The Association between Malaria and β-Carotene Levels: A Systematic Review and Meta-Analysis

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Protocol
2.2. Search Strategy and Selection Criteria
2.3. Eligibility Criteria and Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
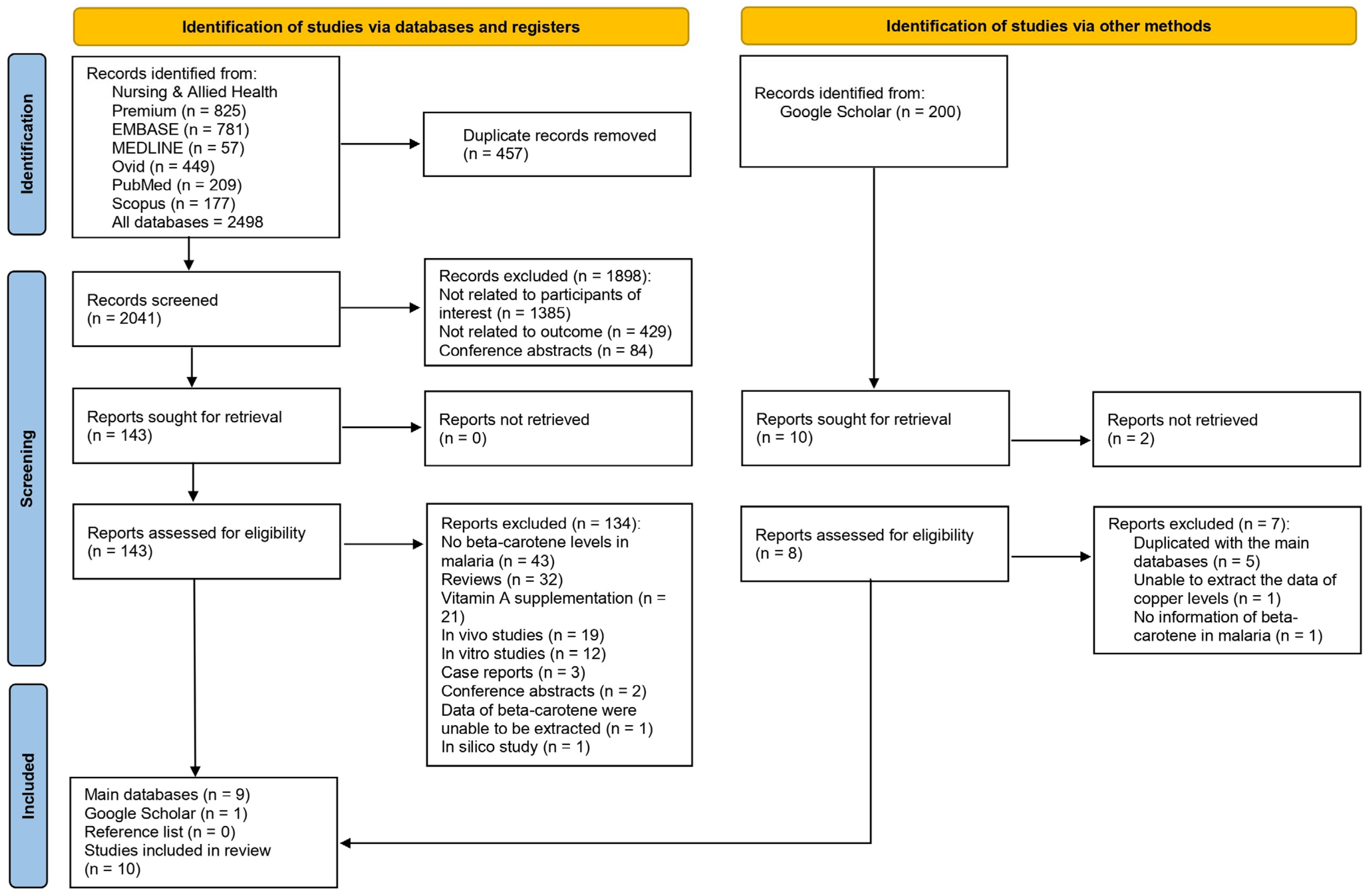
3.1. Search Results
3.2. Characteristics of Studies
3.3. Quality of Studies
3.4. Qualitative Synthesis
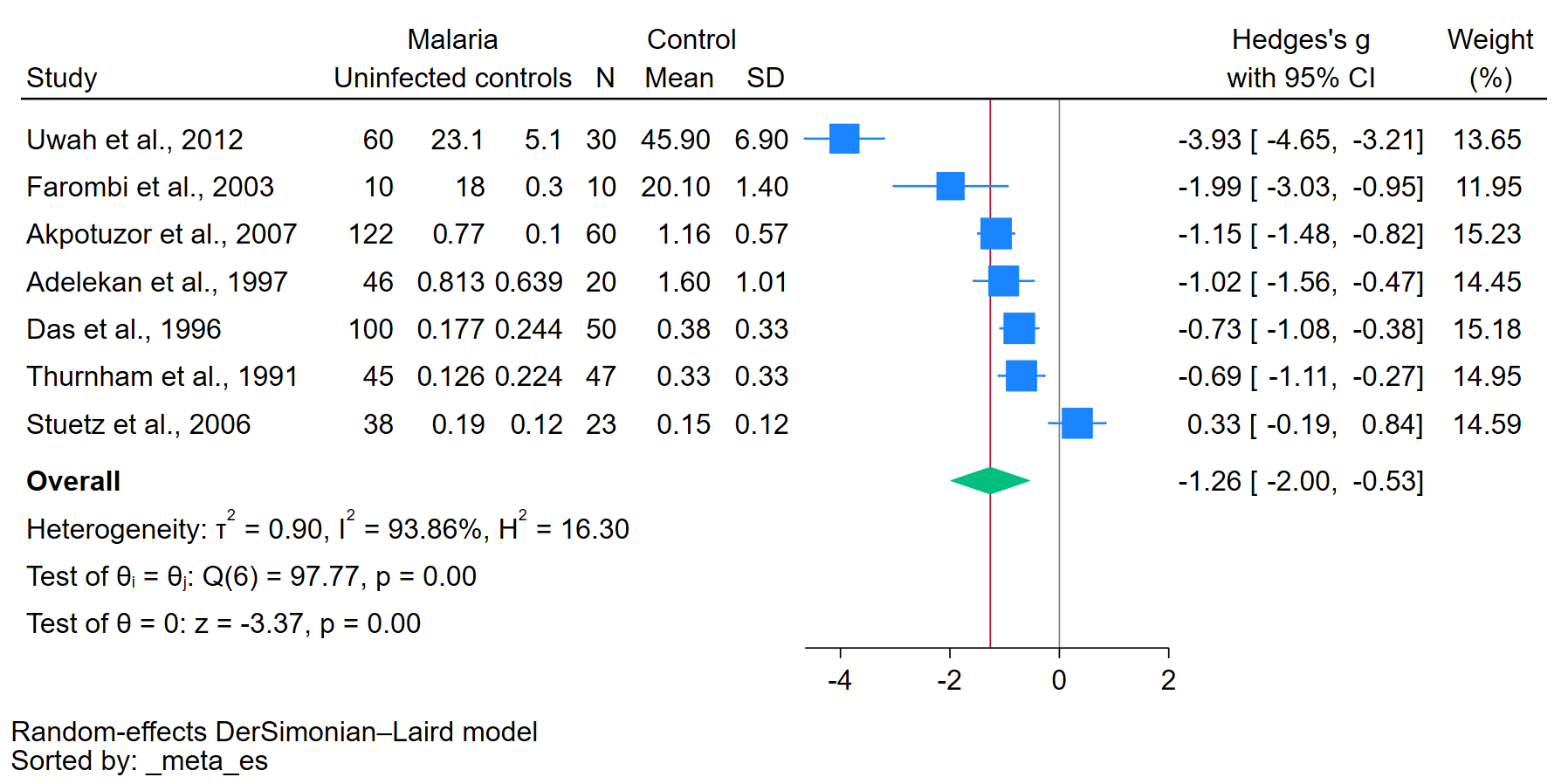
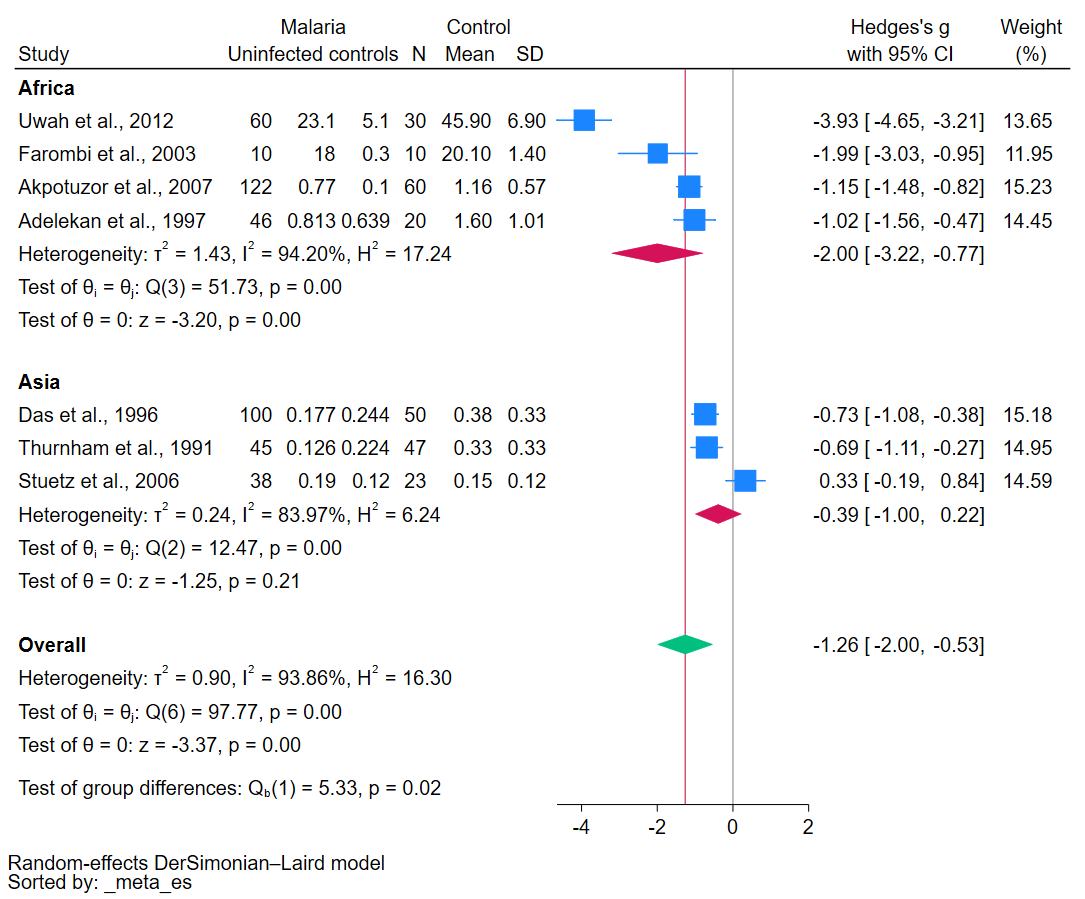
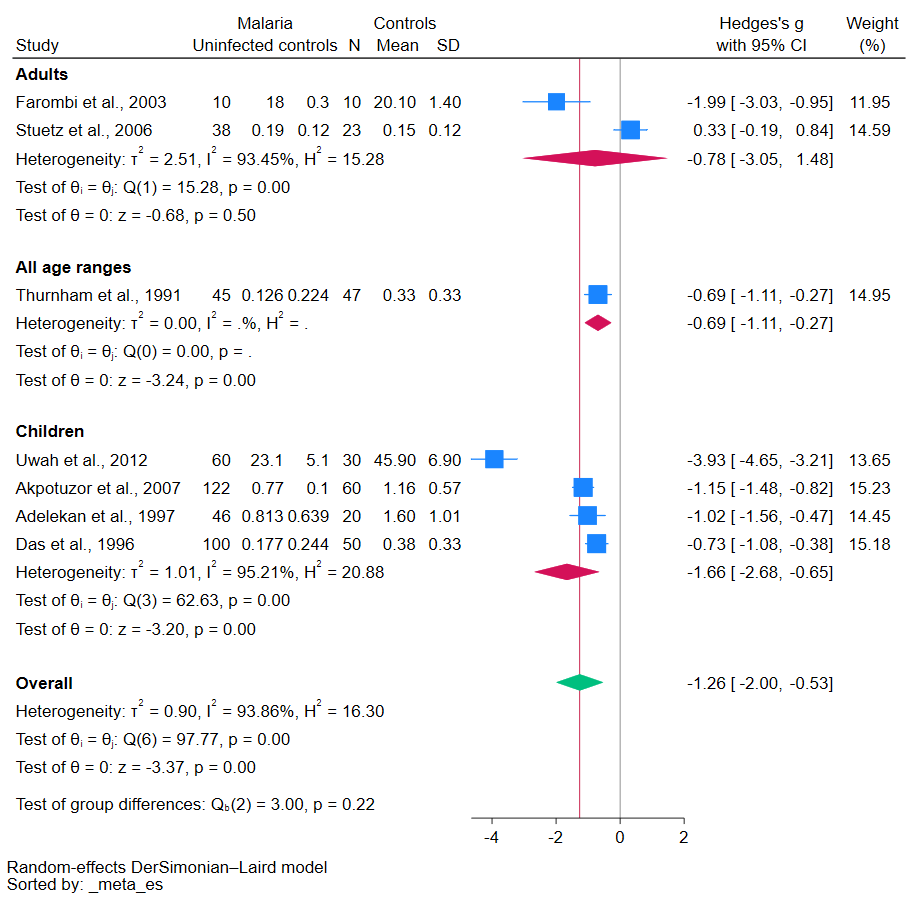
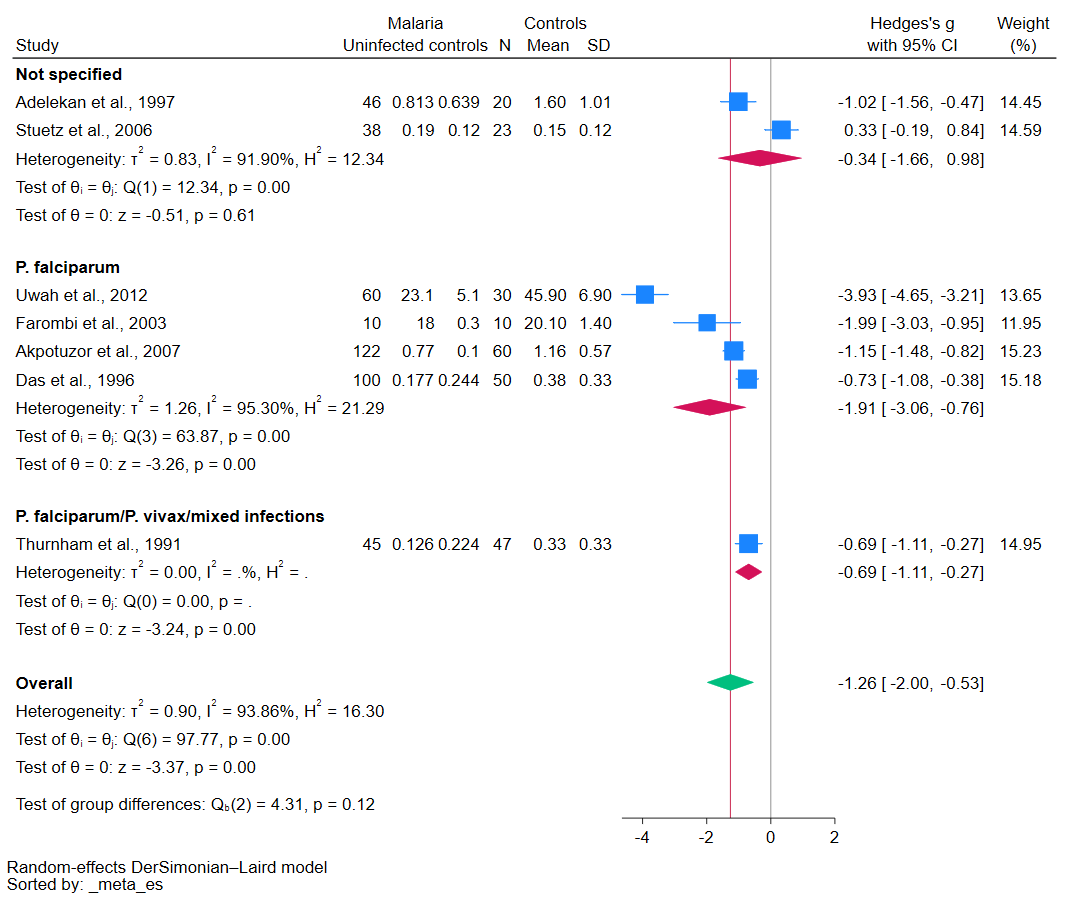
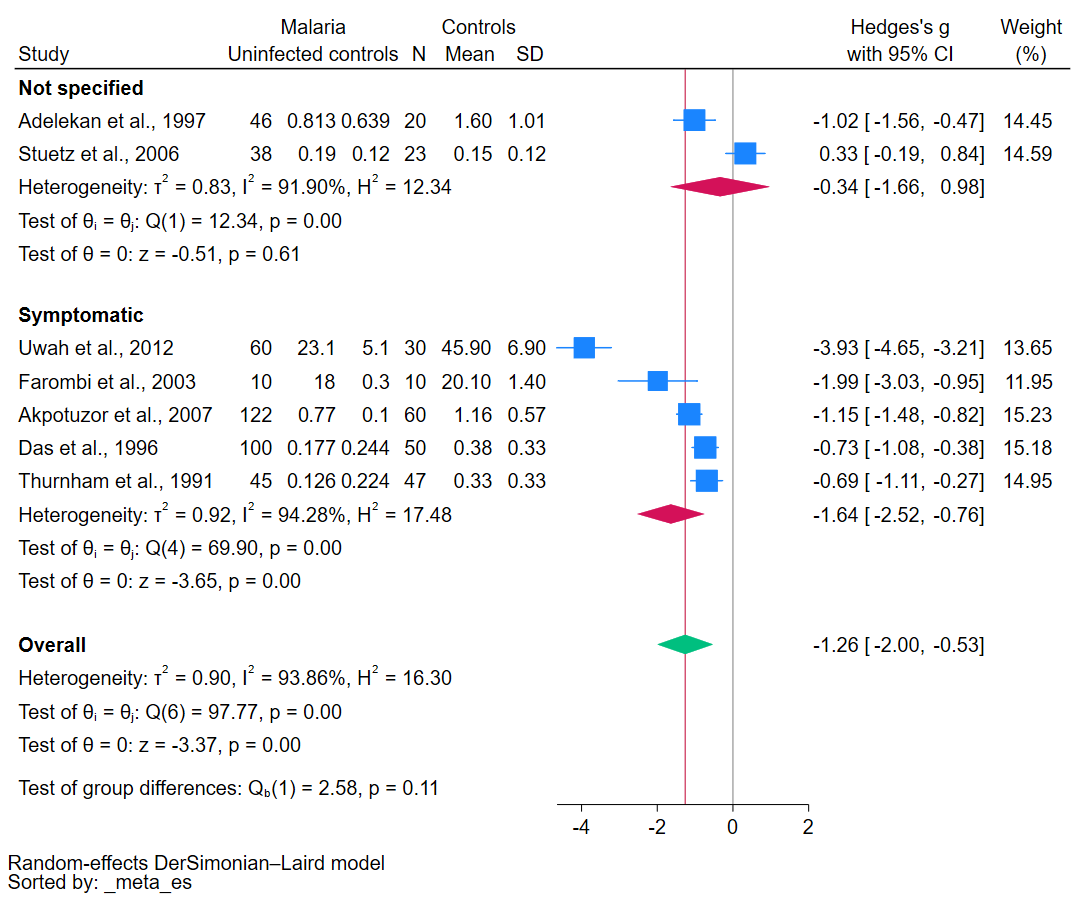
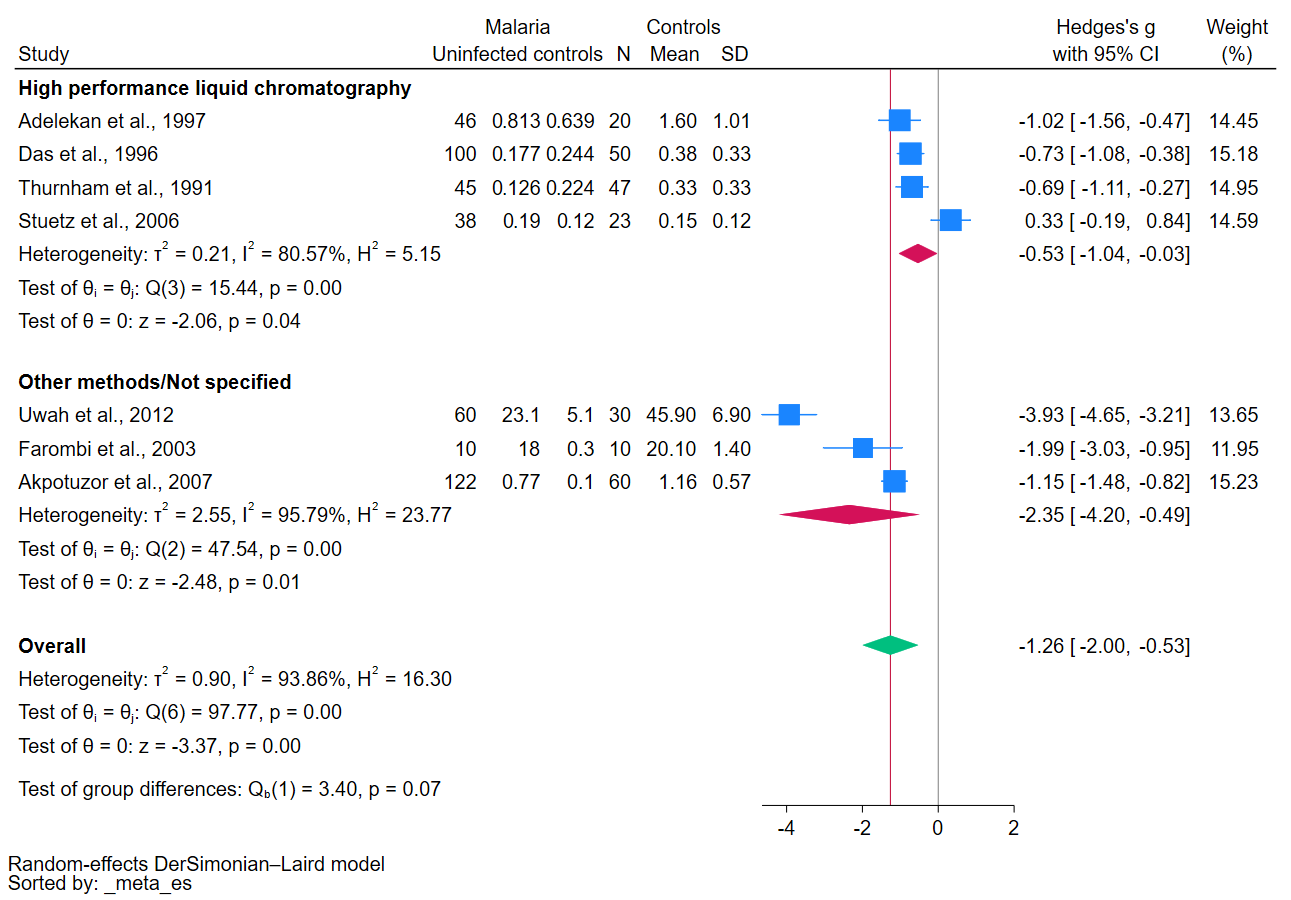
3.5. Meta-Analysis
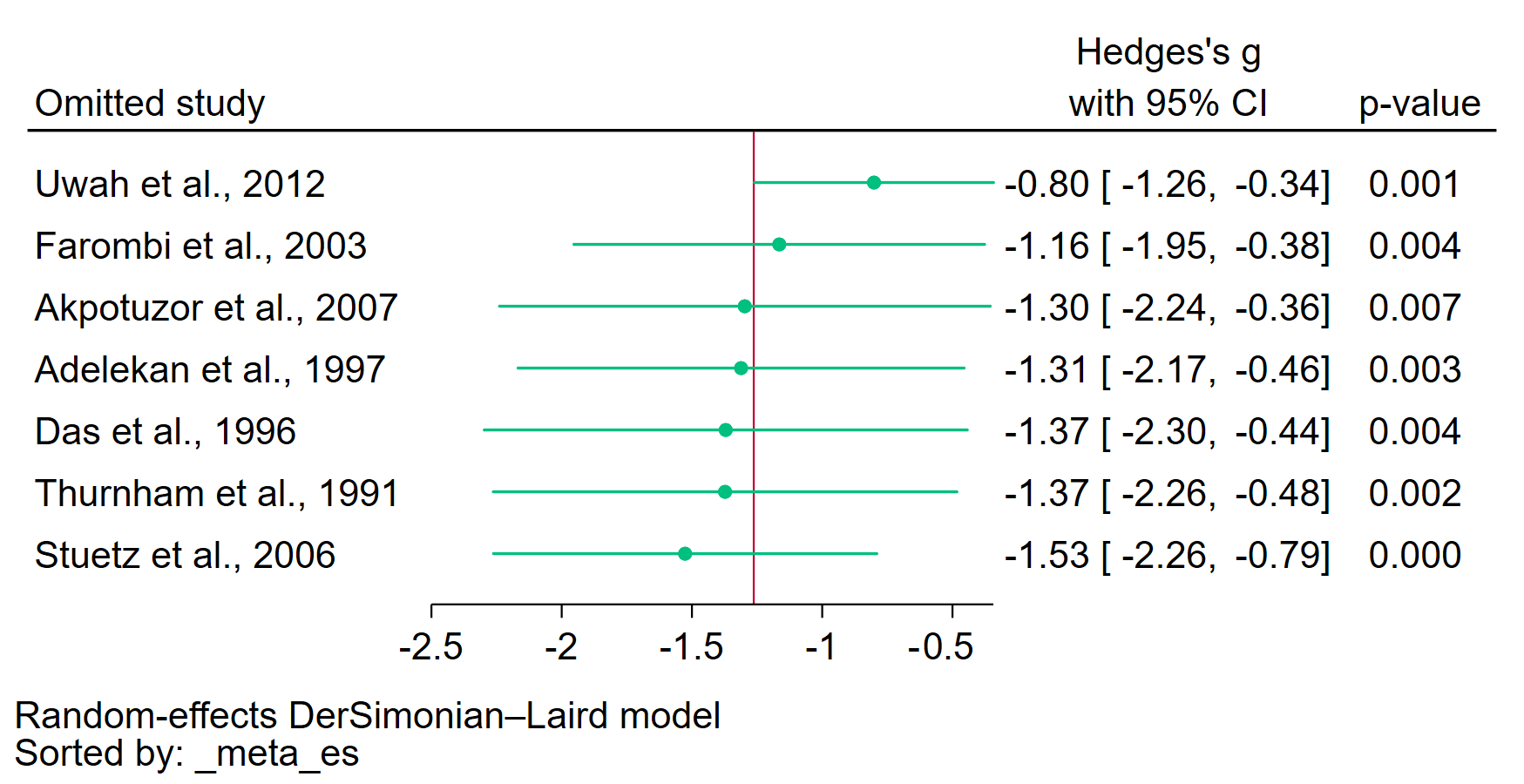
3.6. Sensitivity Analysis
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Malaria Report 2022. 2023. Available online: https://www.who.int/publications/i/item/9789240064898 (accessed on 10 August 2023).
- Sato, S. Plasmodium-a brief introduction to the parasites causing human malaria and their basic biology. J. Physiol. Anthropol. 2021, 40, 1. [Google Scholar] [CrossRef] [PubMed]
- Howes, R.E.; Battle, K.E.; Mendis, K.N.; Smith, D.L.; Cibulskis, R.E.; Baird, J.K.; Hay, S.I. Global Epidemiology of Plasmodium vivax. Am. J. Trop. Med. Hyg. 2016, 95 (Suppl. 6), 15–34. [Google Scholar] [CrossRef]
- Price, R.N.; Tjitra, E.; Guerra, C.A.; Yeung, S.; White, N.J.; Anstey, N.M. Vivax malaria: Neglected and not benign. Am. J. Trop. Med. Hyg. 2007, 77 (Suppl. 6), 79–87. [Google Scholar] [CrossRef] [PubMed]
- Oladipo, H.J.; Tajudeen, Y.A.; Oladunjoye, I.O.; Yusuff, S.I.; Yusuf, R.O.; Oluwaseyi, E.M.; AbdulBasit, M.O.; Adebisi, Y.A.; El-Sherbini, M.S. Increasing challenges of malaria control in sub-Saharan Africa: Priorities for public health research and policymakers. Ann. Med. Surg. 2022, 81, 104366. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Calls for Reinvigorated Action to Fight Malaria. 2020. Available online: https://www.who.int/news/item/30-11-2020-who-calls-for-reinvigorated-action-to-fight-malaria (accessed on 10 August 2023).
- Guyant, P.; Corbel, V.; Guerin, P.J.; Lautissier, A.; Nosten, F.; Boyer, S.; Coosemans, M.; Dondorp, A.M.; Sinou, V.; Yeung, S.; et al. Past and new challenges for malaria control and elimination: The role of operational research for innovation in designing interventions. Malar. J. 2015, 14, 279. [Google Scholar] [CrossRef] [PubMed]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. oxidative stress: Harms and benefits for human health. Oxid. Med. Cell Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef]
- Lobo, V.; Patil, A.; Phatak, A.; Chandra, N. Free radicals, antioxidants and functional foods: Impact on human health. Pharmacogn. Rev. 2010, 4, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.S.; Ahsan, H.; Zia, M.K.; Siddiqui, T.; Khan, F.H. Understanding oxidants and antioxidants: Classical team with new players. J. Food Biochem. 2020, 44, e13145. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.R.Q.; Cunha, N.; Varela, E.L.P.; Brigido, H.P.C.; Vale, V.V.; Dolabela, M.F.; De Carvalho, E.P.; Percario, S. Oxidative stress in malaria: Potential benefits of antioxidant therapy. Int. J. Mol. Sci. 2022, 23, 5949. [Google Scholar] [CrossRef]
- Mironczuk-Chodakowska, I.; Witkowska, A.M.; Zujko, M.E. Endogenous non-enzymatic antioxidants in the human body. Adv. Med. Sci. 2018, 63, 68–78. [Google Scholar] [CrossRef]
- Fiedor, J.; Fiedor, L.; Haessner, R.; Scheer, H. Cyclic endoperoxides of beta-carotene, potential pro-oxidants, as products of chemical quenching of singlet oxygen. Biochim. Biophys. Acta 2005, 1709, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Grune, T.; Lietz, G.; Palou, A.; Ross, A.C.; Stahl, W.; Tang, G.; Thurnham, D.; Yin, S.A.; Biesalski, H.K. Beta-carotene is an important vitamin A source for humans. J. Nutr. 2010, 140, 2268S–2285S. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.W.; Ingold, K.U. beta-Carotene: An unusual type of lipid antioxidant. Science 1984, 224, 569–573. [Google Scholar] [CrossRef]
- Krinsky, N.I.; Johnson, E.J. Carotenoid actions and their relation to health and disease. Mol. Asp. Med. 2005, 26, 459–516. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, Y.; Qi, G.; Brand, D.; Zheng, S.G. Role of vitamin A in the immune system. J. Clin. Med. 2018, 7, 258. [Google Scholar] [CrossRef]
- Narsaria, N.; Mohanty, C.; Das, B.K.; Mishra, S.P.; Prasad, R. Oxidative stress in children with severe malaria. J. Trop. Pediatr. 2012, 58, 147–150. [Google Scholar] [CrossRef]
- Griffiths, M.J.; Ndungu, F.; Baird, K.L.; Muller, D.P.; Marsh, K.; Newton, C.R. Oxidative stress and erythrocyte damage in Kenyan children with severe Plasmodium falciparum malaria. Br. J. Haematol. 2001, 113, 486–491. [Google Scholar] [CrossRef]
- Njoku, O.U.; Ononogbu, I.C.; Nwachukwu, D.E. Plasma cholesterol, B-carotene and ascorbic acid changes in human malaria. J. Commun. Dis. 1995, 27, 186–190. [Google Scholar]
- Nussenblatt, V.; Mukasa, G.; Metzger, A.; Ndeezi, G.; Eisinger, W.; Semba, R.D. Relationship between carotenoids and anaemia during acute uncomplicated Plasmodium falciparum malaria in children. J. Health Popul. Nutr. 2002, 20, 205–214. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk; JBI: Adelaide, Australia, 2020. [Google Scholar]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Adelekan, D.A.; Adeodu, O.O.; Thurnham, D.I. Comparative effects of malaria and malnutrition on plasma concentrations of antioxidant micronutrients in children. Ann. Trop. Paediatr. 1997, 17, 223–227. [Google Scholar] [CrossRef]
- Akpotuzor, J.O.; Udoh, A.E.; Etukudo, M.H. Total antioxidant status, vitamins A, C and ß-carotene levels of children with P. falciparum infection in University of Calabar Teaching Hospital (UCTH), Calabar. Pak. J. Nutr. 2007, 6, 485–489. [Google Scholar] [CrossRef]
- Benzecry, S.G.; Alexandre, M.A.; Vítor-Silva, S.; Salinas, J.L.; de Melo, G.C.; Marinho, H.A.; Paes, Â.T.; de Siqueira, A.M.; Monteiro, W.M.; Lacerda, M.V.; et al. Micronutrient deficiencies and Plasmodium vivax malaria among children in the Brazilian Amazon. PLoS ONE 2016, 11, e0151019. [Google Scholar] [CrossRef]
- Das, B.S.; Thurnham, D.I.; Das, D.B. Plasma α-tocopherol, retinol, and carotenoids in children with falciparum malaria. Am. J. Clin. Nutr. 1996, 64, 94–100. [Google Scholar] [CrossRef]
- Farombi, E.O.; Shyntum, Y.Y.; Emerole, G.O. Influence of chloroquine treatment and Plasmodium falciparum malaria infection on some enzymatic and non-enzymatic antioxidant defense indices in humans. Drug Chem. Toxicol. 2003, 26, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Stuetz, W.; McGready, R.; Cho, T.; Prapamontol, T.; Biesalski, H.K.; Stepniewska, K.; Nosten, F. Relation of DDT residues to plasma retinol, α-tocopherol, and β-carotene during pregnancy and malaria infection: A case-control study in Karen women in northern Thailand. Sci. Total Environ. 2006, 363, 78–86. [Google Scholar] [CrossRef]
- Thurnham, D.I.; Singkamani, R. The acute phase response and vitamin A status in malaria. Trans. R. Soc. Trop. Med. Hyg. 1991, 85, 194–199. [Google Scholar] [CrossRef]
- Uwah, A.F.; Otitoju, O.; Ndem, J.I.; Akpanabiatu, M.I.; Akpanyung, E.O. Effect of malaria infection on serum copper, iron and beta-carotene levels in Nigerian children Eur. J. Sci. Res. 2012, 86, 573–579. [Google Scholar]
- Caulfield, L.E.; Richard, S.A.; Black, R.E. Undernutrition as an underlying cause of malaria morbidity and mortality in children less than five years old. Am. J. Trop. Med. Hyg. 2004, 71 (Suppl. 2), 55–63. [Google Scholar] [CrossRef]
- Mrimi, E.C.; Palmeirim, M.S.; Minja, E.G.; Long, K.Z.; Keiser, J. Malnutrition, anemia, micronutrient deficiency and parasitic infections among schoolchildren in rural Tanzania. PLoS Negl. Trop. Dis. 2022, 16, e0010261. [Google Scholar] [CrossRef]
- Abdulkareem, B.O.; Adam, A.O.; Ahmed, A.O.; Mariam, A.A.; Samuel, U.U. Malaria-induced anaemia and serum micronutrients in asymptomatic Plasmodium falciparum infected patients. J. Parasit. Dis. 2017, 41, 1093–1097. [Google Scholar] [CrossRef]
- Chiste, R.C.; Freitas, M.; Mercadante, A.Z.; Fernandes, E. Carotenoids are effective inhibitors of in vitro hemolysis of human erythrocytes, as determined by a practical and optimized cellular antioxidant assay. J. Food Sci. 2014, 79, H1841-7. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Mahittikorn, A.; Anabire, N.G.; Masangkay, F.R.; Kotepui, K.U. Malaria is associated with diminished levels of ascorbic acid: A systematic review and meta-analysis. Antioxid. Redox Signal 2023. [Google Scholar] [CrossRef] [PubMed]
- Kotepui, M.; Masangkay, F.R.; Mahittikorn, A.; Kotepui, K.U. Effect of malaria on blood levels of vitamin e: A systematic review and meta-analysis. Nutrients 2023, 15, 3472. [Google Scholar] [PubMed]
- Varela, E.L.P.; Gomes, A.R.Q.; da Silva Barbosa Dos Santos, A.; de Carvalho, E.P.; Vale, V.V.; Percario, S. Potential benefits of lycopene consumption: Rationale for using it as an adjuvant treatment for malaria patients and in several diseases. Nutrients 2022, 14, 5303. [Google Scholar] [CrossRef] [PubMed]
- Metzger, A.; Mukasa, G.; Shankar, A.H.; Ndeezi, G.; Melikian, G.; Semba, R.D. Antioxidant status and acute malaria in children in Kampala, Uganda. Am. J. Trop. Med. Hyg. 2001, 65, 115–119. [Google Scholar] [CrossRef]
- Faber, M.; Laubscher, R. Seasonal availability and dietary intake of beta-carotene-rich vegetables and fruit of 2-year-old to 5-year-old children in a rural South African setting growing these crops at household level. Int. J. Food Sci. Nutr. 2008, 59, 46–60. [Google Scholar] [CrossRef] [PubMed]
- Villamor, E.; Msamanga, G.; Saathoff, E.; Fataki, M.; Manji, K.; Fawzi, W.W. Effects of maternal vitamin supplements on malaria in children born to HIV-infected women. Am. J. Trop. Med. Hyg. 2007, 76, 1066–1071. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (10 Studies) |
|---|---|
| Publication year | |
| Before 2000 | 4 |
| 2000–2009 | 4 |
| 2010–2019 | 2 |
| Study designs | |
| Case-control studies | 5 |
| Cohort studies | 4 |
| Cross-sectional studies | 1 |
| Study areas | |
| Africa | |
| Nigeria | 5 |
| Uganda | 1 |
| Asia | |
| Thailand | 2 |
| India | 1 |
| South America | |
| Brazil | 1 |
| Plasmodium species | |
| P. falciparum | 6 |
| P. vivax | 1 |
| P. falciparum, P. vivax, mixed infections | 1 |
| Not specified | 2 |
| Age group | |
| Children | 6 |
| Adults | 2 |
| Children, adults | 2 |
| Clinical status | |
| Symptomatic | 7 |
| Not specified | 3 |
| Methods for malaria detection | |
| Microscopy | 9 |
| Microscopy/PCR | 1 |
| Methods for β-carotene measurement | |
| HPLC | 6 |
| Other methods | 3 |
| Not specified | 1 |
| Meta-Analysis of β-Carotene | Covariates | p-Value | tau2 | I2 (%) | R-Squared (%) | Number of Studies |
|---|---|---|---|---|---|---|
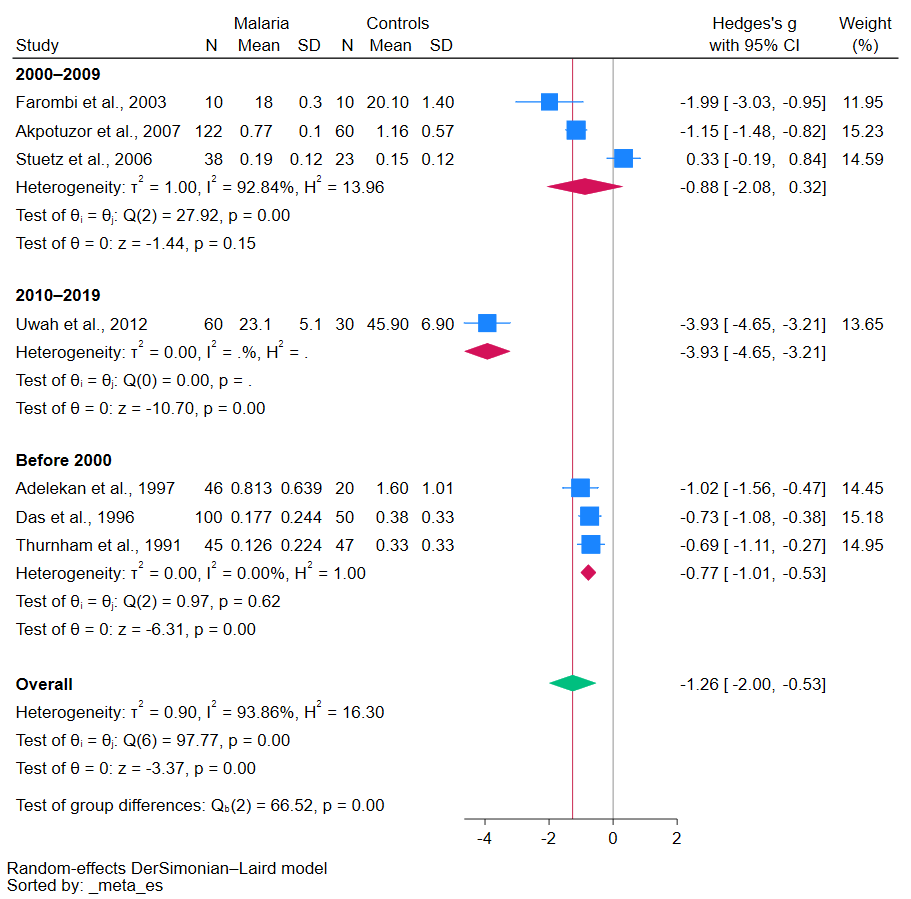
| Malaria patients vs. uninfected individuals | Publication years | <0.01 | 0.368 | 86.15 | 58.88 | 7 |
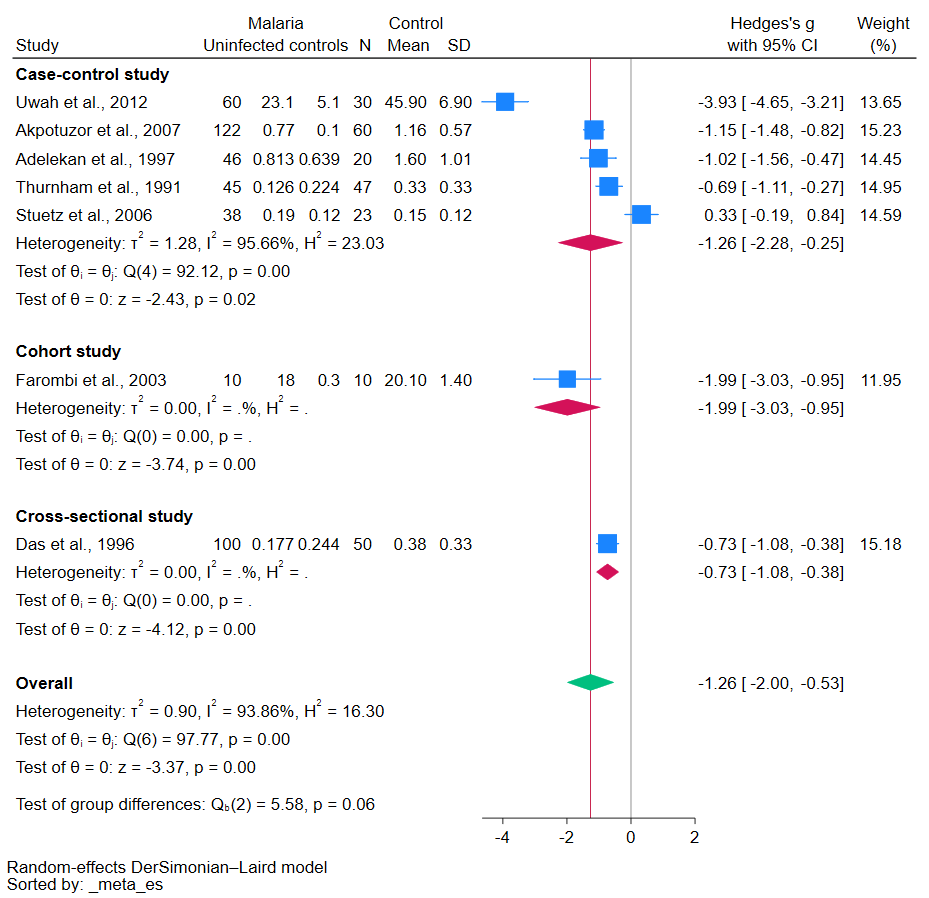
| Study design | 0.760 | 1.284 | 95.66 | 0.00 | 7 | |
| Continent | 0.022 | 0.764 | 92.21 | 14.67 | 7 | |
| Age group | 0.169 | 0.885 | 94.42 | 1.14 | 7 | |
| Plasmodium species | 0.231 | 1.167 | 94.75 | 0.00 | 7 | |
| Clinical status | 0.117 | 0.902 | 93.92 | 0.00 | 7 | |
| Methods for β-carotene | 0.011 | 0.763 | 92.06 | 14.82 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotepui, K.U.; Mahittikorn, A.; Wilairatana, P.; Masangkay, F.R.; Kotepui, M. The Association between Malaria and β-Carotene Levels: A Systematic Review and Meta-Analysis. Antioxidants 2023, 12, 1687. https://doi.org/10.3390/antiox12091687
Kotepui KU, Mahittikorn A, Wilairatana P, Masangkay FR, Kotepui M. The Association between Malaria and β-Carotene Levels: A Systematic Review and Meta-Analysis. Antioxidants. 2023; 12(9):1687. https://doi.org/10.3390/antiox12091687
Chicago/Turabian StyleKotepui, Kwuntida Uthaisar, Aongart Mahittikorn, Polrat Wilairatana, Frederick Ramirez Masangkay, and Manas Kotepui. 2023. "The Association between Malaria and β-Carotene Levels: A Systematic Review and Meta-Analysis" Antioxidants 12, no. 9: 1687. https://doi.org/10.3390/antiox12091687
APA StyleKotepui, K. U., Mahittikorn, A., Wilairatana, P., Masangkay, F. R., & Kotepui, M. (2023). The Association between Malaria and β-Carotene Levels: A Systematic Review and Meta-Analysis. Antioxidants, 12(9), 1687. https://doi.org/10.3390/antiox12091687