
Humoral Response to Hepatitis B and COVID-19 Vaccine among Maintenance Hemodialysis Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
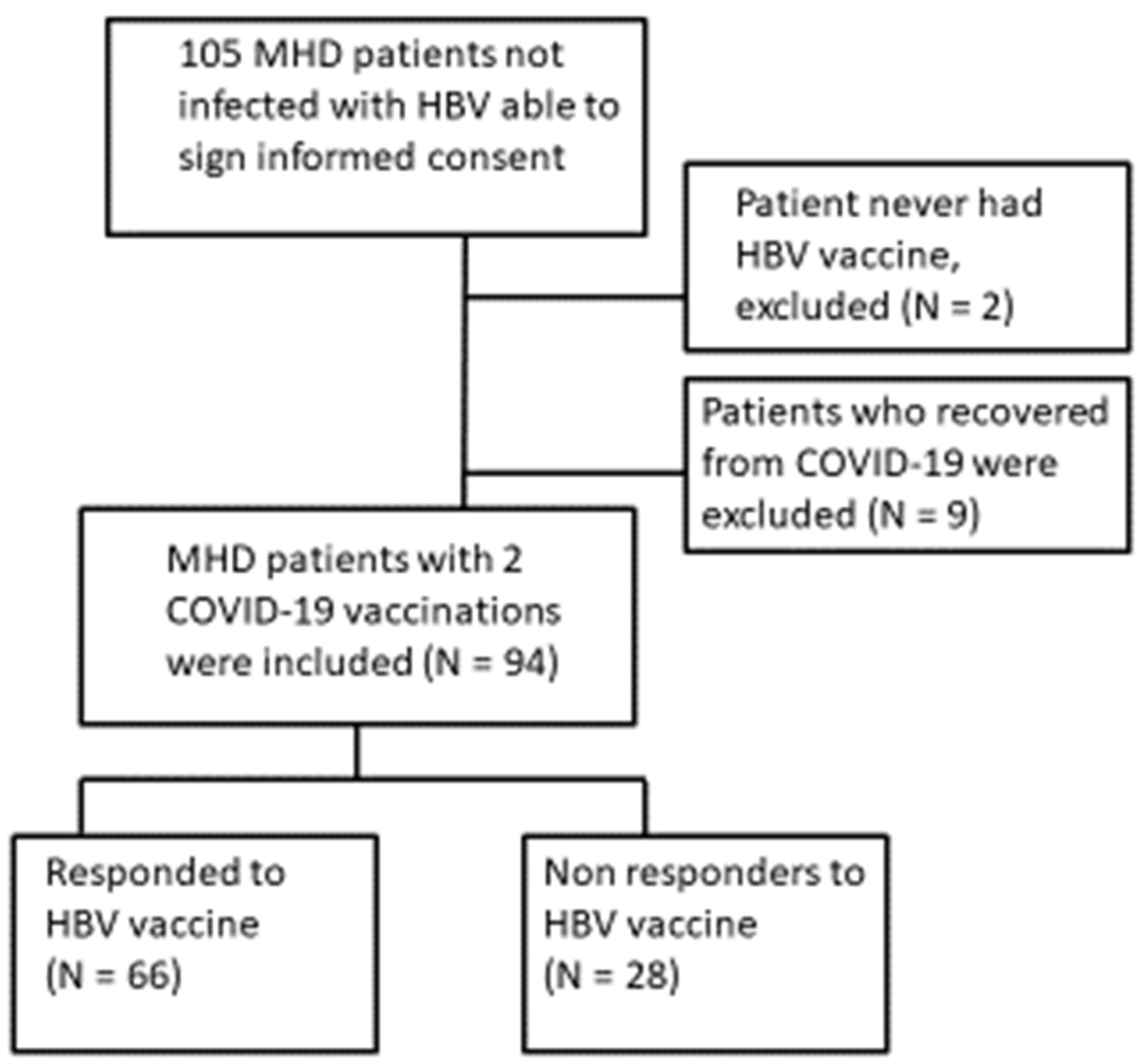
2.1. Patients
2.2. Anti-Hepatitis B Antibodies
2.3. SARS-CoV-2 Spike IgG
2.4. Statistical Analysis
2.5. Ethical Issues
3. Results
3.1. SARS-CoV-2 Spike IgG Titers
3.2. HBV Vaccine Response
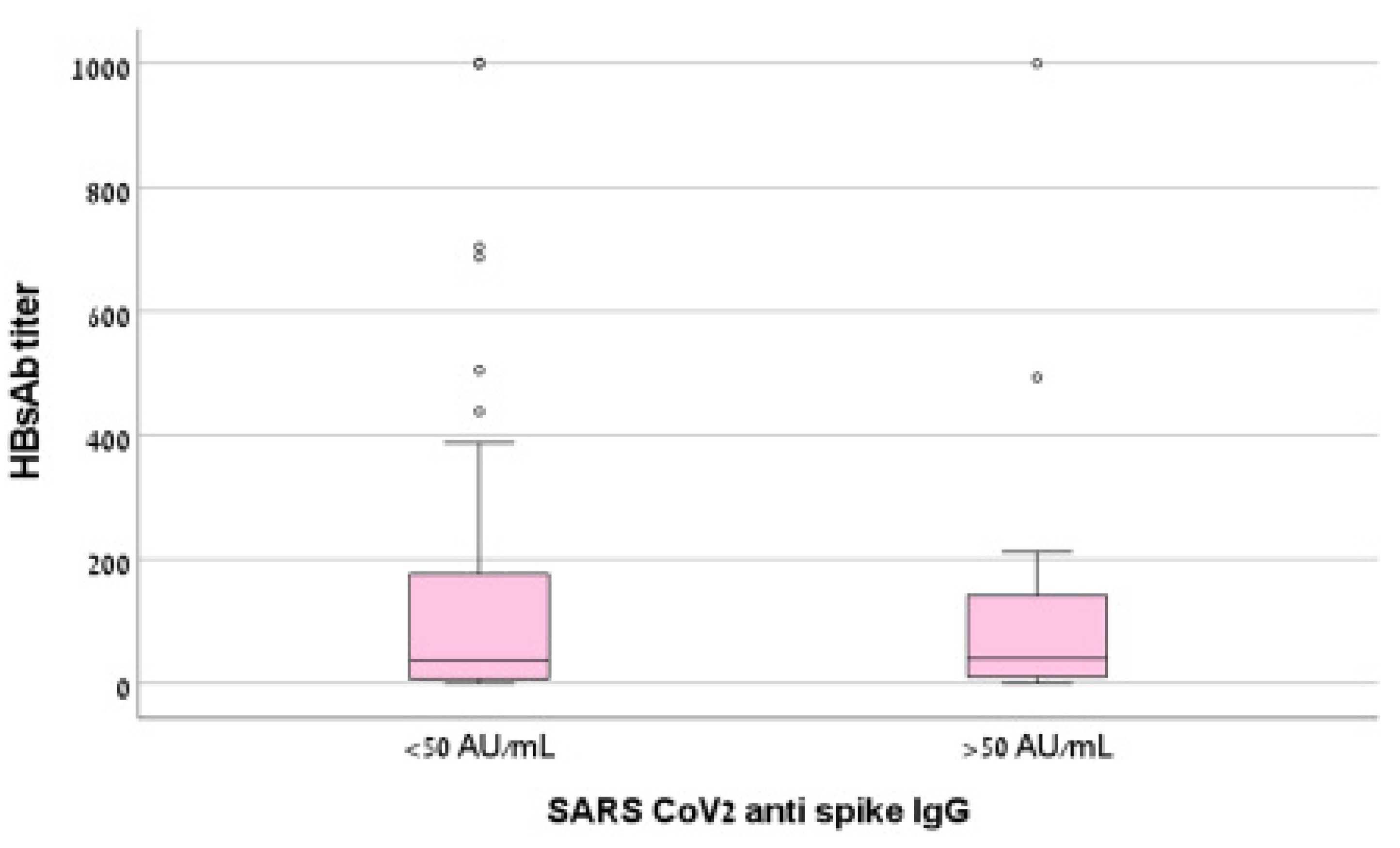
3.3. HBV and SARS-CoV-2 IgGs Titers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fabrizi, F.; Dixit, V.; Martin, P.; Jadoul, M.; Messa, P. Meta-Analysis: The Impact of Nutritional Status on the Immune Response to Hepatitis B Virus Vaccine in Chronic Kidney Disease. Am. J. Dig. Dis. 2012, 57, 1366–1372. [Google Scholar] [CrossRef]
- United States Renal Data System. 2016 USRDS annual data report: Epidemiology of kidney disease in the United States. In National Institutes of Health; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2016. [Google Scholar]
- Stevens, C.E.; Alter, H.J.; Taylor, P.E.; Zang, E.A.; Harley, E.J.; Szmuness, W.; the Dialysis Vaccine Trial Study Group. Hepatitis B Vaccine in Patients Receiving Hemodialysis. N. Engl. J. Med. 1984, 311, 496–501. [Google Scholar] [CrossRef]
- Buti, M.; Viladomiu, L.; Jardí, R.; Olmos, A.; Rodriguez, J.A.; Bartolome, J.; Esteban, R.; Guardia, J. Long-Term Immunogenicity and Efficacy of Hepatitis B Vaccine in Hemodialysis Patients. Am. J. Nephrol. 1992, 12, 144–147. [Google Scholar] [CrossRef]
- Cohen, G. Immune Dysfunction in Uremia 2020. Toxins 2020, 12, 439. [Google Scholar] [CrossRef] [PubMed]
- Verkade, M.A.; Van Druningen, C.J.; Vaessen, L.M.B.; Hesselink, D.A.; Weimar, W.; Betjes, M.G.H. Functional impairment of monocyte-derived dendritic cells in patients with severe chronic kidney disease. Nephrol. Dial. Transplant. 2006, 22, 128–138. [Google Scholar] [CrossRef]
- Kim, J.U.; Kim, M.; Kim, S.; Nguyen, T.T.; Kim, E.; Lee, S.; Kim, S.; Kim, H. Dendritic Cell Dysfunction in Patients with End-stage Renal Disease. Immune Netw. 2017, 17, 152–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stachowski, J.; Pollok, M.; Burrichter, H.; Spithaler, C.; Baldamus, C. Signalling via the TCR/CD3 Antigen Receptor Complex in Uremia Is Limited by the Receptors Number. Nephron Exp. Nephrol. 1993, 64, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Stachowski, J.; Pollok, M.; Burrichter, H. Baldamus CA: Immunodeficiency in ESRD-patients is linked to altered IL-2 receptor density on T cell subsets. J. Clin. Lab. Immunol. 1991, 34, 171–177. [Google Scholar] [PubMed]
- Stachowski, J.; Pollok, M.; Barth, C.; Maciejewski, J.; Baldamus, C.A. Non-responsiveness to hepatitis B vaccination in haemo-dialysis patients: Association with impaired TCR/CD3 antigen receptor expression regulating co-stimulatory processes in an-tigen presentation and recognition. Nephrol. Dial. Transplant. 1994, 9, 144–152. [Google Scholar] [PubMed]
- Eleftheriadis, T.; Antoniadi, G.; Liakopoulos, V.; Kartsios, C.; Stefanidis, I. Basic Science and Dialysis: Disturbances of Acquired Immunity in Hemodialysis Patients. Semin. Dial. 2007, 20, 440–451. [Google Scholar] [CrossRef]
- Lord, J.M. The effect of aging of the immune system on vaccination responses. Hum. Vaccines Immunother. 2013, 9, 1364–1367. [Google Scholar] [CrossRef] [Green Version]
- Fabrizi, F.; Dixit, V.; Martin, P.; Messa, P. Meta-analysis: The impact of diabetes mellitus on the immunological response to hepatitis B virus vaccine in dialysis patients. Aliment. Pharmacol. Ther. 2011, 33, 815–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabrizi, F.; Martin, P.; Dixit, V.; Bunnapradist, S.; Dulai, G. Meta-analysis: The effect of age on immunological response to hepatitis B vaccine in end-stage renal disease patients. Aliment. Pharmacol. Ther. 2004, 20, 1053–1062. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Takkavatakarn, K.; Praditpornsilpa, K.; Nader, C.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Hepatitis B virus vaccine immune response and mortality in dialysis patients: A meta-analysis. J. Nephrol. 2020, 33, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Gur, E.; Topaz, G.; Naser, R.; Kitay-Cohen, Y.; Benchetrit, S.; Sarel, E.; Cohen-Hagai, K.; Wand, O. Mortality prediction using a modified R2CHA2DS2-VASc score among hospitalized COVID-19 patients. Intern. Emerg. Med. 2022, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gur, E.; Levy, D.; Topaz, G.; Naser, R.; Wand, O.; Kitay-Cohen, Y.; Benchetrit, S.; Sarel, E.; Cohen-Hagai, K. Disease severity and renal outcomes of patients with chronic kidney disease infected with COVID-19. Clin. Exp. Nephrol. 2022, 26, 445–452. [Google Scholar] [CrossRef]
- Wand, O.; Mor, O.; Zuckerman, N.; Fadeela, A.; Benchetrit, S.; Nacasch, N.; Cohen-Hagai, K. Outcomes from Infections with Variant Strains of SARS-CoV-2 Among Patients Receiving Maintenance Hemodialysis. Am. J. Kidney Dis. 2021, 78, 617–619. [Google Scholar] [CrossRef]
- Uribarri, A.; Núñez-Gil, I.J.; Aparisi, A.; Becerra-Muñoz, V.M.; Feltes, G.; Trabattoni, D.; Fernández-Rozas, I.; Viana-Llamas, M.C.; Pepe, M.; Cerrato, E.; et al. Impact of renal function on admission in COVID-19 patients: An analysis of the international HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID-19) Registry. J. Nephrol. 2020, 33, 737–745. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T-cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Speer, C.; Göth, D.; Benning, L.; Buylaert, M.; Schaier, M.; Grenz, J.; Nusshag, C.; Kälble, F.; Kreysing, M.; Reichel, P.; et al. Early Humoral Responses of Hemodialysis Patients after COVID-19 Vaccination with BNT162b2. Clin. J. Am. Soc. Nephrol. 2021, 16, 1073–1082. [Google Scholar] [CrossRef]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef]
- Danthu, C.; Hantz, S.; Dahlem, A.; Duval, M.; Ba, B.; Guibbert, M.; El Ouafi, Z.; Ponsard, S.; Berrahal, I.; Achard, J.-M.; et al. Humoral Response after SARS-CoV-2 mRNA Vaccination in a Cohort of Hemodialysis Patients and Kidney Transplant Recipients. J. Am. Soc. Nephrol. 2021, 32, 2153–2158. [Google Scholar] [CrossRef]
- Nacasch, N.; Erez, D.; Lishner, M.; Benchetrit, S.; Rozenberg, I.; Sarel, E.; Shitrit, P.; Wand, O.; Cohen-Hagai, K. Long-term Antibody Response to the BNT162b2 Vaccine Among Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2022, 79, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Shashar, M.; Nacasch, N.; Grupper, A.; Benchetrit, S.; Halperin, T.; Erez, D.; Rozenberg, I.; Shitrit, P.; Sela, Y.; Wand, O.; et al. Humoral Response to Pfizer BNT162b2 Vaccine Booster in Maintenance Hemodialysis Patients. Am. J. Nephrol. 2022, 53, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Mulley, W.R.; Le, S.T.; Ives, K.E. Primary seroresponses to double-dose compared with standard-dose hepatitis B vaccination in patients with chronic kidney disease: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2017, 32, gfv443-143. [Google Scholar] [CrossRef] [Green Version]
- Sayarlioglu, H.; Erkoç, R.; Demir, C.; Dogan, E.; Sayarlioglu, M.; Öner, A.F.; Dilek, I. Nutritional Status and Immune Functions in Maintenance Hemodialysis Patients. Mediat. Inflamm. 2006, 2006, 020264. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Humphreys, M.H.; Block, G. Comparing outcome predictability of markers of malnutrition-inflammation complex syndrome in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1507–1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen-Hagai, K.; Nacasch, N.; Sternschuss, A.; Ohana, M.; Wolach, B.; Benchetrit, S.; Gavrieli, R.; Zitman-Gal, T. Malnutrition and inflammation in hemodialysis patients: Comparative evaluation of neutrophil reactive oxygen formation. Nutrition 2020, 78, 110793. [Google Scholar] [CrossRef]
- Wand, O.; Nacasch, N.; Fadeela, A.; Shashar, M.; Grupper, A.; Benchetrit, S.; Erez, D.; Shitrit, P.; Cohen-Hagai, K. Humoral response and breakthrough infections with SARS-CoV-2 B.1.617.2 variant in vaccinated maintenance hemodialysis patients. J. Nephrol. 2022, 35, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Einbinder, Y.; Hornik-Lurie, T.; Cohen-Hagai, K.; Goldman, S.; Tanasiychuk, T.; Nacasch, N.; Erez, D.; Magen, S.; Zitman-Gal, T.; Wiener-Well, Y.; et al. Correction to: Comparison of long-term antibody response to mRNA SARS-CoV-2 vaccine among peritoneal dialysis and hemodialysis patients. Nephrol. Dial. Transplant. 2022, 37, 1780. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, N.; Weissman, D.; Whitehead, K.A. mRNA vaccines for infectious diseases: Principles, delivery and clinical translation. Nat. Rev. Drug Discov. 2021, 20, 817–838. [Google Scholar] [CrossRef] [PubMed]
- Van Praet, J.; Reynders, M.; De Bacquer, D.; Viaene, L.; Schoutteten, M.K.; Caluwé, R.; Doubel, P.; Heylen, L.; De Bel, A.V.; Van Vlem, B.; et al. Predictors and Dynamics of the Humoral and Cellular Immune Response to SARS-CoV-2 mRNA Vaccines in Hemodialysis Patients: A Multicenter Observational Study. J. Am. Soc. Nephrol. 2021, 32, 3208–3220. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | HbsAb < 10 mIU/mL (n = 28) | HbsAb ≥ 10 mIU/mL (n = 66) | p-Value |
|---|---|---|---|
| Age (years) | 72.1 ± 12.2 | 69.8 ± 15.5 | 0.5 |
| Weight (kg) | 82.1 ± 26.6 | 75.9 ± 16.2 | 0.2 |
| Sex (male) | 18 (64.3) | 44 (66.7) | 0.8 |
| IGG S titer (AU/mL) | 504 ± 781 | 505 ± 644 | 0.9 |
| IGG S < 50 (AU/mL) | 4 (14.3) | 13 (19.7) | 0.5 |
| Diabetes mellitus | 21 (75) | 40 (60.6) | 0.2 |
| Hypertension | 27 (96.4) | 48 (72.7) | 0.01 |
| Coronary heart disease | 19 (67.9) | 15 (22.7) | <0.001 |
| Heart failure | 17 (60.7) | 15 (22.7) | <0.001 |
| Peripheral vascular disease | 3 (10.7) | 7 (10.6) | 0.9 |
| Malignancy | 0 | 1 (1.5) | 0.5 |
| Chronic immunosuppressive therapy | 1 (3.6) | 4 (6.1) | 0.6 |
| kt/V | 1.21 ± 0.22 | 1.31 ± 0.22 | 0.07 |
| Urea reduction ratio | 64.9 ± 7 | 67.5 ± 6.5 | 0.1 |
| Dialysis vintage (months) | 20.6 ± 16.4 | 34.8 ± 25.7 | 0.008 |
| White blood cells (K/µL) | 6 ± 2 | 6.5 ± 2 | 0.4 |
| Lymphocytes (K/µL) | 1 ± 0.4 | 1.4 ± 0.6 | 0.03 |
| Platelets (K/µL) | 169 ± 43 | 195 ± 71 | 0.2 |
| Creatinine (mg/dL) | 6.8 ± 2.4 | 7.5 ± 2.4 | 0.3 |
| Albumin (gr/dL) | 3.6 ± 0.3 | 3.6 ± 0.5 | 0.5 |
| C-reactive protein (mg/dL) | 2.2 ± 1.9 | 2 ± 3.6 | 0.9 |
| PTH (pg/mL) | 359 ± 296 | 290 ± 215 | 0.3 |
| Variable | Correlation Coeffiecient (Spearman’s Rho) | p-Value |
|---|---|---|
| Age (years) | −0.095 | 0.4 |
| Weight (kg) | −0.006 | 0.9 |
| IGG S titer (AU/mL) | 0.15 | 0.2 |
| kt/V | 0.2 | 0.06 |
| Dialysis vintage | 0.3 | 0.005 |
| White blood cells (K/µL) | 0.1 | 0.3 |
| Lymphocytes (K/µL) | 0.3 | 0.005 |
| Albumin (gr/dL) | 0.2 | 0.05 |
| C-reactive protein (mg/dL) | −0.3 | 0.03 |
| PTH (pg/mL) | −0.03 | 0.8 |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Poor response to COVID-19 vaccine | 0.52 | 0.11 | 2.40 | 0.40 |
| Sex (female) | 1.55 | 0.50 | 4.87 | 0.45 |
| Immunosuppressive therapy | 1.19 | 0.06 | 23.82 | 0.91 |
| Diabetes mellitus | 1.06 | 0.31 | 3.63 | 0.92 |
| Hypertension | 3.13 | 0.34 | 28.89 | 0.31 |
| Coronary heart disease | 7.06 | 2.18 | 22.87 | 0.00 |
| Heart failure | 4.22 | 1.41 | 12.64 | 0.01 |
| Malignancy | 0.00 | 1.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nacasch, N.; Cohen-Hagai, K.; Tayar, N.; Levian, A.; Rashid, G.; Benchetrit, S.; Neumark, E.; Wand, O.; Hod, T.; Rosman, Y.; et al. Humoral Response to Hepatitis B and COVID-19 Vaccine among Maintenance Hemodialysis Patients. Vaccines 2022, 10, 1670. https://doi.org/10.3390/vaccines10101670
Nacasch N, Cohen-Hagai K, Tayar N, Levian A, Rashid G, Benchetrit S, Neumark E, Wand O, Hod T, Rosman Y, et al. Humoral Response to Hepatitis B and COVID-19 Vaccine among Maintenance Hemodialysis Patients. Vaccines. 2022; 10(10):1670. https://doi.org/10.3390/vaccines10101670
Chicago/Turabian StyleNacasch, Naomi, Keren Cohen-Hagai, Nurit Tayar, Avraham Levian, Gloria Rashid, Sydney Benchetrit, Eran Neumark, Ori Wand, Tammy Hod, Yossi Rosman, and et al. 2022. "Humoral Response to Hepatitis B and COVID-19 Vaccine among Maintenance Hemodialysis Patients" Vaccines 10, no. 10: 1670. https://doi.org/10.3390/vaccines10101670
APA StyleNacasch, N., Cohen-Hagai, K., Tayar, N., Levian, A., Rashid, G., Benchetrit, S., Neumark, E., Wand, O., Hod, T., Rosman, Y., Shashar, M., Grupper, A., & Shitrit, P. (2022). Humoral Response to Hepatitis B and COVID-19 Vaccine among Maintenance Hemodialysis Patients. Vaccines, 10(10), 1670. https://doi.org/10.3390/vaccines10101670