
Low Vitamin C Concentrations in Patients with Community-Acquired Pneumonia Resolved with Pragmatic Administration of Intravenous and Oral Vitamin C

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Size
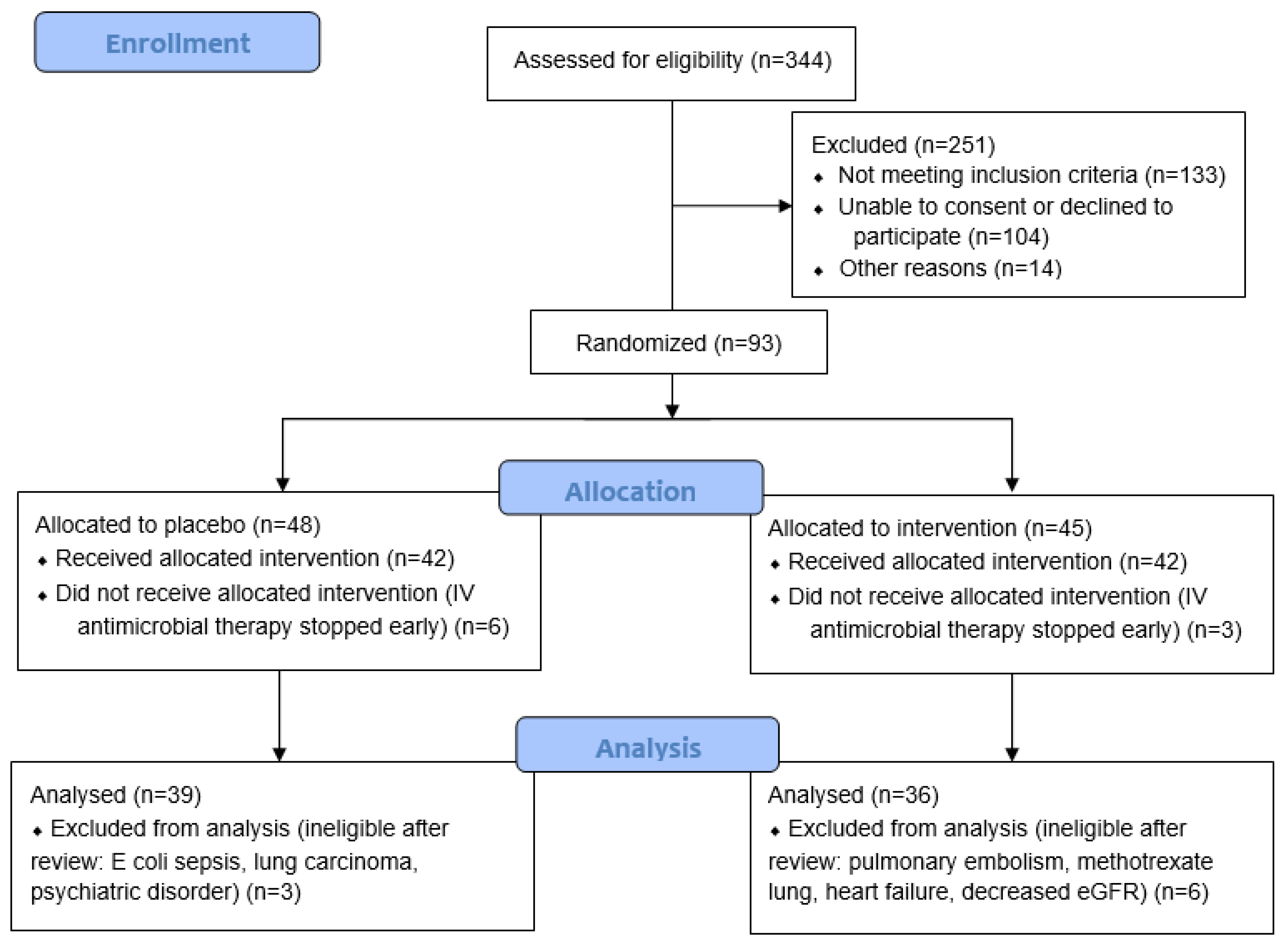
2.3. Randomisation and Masking
2.4. Intervention
2.5. Study Procedures
2.6. Biomarker Assessments
2.7. Statistical Analyses
3. Results
3.1. Participant Characteristics
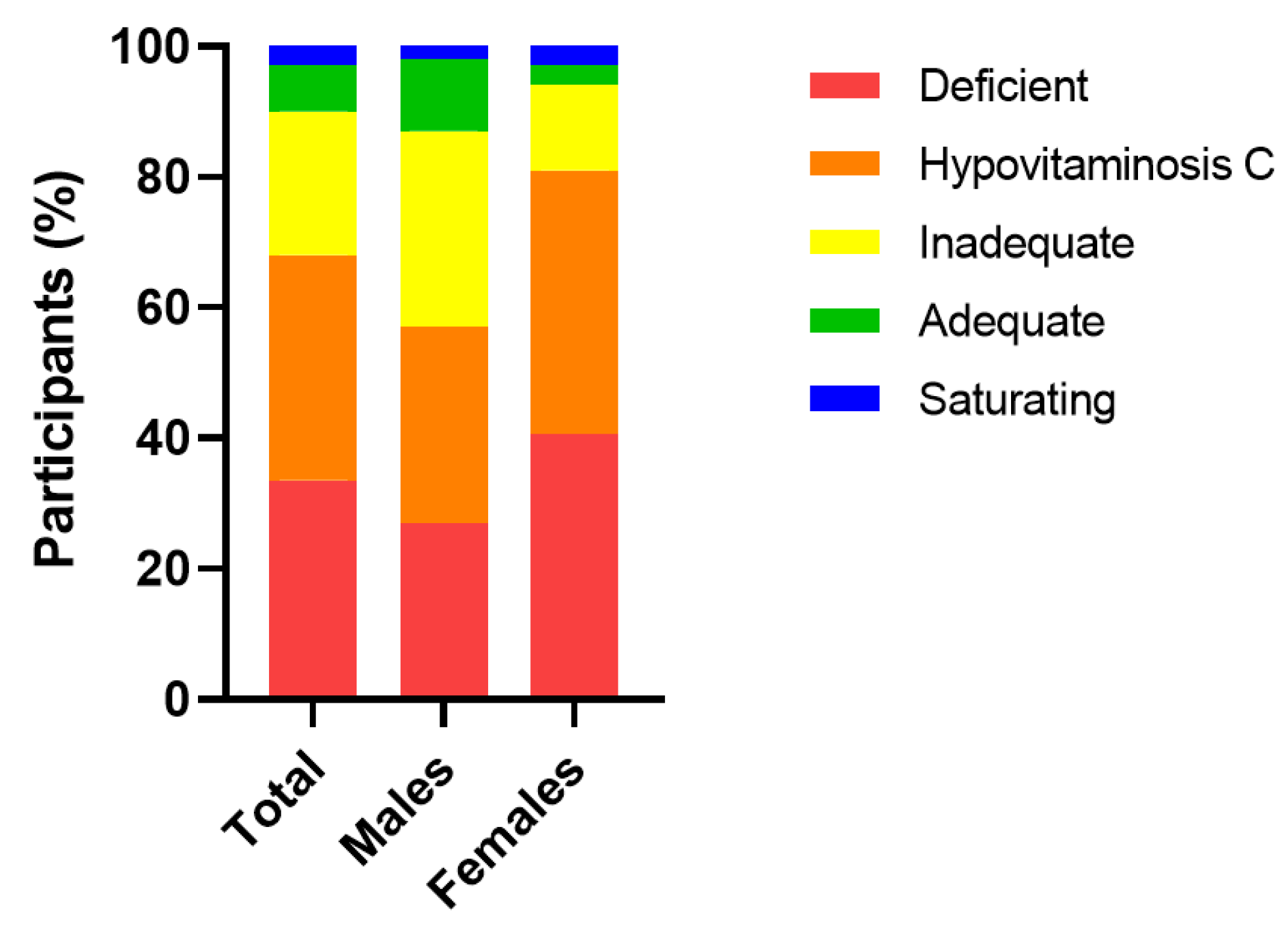
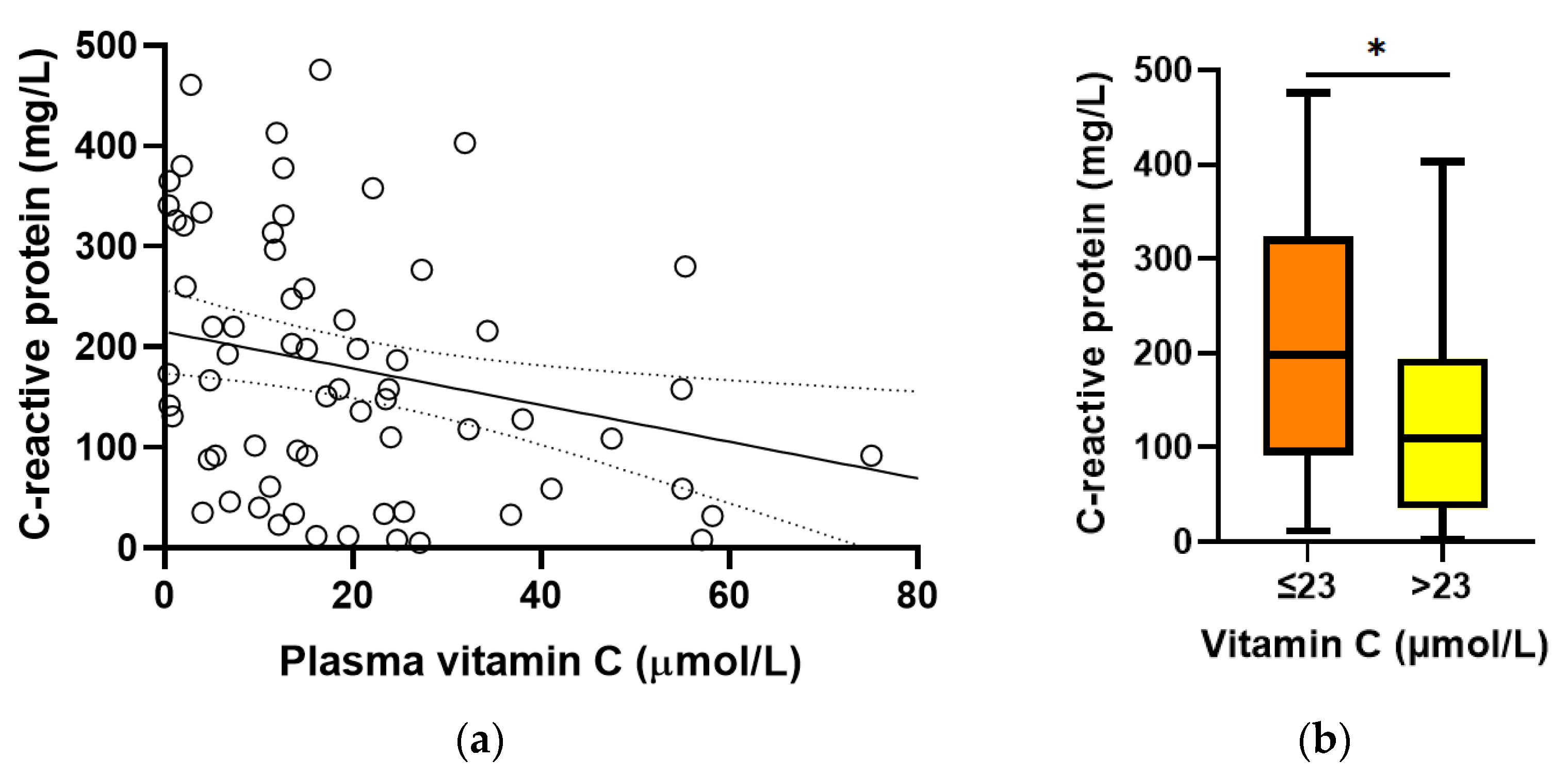
3.2. Baseline Plasma Vitamin C Concentrations
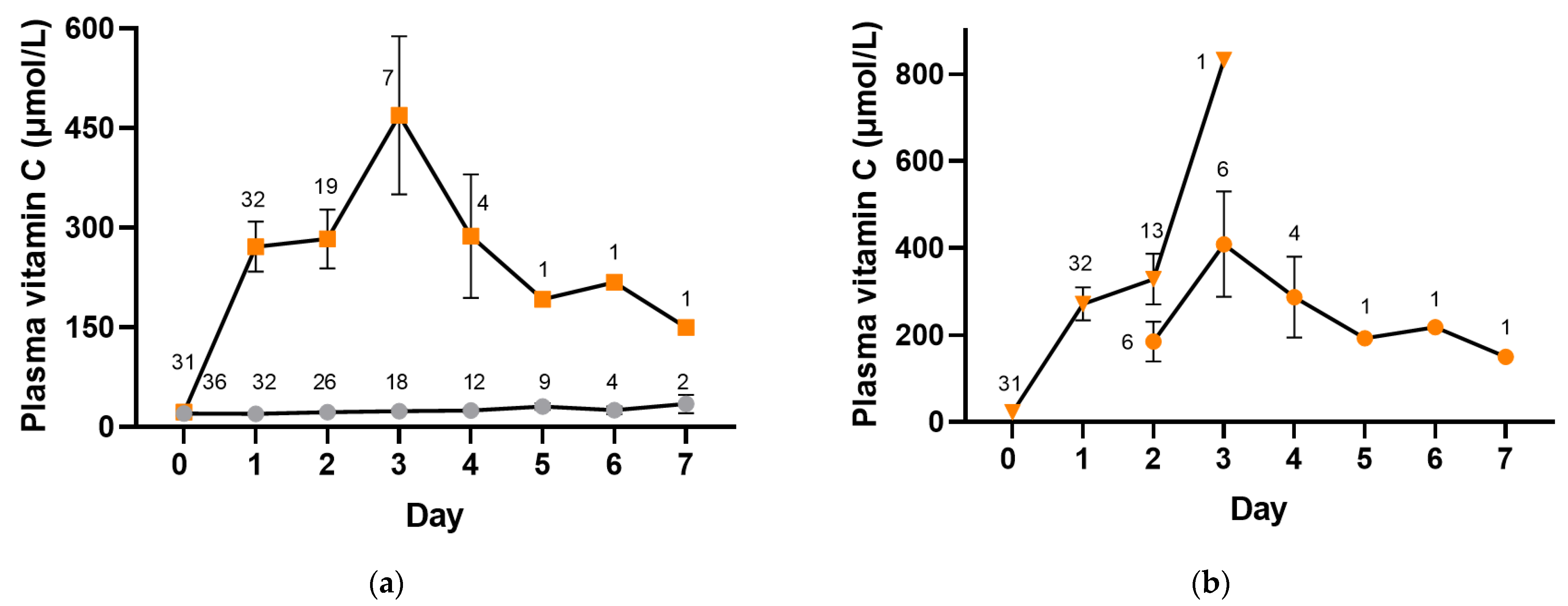
3.3. Plasma Concentrations Achieved with Intravenous and Oral Vitamin C
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cazzola, M.; Matera, M.G.; Pezzuto, G. Inflammation—A new therapeutic target in pneumonia. Respiration 2005, 72, 117–126. [Google Scholar] [CrossRef]
- Travlos, A.; Bakakos, A.; Vlachos, K.F.; Rovina, N.; Koulouris, N.; Bakakos, P. C-reactive protein as a predictor of survival and length of hospital stay in community-acquired pneumonia. J. Pers. Med. 2022, 12, 1710. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Spencer, E.; Dixon, L.; Chambers, S.T. Patients with community acquired pneumonia exhibit depleted vitamin C status and elevated oxidative stress. Nutrients 2020, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [Green Version]
- de Grooth, H.J.; Manubulu-Choo, W.P.; Zandvliet, A.S.; Spoelstra-de Man, A.M.E.; Girbes, A.R.; Swart, E.L.; Oudemans-van Straaten, H.M. Vitamin-C pharmacokinetics in critically ill patients: A randomized trial of four intravenous regimens. Chest 2018, 153, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Long, C.L.; Maull, K.I.; Krishnan, R.S.; Laws, H.L.; Geiger, J.W.; Borghesi, L.; Franks, W.; Lawson, T.C.; Sauberlich, H.E. Ascorbic acid dynamics in the seriously ill and injured. J. Surg. Res. 2003, 109, 144–148. [Google Scholar] [CrossRef]
- Carr, A.C. Vitamin C in pneumonia and sepsis. In Vitamin C: New Biochemical and Functional Insights. Oxidative Stress and Disease; Chen, Q., Vissers, M., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 115–135. [Google Scholar]
- Spencer, E.; Rosengrave, P.; Williman, J.; Shaw, G.; Carr, A.C. Circulating protein carbonyls are specifically elevated in critically ill patients with pneumonia relative to other sources of sepsis. Free Radic. Biol. Med. 2022, 179, 208–212. [Google Scholar] [CrossRef]
- Hemilä, H.; Louhiala, P. Vitamin C for preventing and treating pneumonia. Cochrane Database Syst. Rev. 2013, 8, Cd005532. [Google Scholar] [CrossRef] [Green Version]
- Hunt, C.; Chakravorty, N.K.; Annan, G.; Habibzadeh, N.; Schorah, C.J. The clinical effects of vitamin C supplementation in elderly hospitalised patients with acute respiratory infections. Int. J. Vitam. Nutr. Res. 1994, 64, 212–219. [Google Scholar]
- Mochalkin, N.I. Ascorbic acid in the complex therapy of acute pneumonia. Voen Med. Zh. 1970, 9, 17–21. Available online: http://www.mv.helsinki.fi/home/hemila/T5.pdf (accessed on 6 June 2023). [PubMed]
- Lykkesfeldt, J.; Tveden-Nyborg, P. The pharmacokinetics of vitamin C. Nutrients 2019, 11, 2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoodpoor, A.; Shadvar, K.; Sanaie, S.; Hadipoor, M.R.; Pourmoghaddam, M.A.; Saghaleini, S.H. Effect of Vitamin C on mortality of critically ill patients with severe pneumonia in intensive care unit: A preliminary study. BMC Infect. Dis. 2021, 21, 616. [Google Scholar] [CrossRef]
- Carr, A.C.; Gombart, A.F. Multi-level immune support by vitamins C and D during the SARS-CoV-2 pandemic. Nutrients 2022, 14, 689. [Google Scholar] [CrossRef] [PubMed]
- Holford, P.; Carr, A.C.; Zawari, M.; Vizcaychipi, M.P. Vitamin C intervention for critical COVID-19: A pragmatic review of the current level of evidence. Life 2021, 11, 1166. [Google Scholar] [CrossRef]
- Zhang, J.; Rao, X.; Li, Y.; Zhu, Y.; Liu, F.; Guo, G.; Luo, G.; Meng, Z.; De Backer, D.; Xiang, H.; et al. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 2021, 11, 5. [Google Scholar] [CrossRef]
- Chambers, S.T.; Storer, M.; Scott-Thomas, A.; Slow, S.; Williman, J.; Epton, M.; Murdoch, D.R.; Metcalf, S.; Carr, A.; Isenman, H.; et al. Adjunctive Intravenous then Oral Vitamin C for Moderate and Severe Community-Acquired Pneumonia in Hospitalized Adults: Feasibility of Randomized Controlled Trial. Sci. Rep. 2023, 13, 11879. [Google Scholar]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Neill, A.M.; Martin, I.R.; Weir, R.; Anderson, R.; Chereshsky, A.; Epton, M.J.; Jackson, R.; Schousboe, M.; Frampton, C.; Hutton, S.; et al. Community acquired pneumonia: Aetiology and usefulness of severity criteria on admission. Thorax 1996, 51, 1010–1016. [Google Scholar] [CrossRef] [Green Version]
- Blum, C.A.; Nigro, N.; Briel, M.; Schuetz, P.; Ullmer, E.; Suter-Widmer, I.; Winzeler, B.; Bingisser, R.; Elsaesser, H.; Drozdov, D.; et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: A multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015, 385, 1511–1518. [Google Scholar] [CrossRef]
- Pullar, J.M.; Bayer, S.; Carr, A.C. Appropriate handling, processing and analysis of blood samples is essential to avoid oxidation of vitamin C to dehydroascorbic acid. Antioxidants 2018, 7, E29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, A.C. Principles of Nutritional Assessment: Vitamin C. In Principles of Nutritional Assessment, 3rd ed.; Gibson, R., Ed.; Open Access; Available online: https://nutritionalassessment.org/vitaminc/index.html (accessed on 18 January 2023).
- Pearson, J.F.; Pullar, J.M.; Wilson, R.; Spittlehouse, J.K.; Vissers, M.C.M.; Skidmore, P.M.L.; Willis, J.; Cameron, V.A.; Carr, A.C. Vitamin C status correlates with markers of metabolic and cognitive health in 50-year-olds: Findings of the CHALICE cohort study. Nutrients 2017, 9, E831. [Google Scholar] [CrossRef] [Green Version]
- Padayatty, S.J.; Sun, H.; Wang, Y.; Riordan, H.D.; Hewitt, S.M.; Katz, A.; Wesley, R.A.; Levine, M. Vitamin C pharmacokinetics: Implications for oral and intravenous use. Ann. Intern. Med. 2004, 140, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.S.; Sabui, S.; Subramenium, G.A.; Marchant, J.S.; Said, H.M. Tumor Necrosis Factor alpha (TNF-alpha) reduces intestinal vitamin C uptake: A role for NF-kappaB mediated signaling. Am. J. Physiol. Gastrointest Liver Physiol. 2018, 315, G241–G248. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, V.S.; Sabui, S.; Moradi, H.; Marchant, J.S.; Said, H.M. Inhibition of intestinal ascorbic acid uptake by lipopolysaccharide is mediated via transcriptional mechanisms. Biochim. Biophys. Acta 2017, 1860, 556–565. [Google Scholar] [CrossRef]
- Trang, S.; Fraser, J.; Wilkinson, L.; Steckham, K.; Oliphant, H.; Fletcher, H.; Tzianetas, R.; Arcand, J. A multi-center assessment of nutrient levels and foods provided by hospital patient menus. Nutrients 2015, 7, 9256–9264. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort (n = 75) | Placebo Group (n = 39) | Vitamin C Group (n = 36) |
|---|---|---|---|
| Age, years | 76 (70, 83) | 77 (70, 83) | 76 (70, 85) |
| Gender, male | 42 (56) | 18 (46) | 24 (67) |
| Current smoker | 7 (9) | 4 (10) | 3 (8) |
| CURB-65 score | 3 (2, 3) | 3 (2, 3) | 2.5 (2, 3) |
| CURB-65 category | |||
| 2 | 36 (48) | 18 (46) | 18 (50) |
| 3 | 30 (40) | 14 (36) | 16 (44) |
| 4 | 9 (12) | 7 (18) | 2 (6) |
| C-reactive protein (mg/L) | 158 (61, 277) | 158 (62, 282) | 145 (60, 257) |
| Procalcitonin (ng/L) * | 414 (155, 1708) | 416 (154, 2940) | 344 (145, 1484) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, A.C.; Vlasiuk, E.; Zawari, M.; Scott-Thomas, A.; Storer, M.; Maze, M.; Chambers, S.T. Low Vitamin C Concentrations in Patients with Community-Acquired Pneumonia Resolved with Pragmatic Administration of Intravenous and Oral Vitamin C. Antioxidants 2023, 12, 1610. https://doi.org/10.3390/antiox12081610
Carr AC, Vlasiuk E, Zawari M, Scott-Thomas A, Storer M, Maze M, Chambers ST. Low Vitamin C Concentrations in Patients with Community-Acquired Pneumonia Resolved with Pragmatic Administration of Intravenous and Oral Vitamin C. Antioxidants. 2023; 12(8):1610. https://doi.org/10.3390/antiox12081610
Chicago/Turabian StyleCarr, Anitra C., Emma Vlasiuk, Masuma Zawari, Amy Scott-Thomas, Malina Storer, Michael Maze, and Stephen T. Chambers. 2023. "Low Vitamin C Concentrations in Patients with Community-Acquired Pneumonia Resolved with Pragmatic Administration of Intravenous and Oral Vitamin C" Antioxidants 12, no. 8: 1610. https://doi.org/10.3390/antiox12081610
APA StyleCarr, A. C., Vlasiuk, E., Zawari, M., Scott-Thomas, A., Storer, M., Maze, M., & Chambers, S. T. (2023). Low Vitamin C Concentrations in Patients with Community-Acquired Pneumonia Resolved with Pragmatic Administration of Intravenous and Oral Vitamin C. Antioxidants, 12(8), 1610. https://doi.org/10.3390/antiox12081610