
Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients

 ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
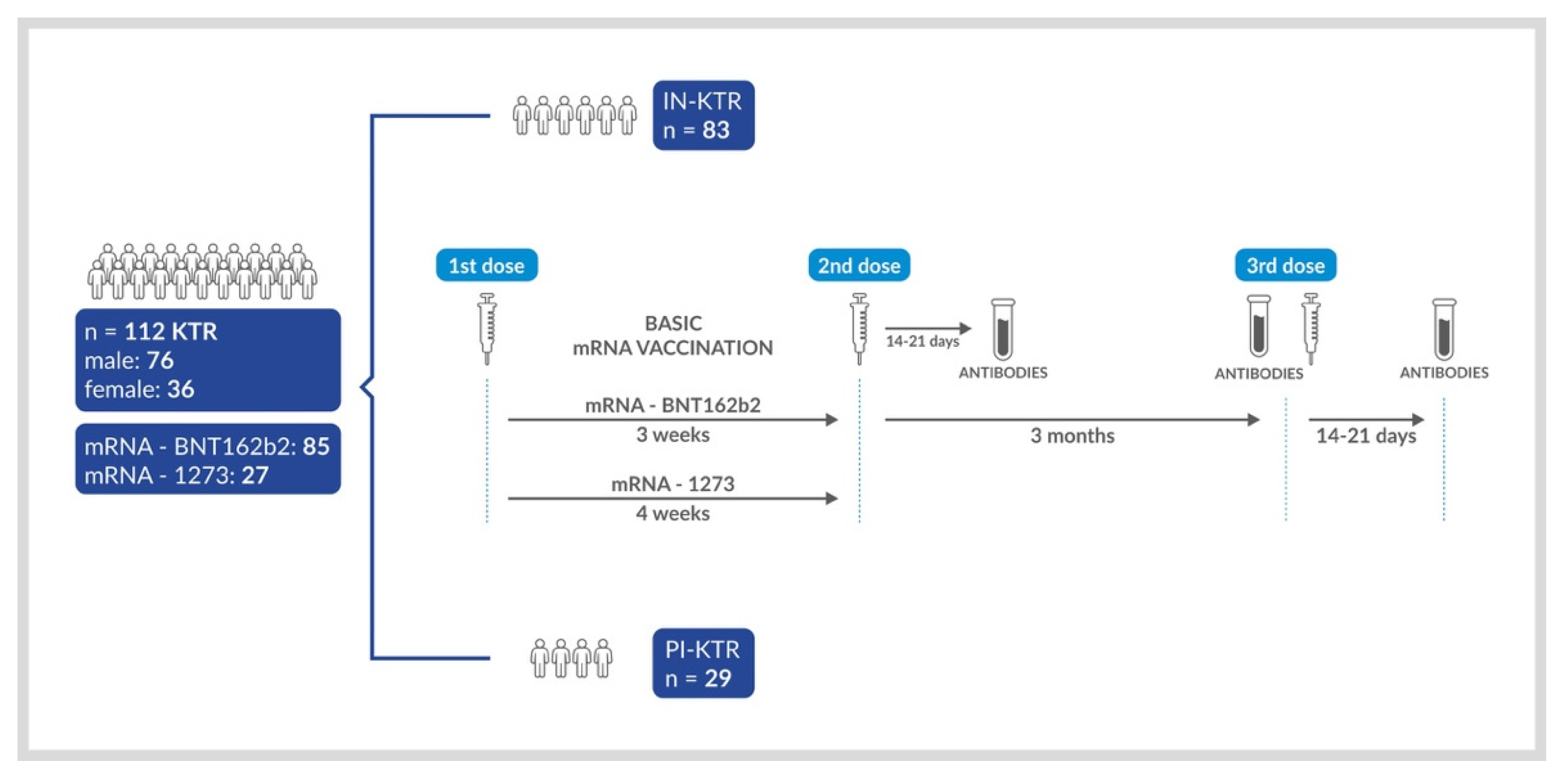
2.1. Study Population
2.2. Study Design
2.3. Procedures and Analytical Methods
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
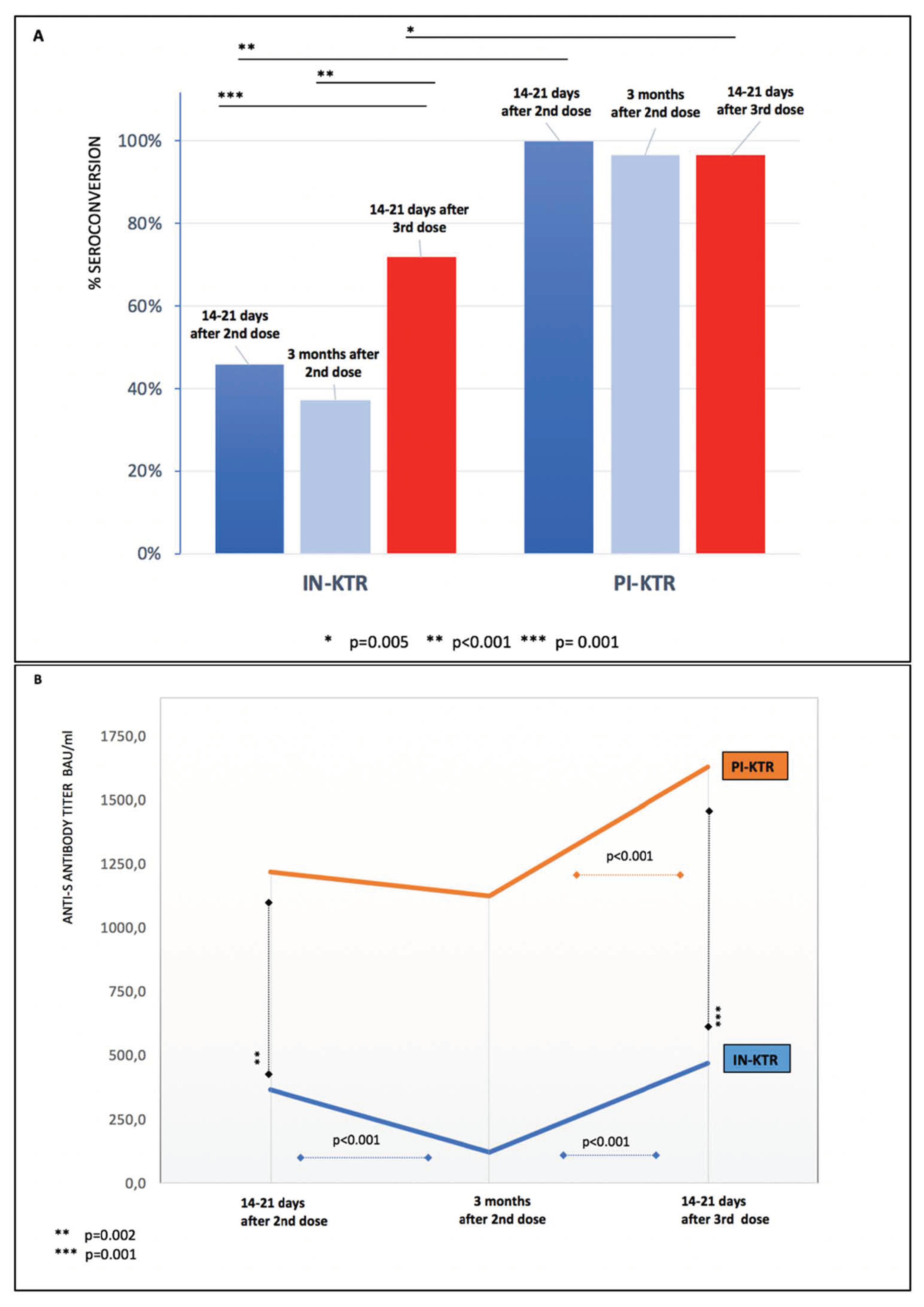
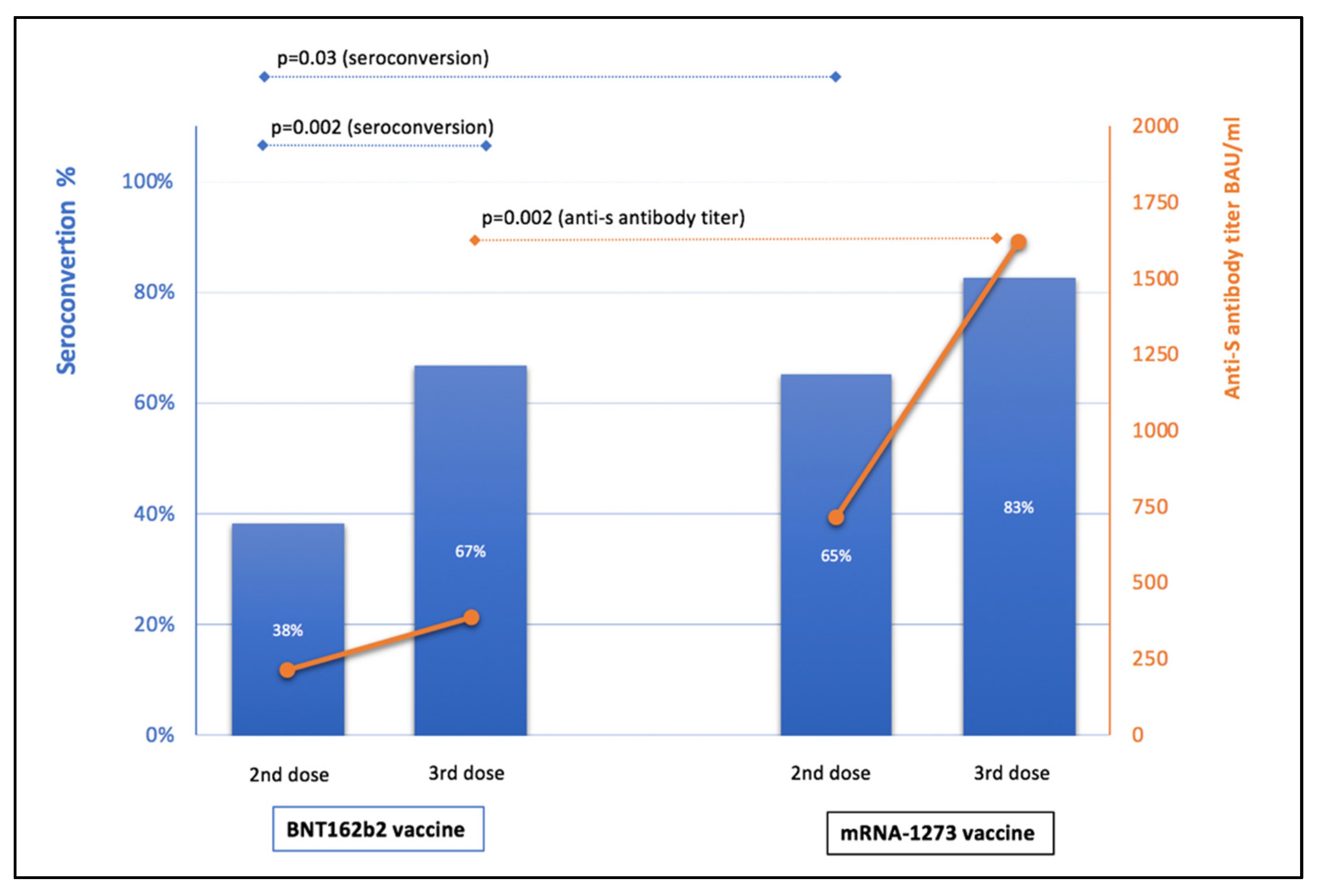
3.2. Anti-S IgG Antibodies before and after the Third mRNA Vaccine Dose
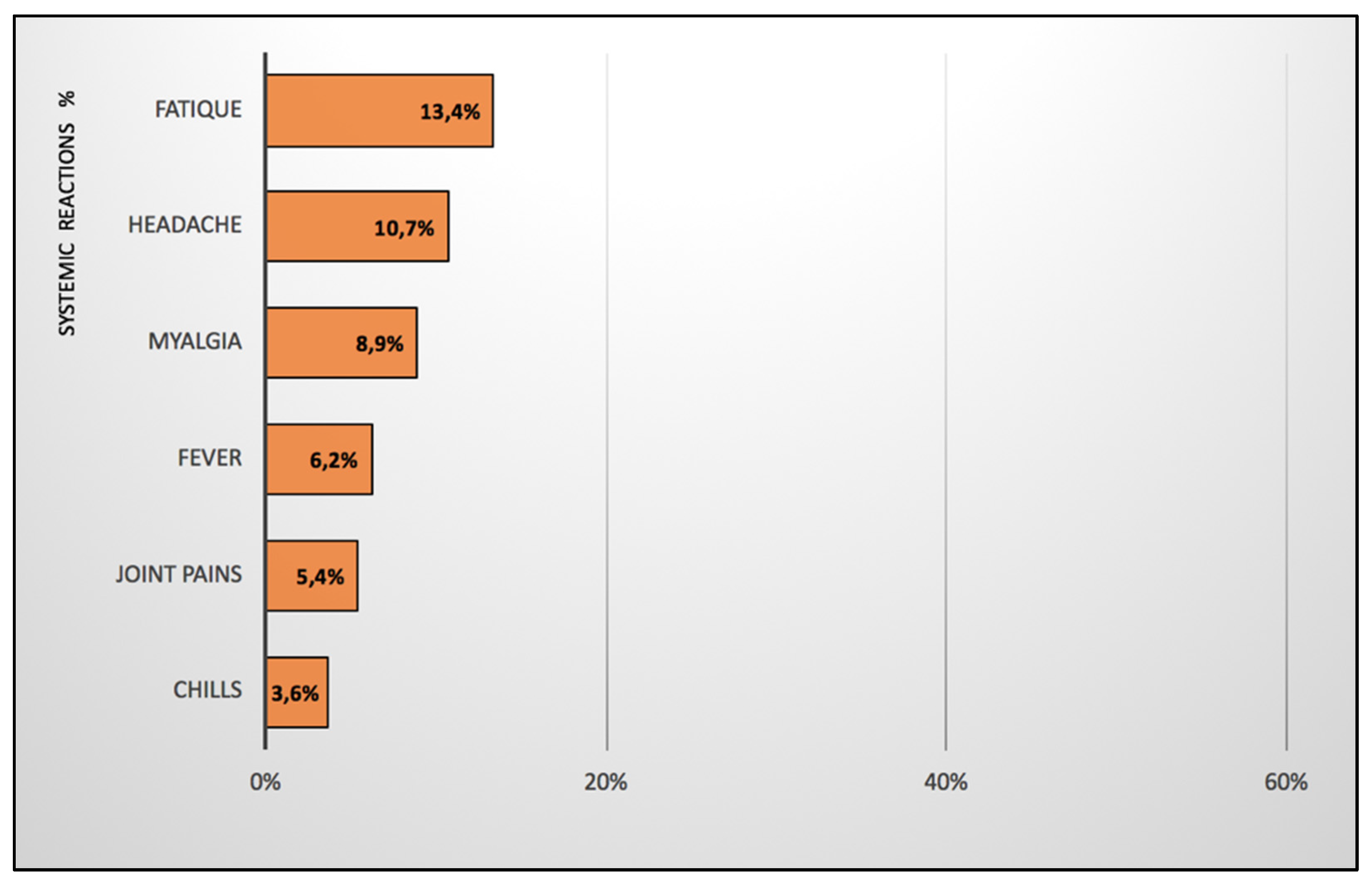
3.3. Reactogenicity to the Third mRNA Vaccine Dose
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P.; et al. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Caillard, S.; Thaunat, O. COVID-19 vaccination in kidney transplant recipients. Nat. Rev. Nephrol. 2021, 17, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Debska-Slizien, A.; Slizien, Z.; Muchlado, M.; Kubanek, A.; Piotrowska, M.; Dabrowska, M.; Tarasewicz, A.; Chamienia, A.; Biedunkiewicz, B.; Renke, M.; et al. Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study-The COViNEPH Project. Vaccines 2021, 9, 1165. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwobel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef] [PubMed]
- Azzi, Y.; Bartash, R.; Scalea, J.; Loarte-Campos, P.; Akalin, E. COVID-19 and Solid Organ Transplantation: A Review Article. Transplantation 2021, 105, 37–55. [Google Scholar] [CrossRef]
- Polewska, K.; Tylicki, P.; Biedunkiewicz, B.; Rucińska, A.; Szydłowska, A.; Kubanek, A.; Rosenberg, I.; Rodak, S.; Ślizień, W.; Renke, M.; et al. Safety and Tolerability of the BNT162b2 mRNA COVID-19 Vaccine in Dialyzed Patients. COViNEPH Project. Medicina 2021, 57, 732. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063–1065. [Google Scholar] [CrossRef]
- Marlet, J.; Gatault, P.; Maakaroun, Z.; Longuet, H.; Stefic, K.; Handala, L.; Eymieux, S.; Gyan, E.; Dartigeas, C.; Gaudy-Graffin, C. Antibody Responses after a Third Dose of COVID-19 Vaccine in Kidney Transplant Recipients and Patients Treated for Chronic Lymphocytic Leukemia. Vaccines 2021, 9, 1055. [Google Scholar] [CrossRef]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. A third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssiere, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transplant. 2021. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination With BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Richards, N.E.; Keshavarz, B.; Workman, L.J.; Nelson, M.R.; Platts-Mills, T.A.E.; Wilson, J.M. Comparison of SARS-CoV-2 Antibody Response by Age Among Recipients of the BNT162b2 vs the mRNA-1273 Vaccine. JAMA Netw. Open 2021, 4, e2124331. [Google Scholar] [CrossRef] [PubMed]
- Buschmann, M.D.; Carrasco, M.J.; Alishetty, S.; Paige, M.; Alameh, M.G.; Weissman, D. Nanomaterial Delivery Systems for mRNA Vaccines. Vaccines 2021, 9, 65. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: Longer interval between Pfizer doses results in higher antibody levels, research finds. BMJ 2021, 374, n1875. [Google Scholar] [CrossRef] [PubMed]
- Pettini, E.; Pastore, G.; Fiorino, F.; Medaglini, D.; Ciabattini, A. Short or Long Interval between Priming and Boosting: Does It Impact on the Vaccine Immunogenicity? Vaccines 2021, 9, 289. [Google Scholar] [CrossRef] [PubMed]
- Firket, L.; Descy, J.; Seidel, L.; Bonvoisin, C.; Bouquegneau, A.; Grosch, S.; Jouret, F.; Weekers, L. Serological response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients depends on prior exposure to SARS-CoV-2. Am. J. Transplant. 2021, 21, 3806–3807. [Google Scholar] [CrossRef]
- Tylicki, L.; Biedunkiewicz, B.; Dąbrowska, M.; Ślizień, W.; Tylicki, P.; Polewska, K.; Rosenberg, I.; Rodak, S.; Dębska-Ślizień, A. Humoral response to SARS-CoV-2 vaccination promises to improve the catastrophic prognosis of hemodialysis patients as a result of COVID-19. The COViNEPH Project. Pol. Arch. Intern. Med. 2021, 131, 797–801. [Google Scholar] [CrossRef]
- Dębska-Ślizień, A.; Muchlado, M.; Ślizień, Z.; Kubanek, A.; Biedunkiewicz, B.; Tylicki, L. Significant humoral response to mRNA COVID-19 vaccine in kidney transplant recipients with prior exposure to SARS-CoV-2. The COViNEPH Project. Pol. Arch. Intern. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. COVID super-immunity: One of the pandemic’s great puzzles. Nature 2021, 598, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Alejo, J.L.; Mitchell, J.; Chiang, T.P.; Abedon, A.T.; Boyarsky, B.J.; Avery, R.K.; Tobian, A.A.R.; Levan, M.L.; Massie, A.B.; Garonzik-Wang, J.M.; et al. Antibody Response to a Fourth Dose of a SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Transplantation 2021, 105, e280–e281. [Google Scholar] [CrossRef]
- Caillard, S.; Thaunat, O.; Benotmane, I.; Masset, C.; Blancho, G. Antibody response to a fourth mRNA COVID-19 vaccine boost in weak responder kidney transplant recipients. medRxiv 2021. [Google Scholar] [CrossRef]
- Pozzetto, B.; Legros, V.; Djebali, S.; Barateau, V.; Guibert, N.; Villard, M.; Peyrot, L.; Allatif, O.; Fassier, J.B.; Massardier-Pilonchery, A.; et al. Immunogenicity and efficacy of heterologous ChadOx1/BNT162b2 vaccination. Nature 2021, 600, 701–706. [Google Scholar] [CrossRef]
- Ho, T.C.; Chen, Y.A.; Chan, H.P.; Chang, C.C.; Chuang, K.P.; Lee, C.H.; Yuan, C.H.; Tyan, Y.C.; Yang, M.H. The Effects of Heterologous Immunization with Prime-Boost COVID-19 Vaccination against SARS-CoV-2. Vaccines 2021, 9, 1163. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Cohen, C.; Hernan, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KTRs, Total n = 112 | IN-KTR n = 83 | PI-KTR n = 29 | p-Value ** | |
|---|---|---|---|---|
| Age (years) | 54.5 (44.5–63) | 55 (42–63) | 54 (48–61) | 0.95 |
| Male sex Female sex | 76 (67.86) 36 (32.14) | 54 (65.06) 29 (34.94) | 22 (75.86) 7 (24.14) | 0.28 0.28 |
| CCI | 4 (2–6) | 4 (2–6) | 4 (2–6) | 0.74 |
| Serum creatinine (mg/dl) | 1.34 (1.13–1.68) | 1.35 (1.13–1.6) | 1.33 (1.19–1.8) | 0.46 |
| BMI (kg/m2) | 25.9 (22.59–28.96) | 25.98 (22.69–28.96) | 25.43 (22.55–28.37) | 0.71 |
| Transplant duration (years) | 8 (3.5–15) | 8 (3.5–15) | 8 (3.0–15) | 0.81 |
| Deceased donor | 102 (91.07) | 75 (90.36) | 27 (93.1) | 0.66 |
| Immunosuppression protocol Protocol without steroids Protocol without MMF/MPS | 10 (8.93) 26 (23.21) | 9 (10.84) 18 (21.89) | 1 (3.45) 8 (27.59) | 0.23 0.52 |
| mRNA-1273 vaccination | 27 (24.11) | 23 (27.71) | 4 (13.79) | 0.13 |
| mRNA BNT162b2 vaccination | 85 (75.89) | 60 (72.29) | 25 (86.21) | 0.13 |
| Seroconversion after second dose a | 67 (59.82) | 38 (45.78) | 29 (100) | < 0.001 |
| Anti-S antibody titer after second dose a,* | 663.0 (213.2–1560) | 365.3 (117.3–915.2) | 1219.4 (647.4–1978.6) | < 0.001 |
| Anti-S antibody titer 3 months after second dose * | 265.0 (110.0–1040.0) | 119.0 (81.1–265.0) | 1128.0 (380.0–4280) | < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tylicki, L.; Dębska-Ślizień, A.; Muchlado, M.; Ślizień, Z.; Gołębiewska, J.; Dąbrowska, M.; Biedunkiewicz, B. Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients. Vaccines 2022, 10, 56. https://doi.org/10.3390/vaccines10010056
Tylicki L, Dębska-Ślizień A, Muchlado M, Ślizień Z, Gołębiewska J, Dąbrowska M, Biedunkiewicz B. Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients. Vaccines. 2022; 10(1):56. https://doi.org/10.3390/vaccines10010056
Chicago/Turabian StyleTylicki, Leszek, Alicja Dębska-Ślizień, Marta Muchlado, Zuzanna Ślizień, Justyna Gołębiewska, Małgorzata Dąbrowska, and Bogdan Biedunkiewicz. 2022. "Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients" Vaccines 10, no. 1: 56. https://doi.org/10.3390/vaccines10010056
APA StyleTylicki, L., Dębska-Ślizień, A., Muchlado, M., Ślizień, Z., Gołębiewska, J., Dąbrowska, M., & Biedunkiewicz, B. (2022). Boosting Humoral Immunity from mRNA COVID-19 Vaccines in Kidney Transplant Recipients. Vaccines, 10(1), 56. https://doi.org/10.3390/vaccines10010056