Associations between Lifestyle Factors and Vitamin E Metabolites in the General Population

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Design
2.2. Lifestyle Factors
2.3. Other Variables
2.4. Serum and Urinary Vitamin E Metabolites
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
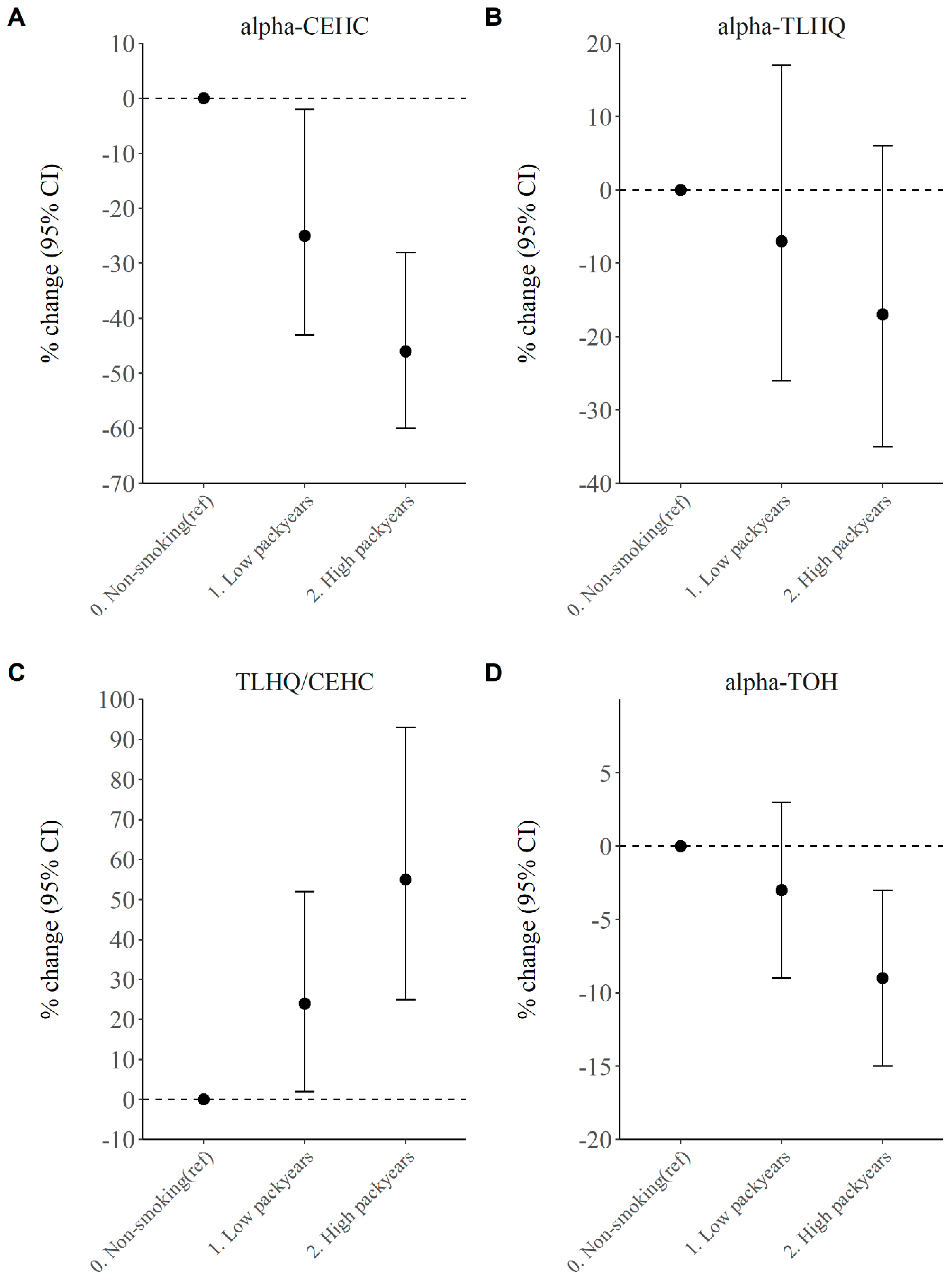
3.2. Association between Smoking (Intensity) and Vitamin E (Metabolite) Levels in Serum and Urine
3.3. Diet Quality and Vitamin E Serum and Urinary Levels
3.4. Sleep Quality and Vitamin E Serum and Urinary Levels
3.5. Physical Activity and Vitamin E Serum and Urinary Levels
3.6. Alcohol Consumption and Vitamin E Serum and Urinary Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res. Rev. 2020, 57, 100982. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohe, R.; Traber, M.G. Vitamin E: Function and metabolism. FASEB J. 1999, 13, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Schmolz, L.; Birringer, M.; Lorkowski, S.; Wallert, M. Complexity of vitamin E metabolism. World J. Biol. Chem. 2016, 7, 14–43. [Google Scholar] [CrossRef] [PubMed]
- Torquato, P.; Bartolini, D.; Giusepponi, D.; Piroddi, M.; Sebastiani, B.; Saluti, G.; Galarini, R.; Galli, F. Increased plasma levels of the lipoperoxyl radical-derived vitamin E metabolite alpha-tocopheryl quinone are an early indicator of lipotoxicity in fatty liver subjects. Free Radic. Biol. Med. 2019, 131, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.E.; Lawson, K.A.; Weinstein, S.J.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Higher baseline serum concentrations of vitamin E are associated with lower total and cause-specific mortality in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Am. J. Clin. Nutr. 2006, 84, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Li, F.J.; Shen, L.; Ji, H.F. Dietary intakes of vitamin E, vitamin C, and beta-carotene and risk of Alzheimer’s disease: A meta-analysis. J. Alzheimer’s Dis. 2012, 31, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Giovannucci, E.; Coldotz, G.A.; Willet, W.C. Vitamin E consumption and the risk of coronary heart disease in men. N. Engl. J. Med. 1993, 328, 1450–1456. [Google Scholar] [CrossRef] [Green Version]
- Brewer, G.J. Why vitamin E therapy fails for treatment of Alzheimer’s disease. J. Alzheimer’s Dis. 2010, 19, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Steinhubl, S.R. Why have antioxidants failed in clinical trials? Am. J. Cardiol. 2008, 101, 14D–19D. [Google Scholar] [CrossRef]
- Wang, L.; Sesso, H.D.; Glynn, R.J.; Christen, W.G.; Bubes, V.; Manson, J.E.; Buring, J.E.; Gaziano, J.M. Vitamin E and C supplementation and risk of cancer in men: Posttrial follow-up in the Physicians’ Health Study II randomized trial. Am. J. Clin. Nutr. 2014, 100, 915–923. [Google Scholar] [CrossRef] [Green Version]
- Klein, E.A.; Thompson, I.M., Jr.; Tangen, C.M.; Crowley, J.J.; Lucia, M.S.; Goodman, P.J.; Minasian, L.M.; Ford, L.G.; Parnes, H.L.; Gaziano, J.M.; et al. Vitamin E and the risk of prostate cancer: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2011, 306, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Farina, N.; Llewellyn, D.; Isaac, M.G.E.K.N.; Tabet, N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2017, 4, CD002854. [Google Scholar] [PubMed]
- Miller, E.R., 3rd; Pastor-Barriuso, R.; Riemersma, R.A.; Appel, L.J.; Guallar, E. Meta-analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann. Intern. Med. 2005, 142, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. JAMA 2007, 297, 842–857. [Google Scholar] [CrossRef]
- Myung, S.K.; Ju, W.; Cho, B.; Oh, S.W.; Park, S.M.; Koo, B.K.; Park, B.J. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: Systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 346, f10. [Google Scholar] [CrossRef] [Green Version]
- Lebold, K.M.; Ang, A.; Traber, M.G.; Arab, L. Urinary alpha-carboxyethyl hydroxychroman can be used as a predictor of alpha-tocopherol adequacy, as demonstrated in the Energetics Study. Am. J. Clin. Nutr. 2012, 96, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [Green Version]
- Ruitenberg, A.; van Swieten, J.C.; Witteman, J.C.M.; Mehta, K.M.; van Duijn, C.M.; Hofman, A.; Breteler, M.M.B. Alcohol consumption and risk of dementia: The Rotterdam Study. Lancet 2002, 359, 281–286. [Google Scholar] [CrossRef]
- Inoue-Choi, M.; Liao, L.M.; Reyes-Guzman, C.; Hartge, P.; Caporaso, N.; Freedman, N.D. Association of Long-term, Low-Intensity Smoking With All-Cause and Cause-Specific Mortality in the National Institutes of Health-AARP Diet and Health Study. JAMA Intern. Med. 2017, 177, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, D.J.; Redline, S.; Nieto, F.J.; Baldwin, C.M.; Newman, A.B.; Resnick, H.E.; Punjabi, N.M. Association of usual sleep duration with hypertension: The Sleep Heart Health Study. Sleep 2006, 29, 1009–1014. [Google Scholar] [CrossRef]
- Will, J.C.; Galuska, D.A.; Ford, E.S.; Mokdad, A.; Calle, E.E. Cigarette smoking and diabetes mellitus: Evidence of a positive association from a large prospective cohort study. Int. J. Epidemiol. 2001, 30, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.; Hwang, S.H.; Choi, H.; Kim, H. The association between smoking or passive smoking and cardiovascular diseases using a Bayesian hierarchical model: Based on the 2008–2013 Korea Community Health Survey. Epidemiol. Health 2017, 39, e2017026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Basyigit, I.; Yildiz, F.; Cekmen, M.; Duman, C.; Bulut, O. Effects of erdosteine on smoking-induced lipid peroxidation in healthy smokers. Drugs R D 2005, 6, 83–89. [Google Scholar] [CrossRef]
- Barranco-Ruiz, Y.; Martínez-Amat, A.; Casals, C.; Aragón-Vela, J.; Rosillo, S.; Gomes, S.N.; Rivas-García, A.; Guisado, R.; Huertas, J.R. A lifelong competitive training practice attenuates age-related lipid peroxidation. J. Physiol. Biochem. 2017, 73, 37–48. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Gamaldo, A.A.; Canas, J.A.; Beydoun, H.A.; Shah, M.T.; McNeely, J.M.; Zonderman, A.B. Serum Nutritional Biomarkers and Their Associations with Sleep among US Adults in Recent National Surveys. PLoS ONE 2014, 9, e103490. [Google Scholar] [CrossRef] [Green Version]
- Evans, W.J. Vitamin E, vitamin C, and exercise. Am. J. Clin. Nutr. 2000, 72, 647–652. [Google Scholar] [CrossRef]
- Bjorklund, G.; Chirumbolo, S. Role of oxidative stress and antioxidants in daily nutrition and human health. Nutrition 2017, 33, 311–321. [Google Scholar] [CrossRef]
- De Mutsert, R.; den Heijer, M.; Rabelink, T.J.; Smit, J.W.A.; Romijn, J.A.; Jukema, J.W.; de Roos, A.; Cobbaert, C.M.; Kloppenburg, M.; le Cessie, S.; et al. The Netherlands Epidemiology of Obesity (NEO) study: Study design and data collection. Eur. J. Epidemiol. 2013, 28, 513–523. [Google Scholar] [CrossRef]
- Evans, A.; Bridgewater, B.R.; Liu, Q.; Mitchell, M.W.; Robinson, R.J.; Dai, H.; Stewart, S.J.; DeHaven, C.D.; Millar, L.A.D. High resolution mass spectrometry improves data quantity and quality as compared to unit mass resolution mass spectrometry in high-throughput profiling metabolomics. Metabolomics 2014, 4, 1. [Google Scholar]
- Rhee, E.P.; Waikar, S.S.; Rebholz, C.M.; Zheng, Z.; Perichon, R.; Clish, C.B.; Evans, A.M.; Avila, J.; Denburg, M.R.; Anderson, A.H.; et al. Variability of Two Metabolomic Platforms in CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Looman, M.; Feskens, E.J.; de Rijk, M.; Meijboom, S.; Biesbroek, S.; Temme, E.T.; de Vries, J.; Geelen, A. Development and evaluation of the Dutch Healthy Diet index 2015. Public Health Nutr. 2017, 20, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.M.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Sharma, G.; Muller, D.P.; O’Riordan, S.M.; Bryan, S.; Dattani, M.T.; Hindmarsh, P.C.; Mills, K. Urinary conjugated alpha-tocopheronolactone—A biomarker of oxidative stress in children with type 1 diabetes. Free Radic. Biol. Med. 2013, 55, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Muller, D.P.; O’Riordan, S.M.; Bryan, S.; Hindmarsh, P.C.; Dattani, M.T.; Mills, K. A novel method for the direct measurement of urinary conjugated metabolites of alpha-tocopherol and its use in diabetes. Mol. Nutr. Food Res. 2010, 54, 599–600. [Google Scholar] [CrossRef]
- Karademirci, M.; Kutlu, R.; Kilinc, I. Relationship between smoking and total antioxidant status, total oxidant status, oxidative stress index, vit C, vit E. Clin. Respir. J. 2018, 12, 2006–2012. [Google Scholar] [CrossRef]
- Kosecik, M.; Erel, O.; Sevinc, E.; Selek, S. Increased oxidative stress in children exposed to passive smoking. Int. J. Cardiol. 2005, 100, 61–64. [Google Scholar] [CrossRef]
- Lourenco, M.A.M.; Braz, M.G.; Aun, A.G.; Pereira, B.L.B.; Fernandes, F.H.; Kazmarek, E.M.; Bachiega, T.F.; Zanati, S.G.; Azevedo, P.S.; Polegato, B.F.; et al. Lipid damage is the best marker of oxidative injury during the cardiac remodeling process induced by tobacco smoke. BMC Pharmacol. Toxicol. 2018, 19, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villafuerte, G.; Miguel-Piga, A.; Rodríguez, E.M.; Machado, S.; Manjarrez, E.; Arias-Carrión, O. Sleep deprivation and oxidative stress in animal models: A systematic review. Oxid. Med. Cell. Longev. 2015, 2015, 234952. [Google Scholar] [CrossRef] [PubMed]
- Alzoubi, K.H.; Khabour, O.F.; Rashid, B.A.; Damaj, I.M.; Salah, H.A. The neuroprotective effect of vitamin E on chronic sleep deprivation-induced memory impairment: The role of oxidative stress. Behav. Brain Res. 2012, 226, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Mayas, M.D.; Ramírez-Expósito, M.J.; Garciá, M.J.; Ramírez, M.; Martínez-Martos, J.M. Ethanol modifies differently aspartyl- and glutamyl-aminopeptidase activities in mouse frontal cortex synaptosomes. Brain Res. Bull. 2002, 57, 195–203. [Google Scholar] [CrossRef]


{kind=link}
| All (N = 530) | Men (N = 246) | Women (N = 284) | |
|---|---|---|---|
| Demography | 55.9 (6.0) | - | - |
| Sex, % men | 46.4 | - | - |
| Age (years), mean (sd) | 55.9 (6.0) | 56.2 (6.2) | 55.6 (5.8) |
| Lifestyle factors | - | - | - |
| BMI (kg/m2), mean (sd) | 25.9 (4.0) | 26.6 (3.3) | 25.4 (4.4) |
| Smoking, N (%) | - | - | - |
| Never | 216 (40.8) | 92 (37.4) | 124 (43.7) |
| Former | 255 (48.1) | 124 (50.4) | 131 (46.1) |
| Current | 59 (11.1) | 30 (12.2) | 29 (10.2) |
| Pack years 1, median (IQR) | 18.1 (8.4, 29.8) | 26.6 (14.0, 36.4) | 13.3 (4.7, 22.7) |
| Alcohol use (g/day), median (IQR) | 9.2 (2.5, 21.5) | 16.7 (5.1, 28.4) | 7.2 (1.0, 14.4) |
| Leisure activity (MET-h), median (IQR) | 30.0 (16.5, 49.6) | 30.0 (16.0, 50.0) | 29.9 (16.5, 47.8) |
| Poor Sleep Quality, N (%) | 205 (38.7) | 76 (30.9) | 129 (45.4) |
| Diet Quality (0–130), mean (sd) | 72.0 (14.6) | 68.4 (13.4) | 75.2 (14.9) |
| Lipid lowering drugs, N (%) | 38 (7.2) | 25 (10.2) | 13 (4.6) |
| Vitamin E metabolites | - | - | - |
| Measurements, median (IQR) | - | - | - |
| α-THLQ (nmol/mmol creatinine) | 1832 (1337, 2745) | 1519 (1194, 2256) | 2091.6 (1470, 3074) |
| α-CEHC (nmol/mmol creatinine) | 265 (180, 439) | 223 (137, 352) | 307 (213, 508) |
| α-TLHQ/α-CEHC | 2.0 (1.6, 2.3) | 2.0 (1.7, 2.4) | 2.0 (1.6, 2.3) |
| α-TOH | 3.5 × 108 (3.2 × 108, 3.9 × 108) | 3.5 × 108 (3.2 × 108, 3.8 × 108) | 3.5 × 108 (3.1 × 108, 3.9 × 108) |
| Lifestyle Factors | α -TOH | Total TLHQ | Total CEHC | Ratio TLHQ/CEHC | |||||
|---|---|---|---|---|---|---|---|---|---|
| N = | % Change | 95% CI | % Change | 95% CI | % Change | 95% CI | % Change | 95% CI | |
| Smoking | - | - | - | - | - | - | - | - | - |
| Nonsmokers | 216 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Former smokers | 255 | −1 | −4 to 2 | 4 | −6 to 15 | 2 | −10 to 15 | 2 | −7 to 12 |
| Current smokers | 59 | −4 | −8 to 0 | −11 | −24 to 5 | −32 | −44 to −18 | 32 | 14 to 53 |
| DHDI | - | - | - | - | - | - | - | - | - |
| 25.4–61.5 | 132 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 61.9–72.5 | 133 | −2 | −3 to 4 | 0 | −13 to 15 | 6 | −10 to 25 | −7 | −18 to 4 |
| 72.5–81.5 | 133 | 1 | −2 to 5 | 13 | −2 to 29 | 6 | −10 to 25 | 5 | −7 to 18 |
| 81.6–117.8 | 132 | 3 | −1 to 7 | 12 | −3 to 29 | 10 | −7 to 31 | −1 | −13 to 12 |
| Sleep Quality | - | - | - | - | - | - | - | - | - |
| Good Quality | 288 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Poor Quality | 205 | 3 | 1 to 6 | 0 | −10 to 10 | -0 | −12 to 13 | 1 | −9 to 9 |
| PA in MET-h/wk | |||||||||
| 0.0–16.3 | 129 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 16.5–29.8 | 130 | 1 | −2 to 5 | −7 | −18 to 7 | 11 | −5 to 31 | −17 | −26 to −6 |
| 30.0–49.5 | 132 | −1 | −4 to 3 | −11 | −22 to 2 | 0 | −14 to 18 | −12 | −22 to −1 |
| 49.8–242.5 | 130 | −2 | −6 to 1 | −5 | −17 to 14 | 4 | −11 to 23 | −9 | −19 to 3 |
| Alcohol use in g/day | |||||||||
| 0–2.49 | 132 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| 2.5–9.2 | 133 | −2 | −5 to 2 | −8 | −19 to 6 | −1 | −16 to 16 | −8 | −18 to 4 |
| 9.2–21.5 | 133 | −0 | −3 to 4 | −9 | −21 to 4 | 2 | −14 to 20 | −12 | −22 to 0 |
| 21.5–171.6 | 132 | 3 | −1 to 7 | −17 | −28 to 4 | −4 | −20 to 14 | −13 | −24 to −1 |
| Cotinine Metabolite | α -TOH | Total TLHQ | Total CEHC | Ratio TLHQ/CEHC | |||||
|---|---|---|---|---|---|---|---|---|---|
| N = | % Change | 95% CI | % Change | 95% CI | % Change | 95% CI | % Change | 95% CI | |
| Cotinine | - | - | - | - | - | - | - | - | - |
| Absent | 412 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Present | 118 | 2 | −2 to 5 | −11 | −21 to −1 | −20 | −30 to −8 | 11 | 0 to 23 |
| Cotinine levels | - | - | - | - | - | - | - | - | - |
| Absent | 412 | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Low | 59 | 5 | 0 to 10 | −6 | −19 to 10 | −11 | −26 to 7 | 6 | −7 to 21 |
| High | 59 | −2 | −6 to 3 | −16 | −29 to −3 | −28 | −40 to −14 | 16 | 1 to 33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martens, L.G.; Luo, J.; Meulmeester, F.L.; Ashrafi, N.; van Eekelen, E.W.; de Mutsert, R.; Mook-Kanamori, D.O.; Rosendaal, F.R.; van Dijk, K.W.; Mills, K.; et al. Associations between Lifestyle Factors and Vitamin E Metabolites in the General Population. Antioxidants 2020, 9, 1280. https://doi.org/10.3390/antiox9121280
Martens LG, Luo J, Meulmeester FL, Ashrafi N, van Eekelen EW, de Mutsert R, Mook-Kanamori DO, Rosendaal FR, van Dijk KW, Mills K, et al. Associations between Lifestyle Factors and Vitamin E Metabolites in the General Population. Antioxidants. 2020; 9(12):1280. https://doi.org/10.3390/antiox9121280
Chicago/Turabian StyleMartens, Leon G., Jiao Luo, Fleur L. Meulmeester, Nadia Ashrafi, Esther Winters van Eekelen, Renée de Mutsert, Dennis O. Mook-Kanamori, Frits R. Rosendaal, Ko Willems van Dijk, Kevin Mills, and et al. 2020. "Associations between Lifestyle Factors and Vitamin E Metabolites in the General Population" Antioxidants 9, no. 12: 1280. https://doi.org/10.3390/antiox9121280
APA StyleMartens, L. G., Luo, J., Meulmeester, F. L., Ashrafi, N., van Eekelen, E. W., de Mutsert, R., Mook-Kanamori, D. O., Rosendaal, F. R., van Dijk, K. W., Mills, K., Noordam, R., & van Heemst, D. (2020). Associations between Lifestyle Factors and Vitamin E Metabolites in the General Population. Antioxidants, 9(12), 1280. https://doi.org/10.3390/antiox9121280