Acute Diarrhea in Dogs: Current Management and Potential Role of Dietary Polyphenols Supplementation

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Traditional Therapeutic and Nutritional Management
2.1. Rehydration Therapy and Electrolytes Replacement
2.2. Dietary Interventions
2.3. Complementary Feeds
2.4. Antibacterial Drugs
2.5. Miscellaneous
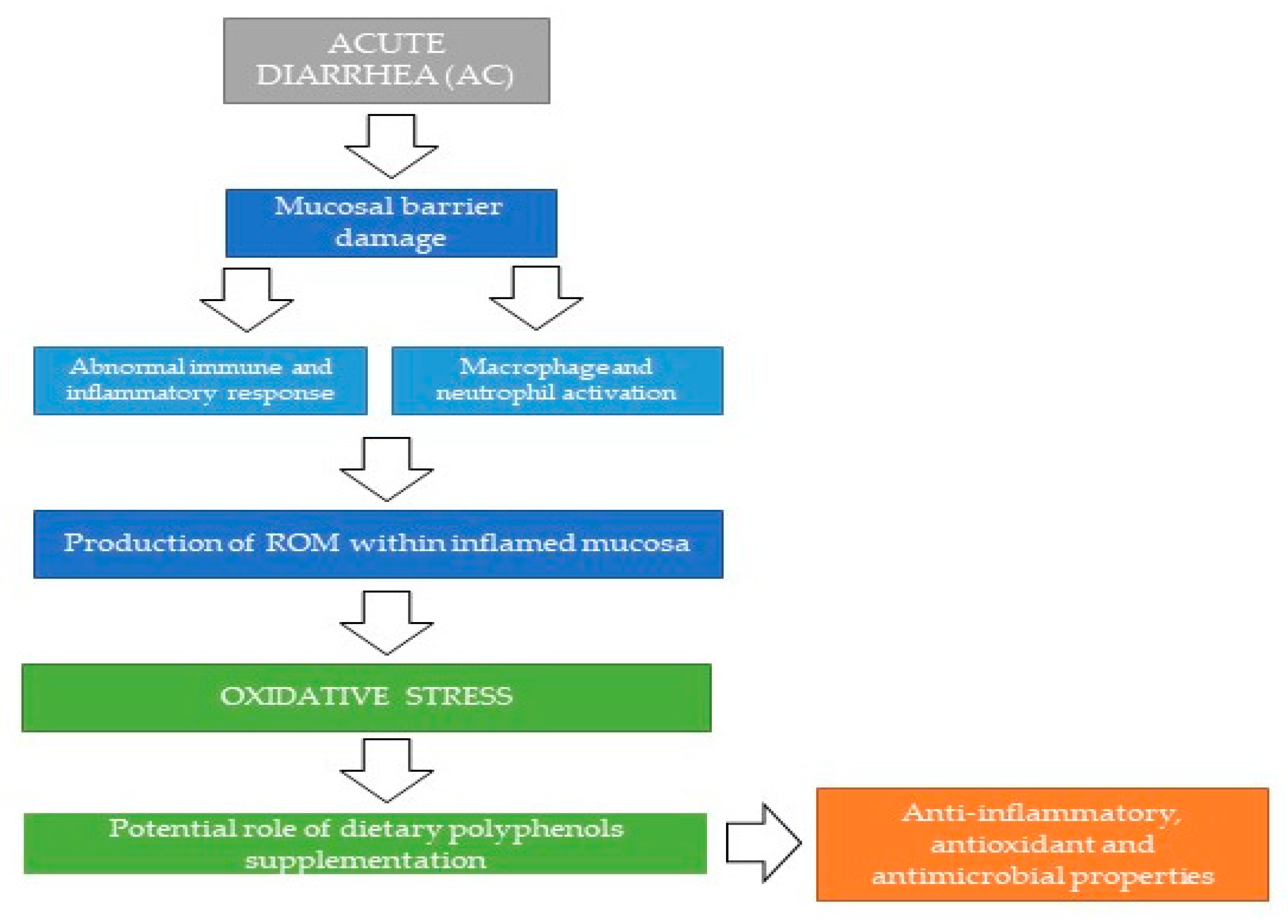
3. Oxidative Stress in Course of AD and Polyphenols Supplementation as a Potential Additional Support Option
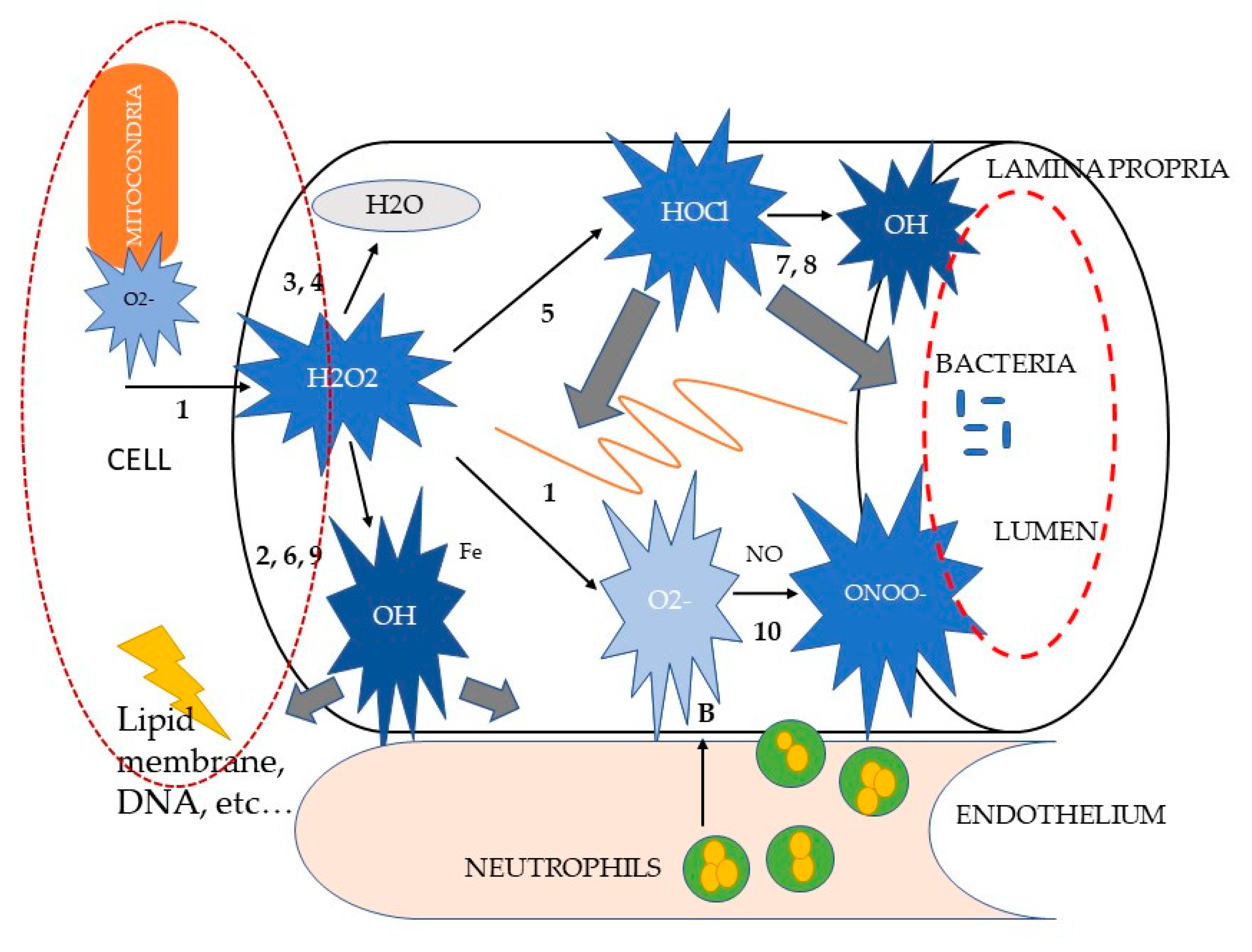
3.1. Mechanisms of Oxidative Stress-Induced Damage
3.2. Role of Polyphenols Supplementation in Course of Intestinal Inflammation
4. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
References
- Hubbard, K.; Skelly, B.J.; McKelvie, J.; Wood, J.L.N. Risk of vomiting and diarrhoea in dogs. Veter. Rec. 2007, 161, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Guarino, A.; Vecchio, A.L.; Dias, J.A.; Berkley, J.A.; Boey, C.; Bruzzese, D.; Cohen, M.B.; Cruchet, S.; Liguoro, I.; Salazar-Lindo, E.; et al. Universal Recommendations for the Management of Acute Diarrhea in Nonmalnourished Children. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 586–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandt, K.G.; Castro Antunes, M.M.; Da Silva, G.A.P. Acute diarrhea: Evidence-based management. J. Pediatr. 2015, 91 (Suppl. S1), S36–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Franco, F.; Sainz-Rodríguez, A. Enfermedades del intestino delgado. In Manual de Gastroenterología Clínica en Pequenos Animales, 1st ed.; Rodríguez-Franco, F., Ed.; Grupo ASIS Biomedia S.L: Zaragoza, Spain, 2018; pp. 123–125. [Google Scholar]
- Langlois, D.K.; Koenigshof, A.M.; Mani, R. Metronidazole treatment of acute diarrhea in dogs: A randomized double blinded placebo-controlled clinical trial. J. Vet. Intern. Med. 2020, 34, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Singleton, D.A.; Noble, P.J.M.; Sánchez-Vizcaíno, F.; Dawson, S.; Pinchbeck, G.L.; Williams, N.J.; Radford, A.D.; Jones, P.H. Pharmaceutical Prescription in Canine Acute Diarrhoea: A Longitudinal Electronic Health Record Analysis of First Opinion Veterinary Practices. Front. Vet. Sci. 2019, 6, 218. [Google Scholar] [CrossRef]
- Willard, M.D. Digestive System Disorders. In Small Animal Internal Medicine, 5th ed.; Nelson, R.W., Couto, C.G., Eds.; Elsevier: St. Louis, MO, USA, 2014; pp. 376–380. [Google Scholar]
- Hall, E.J.; German, A.E. Diseases of the small intestine. In Textbook of Veterinary Internal Medicine, 7th ed.; Ettinger, S.J., Feldman, E.C., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2010; pp. 1544–1546. [Google Scholar]
- Berset-Istratescu, C.M.; Glardon, O.J.; Magouras, I.; Frey, C.F.; Gobeli, S.; Burgener, I. Follow-up of 100 dogs with acute diarrhoea in a primary care practice. Vet. J. 2014, 199, 188–190. [Google Scholar] [CrossRef]
- Werner, M.; Suchodolski, J.S.; Straubinger, R.K.; Wolf, G.; Steiner, J.M.; Lidbury, J.; Neuerer, F.; Hartmann, K.; Unterer, S. Effect of amoxicillin-clavulanic acid on clinical scores, intestinal microbiome, and amoxicillin-resistant Escherichia coli in dogs with uncomplicated acute diarrhea. J. Vet. Intern. Med. 2020, 34, 1166–1176. [Google Scholar] [CrossRef] [Green Version]
- Mantegazza, C.; Molinari, P.; D’Auria, E.; Sonnino, M.; Morelli, L.; Zuccotti, G.V. Probiotics and antibiotic-associated diarrhea in children: A review and new evidence on Lactobacillus rhamnosus GG during and after antibiotic treatment. Pharmacol. Res. 2017, 128, 63–72. [Google Scholar] [CrossRef]
- Walker, C.L.F.; Perin, J.; Aryee, M.J.; Boschi-Pinto, C.; Black, R.E. Diarrhea incidence in low- and middle-income countries in 1990 and 2010: A systematic review. BMC Public Health 2012, 12, 220. [Google Scholar] [CrossRef] [Green Version]
- Da Crus Gouveia, M.A.; Lins, M.T.C.; da Silva, G.A.P. Acute diarrhea with blood: Diagnosis and drug treatment. J. Pediatr. 2020, 96 (Suppl. S1), 20–28. [Google Scholar] [CrossRef]
- Kumar, S.; Pandey, A. Chemistry and Biological Activities of Flavonoids: An Overview. Sci. World J. 2013, 2013, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betts, J.W.; Hornsey, M.; La Ragione, R.M. Novel Antibacterials: Alternatives to Traditional Antibiotics. Adv. Microb. Physiol. 2018, 73, 123–169. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Jiang, Y.; Zhang, B.; Yang, H.; Ma, T. Resveratrol dimer trans-ε -viniferin prevents rotaviral diarrhea in mice by inhibition of the intestinal calcium-activated chloride channel. Pharmacol. Res. 2018, 129, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Denev, P.; Číž, M.; Kratchanova, M.; Blazheva, D. Black chokeberry (Aronia melanocarpa) polyphenols reveal different antioxidant, antimicrobial and neutrophil-modulating activities. Food Chem. 2019, 284, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Parisella, F.R.; Perez, A. Alternatives to antibiotics in an era of difficult-to-treat resistance: New insights. Expert Rev. Clin. Pharmacol. 2019, 12, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Roudsari, N.M.; Lashgari, N.-A.; Momtaz, S.; Farzaei, M.H.; Marques, A.M.; Abdolghaffari, A.H. Natural polyphenols for the prevention of irritable bowel syndrome: Molecular mechanisms and targets; a comprehensive review. DARU J. Pharm. Sci. 2019, 27, 755–780. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Mazzola, M.; Leone, A.; Sinagra, E.; Zummo, G.; Farina, F.; Damiani, P.; Cappello, F.; Geagea, A.G.; Jurjus, A.; et al. Nutrition, oxidative stress and intestinal dysbiosis: Influence of diet on gut microbiota in inflammatory bowel diseases. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2016, 160, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Robles, H.; Castro-Ochoa, K.F.; Citalán-Madrid, A.F.; Schnoor, M. Beneficial effects of nutritional supplements on intestinal epithelial barrier functions in experimental colitis models in vivo. World J. Gastroenterol. 2019, 25, 4181–4198. [Google Scholar] [CrossRef]
- Lee, S.H. Intestinal Permeability Regulation by Tight Junction: Implication on Inflammatory Bowel Diseases. Intest. Res. 2015, 13, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.J.; Mayer, L. The Immune Response in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2007, 102, 2058–2069. [Google Scholar] [CrossRef]
- Romier, B.; Schneider, Y.-J.; Larondelle, Y.; During, A. Dietary polyphenols can modulate the intestinal inflammatory response. Nutr. Rev. 2009, 67, 363–378. [Google Scholar] [CrossRef] [PubMed]
- Ozdal, T.; Sela, D.A.; Ulrih, N.P.; Boyacioglu, D.; Chen, F.; Capanoglu, E. The Reciprocal Interactions between Polyphenols and Gut Microbiota and Effects on Bioaccessibility. Nutrients 2016, 8, 78. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.K.N.; Samson, S.E.; Grover, A. Antioxidant Supplements and Gastrointestinal Diseases: A Critical Appraisal. Med. Princ. Pr. 2017, 26, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Nunes, S.; Danesi, F.; Del Rio, D.; Silva, P. Resveratrol and inflammatory bowel disease: The evidence so far. Nutr. Res. Rev. 2017, 31, 85–97. [Google Scholar] [CrossRef]
- Gil-Cardoso, K.; Comitato, R.; Ginés, I.; Ardèvol, A.; Pinent, M.; Virgili, F.; Terra, X.; Blay, M. Protective Effect of Proanthocyanidins in a Rat Model of Mild Intestinal Inflammation and Impaired Intestinal Permeability Induced by LPS. Mol. Nutr. Food Res. 2019, 63, e1800720. [Google Scholar] [CrossRef]
- Cerquetella, M.; Spaterna, A.; Laus, F.; Tesei, B.; Rossi, G.; Antonelli, E.; Villanacci, V.; Bassotti, G. Inflammatory bowel disease in the dog: Differences and similarities with humans. World J. Gastroenterol. 2010, 16, 1050–1056. [Google Scholar] [CrossRef]
- Cerquetella, M.; Rossi, G.; Suchodolski, J.S.; Schmitz, S.S.; Allenspach, K.; Rodríguez-Franco, F.; Furlanello, T.; Gavazza, A.; Marchegiani, A.; Unterer, S.; et al. Proposal for rational antibacterial use in the diagnosis and treatment of dogs with chronic diarrhoea. J. Small Anim. Pr. 2020, 61, 211–215. [Google Scholar] [CrossRef]
- Subbiah, M.; Caudell, M.; Mair, C.; Davis, M.A.; Matthews, L.; Quinlan, R.J.; Quinlan, M.B.; Lyimo, B.; Buza, J.; Keyyu, J.; et al. Antimicrobial resistant enteric bacteria are widely distributed amongst people, animals and the environment in Tanzania. Nat. Commun. 2020, 11, 228. [Google Scholar] [CrossRef] [Green Version]
- Ossiprandi, M.C.; Bottarelli, E.; Cattabiani, F.; Bianchi, E. Susceptibility to vancomycin and other antibiotics of 165 Enterococcus strains isolated from dogs in Italy. Comp. Immunol. Microbiol. Infect. Dis. 2008, 31, 1–9. [Google Scholar] [CrossRef]
- Teixeira, I.M.; de Oliveira Ferreira, E.; de Araujo Penna, B. Dogs as reservoir of methicillin resistant coagulase negative staphylococci strains—A possible neglected risk. Microb. Pathog. 2019, 135, 103616. [Google Scholar] [CrossRef]
- Desforges, J.F.; Avery, M.E.; Snyder, J.D. Oral Therapy for Acute Diarrhea: The Underused Simple Solution. N. Engl. J. Med. 1990, 323, 891–894. [Google Scholar] [CrossRef] [PubMed]
- Davenport, D.J.; Remillard, R.L. Acute Gastroenteritis and Enteritis. In Small Animal Clinical Nutrition, 5th ed.; Hand, M.S., Thatcher, C.D., Remillard, R.L., Eds.; Mark Morris Ins.: Topeka, KS, USA, 2010; pp. 1053–1064. [Google Scholar]
- Zenger, E.; Willard, M.D. Oral rehydration therapy in companion animals. Compan. Anim. Pract. 1989, 19, 6–10. [Google Scholar]
- Mortier, F.; Strohmeyer, K.; Hartmann, K.; Unterer, S. Acute haemorrhagic diarrhoea syndrome in dogs: 108 cases. Vet. Rec. 2015, 176, 627. [Google Scholar] [CrossRef] [PubMed]
- Tenne, R.; Sullivan, L.A.; Contreras, E.T.; Olea-Popelka, F.; Twedt, D.C.; Fankhauser, J.; Mastrianna, L.; Lappin, M.R. Palatability and Clinical Effects of an Oral Recuperation Fluid During the Recovery of Dogs With Suspected Parvoviral Enteritis. Top. Companion Anim. Med. 2016, 31, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.D.; Vigani, A. Maintenance Fluid Therapy: Isotonic Versus Hypotonic Solutions. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 383–395. [Google Scholar] [CrossRef]
- Cave, N.J. Nutritional Management of Gastrointestinal Diseases. In Applied Veterinary Clinical Nutrition, 1st ed.; Fascetti, A.J., Delaney, S.J., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 175–186. [Google Scholar]
- Guilford, W.G.; Strombeck, D.R.; Rogers, Q.; Frick, O.L.; Lawoko, C. Development of Gastroscopic Food Sensitivity Testing in Dogs. J. Vet. Intern. Med. 1994, 8, 414–422. [Google Scholar] [CrossRef]
- Will, K.; Nolte, I.; Zentek, J. Early Enteral Nutrition in Young Dogs Suffering from Haemorrhagic Gastroenteritis. J. Vet. Med. Ser. A 2005, 52, 371–376. [Google Scholar] [CrossRef]
- Mohr, A.J.; Leisewitz, A.L.; Jacobson, L.S.; Steiner, J.M.; Ruaux, C.G.; Williams, D.A. Effect of early enteral nutrition on intestinal permeability, intestinal protein loss, and outcome in dogs with severe parvoviral enteritis. J. Vet. Int. Med. 2003, 17, 791–798. [Google Scholar] [CrossRef]
- Zhou, Q.; Verne, M.L.; Fields, J.Z.; Lefante, J.J.; Basra, S.; Salameh, H.; Verne, G.N. Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut 2019, 68, 996–1002. [Google Scholar] [CrossRef]
- Lenders, C.M.; Liu, S.; Wilmore, D.W.; Sampson, L.; Dougherty, L.W.; Spiegelman, D.; Willett, W.C. Evaluation of a novel food composition database that includes glutamine and other amino acids derived from gene sequencing data. Eur. J. Clin. Nutr. 2009, 63, 1433–1439. [Google Scholar] [CrossRef]
- Rossi, G.; Cerquetella, M.; Gavazza, A.; Galosi, L.; Berardi, S.; Mangiaterra, S.; Mari, S.; Suchodolski, J.S.; Lidbury, J.; Steiner, J.M.; et al. Rapid Resolution of Large Bowel Diarrhea after the Administration of a Combination of a High-Fiber Diet and a Probiotic Mixture in 30 Dogs. Vet. Sci. 2020, 7, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilla, R.; Suchodolski, J.S. The Role of the Canine Gut Microbiome and Metabolome in Health and Gastrointestinal Disease. Front. Vet. Sci. 2020, 6, 498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, R.L.; Minikhiem, D.; Kiely, B.; O’Mahony, L.; O’Sullivan, D.; Boileau, T.; Park, J.S. Clinical benefits of probiotic canine-derived Bifidobacterium animalis strain AHC7 in dogs with acute idiopathic diarrhea. Vet. Ther. Res. Appl. Vet. Med. 2009, 10, 121–130. [Google Scholar]
- Herstad, H.K.; Nesheim, B.B.; L’Abée-Lund, T.; Larsen, S.; Skancke, E. Effects of a probiotic intervention in acute canine gastroenteritis – a controlled clinical trial. J. Small Anim. Pract. 2010, 51, 34–38. [Google Scholar] [CrossRef]
- Gómez-Gallego, C.; Junnila, J.; Männikkö, S.; Hämeenoja, P.; Valtonen, E.; Salminen, S.; Beasley, S. A canine-specific probiotic product in treating acute or intermittent diarrhea in dogs: A double-blind placebo-controlled efficacy study. Vet. Microbiol. 2016, 197, 122–128. [Google Scholar] [CrossRef]
- Ziese, A.-L.; Suchodolski, J.S.; Hartmann, K.; Busch, K.; Anderson, A.; Sarwar, F.; Sindern, N.; Unterer, S. Effect of probiotic treatment on the clinical course, intestinal microbiome, and toxigenic Clostridium perfringens in dogs with acute hemorrhagic diarrhea. PLoS ONE 2018, 13, e0204691. [Google Scholar] [CrossRef]
- Shmalberg, J.; Montalbano, C.; Morelli, G.; Buckley, G.J. A Randomized Double Blinded Placebo-Controlled Clinical Trial of a Probiotic or Metronidazole for Acute Canine Diarrhea. Front. Vet. Sci. 2019, 6, 163. [Google Scholar] [CrossRef] [Green Version]
- Jensen, A.P.; Bjornvad, C.R. Clinical effect of probiotics in prevention or treatment of gastrointestinal disease in dogs: A systematic review. J. Vet. Intern. Med. 2019, 33, 1849–1864. [Google Scholar] [CrossRef]
- Unterer, S.; Strohmeyer, K.; Kruse, B.; Sauter-Louis, C.; Hartmann, K. Treatment of Aseptic Dogs with Hemorrhagic Gastroenteritis with Amoxicillin/Clavulanic Acid: A Prospective Blinded Study. J. Vet. Intern. Med. 2011, 25, 973–979. [Google Scholar] [CrossRef]
- Unterer, S.; Lechner, E.; Mueller, R.S.; Wolf, G.; Straubinger, R.; Schulz, B.S.; Hartmann, K. Prospective study of bacteraemia in acute haemorrhagic diarrhoea syndrome in dogs. Vet. Rec. 2015, 176, 309. [Google Scholar] [CrossRef]
- Alves, F.; Prata, S.; Nunes, T.; Gomes, J.; Aguiar, S.; Da Silva, F.A.; Tavares, L.; Almeida, V.; A Gil, S. Canine parvovirus: A predicting canine model for sepsis. BMC Vet. Res. 2020, 16, 199. [Google Scholar] [CrossRef] [PubMed]
- Manchester, A.; Webb, C.B.; Blake, A.B.; Sarwar, F.; Lidbury, J.; Steiner, J.M.; Suchodolski, J.S. Long-term impact of tylosin on fecal microbiota and fecal bile acids of healthy dogs. J. Vet. Intern. Med. 2019, 33, 2605–2617. [Google Scholar] [CrossRef] [PubMed]
- Guard, B.C.; Barr, J.W.; Reddivari, L.; Klemashevich, C.; Jayaraman, A.; Steiner, J.M.; Vanamala, J.; Suchodolski, J.S. Characterization of Microbial Dysbiosis and Metabolomic Changes in Dogs with Acute Diarrhea. PLoS ONE 2015, 10, e0127259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, P.; Curtis, N. The effect of antibiotics on the composition of the intestinal microbiota—A systematic review. J. Infect. 2019, 79, 471–489. [Google Scholar] [CrossRef]
- Pereira, G.Q.; Gomes, L.A.; Santos, I.S.; Alfieri, A.F.; Weese, J.S.; Costa, M.C. Fecal microbiota transplantation in puppies with canine parvovirus infection. J. Vet. Intern. Med. 2018, 32, 707–711. [Google Scholar] [CrossRef]
- Chaitman, J.; Ziese, A.-L.; Pilla, R.; Minamoto, Y.; Blake, A.B.; Guard, B.C.; Isaiah, A.; Lidbury, J.A.; Steiner, J.M.; Unterer, S.; et al. Fecal Microbial and Metabolic Profiles in Dogs with Acute Diarrhea Receiving Either Fecal Microbiota Transplantation or Oral Metronidazole. Front. Vet. Sci. 2020, 7. [Google Scholar] [CrossRef]
- Romier, B.; Van De Walle, J.; During, A.; Larondelle, Y.; Schneider, Y.-J. Modulation of signalling nuclear factor-κB activation pathway by polyphenols in human intestinal Caco-2 cells. Br. J. Nutr. 2008, 100, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Salim, S.; Söderholm, J.D. Importance of disrupted intestinal barrier in inflammatory bowel diseases. Inflamm. Bowel Dis. 2011, 17, 362–381. [Google Scholar] [CrossRef]
- Ramanan, D.; Cadwell, K. Intrinsic Defense Mechanisms of the Intestinal Epithelium. Cell Host Microbe 2016, 19, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Kühl, A.A.; Erben, U.; Kredel, L.I.; Siegmund, B. Diversity of Intestinal Macrophages in Inflammatory Bowel Diseases. Front. Immunol. 2015, 6, 613. [Google Scholar] [CrossRef] [Green Version]
- Kruidenier, L.; Verspaget, H.W. Review article: Oxidative stress as a pathogenic factor in inflammatory bowel disease--radicals or ridiculous? Aliment. Pharmacol. Ther. 2002, 16, 1997–2015. [Google Scholar] [CrossRef] [PubMed]
- Richter, C.; Schweizer, M. Oxidative stress in mitochondria. In Oxidative Stress and the Molecular Biology of Antioxidant Defenses, 1st ed.; Scandalios, J.G., Ed.; Cold Spring Harbor: Plainview, NY, USA, 1997; pp. 169–200. [Google Scholar]
- Ma, T.Y.; Hollander, D.; Freeman, D.; Nguyen, T.; Krugliak, P. Oxygen free radical injury of IEC-18 small intestinal epithelial cell monolayers. Gastroenterology 1991, 100, 1533–1543. [Google Scholar] [CrossRef]
- Baker, S.S.; Campbell, C.L. Rat enterocyte injury by oxygen-dependent processes. Gastroenterology 1991, 101, 716–720. [Google Scholar] [CrossRef]
- Mulier, B.; Rahman, I.; Watchorn, T.; Donaldson, K.; MacNee, W.; Jeffery, P.K. Hydrogen peroxide-induced epithelial injury: The protective role of intracellular nonprotein thiols (NPSH). Eur. Respir. J. 1998, 11, 384–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehrer, J.P. The Haber–Weiss reaction and mechanisms of toxicity. Toxicology 2000, 149, 43–50. [Google Scholar] [CrossRef]
- He, J.; Xu, L.; Yang, L.; Wang, X. Epigallocatechin Gallate Is the Most Effective Catechin Against Antioxidant Stress via Hydrogen Peroxide and Radical Scavenging Activity. Med. Sci. Monit. 2018, 24, 8198–8206. [Google Scholar] [CrossRef]
- Liso, M.; De Santis, S.; Scarano, A.; Verna, G.; Dicarlo, M.; Vanessa, G.; Campiglia, P.; Mastronardi, M.; Lippolis, A.; Vacca, M.; et al. A Bronze-Tomato Enriched Diet Affects the Intestinal Microbiome under Homeostatic and Inflammatory Conditions. Nutrients 2018, 10, 1862. [Google Scholar] [CrossRef] [Green Version]
- Castangia, I.; Nácher, A.; Caddeo, C.; Merino, V.; Diez-Sales, O.; Catalan-Latorre, A.; Fernàndez-Busquets, X.; Fadda, A.M.; Manconi, M. Therapeutic efficacy of quercetin enzyme-responsive nanovesicles for the treatment of experimental colitis in rats. Acta Biomater. 2015, 13, 216–227. [Google Scholar] [CrossRef]
- Hong, Z.; Piao, M. Effect of Quercetin Monoglycosides on Oxidative Stress and Gut Microbiota Diversity in Mice with Dextran Sodium Sulphate-Induced Colitis. BioMed Res. Int. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Dicarlo, M.; Teti, G.; Verna, G.; Liso, M.; Cavalcanti, E.; Sila, A.; Raveenthiraraj, S.; Mastronardi, M.; Santino, A.; Serino, G.; et al. Quercetin Exposure Suppresses the Inflammatory Pathway in Intestinal Organoids from Winnie Mice. Int. J. Mol. Sci. 2019, 20, 5771. [Google Scholar] [CrossRef] [Green Version]
- Stan, M.S.; Voicu, S.N.P.; Caruntu, S.; Nica, I.C.; Olah, N.-K.; Burtescu, R.; Balta, C.; Roșu, M.; Herman, H.; Hermenean, A.; et al. Antioxidant and Anti-Inflammatory Properties of a Thuja occidentalis Mother Tincture for the Treatment of Ulcerative Colitis. Antioxidants 2019, 8, 416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergent, T.; Piront, N.; Meurice, J.; Toussaint, O.; Schneider, Y.-J. Anti-inflammatory effects of dietary phenolic compounds in an in vitro model of inflamed human intestinal epithelium. Chem. Biol. Interact. 2010, 188, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.R.; Villegas, I.; Sánchez-Hidalgo, M.; de la Lastra, C.A. The effects of resveratrol, a phytoalexin derived from red wines, on chronic inflammation induced in an experimentally induced colitis model. Br. J. Pharmacol. 2006, 147, 873–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minamoto, Y.; Otoni, C.C.; Steelman, S.M.; Büyükleblebici, O.; Steiner, J.M.; Jergens, A.E.; Suchodolski, J.S. Alteration of the fecal microbiota and serum metabolite profiles in dogs with idiopathic inflammatory bowel disease. Gut Microbes 2015, 6, 33–47. [Google Scholar] [CrossRef] [Green Version]
- Zannoni, A.; Pietra, M.; Gaspardo, A.; Accorsi, P.A.; Barone, M.; Turroni, S.; Laghi, L.; Zhu, C.; Brigidi, P.; Forni, M. Non-invasive Assessment of Fecal Stress Biomarkers in Hunting Dogs During Exercise and at Rest. Front. Vet. Sci. 2020, 7, 126. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Wan, S.B.; Yang, H.; Yuan, J.; Chan, T.H.; Dou, Q.P. EGCG, green tea polyphenols and their synthetic analogs and prodrugs for human cancer prevention and treatment. Adv. Clin. Chem. 2011, 53, 155–177. [Google Scholar] [CrossRef] [Green Version]
- Weng, C.-J.; Yen, G.-C. Chemopreventive effects of dietary phytochemicals against cancer invasion and metastasis: Phenolic acids, monophenol, polyphenol, and their derivatives. Cancer Treat. Rev. 2012, 38, 76–87. [Google Scholar] [CrossRef]
- Liu, L.; Zubik, L.; Collins, F.; Marko, M.; Meydani, M. The antiatherogenic potential of oat phenolic compounds. Atherosclerosis 2004, 175, 39–49. [Google Scholar] [CrossRef]
- Kuriyama, S.; Shimazu, T.; Ohmori, K.; Kikuchi, N.; Nakaya, N.; Nishino, Y.; Tsubono, Y.; Tsuji, I. Green Tea Consumption and Mortality Due to Cardiovascular Disease, Cancer, and All Causes in Japan. JAMA 2006, 296, 1255–1265. [Google Scholar] [CrossRef]
- Zakaria, Z.; Hisam, E.A.; Rofiee, M.; Norhafizah, M.; Somchit, M.; Teh, L.; Salleh, M.; Somchit, N. In vivo antiulcer activity of the aqueous extract of Bauhinia purpurea leaf. J. Ethnopharmacol. 2011, 137, 1047–1054. [Google Scholar] [CrossRef]
- Han, N.; Gu, Y.; Ye, C.; Cao, Y.; Liu, Z.; Yin, J. Antithrombotic activity of fractions and components obtained from raspberry leaves (Rubus chingii). Food Chem. 2012, 132, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.-W.; Duan, J.-A.; Yang, N.-Y.; Tang, Y.-P.; Liu, M.-Z.; Qian, Y.-F. Antithrombotic phenolic compounds from Glycyrrhiza uralensis. Fitoterapia 2012, 83, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Beara, I.; Lesjak, M.; Orčić, D.; Simin, N.; Četojević-Simin, D.D.; Bozin, B.; Mimica-Dukic, N. Comparative analysis of phenolic profile, antioxidant, anti-inflammatory and cytotoxic activity of two closely-related Plantain species: Plantago altissima L. and Plantago lanceolata L. LWT Food Sci. Technol. 2012, 47, 64–70. [Google Scholar] [CrossRef]
- Zimmer, A.R.; Leonardi, B.; Miron, D.; Schapoval, E.; De Oliveira, J.R.; Gosmann, G. Antioxidant and anti-inflammatory properties of Capsicum baccatum: From traditional use to scientific approach. J. Ethnopharmacol. 2012, 139, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schütz, K.; Saß, M.; De With, A.; Graubaum, H.-J.; Grünwald, J. Immune-modulating efficacy of a polyphenol-rich beverage on symptoms associated with the common cold: A double-blind, randomised, placebo-controlled, multi-centric clinical study. Br. J. Nutr. 2010, 104, 1156–1164. [Google Scholar] [CrossRef]
- Xia, D.; Wu, X.; Shi, J.; Yang, Q.; Zhang, Y. Phenolic compounds from the edible seeds extract of Chinese Mei (Prunus mume Sieb. et Zucc) and their antimicrobial activity. LWT Food Sci. Technol. 2011, 44, 347–349. [Google Scholar] [CrossRef]
- Silva, J.C.; Rodrigues, S.; Feás, X.; Estevinho, L.M.; Estevinho, L.M. Antimicrobial activity, phenolic profile and role in the inflammation of propolis. Food Chem. Toxicol. 2012, 50, 1790–1795. [Google Scholar] [CrossRef]
- Dos Santos, M.D.; Almeida, M.C.; Lopes, N.P.; Souza, G.E. Evaluation of the anti-inflammatory, analgesic and antipyretic activities of the natural polyphenols CGA. Biol. Pharm. Bull. 2006, 29, 2236–2240. [Google Scholar] [CrossRef] [Green Version]
- Selma, M.V.; Espín, J.C.; Tomás-Barberán, F.A. Interaction between Phenolics and Gut Microbiota: Role in Human Health. J. Agric. Food Chem. 2009, 57, 6485–6501. [Google Scholar] [CrossRef]
- Faria, A.; Fernandes, I.; Norberto, S.; Mateus, N.; Calhau, C. Interplay between Anthocyanins and Gut Microbiota. J. Agric. Food Chem. 2014, 62, 6898–6902. [Google Scholar] [CrossRef]
- Cardona, F.; Andres-Lacueva, C.; Tulipani, S.; Tinahones, F.J.; Queipo-Ortuño, M.I. Benefits of polyphenols on gut microbiota and implications in human health. J. Nutr. Biochem. 2012, 24, 1415–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzounis, X.; Vulevic, J.; Kuhnle, G.G.C.; George, T.; Leonczak, J.; Gibson, G.R.; Kwik-Uribe, C.; Spencer, J.P. Flavanol monomer-induced changes to the human faecal microflora. Br. J. Nutr. 2007, 99, 782–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolara, P.; Luceri, C.; De Filippo, C.; Femia, A.P.; Giovannelli, L.; Caderni, G.; Cecchini, C.; Silvi, S.; Orpianesi, C.; Cresci, A. Red wine polyphenols influence carcinogenesis, intestinal microflora, oxidative damage and gene expression profiles of colonic mucosa in F344 rats. Mutat. Res. Mol. Mech. Mutagen. 2005, 591, 237–246. [Google Scholar] [CrossRef] [PubMed]
- De Medina, F.S.; Gálvez, J.; Romero, J.A.; Zarzuelo, A. Effect of quercitrin on acute and chronic experimental colitis in the rat. J. Pharmacol. Exp. Ther. 1996, 278, 771–779. [Google Scholar]
- De Medina, F.S.; Vera, B.; Galvez, J.; Zarzuelo, A. Effect of quercitrin on the early stages of hapten induced colonic inflammation in the rat. Life Sci. 2002, 70, 3097–3108. [Google Scholar] [CrossRef] [Green Version]
- Cibiček, N.; Roubalova, L.; Vrba, J.; Zatloukalová, M.; Ehrmann, J.; Zapletalová, J.; Večeřa, R.; Křen, V.; Ulrichová, J. Protective effect of isoquercitrin against acute dextran sulfate sodium-induced rat colitis depends on the severity of tissue damage. Pharmacol. Rep. 2016, 68, 1197–1204. [Google Scholar] [CrossRef]
- Cavalcanti, E.; Vadrucci, E.; DelVecchio, F.R.; Addabbo, F.; Bettini, S.; Liou, R.; Monsurrò, V.; Huang, A.Y.; Pizarro, T.T.; Santino, A.; et al. Administration of Reconstituted Polyphenol Oil Bodies Efficiently Suppresses Dendritic Cell Inflammatory Pathways and Acute Intestinal Inflammation. PLoS ONE 2014, 9, e88898. [Google Scholar] [CrossRef] [Green Version]
- Cui, Q.; Fu, Q.; Zhao, X.; Song, X.; Yu, J.; Yang, Y.; Sun, K.; Bai, L.; Tian, Y.; Chen, S.; et al. Protective effects and immunomodulation on piglets infected with rotavirus following resveratrol supplementation. PLoS ONE 2018, 13, e0192692. [Google Scholar] [CrossRef] [Green Version]
- Gan, Z.; Wei, W.; Li, Y.; Wu, J.; Zhao, Y.; Zhang, L.; Wang, T.; Zhong, X. Curcumin and Resveratrol Regulate Intestinal Bacteria and Alleviate Intestinal Inflammation in Weaned Piglets. Molecules 2019, 24, 1220. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Garza, S.L.; Laveriano-Santos, E.P.; Marhuenda-Muñoz, M.; Storniolo, C.E.; Tresserra-Rimbau, A.; Vallverdú-Queralt, A.; Lamuela-Raventos, R.M. Health Effects of Resveratrol: Results from Human Intervention Trials. Nutrients 2018, 10, 1892. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Factors | Recommended Levels * |
|---|---|
| Energy density | 4.0–4.5 kcal/g |
| Fat | 12–25% (highly digestible food); 8–12% (increased fiber-food) |
| Fiber | ≤5% in highly digestible food (mixed fiber source preferred); 7–15% in fiber-enhanced food (insoluble or mixed fiber source preferred) |
| Digestibility | ≥87% for protein and ≥90% for fat and carbohydrate (highly digestible food) ≥80% for protein and ≥90% for fat and carbohydrate (fiber-enhanced food) |
| Sodium | 0.3–0.5% |
| Chloride | 0.5–1.3% |
| Potassium | 0.8–1.1% |
| Phenolic Compound | Model | Effect on Gut Microbiota | Reference |
|---|---|---|---|
| tea phenolics (epicatechin, catechin, 3-O-methylgallic acid, gallic acid and caffeic acid) | Culture broth and culture broth with additional 0.1% (w/v) phenolic compounds inoculated with a 5% (v/v) bacterial inoculum and incubated at 37 °C under aerobic and anaerobic conditions | ↓Clostridium perfringens, Clostridium difficile and Bacteroides spp. No effect on Clostridium spp., Bifidobacterium spp. and Lactobacillus spp. | [95,97] |
| proanthocyanidin- rich red wine extracts | rats | ↑Bacteroides, Lactobacillus and Bifidobacterium spp. Bacteroides, ↓Clostridium and Propionibacterium spp. | [96,97] |
| (−)epicatechin and (+)catechin | batch-culture model, reflective of the distal region of the human large intestine | ↑E. coli, Clostridium coccoides–Eubacterium rectale group ↓Clostridium histolyticum No effect on Bifidobacterium and Lactobacillus spp. | [98] |
| Wine polyphenols (4.4% anthocyanins, 0.8% flavonols, 2.0% phenolic acids, 1.4% catechin, 1.0% epicatechin and 28.0% proanthocyanidin units, consisting of 18.0% epigallocatechin, 13.2% catechin, 65.0% epicatechin and 3.8% epicatechin gallate) | F344 rats | ↑Bacteroides, Lactobacillus and Bifidobacterium spp. | [99] |
| Phenolic Compound | In Vivo Model | Effect | Reference |
|---|---|---|---|
| Quercitrin | Rat with trinitrobenzene sulfonic acid-induced colitis. | ↓myeloperoxidase and alkaline phosphatase levels, counteract glutathione depletion, preserve normal fluid absorption and ↓ colonic damage. | [100] |
| Quercitin | Rat with trinitrobenzene sulfonic acid-induced colitis. | downregulate the inflammatory cascade associated with ↓of the disturbances in hydro-electrolytic transport. | [101] |
| Isoquercitin | Rat with acute dextran sulfate sodium (DSS)-induced colitis. | Dose-dependent ↓ of colon shortening and mitigation of DSS-induced expression of cyclooxygenase-2 and inducible nitric oxide synthase in the descending colon; protective effects depend on the site and the severity of tissue damage. | [102] |
| Quercetin + piperine, encapsulated into reconstituted oil bodies (ROBs) | Mice with acute dextran sulfate sodium (DSS)-induced colitis. | ↓ LPS-mediated inflammatory cytokine secretion (IL-6, IL-23, and IL-12); ↑ IL-10 and IL-1Rα production. ↓ weight loss, mortality and inflammatory scores. | [104] |
| Resveratrol alone or with curcumin | Piglets orally challenged with rotavirus (RV). | alleviate RV-induced diarrhea, by ↓TNF-α production; down-regulate the level of Toll-like-receptor 4 mRNA and protein expression in the intestine; ↓ the critical inflammation molecules release, and immunoglobulin secretion. | [105] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candellone, A.; Cerquetella, M.; Girolami, F.; Badino, P.; Odore, R. Acute Diarrhea in Dogs: Current Management and Potential Role of Dietary Polyphenols Supplementation. Antioxidants 2020, 9, 725. https://doi.org/10.3390/antiox9080725
Candellone A, Cerquetella M, Girolami F, Badino P, Odore R. Acute Diarrhea in Dogs: Current Management and Potential Role of Dietary Polyphenols Supplementation. Antioxidants. 2020; 9(8):725. https://doi.org/10.3390/antiox9080725
Chicago/Turabian StyleCandellone, Alessia, Matteo Cerquetella, Flavia Girolami, Paola Badino, and Rosangela Odore. 2020. "Acute Diarrhea in Dogs: Current Management and Potential Role of Dietary Polyphenols Supplementation" Antioxidants 9, no. 8: 725. https://doi.org/10.3390/antiox9080725
APA StyleCandellone, A., Cerquetella, M., Girolami, F., Badino, P., & Odore, R. (2020). Acute Diarrhea in Dogs: Current Management and Potential Role of Dietary Polyphenols Supplementation. Antioxidants, 9(8), 725. https://doi.org/10.3390/antiox9080725