



Long-Term Dynamic Humoral Response to SARS-CoV-2 mRNA Vaccines in Patients on Peritoneal Dialysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population
2.3. Objectives and Outcomes
2.4. Variables
2.5. Statistics
3. Results
3.1. Baseline Characteristics
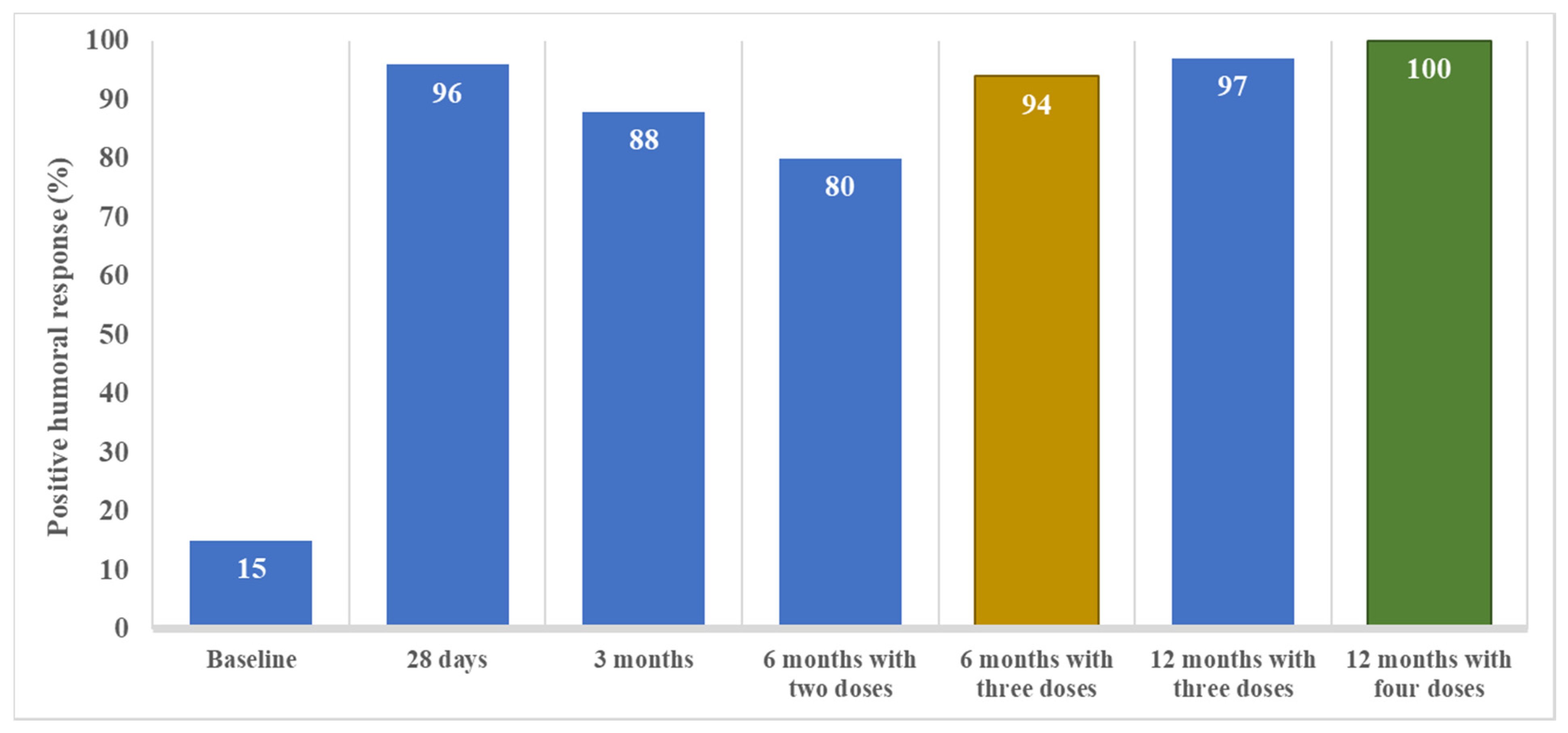
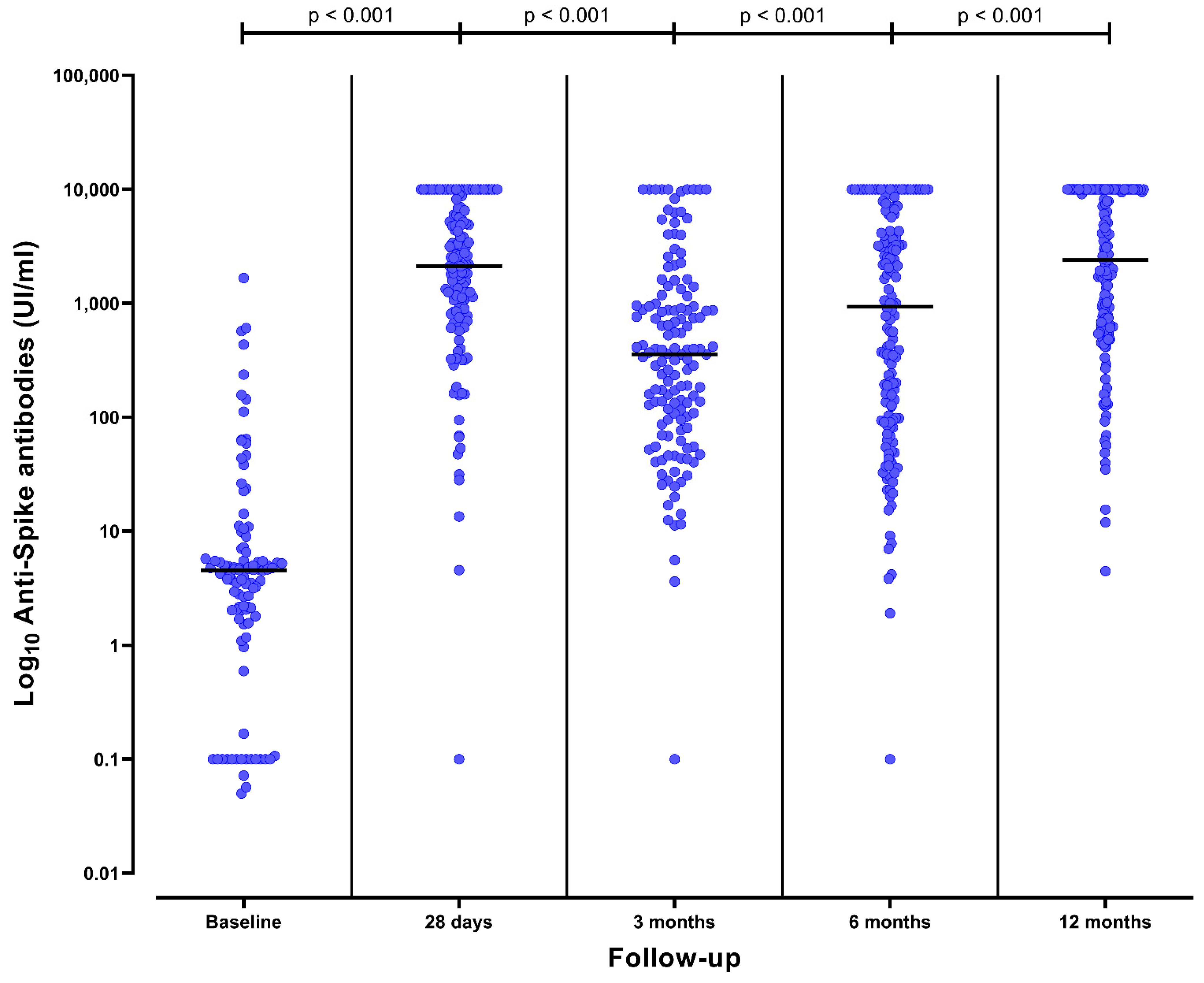
3.2. Humoral Response after the Initial Vaccination Schedule
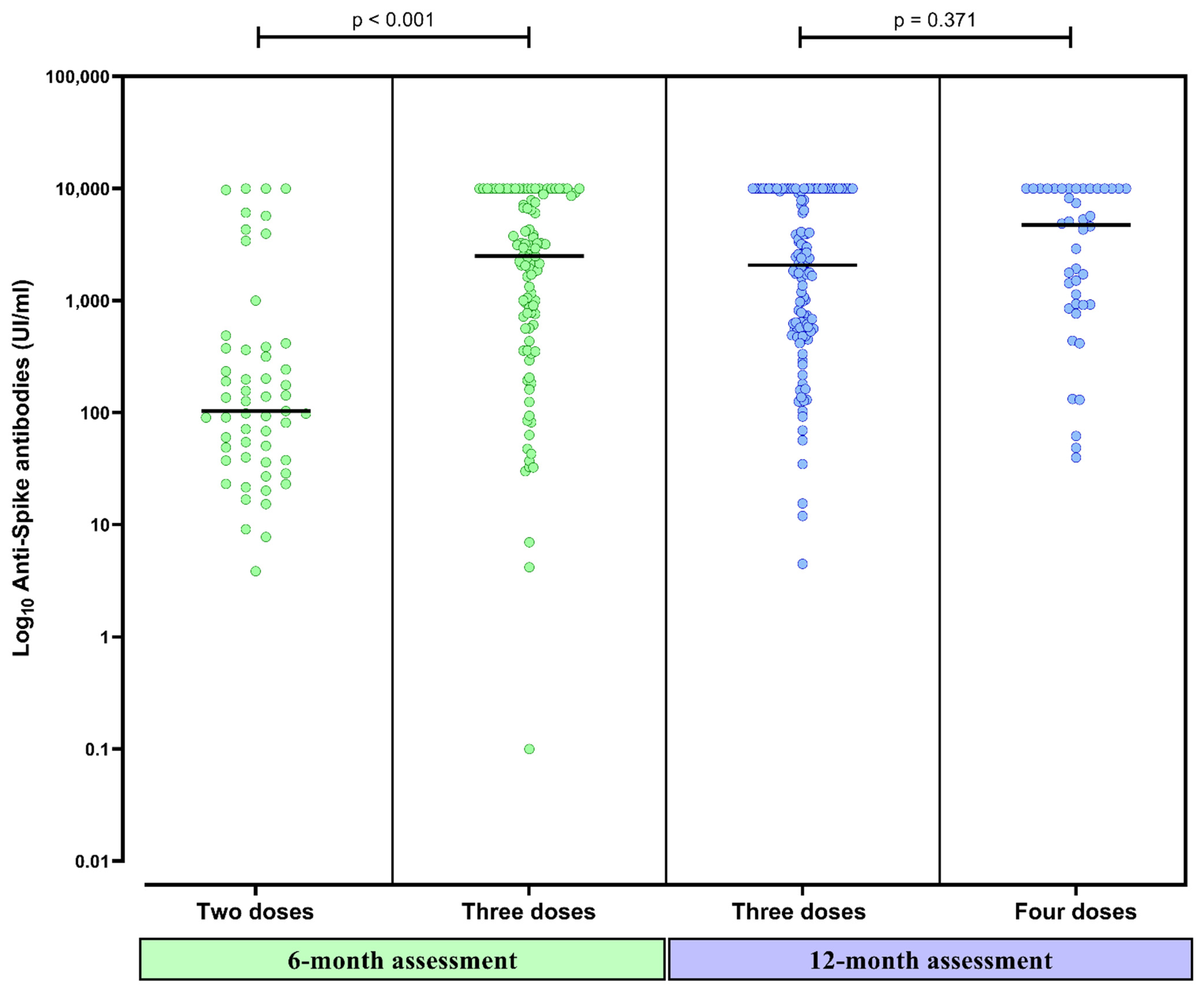
3.3. Humoral Response after the Third Dose at 6 Months
3.4. Humoral Response after the Fourth Dose at 6 Months
3.5. Factors Associated with Stronger Humoral Response at 12 Months
3.6. Breakthrough Infections
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Goffin, E.; Candellier, A.; Vart, P.; Noordzij, M.; Arnol, M.; Covic, A.; Lentini, P.; Malik, S.; Reichert, L.J.; Sever, M.S.; et al. COVID-19-Related Mortality in Kidney Transplant and Haemodialysis Patients: A Comparative, Prospective Registry-Based Study. Nephrol. Dial. Transplant. 2021, 36, 2094–2105. [Google Scholar] [CrossRef] [PubMed]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; de Vries, H.; et al. COVID-19-Related Mortality in Kidney Transplant and Dialysis Patients: Results of the ERACODA Collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Badrouchi, S.; Barbouch, S.; Bettaieb, A.; Sellami, N.; Hajji, M.; Ben Abdallah, T.; Ben Hamida, F.; Harzallah, A.; Abderrahim, E. Peritoneal Dialysis in the Era of COVID-19: Experience of a Tunisian Center. J. Nephrol. 2022, 1–5. [Google Scholar] [CrossRef]
- Fernandez-Prado, R.; Gonzalez-Parra, E.; Ortiz, A. Often Forgotten, Transport Modality to Dialysis May Be Life-Saving. Clin. Kidney J. 2020, 13, 510–512. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Martínez Vaquera, S.; Jarava Mantecón, C.J.; Useche, G.; Sánchez Márquez, M.G.; Carnerero, M.; Jaldo Rodríguez, M.T.; Muñoz Ramos, P.; et al. Safety and Immediate Humoral Response of COVID-19 Vaccines in Chronic Kidney Disease Patients: The SENCOVAC Study. Nephrol. Dial. Transplant. 2021, 37, 1868–1878. [Google Scholar] [CrossRef]
- Quiroga, B.; Ortiz, A.; Cabezas-Reina, C.J.; Ruiz Fuentes, M.C.; Jiménez, V.L.; Larrondo, S.Z.; Toapanta, N.; Gómez, M.M.; de Sequera, P.; Sánchez-Álvarez, E.; et al. Evolving Spectrum but Persistent High Mortality of COVID-19 among Patients on Kidney Replacement Therapy in the Vaccine Era: The Spanish COVID-19 KRT Registry. Clin. Kidney J. 2022, 15, 1685–1697. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Bernat, A.; Muñoz Díaz, A.B.; Jarava Mantecón, C.J.; Gómez Pérez, V.O.; Calderón González, C.; Cervienka, M.; Mazuecos, A.; et al. Loss of Humoral Response 3 Months after SARS-CoV-2 Vaccination in the CKD Spectrum: The Multicentric SENCOVAC Study. Nephrol. Dial. Transplant. 2022, 37, 994–999. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Orero, E.; Tejedor, S.; Mantecón, C.J.J.; Gómez Pérez, V.O.; Marín Franco, A.J.; Alfaro Sánchez, C.; Puerta Carretero, M.; et al. Humoral Response to Third Dose of SARS-CoV-2 Vaccines in the CKD Spectrum. CJASN 2022, 17, 872–876. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Jaravaca Mantecón, C.J.; Nava Pérez, N.; Serra Martín, M.; Sato, Y.; Marin Franco, A.J.; Pazmiño Zambrano, D.F.; Lucena Valverde, R.; et al. Anti-Spike Antibodies 3 Months after SARS-CoV-2 MRNA Vaccine Booster Dose in Patients on Hemodialysis: The Prospective SENCOVAC Study. Clin. Kidney J. 2022, 15, 1856–1864. [Google Scholar] [CrossRef]
- Glowinska, I.; Labij-Reduta, B.; Juzwiuk, J.; Lukaszewicz, M.; Pietruczuk, A.; Poplawska, A.; Daniluk-Jamro, A.; Kakareko, K.; Rydzewska-Rosolowska, A.; Naumnik, B.; et al. Factors Influencing Longevity of Humoral Response to SARS-CoV-2 Vaccination in Patients with End Stage Kidney Disease Receiving Renal Replacement Therapy. JCM 2022, 11, 4984. [Google Scholar] [CrossRef] [PubMed]
- Boongird, S.; Setthaudom, C.; Kitpermkiat, R.; Prasongtanakij, S.; Srisala, S.; Chuengsaman, P.; Nongnuch, A.; Assanatham, M.; Kiertiburanakul, S.; Malathum, K.; et al. Durability of Humoral and Cellular Immunity after an Extended Primary Series with Heterologous Inactivated SARS-CoV-2 Prime-Boost and ChAdOx1 NCoV-19 in Dialysis Patients (ICON3). Vaccines 2022, 10, 1064. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Schwöbel, J.; Lindner, T.; Anders, L.; Siepmann, T.; Karger, C.; Hüther, J.; Martin, H.; Müller, P.; Faulhaber-Walter, R.; et al. Risk of Strong Antibody Decline in Dialysis and Transplant Patients after SARS-CoV-2mRNA Vaccination: Six Months Data from the Observational Dia-Vacc Study. Lancet Reg. Health Eur. 2022, 17, 100371. [Google Scholar] [CrossRef] [PubMed]
- Beilhack, G.; Monteforte, R.; Frommlet, F.; Reindl-Schwaighofer, R.; Strassl, R.; Vychytil, A. Humoral Response to MRNA-1273 SARS-CoV-2 Vaccine in Peritoneal Dialysis Patients: Is Boostering After Six Months Adequate? Front. Med. 2022, 9, 905798. [Google Scholar] [CrossRef]
- Housset, P.; Kubab, S.; Pardon, A.; Vittoz, N.; Bozman, D.-F.; Hanafi, L.; Caudwell, V.; Faucon, A.-L. Waning but Persistent Humoral Response 6 Months after the Third Dose of the MRNA BNT162b2 Vaccine in Hemodialysis and Peritoneal Dialysis Patients. J. Nephrol. 2022, 35, 783–785. [Google Scholar] [CrossRef]
- Murt, A.; Dinc, H.O.; Altiparmak, M.R.; Yalin, S.F.; Yadigar, S.; Parmaksiz, E.; Kocazeybek, B.; Pekpak, M.; Ataman, M.R. Waning of SARS-CoV-2 Vaccine-Induced Immune Response over 6 Months in Peritoneal Dialysis Patients and the Role of a Booster Dose in Maintaining Seropositivity. Nephron 2022, 1–5. [Google Scholar] [CrossRef]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Bozman, D.-F.; Hanafi, L.; Faucon, A.-L.; Housset, P. SARS-CoV-2 Antibody Response After a Third Dose of the BNT162b2 Vaccine in Patients Receiving Maintenance Hemodialysis or Peritoneal Dialysis. Am. J. Kidney Dis. 2022, 79, 185–192. [Google Scholar] [CrossRef]
- Bates, T.A.; Leier, H.C.; Lyski, Z.L.; McBride, S.K.; Coulter, F.J.; Weinstein, J.B.; Goodman, J.R.; Lu, Z.; Siegel, S.A.R.; Sullivan, P.; et al. Neutralization of SARS-CoV-2 Variants by Convalescent and BNT162b2 Vaccinated Serum. Nat. Commun. 2021, 12, 5135. [Google Scholar] [CrossRef]
- Cheng, C.-C.; Platen, L.; Christa, C.; Tellenbach, M.; Kappler, V.; Bester, R.; Liao, B.-H.; Holzmann-Littig, C.; Werz, M.; Schönhals, E.; et al. Improved SARS-CoV-2 Neutralization of Delta and Omicron BA.1 Variants of Concern after Fourth Vaccination in Hemodialysis Patients. Vaccines 2022, 10, 1328. [Google Scholar] [CrossRef]
- da Silva, E.S.; Kohnen, M.; Gilson, G.; Staub, T.; Arendt, V.; Hilger, C.; Servais, J.-Y.; Charpentier, E.; Domingues, O.; Snoeck, C.J.; et al. Pre-Omicron Vaccine Breakthrough Infection Induces Superior Cross-Neutralization against SARS-CoV-2 Omicron BA.1 Compared to Infection Alone. Int. J. Mol. Sci. 2022, 23, 7675. [Google Scholar] [CrossRef]
- Herman-Edelstein, M.; Ben-Dor, N.; Agur, T.; Guetta, T.; Raiter, A.; Meisel, E.; Alkeesh, W.; Ori, Y.; Rozen-Zvi, B.; Zingerman, B. BNT162b2 Booster Vaccination Induced Immunity against SARS-CoV-2 Variants among Hemodialysis Patients. Vaccines 2022, 10, 967. [Google Scholar] [CrossRef] [PubMed]
- Attias, P.; Azzaoui, I.; El Karoui, K.; de La Selle, A.; Sokal, A.; Chappert, P.; Grimbert, P.; Fernandez, I.; Bouvier, M.; Samson, C.; et al. Immune Responses after a Third Dose of MRNA Vaccine Differ in Virus-Naive versus SARS-CoV-2-Recovered Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2022, 17, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Giorgi, M.; Barril, G. During COVID-19 Stay at Home Even If You Are a Hemodialysis Patient. Ther. Apher. Dial. 2021, 25, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Einbinder, Y.; Perl, J.; Nacasch, N.; Bnaya, A.; Shavit, L.; Erez, D.; Shashar, M.; Halperin, T.; Grupper, A.; Benchetrit, S.; et al. Humoral Response and SARS-CoV-2 Infection Risk Following the Third and Fourth Doses of the BNT162b2 Vaccine in Dialysis Patients. Am. J. Nephrol. 2022, 53, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Niedźwiedzka-Rystwej, P.; Majchrzak, A.; Aksak-Wąs, B.; Serwin, K.; Czajkowski, Z.; Grywalska, E.; Korona-Głowniak, I.; Roliński, J.; Parczewski, M. Programmed Cell Death-1/Programmed Cell Death-1 Ligand as Prognostic Markers of Coronavirus Disease 2019 Severity. Cells 2022, 11, 1978. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.Q.; Moorman, J.P. Immune Exhaustion and Immune Senescence: Two Distinct Pathways for HBV Vaccine Failure during HCV and/or HIV Infection. Arch. Immunol. Ther. Exp. 2013, 61, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Ponce, P.; Peralta, R.; Felix, C.; Pinto, C.; Pinto, B.; Matos, J.F. Vaccination against SARS-CoV-2 in Haemodialysis Patients: Spike’s Ab Response and the Influence of BMI and Age. Int. J. Environ. Res. Public Health 2022, 19, 10091. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| B (95%CI) | p | |
|---|---|---|
| Age (years) | 44 (−52, 141) | 0.913 |
| Gender (male) | 1726 (−519, 3972) | 0.129 |
| mRNA-based vaccine (mRNA-1273) | −914 (−3054, 1225) | 0.394 |
| Fourth dose (yes) | 2086 (−386, 4560) | 0.096 |
| Anti-Spike antibody titers at 6 months (per UI/mL) | 0.530 (0.274, 0.786) | <0.001 |
| Patient | Timing of COVID-19 | Initial SARS-CoV-2 Vaccine | Third SARS-CoV-2 Vaccine Dose | Last Anti-Spike Titers Prior to COVID-19 (mUI/L) | Infection Severity | Anti-Spike Titers Post-COVID-19 (mUI/L) |
|---|---|---|---|---|---|---|
| 1 | Before 3rd dose | BNT162b2 | -- | 1065 | Mild symptoms without admission | 6599 |
| 2 | Before 4th dose | mRNA-1273 | mRNA-1273 | 3135 | Mild symptoms without admission | 10,000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quiroga, B.; Soler, M.J.; Ortiz, A.; Gansevoort, R.T.; Leyva, A.; Rojas, J.; de Sequera, P., on behalf of SENCOVAC Collaborative Network. Long-Term Dynamic Humoral Response to SARS-CoV-2 mRNA Vaccines in Patients on Peritoneal Dialysis. Vaccines 2022, 10, 1738. https://doi.org/10.3390/vaccines10101738
Quiroga B, Soler MJ, Ortiz A, Gansevoort RT, Leyva A, Rojas J, de Sequera P on behalf of SENCOVAC Collaborative Network. Long-Term Dynamic Humoral Response to SARS-CoV-2 mRNA Vaccines in Patients on Peritoneal Dialysis. Vaccines. 2022; 10(10):1738. https://doi.org/10.3390/vaccines10101738
Chicago/Turabian StyleQuiroga, Borja, María José Soler, Alberto Ortiz, Ron T. Gansevoort, Alba Leyva, José Rojas, and Patricia de Sequera on behalf of SENCOVAC Collaborative Network. 2022. "Long-Term Dynamic Humoral Response to SARS-CoV-2 mRNA Vaccines in Patients on Peritoneal Dialysis" Vaccines 10, no. 10: 1738. https://doi.org/10.3390/vaccines10101738
APA StyleQuiroga, B., Soler, M. J., Ortiz, A., Gansevoort, R. T., Leyva, A., Rojas, J., & de Sequera, P., on behalf of SENCOVAC Collaborative Network. (2022). Long-Term Dynamic Humoral Response to SARS-CoV-2 mRNA Vaccines in Patients on Peritoneal Dialysis. Vaccines, 10(10), 1738. https://doi.org/10.3390/vaccines10101738