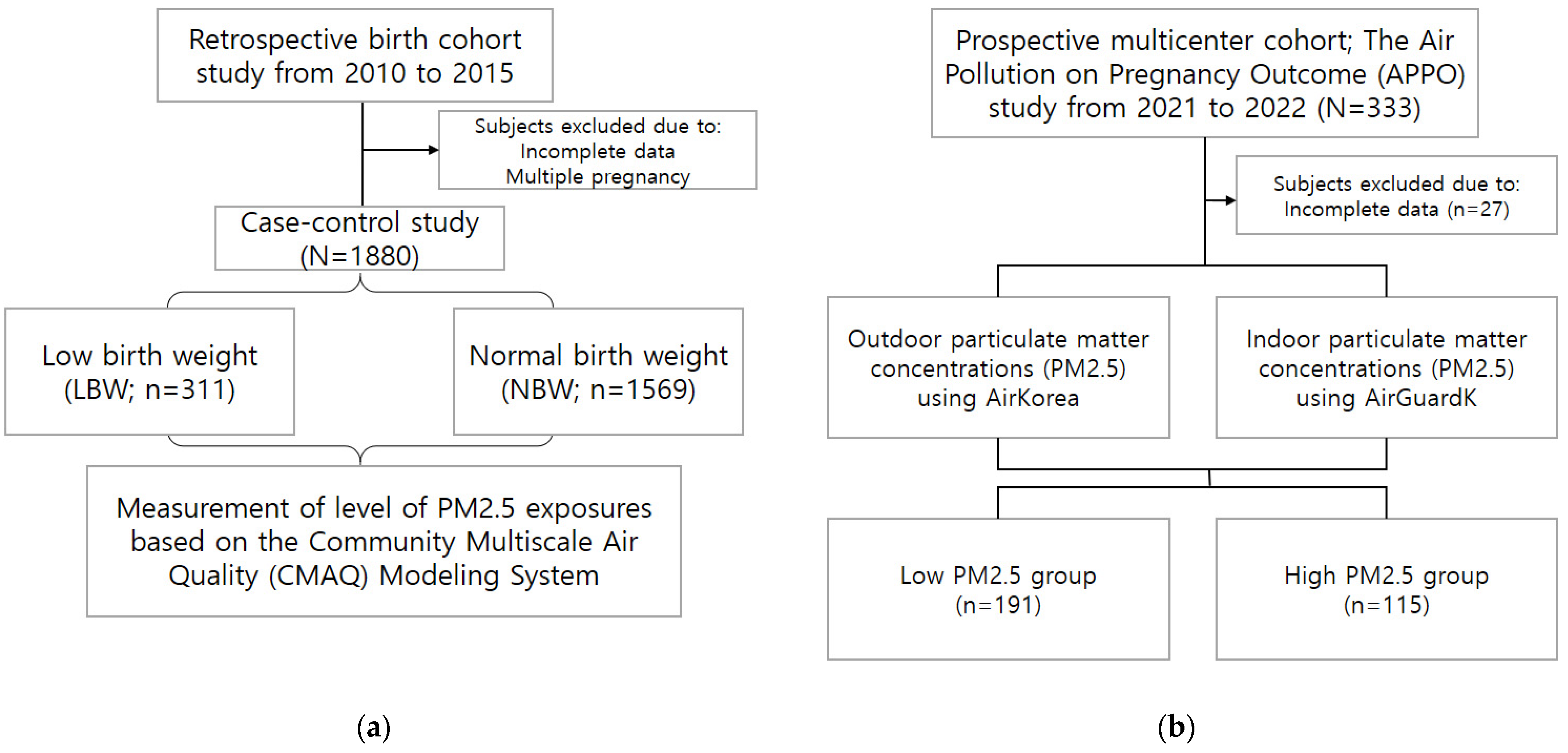
2.1. Study Design of Cohort I
2.2. Study Design of Cohort II
2.3. PM Exposure Assessment
2.4. Collection of Blood and Urine Samples
2.5. Measurement of Oxidative Stress and Inflammatory Markers
2.6. Statistical Analysis
3. Results
3.1. Association between PM2.5 Exposure and Birth Weight and Height According to Neonatal Sex Using a Retrospective Cohort Study
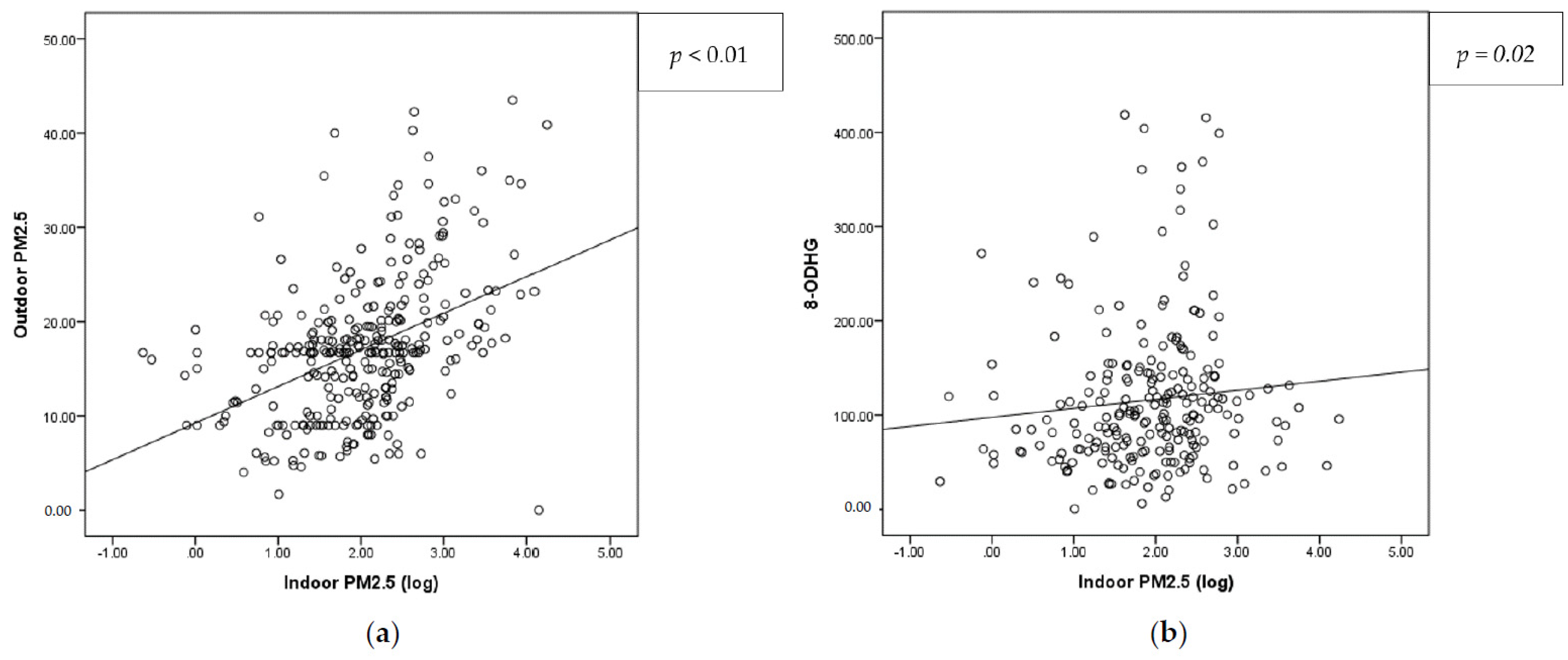
3.2. Study Population of APPO and Measurement and Correlation of Indoor/Outdoor PM2.5
3.3. Association between PM2.5 Exposure and Pregnancy Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, S.; Moon, J.; Kang, N.; Kim, Y.H.; You, Y.A.; Kwon, E.; Ansari, A.; Hur, Y.M.; Park, T.; Kim, Y.J. Predicting preterm birth through vaginal microbiota, cervical length, and WBC using a machine learning model. Front. Microbiol. 2022, 13, 912853. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Chen, R.; Gu, X.; Xu, J.; Yang, L.; Zhao, J.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; et al. Association of fine particulate matter air pollution and its constituents with lung function: The China Pulmonary Health study. Environ. Int. 2021, 156, 106707. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, C.; Yu, G.; Meng, X.; Wang, W.; Kan, H.; Zhang, J.; Cai, J. Associations of Ambient Fine Particulate Matter and Its Chemical Constituents with Birth Weight for Gestational Age in China: A Nationwide Survey. Environ. Sci. Technol. 2022, 56, 8406–8415. [Google Scholar] [CrossRef]
- Gray, S.C.; Edwards, S.E.; Miranda, M.L. Assessing exposure metrics for PM and birth weight models. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 469–477. [Google Scholar] [CrossRef]
- Percy, Z.; DeFranco, E.; Xu, F.; Hall, E.S.; Haynes, E.N.; Jones, D.; Muglia, L.J.; Chen, A. Trimester specific PM2.5 exposure and fetal growth in Ohio, 2007–2010. Environ. Res. 2019, 171, 111–118. [Google Scholar] [CrossRef]
- Kloog, I.; Melly, S.J.; Ridgway, W.L.; Coull, B.A.; Schwartz, J. Using new satellite based exposure methods to study the association between pregnancy PM2.5 exposure, premature birth and birth weight in Massachusetts. Environ. Health 2012, 11, 40. [Google Scholar] [CrossRef]
- Han, Z.; Lutsiv, O.; Mulla, S.; Rosen, A.; Beyene, J.; McDonald, S.D. Low gestational weight gain and the risk of preterm birth and low birthweight: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2011, 90, 935–954. [Google Scholar] [CrossRef]
- Salihu, H.M.; Garcia, B.Y.; Dongarwar, D.; Maiyegun, S.O.; Yusuf, K.K.; Agili, D.E.A. Maternal pre-pregnancy underweight and the risk of small-for-gestational-age in Asian-American ethnic groups. Obstet. Gynecol. Sci. 2021, 64, 496–505. [Google Scholar] [CrossRef]
- Valero De Bernabé, J.; Soriano, T.; Albaladejo, R.; Juarranz, M.; Calle, M.E.; Martínez, D.; Domínguez-Rojas, V. Risk factors for low birth weight: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 3–15. [Google Scholar] [CrossRef]
- Bachwenkizi, J.; Liu, C.; Meng, X.; Zhang, L.; Wang, W.; van Donkelaar, A.; Martin, R.V.; Hammer, M.S.; Chen, R.; Kan, H. Maternal exposure to fine particulate matter and preterm birth and low birth weight in Africa. Environ. Int. 2022, 160, 107053. [Google Scholar] [CrossRef]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef]
- Guo, P.; Chen, Y.; Wu, H.; Zeng, J.; Zeng, Z.; Li, W.; Zhang, Q.; Huo, X.; Feng, W.; Lin, J.; et al. Ambient air pollution and markers of fetal growth: A retrospective population-based cohort study of 2.57 million term singleton births in China. Environ. Int. 2020, 135, 105410. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Ou, C.; Magana-Arachchi, D.; Vithanage, M.; Vanka, K.S.; Palanisami, T.; Masakorala, K.; Wijesekara, H.; Yan, Y.; Bolan, N.; et al. Indoor Particulate Matter in Urban Households: Sources, Pathways, Characteristics, Health Effects, and Exposure Mitigation. Int. J. Environ. Res. Public Health 2021, 18, 1055. [Google Scholar] [CrossRef]
- Shezi, B.; Jafta, N.; Naidoo, R.N. Exposure assessment of indoor particulate matter during pregnancy: A narrative review of the literature. Rev. Environ. Health 2020, 35, 427–442. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Lee, S.H.; Lee, S.Y.; Kim, H.C.; Kim, H.B.; Park, M.J.; Yoon, J.; Jung, S.; Yang, S.I.; Lee, E.; et al. Mid-pregnancy PM2.5 exposure affects sex-specific growth trajectories via ARRDC3 methylation. Environ. Res. 2021, 200, 111640. [Google Scholar] [CrossRef] [PubMed]
- Patelarou, E.; Kelly, F.J. Indoor exposure and adverse birth outcomes related to fetal growth, miscarriage and prematurity-a systematic review. Int. J. Environ. Res. Public Health 2014, 11, 5904–5933. [Google Scholar] [CrossRef]
- Kim, J.Y.; Lee, E.Y.; Choi, I.; Kim, J.; Cho, K.H. Effects of the Particulate Matter2.5 (PM2.5) on Lipoprotein Metabolism, Uptake and Degradation, and Embryo Toxicity. Mol. Cells 2015, 38, 1096–1104. [Google Scholar] [CrossRef]
- Nääv, Å.; Erlandsson, L.; Isaxon, C.; Åsander Frostner, E.; Ehinger, J.; Sporre, M.K.; Krais, A.M.; Strandberg, B.; Lundh, T.; Elmér, E.; et al. Urban PM2.5 Induces Cellular Toxicity, Hormone Dysregulation, Oxidative Damage, Inflammation, and Mitochondrial Interference in the HRT8 Trophoblast Cell Line. Front. Endocrinol. 2020, 11, 75. [Google Scholar] [CrossRef]
- Rosa, M.J.; Hsu, H.L.; Just, A.C.; Brennan, K.J.; Bloomquist, T.; Kloog, I.; Pantic, I.; Mercado García, A.; Wilson, A.; Coull, B.A.; et al. Association between prenatal particulate air pollution exposure and telomere length in cord blood: Effect modification by fetal sex. Environ. Res. 2019, 172, 495–501. [Google Scholar] [CrossRef]
- Liu, X.C.; Strodl, E.; Wu, C.A.; Huang, L.H.; Yin, X.N.; Wen, G.M.; Sun, D.L.; Xian, D.X.; Chen, W.Q. Critical window for the association between prenatal environmental tobacco smoke exposure and preterm birth. Environ. Res. 2022, 212, 113427. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.J.; Rector, A.M.; Guxens, M.; Iniguez, C.; Swartz, M.D.; Symanski, E.; Ibarluzea, J.; Ambros, A.; Estarlich, M.; Lertxundi, A.; et al. Susceptible windows of exposure to fine particulate matter and fetal growth trajectories in the Spanish INMA (INfancia y Medio Ambiente) birth cohort. Environ. Res. 2022, 216, 114628. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Lv, S.; Liu, Y.; Li, Y. Biomarkers for the adverse effects on respiratory system health associated with atmospheric particulate matter exposure. J. Hazard. Mater. 2022, 421, 126760. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.G.; Cowell, W.; Kannan, S.; Ganguri, H.B.; Nentin, F.; Wilson, A.; Coull, B.A.; Wright, R.O.; Baccarelli, A.; Bollati, V.; et al. Prenatal particulate air pollution and newborn telomere length: Effect modification by maternal antioxidant intakes and infant sex. Environ. Res. 2020, 187, 109707. [Google Scholar] [CrossRef]
- Kim, Y.J.; Hong, Y.C.; Lee, K.H.; Park, H.J.; Park, E.A.; Moon, H.S.; Ha, E.H. Oxidative stress in pregnant women and birth weight reduction. Reprod. Toxicol. 2005, 19, 487–492. [Google Scholar] [CrossRef]
- Shastri, L.; Pammal, R.S.; Mani, I.; Thomas, T.; Kurpad, A.V. Oxidative stress during early pregnancy and birth outcomes. Public. Health Nutr. 2016, 19, 3210–3215. [Google Scholar] [CrossRef]
- Quraishi, S.M.; Hazlehurst, M.F.; Loftus, C.T.; Nguyen, R.H.N.; Barrett, E.S.; Kaufman, J.D.; Bush, N.R.; Karr, C.J.; LeWinn, K.Z.; Sathyanarayana, S.; et al. Association of prenatal exposure to ambient air pollution with adverse birth outcomes and effect modification by socioeconomic factors. Environ. Res. 2022, 212, 113571. [Google Scholar] [CrossRef]
- Liang, Z.; Yang, Y.; Qian, Z.; Ruan, Z.; Chang, J.; Vaughn, M.G.; Zhao, Q.; Lin, H. Ambient PM2.5 and birth outcomes: Estimating the association and attributable risk using a birth cohort study in nine Chinese cities. Environ. Int. 2019, 126, 329–335. [Google Scholar] [CrossRef]
- Klepac, P.; Locatelli, I.; Korošec, S.; Künzli, N.; Kukec, A. Ambient air pollution and pregnancy outcomes: A comprehensive review and identification of environmental public health challenges. Environ. Res. 2018, 167, 144–159. [Google Scholar] [CrossRef]
- Yang, S.; Tan, Y.; Mei, H.; Wang, F.; Li, N.; Zhao, J.; Zhang, Y.; Qian, Z.; Chang, J.J.; Syberg, K.M.; et al. Ambient air pollution the risk of stillbirth: A prospective birth cohort study in Wuhan, China. Int. J. Hyg. Environ. Health 2018, 221, 502–509. [Google Scholar] [CrossRef]
- Kannan, S.; Misra, D.P.; Dvonch, J.T.; Krishnakumar, A. Exposures to airborne particulate matter and adverse perinatal outcomes: A biologically plausible mechanistic framework for exploring potential effect modification by nutrition. Environ. Health Perspect. 2006, 114, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Bekkar, B.; Pacheco, S.; Basu, R.; DeNicola, N. Association of Air Pollution and Heat Exposure With Preterm Birth, Low Birth Weight, and Stillbirth in the US: A Systematic Review. JAMA Netw. Open 2020, 3, e208243. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Perera, F.; Mrozek-Budzyn, D.; Mroz, E.; Flak, E.; Spengler, J.D.; Edwards, S.; Jacek, R.; Kaim, I.; Skolicki, Z. Gender differences in fetal growth of newborns exposed prenatally to airborne fine particulate matter. Environ. Res. 2009, 109, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Challis, J.; Newnham, J.; Petraglia, F.; Yeganegi, M.; Bocking, A. Fetal sex and preterm birth. Placenta 2013, 34, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Bukowski, R.; Smith, G.C.; Malone, F.D.; Ball, R.H.; Nyberg, D.A.; Comstock, C.H.; Hankins, G.D.; Berkowitz, R.L.; Gross, S.J.; Dugoff, L.; et al. Human sexual size dimorphism in early pregnancy. Am. J. Epidemiol. 2007, 165, 1216–1218. [Google Scholar] [CrossRef]
- Peters, A.; Döring, A.; Wichmann, H.E.; Koenig, W. Increased plasma viscosity during an air pollution episode: A link to mortality? Lancet 1997, 349, 1582–1587. [Google Scholar] [CrossRef]
- Edwards, A.; Megens, A.; Peek, M.; Wallace, E.M. Sexual origins of placental dysfunction. Lancet 2000, 355, 203–204. [Google Scholar] [CrossRef]
- Ghidini, A.; Salafia, C.M. Gender differences of placental dysfunction in severe prematurity. Bjog 2005, 112, 140–144. [Google Scholar] [CrossRef]
- Hu, W.; Wang, Y.; Wang, T.; Ji, Q.; Jia, Q.; Meng, T.; Ma, S.; Zhang, Z.; Li, Y.; Chen, R.; et al. Ambient particulate matter compositions and increased oxidative stress: Exposure-response analysis among high-level exposed population. Environ. Int. 2021, 147, 106341. [Google Scholar] [CrossRef]
- Pilger, A.; Rüdiger, H.W. 8-Hydroxy-2′-deoxyguanosine as a marker of oxidative DNA damage related to occupational and environmental exposures. Int. Arch. Occup. Environ. Health 2006, 80, 1–15. [Google Scholar] [CrossRef]
- Poulsen, H.E.; Loft, S.; Prieme, H.; Vistisen, K.; Lykkesfeldt, J.; Nyyssonen, K.; Salonen, J.T. Oxidative DNA damage in vivo: Relationship to age, plasma antioxidants, drug metabolism, glutathione-S-transferase activity and urinary creatinine excretion. Free Radic. Res. 1998, 29, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Liu, Y.; Liu, B.; Hu, Y.Q.; Ding, Y.Q.; Zhang, J.; Feng, L. Maternal urban particulate matter exposure and signaling pathways in fetal brains and neurobehavioral development in offspring. Toxicology 2022, 474, 153225. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, H.N.O.; Türker, P.F. Fetal programming: Could intrauterin life affect health status in adulthood? Obstet. Gynecol. Sci. 2021, 64, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Zhang, Y.; Wang, W.; Chen, R.; Liu, Y.; Liu, C.; Kan, H.; Gao, Y.; Tian, Y. Critical windows for maternal fine particulate matter exposure and adverse birth outcomes: The Shanghai birth cohort study. Chemosphere 2020, 240, 124904. [Google Scholar] [CrossRef]
- Li, Z.; Wen, Q.; Zhang, R. Sources, health effects and control strategies of indoor fine particulate matter (PM2.5): A review. Sci. Total Environ. 2017, 586, 610–622. [Google Scholar] [CrossRef]
- Park, S.; Marcotte, R.T.; Staudenmayer, J.W.; Strath, S.J.; Freedson, P.S.; Chasan-Taber, L. The impact of the COVID-19 pandemic on physical activity and sedentary behavior during pregnancy: A prospective study. BMC Pregnancy Childbirth 2022, 22, 899. [Google Scholar] [CrossRef]
- Ju, M.J.; Oh, J.; Choi, Y.H. Changes in air pollution levels after COVID-19 outbreak in Korea. Sci. Total Environ. 2021, 750, 141521. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | NBW (n = 1569) | LBW (n = 311) | p-Value | ||
|---|---|---|---|---|---|
| Age (years) | 33.20 | 4.16 | 32.79 | 4.47 | 0.12 |
| Pre-BMI (kg/m2) | 21.46 | 3.59 | 21.52 | 3.65 | 0.92 |
| GAB (wks) | 39.02 | 1.35 | 33.30 | 3.49 | <0.01 * |
| Neonate Sex | |||||
| Male | 791 | 82.14% | 172 | 17.86% | 0.12 |
| Female | 780 | 84.78% | 140 | 15.22% | |
| Birth weight (g) | 3266.44 | 394.83 | 1824.04 | 497.55 | <0.01 * |
| Birth height (cm) | 49.76 | 1.88 | 42.08 | 4.06 | <0.01 * |
| APGAR 1 min | 9.30 | 1.12 | 6.76 | 2.54 | <0.01 * |
| APGAR 5 min | 9.88 | 0.55 | 8.27 | 2.24 | <0.01 * |
| Pregnancy complications | |||||
| PTB | 81 | 24.40% | 251 | 75.60% | <0.01 * |
| Mean | SD | Min | 25th | 50th | 75th | Max | p-Value | |
|---|---|---|---|---|---|---|---|---|
| [Cohort I] | 27.35 | 4.48 | 17.73 | 23.33 | 27.89 | 30.72 | 41.68 | <0.01 *,1 |
| [Cohort II] | <0.01 *,2 | |||||||
| Indoor | 10.57 | 10.47 | 0.53 | 4.35 | 7.8 | 12.02 | 69.25 | |
| Outdoor | 17.27 | 7.48 | 1.69 | 12.00 | 16.71 | 20.14 | 43.50 |
| Exposure Period | All Newborns | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|---|
| NBW (n = 1567) | LBW (n = 313) | p-Value | NBW (n = 791) | LBW (n = 169) | p-Value | NBW (n = 774) | LBW (n = 141) | p-Value | |
| Entire | 27.17 ± 4.30 | 27.40 ± 4.67 | 0.43 | 27.24 ± 4.37 | 27.79 ± 4.82 | 0.17 | 27.11 ± 4.24 | 26.93 ± 4.48 | 0.65 |
| First trimester | 28.75 ± 7.63 | 28.04 ± 7.70 | 0.15 | 28.91 ± 7.87 | 28.38 ± 7.94 | 0.45 | 28.59 ± 7.38 | 27.71 ± 7.42 | 0.21 |
| Second trimester | 26.23 ± 6.78 | 27.21 ± 6.53 | 0.02 * | 26.26 ± 6.70 | 27.89 ± 6.79 | 0.01 * | 26.22 ± 6.86 | 26.38 ± 6.15 | 0.78 |
| Third trimester | 26.40 ± 6.43 | 27.04 ± 8.56 | 0.23 | 26.39 ± 6.28 | 26.94 ± 8.63 | 0.46 | 26.38 ± 6.57 | 27.03 ± 8.40 | 0.40 |
| Exposure Period | All Newborns | Male Infants | Female Infants | ||||||
|---|---|---|---|---|---|---|---|---|---|
| PNBW (n = 84) | PLBW (n = 260) | p-Value | PNBW (n = 48) | PLBW (n = 149) | p-Value | PNBW (n = 36) | PLBW (n = 111) | p-Value | |
| Entire | 25.89 ± 4.15 | 27.29 ± 4.78 | 0.02 * | 25.06 ± 4.03 | 27.61 ± 4.90 | <0.01 * | 27.00 ± 4.10 | 26.87 ± 4.64 | 0.88 |
| First trimester | 25.81 ± 6.63 | 27.58 ± 7.57 | 0.05 | 24.35 ± 6.21 | 27.73 ± 7.65 | <0.01 * | 27.77 ± 6.76 | 27.48 ± 7.50 | 0.84 |
| Second trimester | 25.57 ± 6.26 | 27.25 ± 6.58 | 0.04 * | 24.82 ± 5.87 | 27.81 ± 6.82 | 0.01 * | 26.58 ± 6.69 | 26.51 ± 6.22 | 0.95 |
| Third trimester | 26.69 ± 6.15 | 27.23 ± 8.98 | 0.55 | 26.92 ± 5.61 | 27.27 ± 9.09 | 0.80 | 26.39 ± 6.86 | 27.02 ± 8.77 | 0.66 |
| Risk of LBW by PM2.5 Exposure (per 1 μg/m3) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| All Newborns | Male Infants | Female Infants | |||||||
| Stage | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Entire | 1.06 | 1.01–1.10 | 0.02 * | 1.12 | 1.04–1.20 | <0.01 * | 1.00 | 0.93–1.07 | 0.94 |
| First trimester | 1.02 | 1.00–1.05 | 0.08 | 1.05 | 1.01–1.10 | 0.02 * | 1.00 | 0.96–1.04 | 0.86 |
| Second trimester | 1.03 | 1.00–1.06 | 0.04 * | 1.07 | 1.03–1.12 | <0.01 * | 1.00 | 0.96–1.04 | 0.90 |
| Third trimester | 1.00 | 0.98–1.03 | 0.80 | 1.00 | 0.96–1.04 | 0.85 | 1.01 | 0.97–1.05 | 0.73 |
| Characteristics | Low PM2.5 (n = 191) | High PM2.5 (n = 115) | p-Value | ||
|---|---|---|---|---|---|
| Age (years) | 33.74 | ±3.62 | 33.12 | ±4.50 | 0.19 |
| Pre-BMI (kg/m2) | 21.86 | ±3.31 | 21.56 | ±3.17 | 0.43 |
| Married state | |||||
| Married | 167 | 100.0% | 133 | 97.8% | 0.16 |
| Unmarried | 0 | 0.0% | 3 | 2.2% | |
| Education level | 0.14 | ||||
| High school graduation or below | 13 | 6.8% | 13 | 9.5% | |
| University graduates | 154 | 92.3% | 123 | 90.4% | |
| Occupation | |||||
| Yes | 112 | 67.1% | 94 | 69.1% | 0.70 |
| No | 55 | 32.9% | 42 | 30.9% | |
| Monthly income | |||||
| <4 million won | 35 | 36.1% | 35 | 37.6% | 0.95 |
| 4–6 million won | 27 | 27.8% | 24 | 25.8% | |
| >6 million won | 35 | 36.1% | 34 | 36.6% | |
| Gravidity | |||||
| 1 | 80 | 47.9% | 68 | 50.0% | 0.65 |
| 2 | 61 | 36.5% | 50 | 36.8% | |
| ≥3 | 26 | 15.6% | 18 | 13.2% | |
| Pregnancy methods | |||||
| Natural | 143 | 85.6% | 116 | 85.3% | 0.91 |
| IUI | 2 | 1.2% | 1 | 0.7% | |
| IVF-ET | 22 | 13.2% | 19 | 14.0% | |
| Low PM2.5 (n = 191) | High PM2.5 (n = 115) | p-Value | |||
|---|---|---|---|---|---|
| Oxidative stress marker | |||||
| 8-OHdG (ng/mL) | 92.20 | 61.16–138.19 | 113.55 | 79.69–153.27 | 0.02 * |
| MDA (μM) | 18.49 | 8.66–37.18 | 16.02 | 9.99–30.34 | 0.54 |
| Inflammatory marker | |||||
| Hs-CRP (mg/L) | 2.00 | 1.00–3.00 | 1.79 | 1.00–2.99 | 0.74 |
| WBC (1 × 103/μL) | 8.80 | 7.00–9.72 | 8.00 | 7.00–10.00 | 0.98 |
| Low PM2.5 (n = 191) | High PM2.5 (n = 115) | p-Value | |||
|---|---|---|---|---|---|
| Pregnancy outcome | |||||
| GAB (wks) | 38.22 | ±1.59 | 37.96 | ±1.95 | 0.22 |
| Delivery mode | 0.86 | ||||
| ND | 61 | 36.5% | 51 | 37.5% | |
| CS | 106 | 63.5% | 85 | 62.5% | |
| Neonate Sex | |||||
| Male | 112 | 58.9% | 56 | 49.1% | 0.10 |
| Female | 78 | 41.1% | 58 | 50.9% | |
| Birth weight (g) | 3150.7 | ±391.6 | 3112.0 | ±522.5 | 0.50 |
| Birth height (cm) | 49.5 | ±2.2 | 48.9 | ±2.8 | 0.04 * |
| APGAR 1 min | 8.45 | ±1.22 | 8.36 | ± | 0.61 |
| APGAR 5 min | 9.43 | ±0.84 | 9.21 | ±1.37 | 0.13 |
| Pregnancy complications | |||||
| LBW | 4 | 5.1% | 4 | 6.9% | 0.47 |
| LBH | 5 | 2.6% | 8 | 7.0% | 0.07 |
| PTB | 8 | 4.2% | 15 | 13.2% | <0.01 * |
| SGA | 1 | 0.6% | 7 | 5.1% | 0.01 * |
| NICU admission | 20 | 12.0% | 23 | 16.9% | 0.32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Kwon, E.; Lee, G.; You, Y.-A.; Kim, S.M.; Hur, Y.M.; Jung, S.; Jee, Y.; Park, M.H.; Na, S.H.; et al. Effect of Particulate Matter 2.5 on Fetal Growth in Male and Preterm Infants through Oxidative Stress. Antioxidants 2023, 12, 1916. https://doi.org/10.3390/antiox12111916
Park S, Kwon E, Lee G, You Y-A, Kim SM, Hur YM, Jung S, Jee Y, Park MH, Na SH, et al. Effect of Particulate Matter 2.5 on Fetal Growth in Male and Preterm Infants through Oxidative Stress. Antioxidants. 2023; 12(11):1916. https://doi.org/10.3390/antiox12111916
Chicago/Turabian StylePark, Sunwha, Eunjin Kwon, Gain Lee, Young-Ah You, Soo Min Kim, Young Min Hur, Sooyoung Jung, Yongho Jee, Mi Hye Park, Sung Hun Na, and et al. 2023. "Effect of Particulate Matter 2.5 on Fetal Growth in Male and Preterm Infants through Oxidative Stress" Antioxidants 12, no. 11: 1916. https://doi.org/10.3390/antiox12111916
APA StylePark, S., Kwon, E., Lee, G., You, Y. -A., Kim, S. M., Hur, Y. M., Jung, S., Jee, Y., Park, M. H., Na, S. H., Kim, Y. -H., Cho, G. J., Bae, J. -G., Lee, S. -J., Lee, S. H., & Kim, Y. J. (2023). Effect of Particulate Matter 2.5 on Fetal Growth in Male and Preterm Infants through Oxidative Stress. Antioxidants, 12(11), 1916. https://doi.org/10.3390/antiox12111916