

Estimation of mRNA COVID-19 Vaccination Effectiveness in Tokyo for Omicron Variants BA.2 and BA.5: Effect of Social Behavior

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Computational Approach
2.3. Data for Vaccination
2.4. Data Associated with Social Behavior
2.5. Statistical Analysis
3. Results
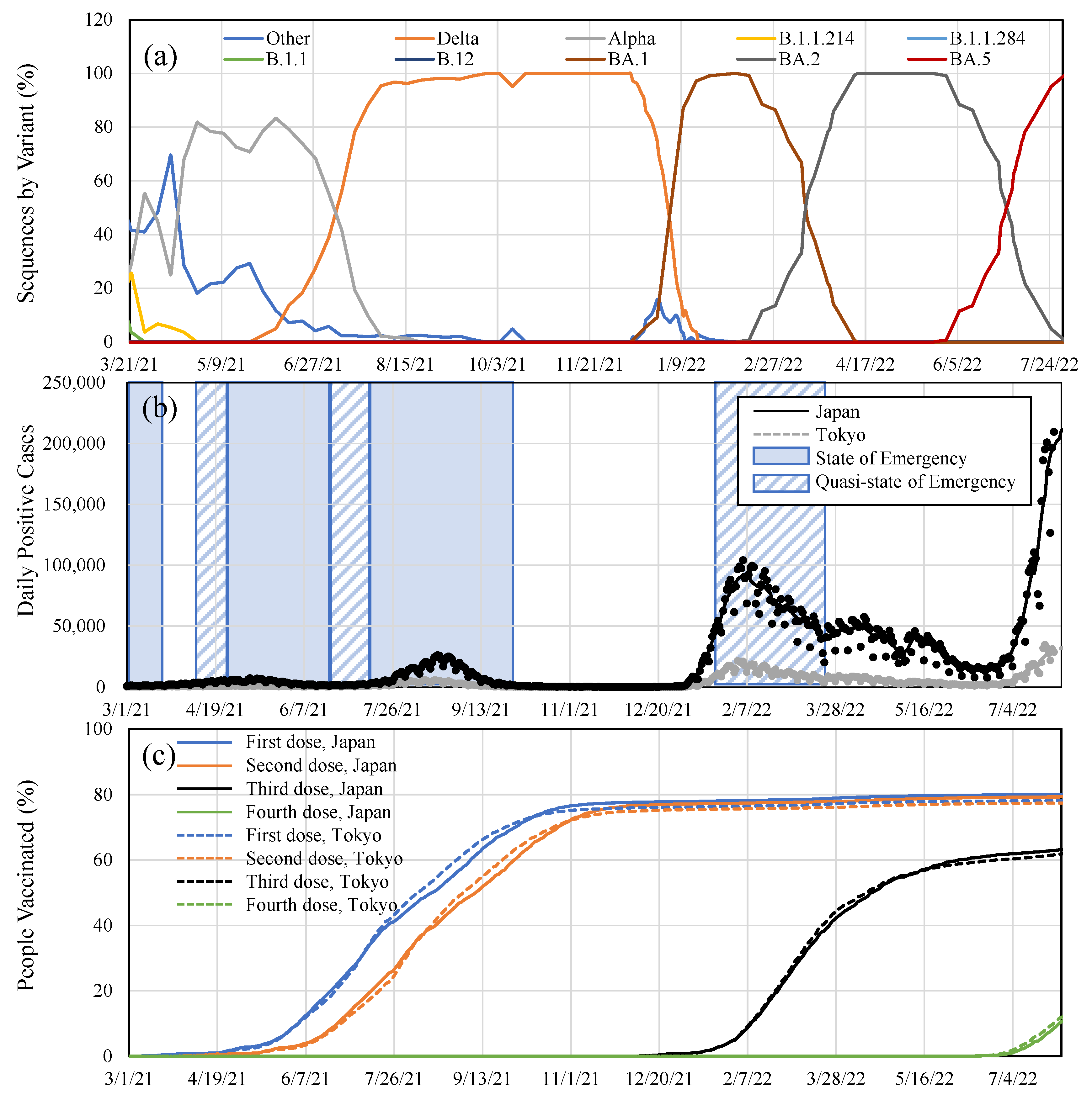
3.1. Vaccination Effectiveness for BA.2 and BA.5
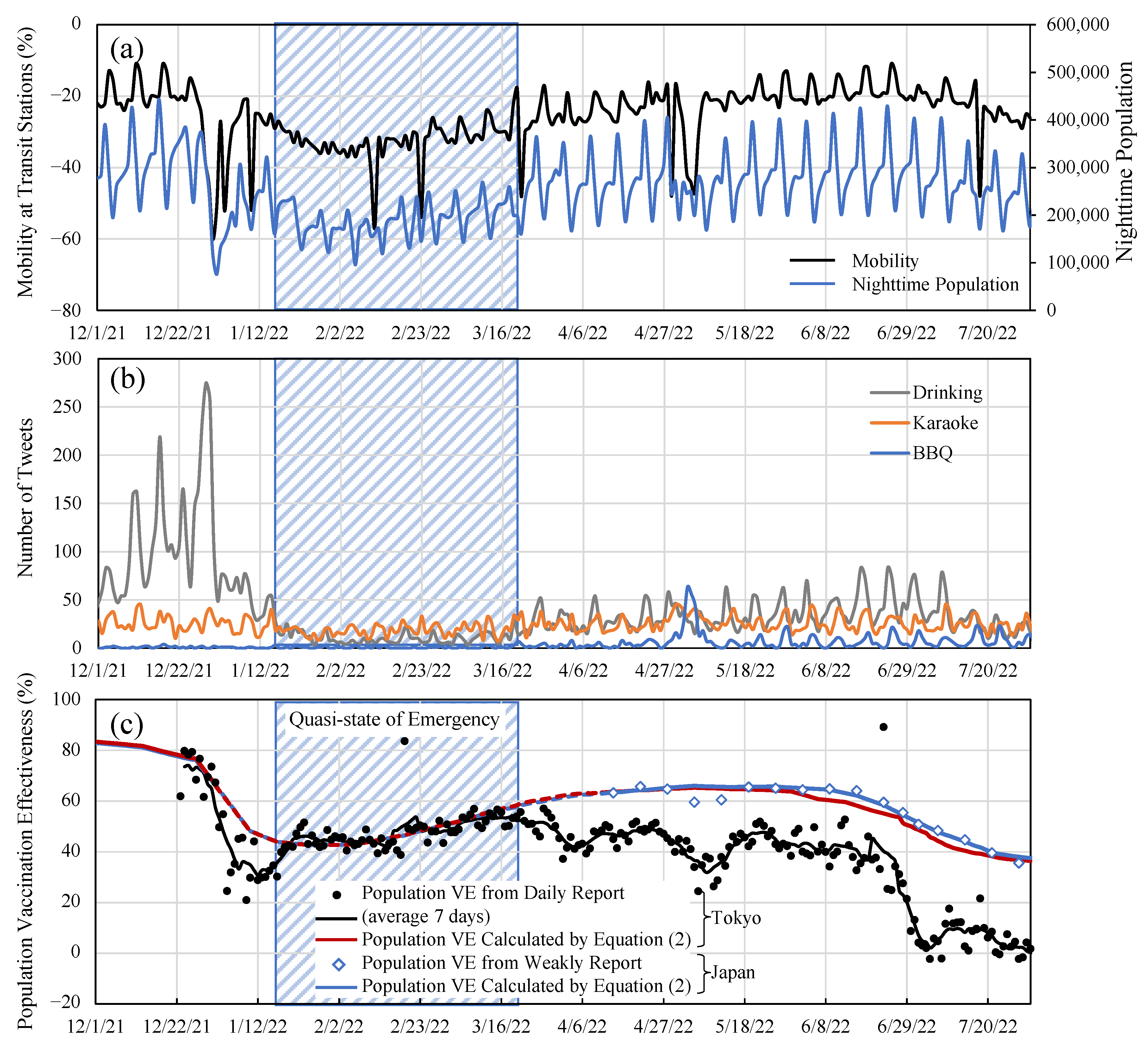
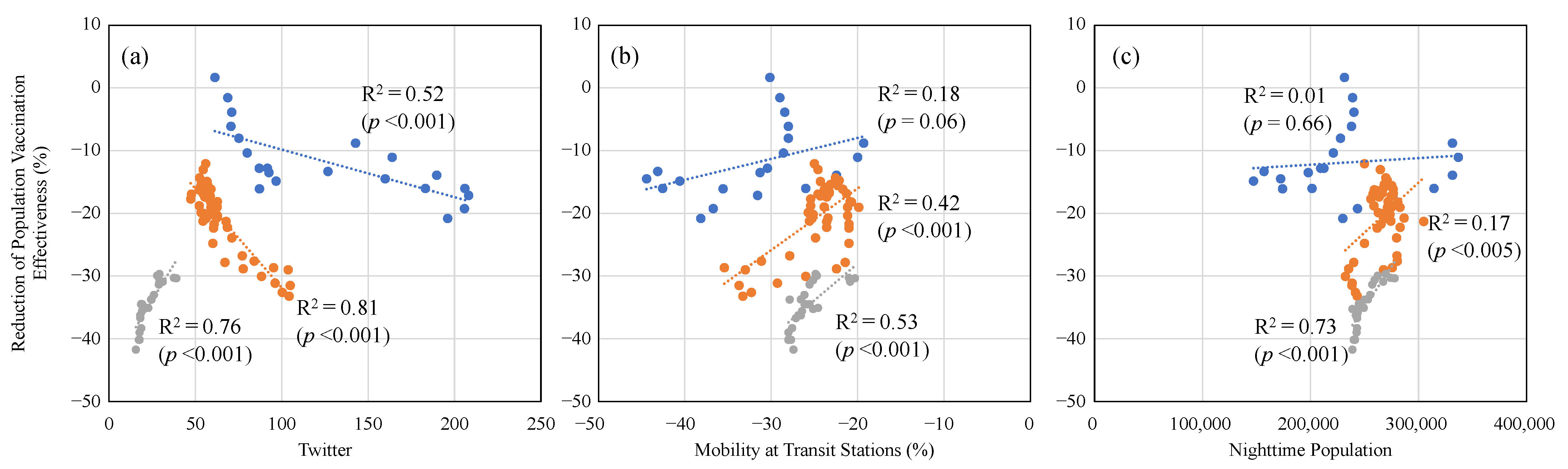
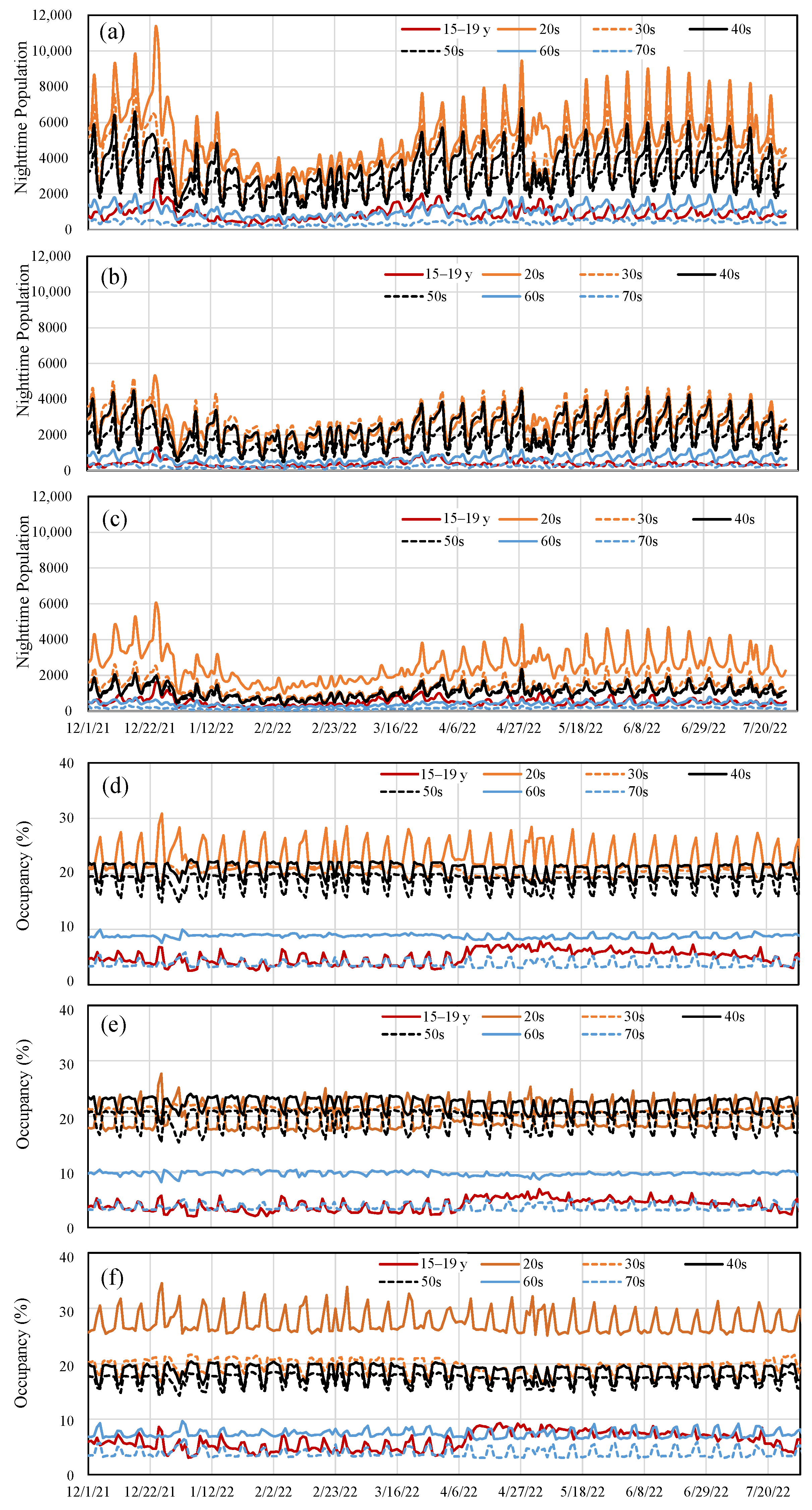
3.2. Effect of Different Factors on Vaccination Effectiveness in Tokyo
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 27 November 2021).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 27 November 2021).
- Wadman, M. A grim warning from Israel: Vaccination blunts, but does not defeat Delta. Science 2021, 373, 838–839. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning immunity after the BNT162b2 vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M. Covid-19 vaccine effectiveness against the omicron (B. 1.1. 529) variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Hafiz, I.; Illian, D.N.; Meila, O.; Utomo, A.R.H.; Susilowati, A.; Susetya, I.E.; Desrita, D.; Siregar, G.A.; Basyuni, M. Effectiveness and Efficacy of Vaccine on Mutated SARS-CoV-2 Virus and Post Vaccination Surveillance: A Narrative Review. Vaccines 2022, 10, 82. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. How Flu Vaccine Effectiveness and Efficacy are Measured. Available online: https://www.cdc.gov/flu/vaccines-work/effectivenessqa.htm (accessed on 29 September 2022).
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Gumeni, S.; Malandrakis, P.; Papanagnou, E.-D.; Kastritis, E.; Trougakos, I.P.; Dimopoulos, M.A. Robust Neutralizing Antibody Responses 6 Months Post Vaccination with BNT162b2: A Prospective Study in 308 Healthy Individuals. Life 2021, 11, 1077. [Google Scholar] [CrossRef]
- Bayart, J.-L.; Douxfils, J.; Gillot, C.; David, C.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Gerin, V.; et al. Waning of IgG, Total and Neutralizing Antibodies 6 Months Post-Vaccination with BNT162b2 in Healthcare Workers. Vaccines 2021, 9, 1092. [Google Scholar] [CrossRef]
- Sanderson, K. COVID Vaccines Protect Against Delta, but Their Effectiveness Wanes. Available online: https://www.nature.com/articles/d41586-021-02261-8 (accessed on 2 September 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Cocchio, S.; Zabeo, F.; Tremolada, G.; Facchin, G.; Venturato, G.; Marcon, T.; Saia, M.; Tonon, M.; Mongillo, M.; Da Re, F. COVID-19 Vaccine Effectiveness against Omicron Variant among Underage Subjects: The Veneto Region’s Experience. Vaccines 2022, 10, 1362. [Google Scholar] [CrossRef]
- Cocchio, S.; Zabeo, F.; Facchin, G.; Piva, N.; Furlan, P.; Nicoletti, M.; Saia, M.; Tonon, M.; Mongillo, M.; Russo, F. The Effectiveness of a Diverse COVID-19 Vaccine Portfolio and Its Impact on the Persistence of Positivity and Length of Hospital Stays: The Veneto Region’s Experience. Vaccines 2022, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: A systematic review and meta-analysis. BMC Med. 2022, 20, 1–15. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M. Effectiveness of COVID-19 vaccines against Omicron or Delta infection. medRxiv 2022, 12, 21268565. [Google Scholar]
- Kirsebom, F.C.; Andrews, N.; Stowe, J.; Toffa, S.; Sachdeva, R.; Gallagher, E.; Groves, N.; O’Connell, A.-M.; Chand, M.; Ramsay, M. COVID-19 vaccine effectiveness against the omicron (BA. 2) variant in England. Lancet Infect. Dis. 2022, 22, 931–933. [Google Scholar] [CrossRef]
- Langwig, K.E.; Gomes, M.G.M.; Clark, M.D.; Kwitny, M.; Yamada, S.; Wargo, A.R.; Lipsitch, M. Limited available evidence supports theoretical predictions of reduced vaccine efficacy at higher exposure dose. Sci. Rep. 2019, 9, 3203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez-Brito, A.; El Bcheraoui, C.; Pozo-Martin, F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J. Infect. 2021, 83, 281–293. [Google Scholar] [CrossRef]
- Kodera, S.; Rashed, E.A.; Hirata, A. Estimation of Real-World Vaccination Effectiveness of mRNA COVID-19 Vaccines against Delta and Omicron Variants in Japan. Vaccines 2022, 10, 430. [Google Scholar] [CrossRef]
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef]
- Tetteh, J.N.; Hernandez-Vargas, E.A. Network models to evaluate vaccine strategies towards herd immunity in COVID-19. J. Theor. Biol. 2021, 531, 110894. [Google Scholar] [CrossRef]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; Bogan, A. Covid-19 antibody seroprevalence in santa clara county, california. Int. J. Epidemiol. 2021, 50, 410–419. [Google Scholar] [CrossRef]
- Jefferson, T.; Rivetti, D.; Rivetti, A.; Rudin, M.; Di Pietrantonj, C.; Demicheli, V. Efficacy and effectiveness of influenza vaccines in elderly people: A systematic review. Lancet 2005, 366, 1165–1174. [Google Scholar] [CrossRef]
- Prime Minister of Japan and His Cabinet. COVID-19 Vaccines. Available online: https://japan.kantei.go.jp/ongoingtopics/vaccine.html (accessed on 2 September 2022).
- Tokyo Metropolitan Government. The Disaster Prevention Information, Tokyo. Available online: https://www.bousai.metro.tokyo.lg.jp/taisaku/saigai/index.html (accessed on 2 September 2022).
- Rashed, E.A.; Kodera, S.; Hirata, A. COVID-19 forecasting using new viral variants and vaccination effectiveness models. Comput. Biol. Med. 2022, 149, 105986. [Google Scholar] [CrossRef] [PubMed]
- Digital Agency. Vaccination Recording System. Available online: https://info.vrs.digital.go.jp/dashboard/ (accessed on 2 September 2022).
- Ministry of Health Labour and Welfare. Advisory Board Meetings of COVID-19 Measures. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00294.html (accessed on 2 September 2022).
- Tokyo Metropolitan Government. Available online: https://www.metro.tokyo.lg.jp/tosei/hodohappyo/ichiran.html (accessed on 2 September 2022).
- Nakanishi, M.; Shibasaki, R.; Yamasaki, S.; Miyazawa, S.; Usami, S.; Nishiura, H.; Nishida, A. On-site Dining in Tokyo During the COVID-19 Pandemic: Time Series Analysis Using Mobile Phone Location Data. JMIR Mhealth Uhealth 2021, 9, e27342. [Google Scholar] [CrossRef]
- Chang, S.; Pierson, E.; Koh, P.W.; Gerardin, J.; Redbird, B.; Grusky, D.; Leskovec, J. Mobility network models of COVID-19 explain inequities and inform reopening. Nature 2021, 589, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Google. Google Mobility. Available online: https://www.google.com/covid19/mobility/ (accessed on 2 September 2022).
- Kodera, S.; Rashed, E.A.; Hirata, A. Mobility-dependent and mobility-compensated effective reproduction number of COVID-19 viral variants: New metric for infectivity evaluation. arXiv 2021, arXiv:2111.02961. [Google Scholar]
- Arashiro, T.; Arima, Y.; Muraoka, H.; Sato, A.; Oba, K.; Uehara, Y.; Arioka, H.; Yanai, H.; Kuramochi, J.; Ihara, G. COVID-19 vaccine effectiveness against symptomatic SARS-CoV-2 infection during Delta-dominant and Omicron-dominant periods in Japan: A multi-center prospective case-control study (FASCINATE study). Clin. Infect. Dis. 2022, ciac635. [Google Scholar] [CrossRef]
- Sanada, T.; Honda, T.; Yasui, F.; Yamaji, K.; Munakata, T.; Yamamoto, N.; Kurano, M.; Matsumoto, Y.; Kohno, R.; Toyama, S. Serologic Survey of IgG Against SARS-CoV-2 Among Hospital Visitors Without a History of SARS-CoV-2 Infection in Tokyo, 2020–2021. J. Epidemiol. 2021, 32, 105–111. [Google Scholar] [CrossRef]
- Hu, H.; Nigmatulina, K.; Eckhoff, P. The scaling of contact rates with population density for the infectious disease models. Math. Biosci. 2013, 244, 125–134. [Google Scholar] [CrossRef]
- Kodera, S.; Rashed, E.A.; Hirata, A. Correlation Between COVID-19 Morbidity and Mortality Rates in Japan and Local Population Density, Temperature, and Absolute Humidity. Int. J. Environ. Res. Public Health 2020, 17, 5477. [Google Scholar] [CrossRef]
- Diao, Y.; Kodera, S.; Anzai, D.; Gomez-Tames, J.; Rashed, E.A.; Hirata, A. Influence of population density, temperature, and absolute humidity on spread and decay durations of COVID-19: A comparative study of scenarios in China, England, Germany, and Japan. One Health 2021, 12, 100203. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Shot (a1) | 2nd Shot (a2) | 3rd Shot (a3) | ||
|---|---|---|---|---|
| Delta [16] | Mean | 75 | 96 | |
| (Japan) | 95% CI | (71–79) | (96–97) | |
| Omicron (BA.2) (Japan) | Mean | 61 | 86 | |
| 95% CI | (57–65) | (84–88) | ||
| Omicron (BA.5) (Japan) | Mean | 37 | 63 | |
| 95% CI | (33–40) | (61–65) | ||
| Omicron (BA.1) (Tokyo) | Mean | 63 | 85 | |
| 95% CI | (61–64) | (80–90) |
| Twitter (Three Keywords) | Twitter (Social Drinking) | Nighttime Population | Mobility | ||
|---|---|---|---|---|---|
| 24 December 2021–13 January 2022 | ρ | −0.83 | −0.83 | 0.16 | 0.54 |
| p-value | <0.001 | <0.001 | 0.47 | 0.01 | |
| 24 March 2022–14 May 2022 | ρ | −0.80 | −0.36 | 0.16 | 0.35 |
| p-value | <0.001 | <0.001 | 0.47 | 0.01 | |
| 15 July 2022–31 July 2022 | ρ | 0.92 | 0.93 | 0.93 | 0.79 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kodera, S.; Niimi, Y.; Rashed, E.A.; Yoshinaga, N.; Toyoda, M.; Hirata, A. Estimation of mRNA COVID-19 Vaccination Effectiveness in Tokyo for Omicron Variants BA.2 and BA.5: Effect of Social Behavior. Vaccines 2022, 10, 1820. https://doi.org/10.3390/vaccines10111820
Kodera S, Niimi Y, Rashed EA, Yoshinaga N, Toyoda M, Hirata A. Estimation of mRNA COVID-19 Vaccination Effectiveness in Tokyo for Omicron Variants BA.2 and BA.5: Effect of Social Behavior. Vaccines. 2022; 10(11):1820. https://doi.org/10.3390/vaccines10111820
Chicago/Turabian StyleKodera, Sachiko, Yuki Niimi, Essam A. Rashed, Naoki Yoshinaga, Masashi Toyoda, and Akimasa Hirata. 2022. "Estimation of mRNA COVID-19 Vaccination Effectiveness in Tokyo for Omicron Variants BA.2 and BA.5: Effect of Social Behavior" Vaccines 10, no. 11: 1820. https://doi.org/10.3390/vaccines10111820
APA StyleKodera, S., Niimi, Y., Rashed, E. A., Yoshinaga, N., Toyoda, M., & Hirata, A. (2022). Estimation of mRNA COVID-19 Vaccination Effectiveness in Tokyo for Omicron Variants BA.2 and BA.5: Effect of Social Behavior. Vaccines, 10(11), 1820. https://doi.org/10.3390/vaccines10111820