

SunGold Kiwifruit Consumption Restores Adequate to Optimal Vitamin C Status in People with a History of Severe Respiratory Infections

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment and Eligibility Criteria
2.3. Baseline Clinical Data
2.4. Intervention Dosing
2.5. Dietary Intake Assessment
2.6. Biosample Collection
2.7. Vitamin C Analyses
2.8. Inflammatory Biomarker Analyses
2.9. Oxidative Biomarker Analyses
2.10. Self-Reported Fatigue and Subjective Mood
2.11. Susceptibility and Severity of Respiratory Symptoms
2.12. Data Analysis
3. Results
3.1. Participant Characteristics
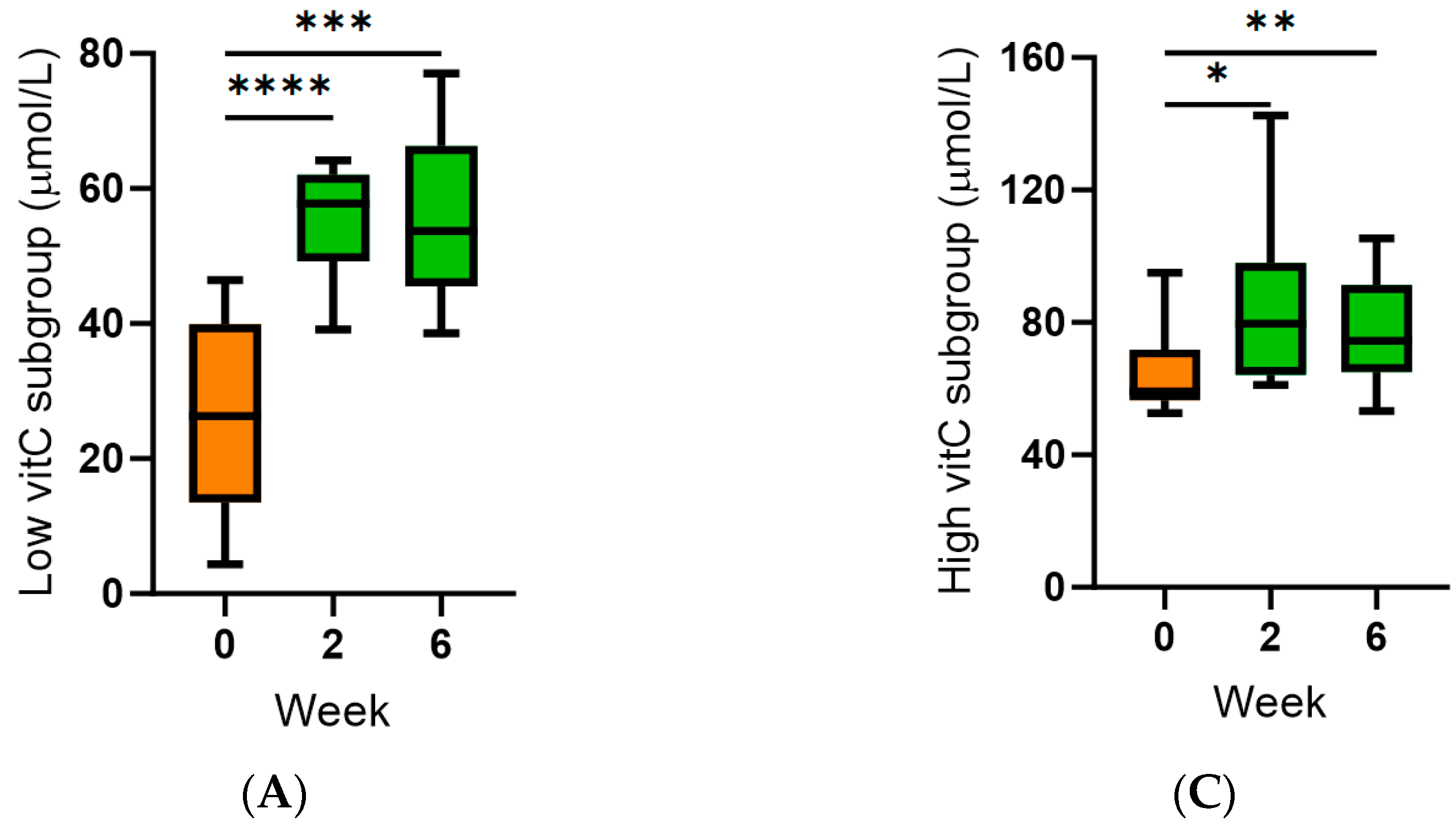
3.2. Effect of Kiwifruit Intervention on Vitamin C Status
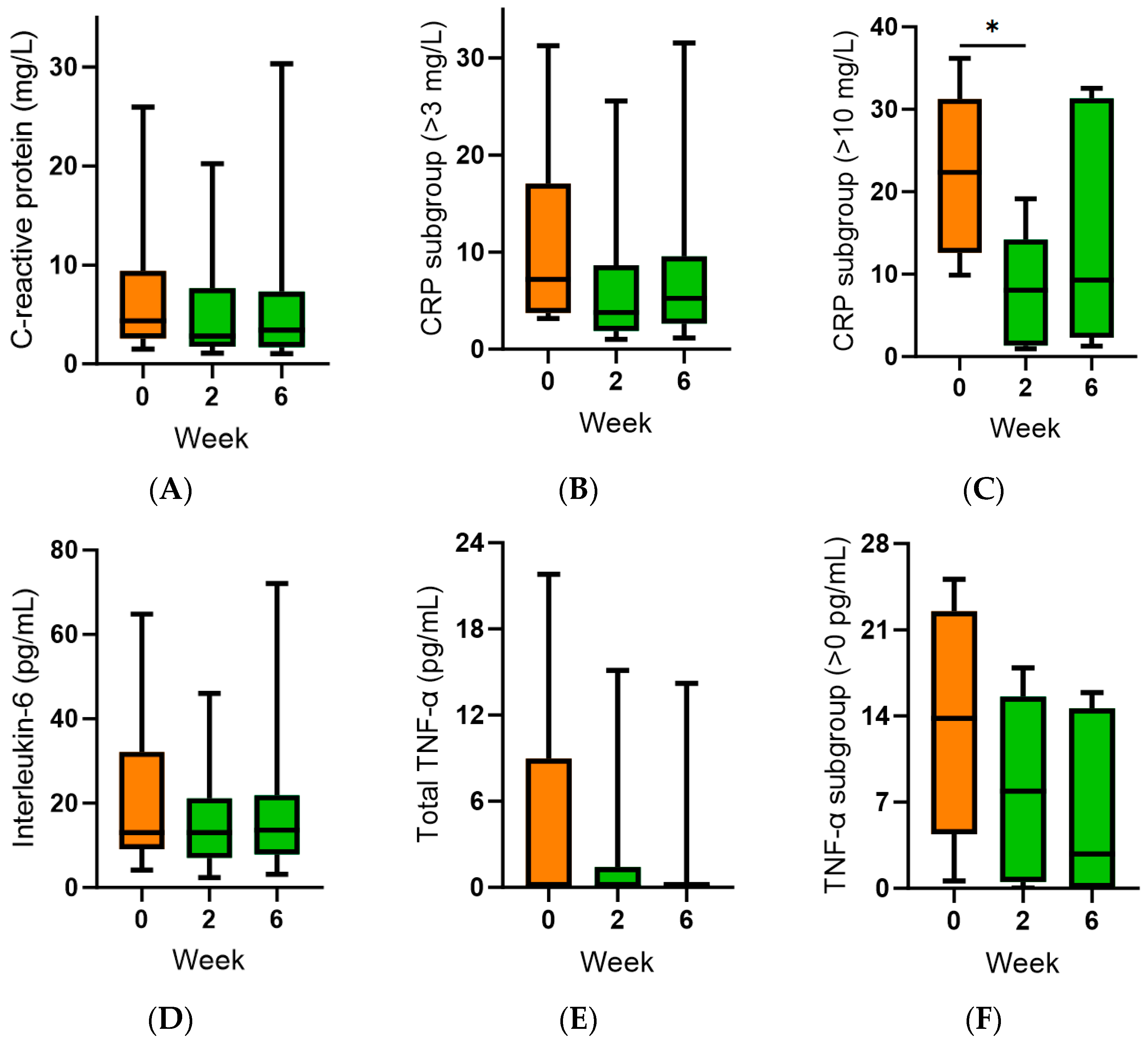
3.3. Effect of Kiwifruit Intervention on Inflammatory and Oxidative Biomarkers
3.4. Effect of Kiwifruit Intervention on Self-Reported Fatigue and Subjective Mood
3.5. Effect of Kiwifruit on Respiratory Symptom Incidence, Duration and Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carr, A.C.; Maggini, S. Vitamin C and immune function. Nutrients 2017, 9, E1211. [Google Scholar] [CrossRef]
- Hemilä, H. Vitamin C and infections. Nutrients 2017, 9, E339. [Google Scholar] [CrossRef]
- Bakaev, V.V.; Duntau, A.P. Ascorbic acid in blood serum of patients with pulmonary tuberculosis and pneumonia. Int. J. Tuberc. Lung Dis. 2004, 8, 263–266. [Google Scholar]
- Hunt, C.; Chakravorty, N.K.; Annan, G.; Habibzadeh, N.; Schorah, C.J. The clinical effects of vitamin C supplementation in elderly hospitalised patients with acute respiratory infections. Int. J. Vitam. Nutr. Res. 1994, 64, 212–219. [Google Scholar]
- Mochalkin, N.I. Ascorbic acid in the complex therapy of acute pneumonia. Voen. Med. Zh. 1970, 9, 17–21, (English Translation). Available online: http://www.mv.helsinki.fi/home/hemila/T5.pdf (accessed on 1 March 2021).
- Carr, A.C.; Spencer, E.; Dixon, L.; Chambers, S.T. Patients with community acquired pneumonia exhibit depleted vitamin C status and elevated oxidative stress. Nutrients 2020, 12, 1318. [Google Scholar] [CrossRef]
- Metnitz, P.G.; Bartens, C.; Fischer, M.; Fridrich, P.; Steltzer, H.; Druml, W. Antioxidant status in patients with acute respiratory distress syndrome. Intensive Care Med. 1999, 25, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Rosengrave, P.C.; Bayer, S.; Chambers, S.; Mehrtens, J.; Shaw, G.M. Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes. Crit. Care 2017, 21, 300. [Google Scholar] [CrossRef] [PubMed]
- de Grooth, H.J.; Manubulu-Choo, W.P.; Zandvliet, A.S.; Spoelstra-de Man, A.M.E.; Girbes, A.R.; Swart, E.L.; Oudemans-van Straaten, H.M. Vitamin-C pharmacokinetics in critically ill patients: A randomized trial of four intravenous regimens. Chest 2018, 153, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Long, C.L.; Maull, K.I.; Krishnan, R.S.; Laws, H.L.; Geiger, J.W.; Borghesi, L.; Franks, W.; Lawson, T.C.; Sauberlich, H.E. Ascorbic acid dynamics in the seriously ill and injured. J. Surg. Res. 2003, 109, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Edmond, K.; Scott, S.; Korczak, V.; Ward, C.; Sanderson, C.; Theodoratou, E.; Clark, A.; Griffiths, U.; Rudan, I.; Campbell, H. Long term sequelae from childhood pneumonia; systematic review and meta-analysis. PLoS ONE 2012, 7, e31239. [Google Scholar] [CrossRef]
- Martínez-García, M.; Faner, R.; Oscullo, G.; la Rosa-Carrillo, D.; Soler-Cataluña, J.J.; Ballester, M.; Muriel, A.; Agusti, A. Chronic Bronchial Infection Is Associated with More Rapid Lung Function Decline in Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2022, 19, 1842–1847. [Google Scholar] [CrossRef] [PubMed]
- Amati, F.; Simonetta, E.; Gramegna, A.; Tarsia, P.; Contarini, M.; Blasi, F.; Aliberti, S. The biology of pulmonary exacerbations in bronchiectasis. Eur. Respir. Rev. 2019, 28, 190055. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Hill, H.R. Role of Host Immune and Inflammatory Responses in COVID-19 Cases with Underlying Primary Immunodeficiency: A Review. J. Interferon Cytokine Res. 2020, 40, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Pincemail, J.; Cavalier, E.; Charlier, C.; Cheramy-Bien, J.P.; Brevers, E.; Courtois, A.; Fadeur, M.; Meziane, S.; Goff, C.L.; Misset, B.; et al. Oxidative Stress Status in COVID-19 Patients Hospitalized in Intensive Care Unit for Severe Pneumonia. Antioxidants 2021, 10, 257. [Google Scholar] [CrossRef] [PubMed]
- Trefler, S.; Rodriguez, A.; Martin-Loeches, I.; Sanchez, V.; Marin, J.; Llaurado, M.; Romeu, M.; Diaz, E.; Nogues, R.; Giralt, M. Oxidative stress in immunocompetent patients with severe community-acquired pneumonia. Med. Intensiv. 2014, 38, 73–82. [Google Scholar] [CrossRef]
- Buettner, G.R. The pecking order of free radicals and antioxidants: Lipid peroxidation, alpha-tocopherol, and ascorbate. Arch. Biochem. Biophys. 1993, 300, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Drummond, L. The composition and nutritional value of kiwifruit. Adv. Food Nutr. Res. 2013, 68, 33–57. [Google Scholar] [PubMed]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Simcock, J.W.; Vissers, M.C. A randomised steady-state bioavailability study of synthetic and natural (kiwifruit-derived) vitamin C. Nutrients 2013, 5, 3684–3695. [Google Scholar] [CrossRef]
- Hunter, D.C.; Skinner, M.A.; Wolber, F.M.; Booth, C.L.; Loh, J.M.; Wohlers, M.; Stevenson, L.M.; Kruger, M.C. Consumption of gold kiwifruit reduces severity and duration of selected upper respiratory tract infection symptoms and increases plasma vitamin C concentration in healthy older adults. Br. J. Nutr. 2012, 108, 1235–1245. [Google Scholar] [CrossRef]
- Rai, R.R.; Phadke, M.S. Plasma oxidant-antioxidant status in different respiratory disorders. Indian. J. Clin. Biochem. 2006, 21, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Sivakumaran, S.; Huffman, L.; Sivakumaran, S.; Drummond, L. The nutritional composition of Zespri® SunGold Kiwifruit and Zespri® Sweet Green Kiwifruit. Food Chem. 2018, 238, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Eating and Activity Guidelines for New Zealand Adults; Ministry of Health: Wellington, New Zealand, 2020; 148p. [Google Scholar]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; NHMRC Publications: Melbourne, Australia, 2006. [Google Scholar]
- Robitaille, L.; Hoffer, L.J. A simple method for plasma total vitamin C analysis suitable for routine clinical laboratory use. Nutr. J. 2016, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Pullar, J.M.; Moran, S.; Vissers, M.C. Bioavailability of vitamin C from kiwifruit in non-smoking males: Determination of ‘healthy’ and ‘optimal’ intakes. J. Nutr. Sci. 2012, 1, e14. [Google Scholar] [CrossRef]
- Buss, H.; Chan, T.P.; Sluis, K.B.; Domigan, N.M.; Winterbourn, C.C. Protein carbonyl measurement by a sensitive ELISA method. Free Radic. Biol. Med. 1997, 23, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.D.; Jacobsen, P.B.; Blanchard, C.M.; Thors, C. Further validation of the multidimensional fatigue symptom inventory-short form. J. Pain Symptom Manag. 2004, 27, 14–23. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Ponce, M.C.; Sankari, A.; Sharma, S. Pulmonary Function Tests. StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Ministry of Health. A Focus on Nutrition: Key Findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011; p. 359. [Google Scholar]
- Pearson, J.F.; Pullar, J.M.; Wilson, R.; Spittlehouse, J.K.; Vissers, M.C.M.; Skidmore, P.M.L.; Willis, J.; Cameron, V.A.; Carr, A.C. Vitamin C status correlates with markers of metabolic and cognitive health in 50-year-olds: Findings of the CHALICE cohort study. Nutrients 2017, 9, 831. [Google Scholar] [CrossRef]
- Carr, A.C.; Lykkesfeldt, J. Factors affecting the vitamin C dose-concentration relationship: Implications for global vitamin C dietary recommendations. Nutrients 2023, 15, 19. [Google Scholar] [CrossRef]
- The Lancet Gastroenterology, H. Obesity: Another ongoing pandemic. Lancet Gastroenterol. Hepatol. 2021, 6, 411. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef]
- Phung, D.T.; Wang, Z.; Rutherford, S.; Huang, C.; Chu, C. Body mass index and risk of pneumonia: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 839–857. [Google Scholar] [CrossRef] [PubMed]
- Dobner, J.; Kaser, S. Body mass index and the risk of infection-from underweight to obesity. Clin. Microbiol. Infect. 2018, 24, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.S.; Chang, Y.C.; Chang, C.H.; Wu, L.C.; Wang, J.L.; Lin, H.H. The Association Between Body Mass Index and the Risk of Hospitalization and Mortality due to Infection: A Prospective Cohort Study. Open Forum Infect. Dis. 2021, 8, ofaa545. [Google Scholar] [CrossRef] [PubMed]
- Bozonet, S.M.; Carr, A.C.; Pullar, J.M.; Vissers, M.C.M. Enhanced human neutrophil vitamin C status, chemotaxis and oxidant generation following dietary supplementation with vitamin C-rich SunGold kiwifruit. Nutrients 2015, 7, 2574–2588. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Bozonet, S.M.; Pullar, J.M.; Vissers, M.C. Mood improvement in young adult males following supplementation with gold kiwifruit, a high vitamin C food. J. Nutr. Sci. 2013, 2, 24. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, B.D.; Haszard, J.J.; Vissers, M.C.M.; Conner, T.S. Smartphone survey data reveal the timecourse of changes in mood outcomes following vitamin C or kiwifruit intervention in adults with low vitamin C. Br. J. Nutr. 2023, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Billows, M.; Kakoschke, N.; Zajac, I.T. The role of kiwifruit in supporting psychological well-being: A rapid review of the literature. Nutrients 2022, 14, 4657. [Google Scholar] [CrossRef]
- The Concise New Zealand Food Composition Tables, 8th ed.; New Zealand Institute for Plant & Food Research Ltd.: Palmerston North, New Zealand, 2009; p. 186.
- Tanaka, K.; Hashimoto, T.; Tokumaru, S.; Iguchi, H.; Kojo, S. Interactions between vitamin C and vitamin E are observed in tissues of inherently scorbutic rats. J. Nutr. 1997, 127, 2060–2064. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef]
- Lykkesfeldt, J. On the effect of vitamin C intake on human health: How to (mis)interprete the clinical evidence. Redox Biol. 2020, 34, 101532. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter N (%) | Total Cohort (n = 20) | Variable Median (IQR) | Total Cohort (n = 20) |
|---|---|---|---|
| Sex: | Age, years | 71 (67, 79) | |
| Female | 13 (65) | NZDep index | 5 (2.3, 6.8) |
| Male | 7 (35) | Weight, kg | 65 (59, 78) |
| Ethnicity: | BMI, kg/m2 | 25 (21, 29) | |
| NZ/European | 18 (90) | FEV1, L | 1.5 (1.0, 1.9) |
| Māori | 3 (15) | % predicted | 61 (46, 90) |
| Smoking status: | FVC, L | 2.4 (2.0, 3.1) | |
| Never smoked | 17 (85) | % predicted | 91 (73, 103) |
| Former smoker | 2 (10) | FEV1/FVC ratio | 0.6 (0.4, 0.8) |
| Current smoker | 1 (5) | Recent hospital visits, % | |
| Respiratory conditions: | <1/y:~1/y:>1/y IV Ab duration, days | 35:40:25 14 (5, 14) | |
| History of pneumonia Bronchiectasis COPD | 12 (60) 19 (95) 6 (30) | ||
| Comorbidities: | |||
| Coronary artery disease Asthma Depression | 6 (30) 6 (30) 3 (15) |
| Weeks 1–6 (2 Kiwifruit/Day) | Weeks 11–16 (No Kiwifruit) | |||||
|---|---|---|---|---|---|---|
| Symptom | Number of Participants | Duration of Symptoms | Severity of Symptoms | Number of Participants | Duration of Symptoms | Severity of Symptoms |
| Individual symptoms: | ||||||
| Runny nose | 9 | 3.0 (2.0, 16) | 2.3 (2.2, 3.5) | 9 | 6.0 (4.0, 12) | 2.5 (1.3, 3.0) |
| Plugged nose | 6 | 3.0 (2.0, 7.5) | 1.4 (1.0, 2.6) | 8 | 5.5 (3.3, 9.5) | 2.7 (1.3, 2.8) |
| Sneezing | 8 | 5.0 (2.0, 13) | 2.2 (1.2, 2.8) | 9 | 6.0 (3.0, 10) | 1.7 (1.4, 2.5) |
| Sore throat | 8 | 4.5 (1.3, 11) | 1.8 (1.0, 2.8) | 10 | 4.5 (1.8, 9.5) | 2.7 (2.0, 3.0) |
| Scratchy throat | 8 | 5.5 (1.3, 11) | 1.9 (1.2, 3.9) | 10 | 4.0 (2.8, 8.0) | 2.3 (2.0, 2.5) |
| Cough | 10 | 4.5 (2.0, 21) | 4.3 (2.5, 5.3) | 11 | 10 (3.0, 11) | 2.7 (1.8, 3.0) * |
| Hoarseness | 6 | 9.0 (2.0, 23) | 3.4 (2.6, 5.1) | 10 | 6.0 (2.8, 11) | 2.7 (1.7, 2.9) |
| Head congestion | 9 | 6.0 (2.0, 18) | 2.8 (1.7, 3.9) | 8 | 8.0 (5.5, 11) | 2.2 (1.5, 2.7) |
| Chest congestion | 9 | 4.0 (2.0, 16) | 4.0 (2.7, 5.7) | 10 | 7.5 (3.8, 11) | 2.6 (2.2, 3.3) |
| Feeling tired | 10 | 4.5 (2.0, 20) | 3.5 (2.2, 6.1) | 11 | 9.0 (3.0, 12) | 3.0 (2.3, 4.0) |
| Median symptoms | 8.5 (7.5, 9.3) | 3.3 (1.8, 14) | 3.0 (1.7, 3.8) | 10 (8.8, 10) * | 7.3 (3.0, 10) | 2.4 (2.1, 2.8) |
| Total symptoms | 10 of 19 | 5.0 (2.8, 22) | 21 (10, 33) | 11 of 18 | 10 (4.0, 12) | 21 (10, 22) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlasiuk, E.; Zawari, M.; Storer, M.; Maze, M.J.; Williman, J.; Chambers, S.T.; Carr, A.C. SunGold Kiwifruit Consumption Restores Adequate to Optimal Vitamin C Status in People with a History of Severe Respiratory Infections. Antioxidants 2024, 13, 272. https://doi.org/10.3390/antiox13030272
Vlasiuk E, Zawari M, Storer M, Maze MJ, Williman J, Chambers ST, Carr AC. SunGold Kiwifruit Consumption Restores Adequate to Optimal Vitamin C Status in People with a History of Severe Respiratory Infections. Antioxidants. 2024; 13(3):272. https://doi.org/10.3390/antiox13030272
Chicago/Turabian StyleVlasiuk, Emma, Masuma Zawari, Malina Storer, Michael J. Maze, Jonathan Williman, Stephen T. Chambers, and Anitra C. Carr. 2024. "SunGold Kiwifruit Consumption Restores Adequate to Optimal Vitamin C Status in People with a History of Severe Respiratory Infections" Antioxidants 13, no. 3: 272. https://doi.org/10.3390/antiox13030272
APA StyleVlasiuk, E., Zawari, M., Storer, M., Maze, M. J., Williman, J., Chambers, S. T., & Carr, A. C. (2024). SunGold Kiwifruit Consumption Restores Adequate to Optimal Vitamin C Status in People with a History of Severe Respiratory Infections. Antioxidants, 13(3), 272. https://doi.org/10.3390/antiox13030272