
Drivers of and Barriers to COVID-19 Vaccine Booster Dose Acceptance in Indonesia

 , , , , , , ,
, , , , , , ,  , , and
, , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Variables and Study Instrument
2.3. Data Collection Procedure
2.4. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of Respondents
3.2. Characteristics of Experience, Knowledge, Perception, Perceived Severity, Perceived Benefit and Perceived Barriers
3.3. Acceptance of the Booster Dose of COVID-19 Vaccine
3.4. Factors Associated with Booster Dose Acceptance
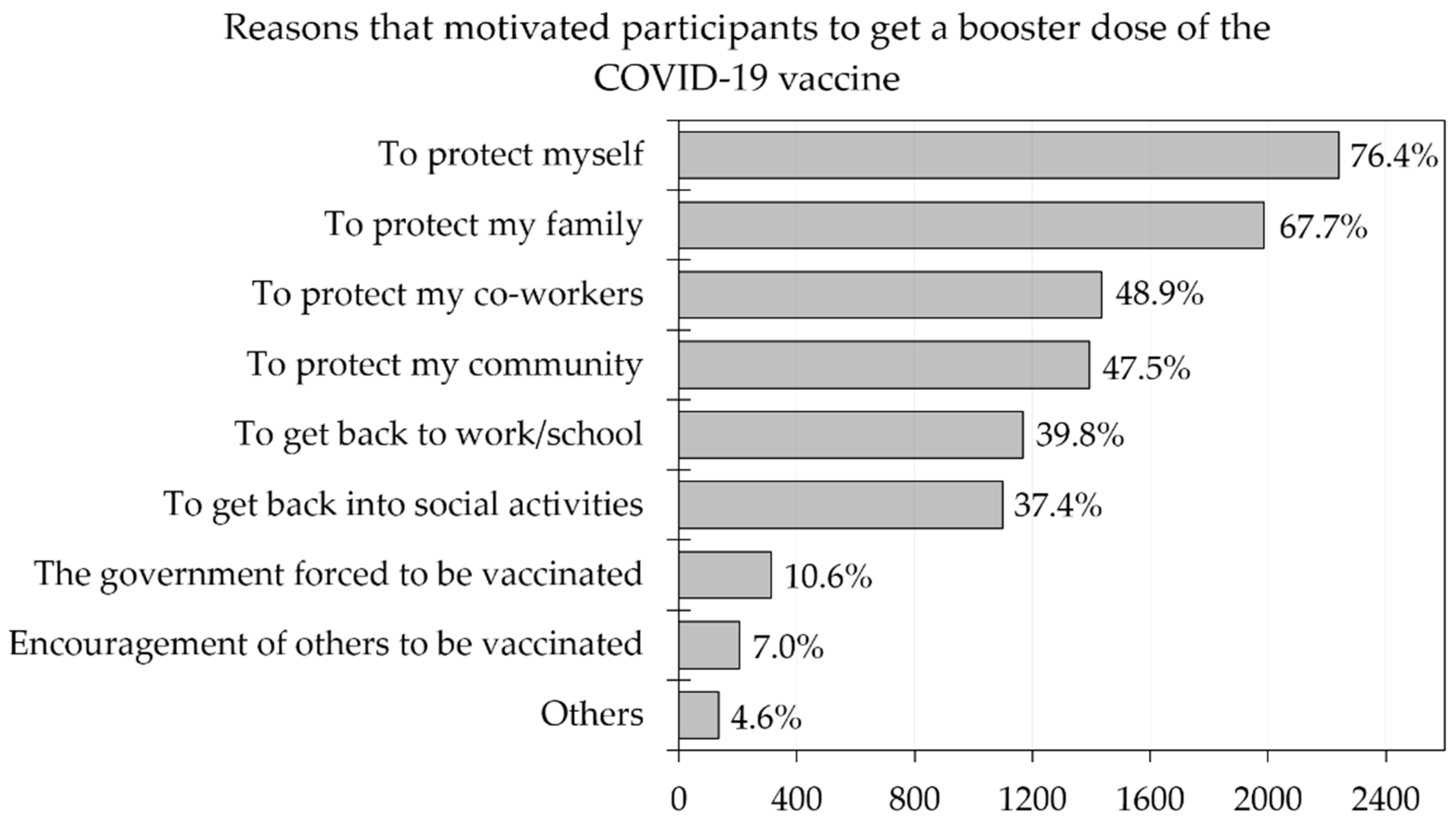
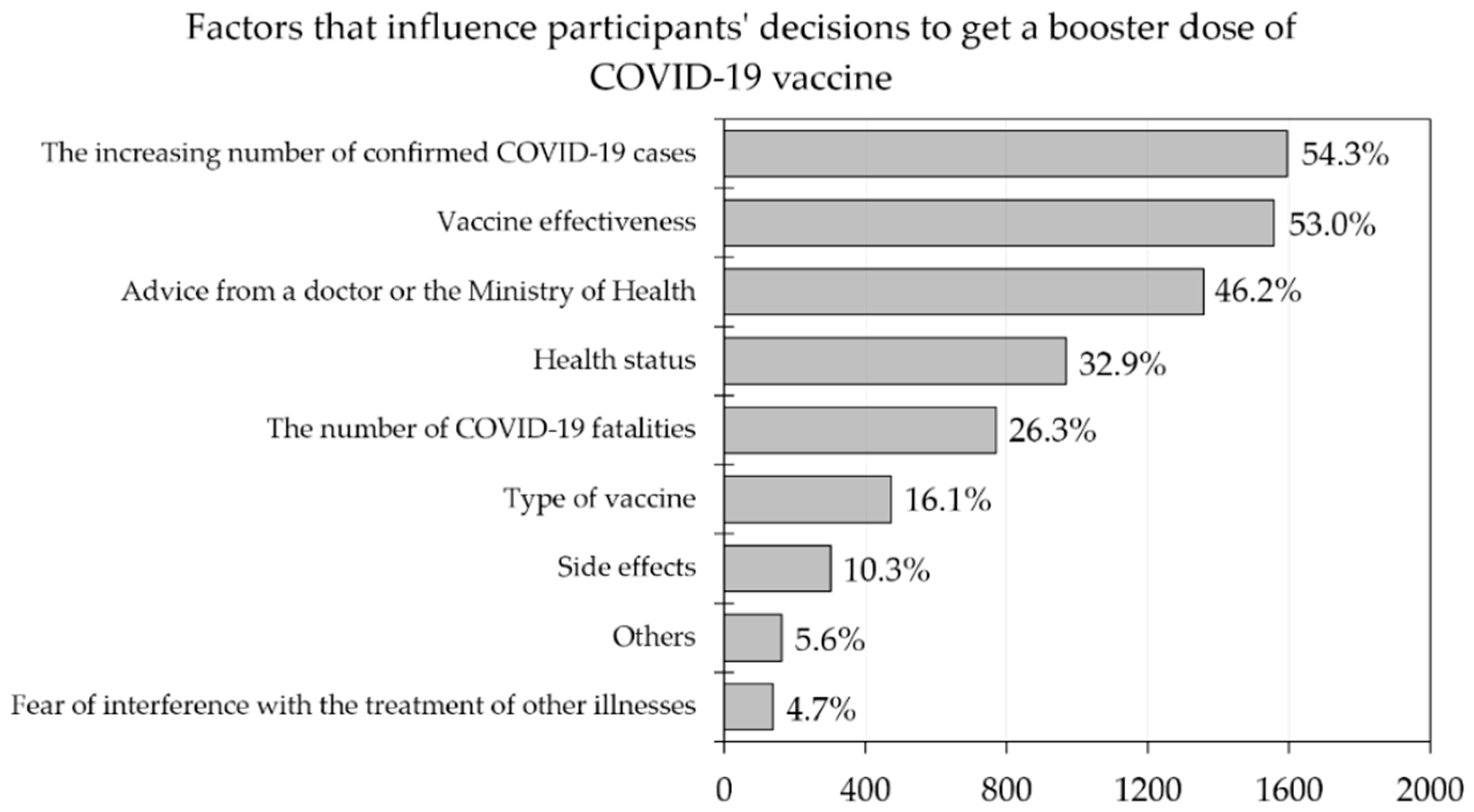
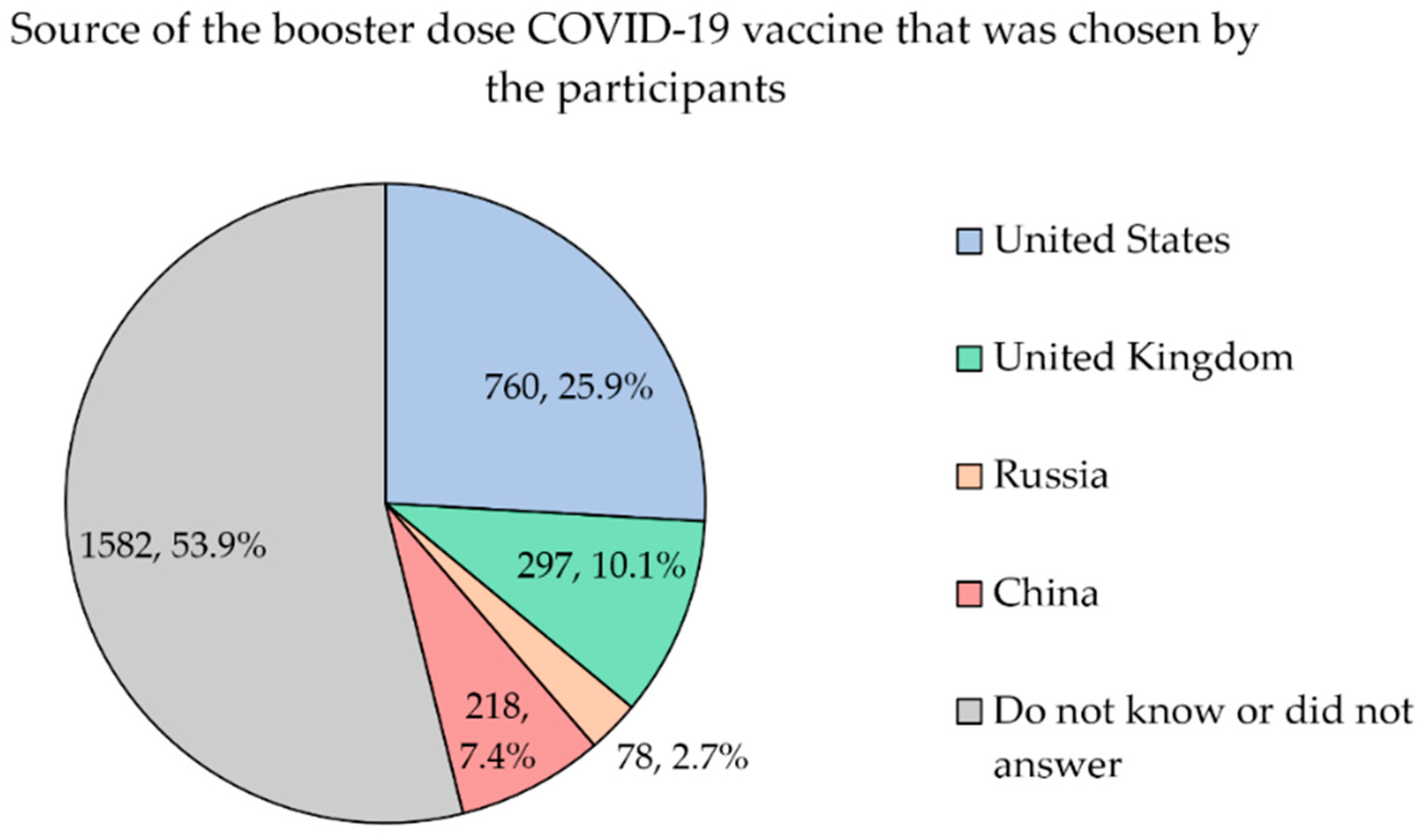
3.5. Motivations, Factors That Influence and Source of Vaccine Associated to Booster Dose Acceptance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard: Indonesia Situation. Available online: https://covid19.who.int/region/searo/country/id (accessed on 2 September 2022).
- COVID-19 Handling Task Force. The Situation of COVID-19 in Indonesia (Updated on 5 August 2022). Available online: https://covid19.go.id/artikel/2022/08/05/situasi-covid-19-di-indonesia-update-5-agustus-2022#main (accessed on 2 September 2022).
- Toharudin, T.; Pontoh, R.S.; Caraka, R.E.; Zahroh, S.; Kendogo, P.; Sijabat, N.; Sari, m.; Gio, P.; Basyuni, M.; Pardamean, B. National Vaccination and Local Intervention Impacts on COVID-19 Cases. Sustainability 2021, 13, 8282. [Google Scholar] [CrossRef]
- Lin, D.Y.; Gu, Y.; Wheeler, B.; Young, H.; Holloway, S.; Sunny, S.K.; Moore, Z.; Zeng, D. Effectiveness of COVID-19 Vaccines over a 9-Month Period in North Carolina. N. Engl. J. Med. 2022, 386, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef]
- Zhao, Y.M.; Liu, L.; Sun, J.; Yan, W.; Yuan, K.; Zheng, Y.B.; Lu, Z.A.; Liu, L.; Ni, S.Y.; Su, S.Z.; et al. Public Willingness and Determinants of COVID-19 Vaccination at the Initial Stage of Mass Vaccination in China. Vaccines 2021, 9, 1172. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 Vaccine Acceptance among Low- and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Bono, S.A.; Villela, E.F.d.M.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low- and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- He, J.; He, L. Knowledge of HPV and acceptability of HPV vaccine among women in western China: A cross-sectional survey. BMC Womens Health 2018, 18, 130. [Google Scholar] [CrossRef] [Green Version]
- Yeung, M.P.; Lam, F.L.; Coker, R. Factors associated with the uptake of seasonal influenza vaccination in adults: A systematic review. J. Public Health 2016, 38, 746–753. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Hassan, W.; Kazmi, S.K.; Tahir, M.J.; Ullah, I.; Royan, H.A.; Fahriani, M.; Nainu, F.; Rosa, S.G.V. Global acceptance and hesitancy of COVID-19 vaccination: A narrative review. Narra J. 2021, 1, e57. [Google Scholar] [CrossRef]
- Rosiello, D.; Anwar, S.; Yufika, A.; Adam, R.; Ismaeil, M.; Ismail, A.; Dahman, N.; Hafsi, M.; Ferjani, M.; Sami, F.; et al. Acceptance of COVID-19 vaccination at different hypothetical efficacy and safety levels in ten countries in Asia, Africa, and South America. Narra J. 2021, 1, e55. [Google Scholar] [CrossRef]
- Wagner, A.L.; Rajamoorthy, Y.; Taib, N.M. Impact of economic disruptions and disease experiences on COVID-19 vaccination uptake in Asia: A study in Malaysia. Narra J. 2021, 1, e42. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, R.M.; Al Shamsi, N.S. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE—An Observational Study. Front. Public Health 2022, 10, 876336. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.J.; Dutta, S.; Bhardwaj, P.; Charan, J.; Dhingra, S.; Mitra, P.; Singh, K.; Yadav, D.; Sharma, P.; Misra, S. Adverse events reported from COVID-19 vaccine trials: A systematic review. Indian J. Clin. Biochem. 2021, 36, 427–439. [Google Scholar] [CrossRef]
- Sangli, S.; Virani, A.; Cheronis, N.; Vannatter, B.; Minich, C.; Noronha, S.; Bhagavatula, R.; Speredelozzi, D.; Sareen, M.; Kaplan, R.B. Thrombosis with thrombocytopenia after the messenger RNA–1273 vaccine. Ann. Intern. Med. 2021, 174, 1480–1482. [Google Scholar] [CrossRef]
- Rodriguez, E.V.; Bouazza, F.-Z.; Dauby, N.; Mullier, F.; d’Otreppe, S.; Jissendi Tchofo, P.; Bartiaux, M.; Sirjacques, C.; Roman, A.; Hermans, C. Fatal vaccine-induced immune thrombotic thrombocytopenia (VITT) post Ad26. COV2. S: First documented case outside US. Infection 2022, 50, 531–536. [Google Scholar] [CrossRef]
- Franchini, M.; Testa, S.; Pezzo, M.; Glingani, C.; Caruso, B.; Terenziani, I.; Pognani, C.; Bellometti, S.A.; Castelli, G. Cerebral venous thrombosis and thrombocytopenia post-COVID-19 vaccination. Thromb. Res. 2021, 202, 182–183. [Google Scholar] [CrossRef]
- Jamme, M.; Mosnino, E.; Hayon, J.; Franchineau, G. Fatal cerebral venous sinus thrombosis after COVID-19 vaccination. Intensive Care Med. 2021, 47, 790. [Google Scholar] [CrossRef]
- Verma, A.K.; Lavine, K.J.; Lin, C.-Y. Myocarditis after COVID-19 mRNA vaccination. N. Engl. J. Med. 2021, 385, 1332–1334. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, S.; Seo, J.-W.; Kim, M.-j.; Jeon, Y.H.; Park, J.H.; Lee, J.K.; Yeo, N.S. Myocarditis-induced sudden death after BNT162b2 mRNA COVID-19 vaccination in Korea: Case report focusing on histopathological findings. J. Korean Med. Sci. 2021, 36, e286. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Permezel, F.; Borojevic, B.; Lau, S.; de Boer, H.H. Acute disseminated encephalomyelitis (ADEM) following recent Oxford/AstraZeneca COVID-19 vaccination. Forensic Sci. Med. Pathol. 2022, 18, 74–79. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Karasawa, S.; Ohashi, N.; Yamamoto, K. A case of encephalitis following COVID-19 vaccine. J. Infect. Chemother. 2022, 28, 975–977. [Google Scholar] [CrossRef]
- Fan, H.-T.; Lin, Y.-Y.; Chiang, W.-F.; Lin, C.-Y.; Chen, M.-H.; Wu, K.-A.; Chan, J.-S.; Kao, Y.-H.; Shyu, H.-Y.; Hsiao, P.-J. COVID-19 vaccine-induced encephalitis and status epilepticus. QJM Int. J. Med. 2022, 115, 91–93. [Google Scholar] [CrossRef]
- Schneider, J.; Sottmann, L.; Greinacher, A.; Hagen, M.; Kasper, H.-U.; Kuhnen, C.; Schlepper, S.; Schmidt, S.; Schulz, R.; Thiele, T. Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int. J. Leg. Med. 2021, 135, 2335–2345. [Google Scholar] [CrossRef]
- Sun, C.L.; Jaffe, E.; Levi, R. Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave. Sci. Rep. 2022, 12, 6978. [Google Scholar] [CrossRef]
- Maiese, A.; Baronti, A.; Manetti, A.C.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated? Vaccines 2022, 10, 308. [Google Scholar] [CrossRef]
- Wirawan, G.B.S.; Harjana, N.P.A.; Nugrahani, N.W.; Januraga, P.P. Health Beliefs and Socioeconomic Determinants of COVID-19 Booster Vaccine Acceptance: An Indonesian Cross-Sectional Study. Vaccines 2022, 10, 724. [Google Scholar] [CrossRef]
- Ministry of Health of Indonesian. Four Benefits of COVID-19 Vaccine That Are Rarely Known. Available online: https://upk.kemkes.go.id/new/4-manfaat-vaksin-covid-19-yang-wajib-diketahui (accessed on 14 September 2022).
- Tokiya, M.; Hara, M.; Matsumoto, A.; Ashenagar, M.S.; Nakano, T.; Hirota, Y. Acceptance of Booster COVID-19 Vaccine and Its Association with Components of Vaccination Readiness in the General Population: A Cross-Sectional Survey for Starting Booster Dose in Japan. Vaccines 2022, 10, 1102. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Yuan, Y.; Deng, Z.; Yin, D.; Shen, Q.; Zeng, J.; Xie, Y.; Xu, M.; Yang, M.; Jiang, S.; et al. Acceptance of COVID-19 booster vaccination based on the protection motivation theory: A cross-sectional study in China. J. Med. Virol. 2022, 94, 4115–4124. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Issa, J.; Hussain, S.; Tanasiewicz, M.; Wojtyczka, R.; Kubina, R.; Konwinska, M.D.; Riad, A. COVID-19 vaccine booster hesitancy (VBH) of healthcare professionals and students in Poland: Cross-sectional survey-based study. Front. Public Health 2022, 10, 938067. [Google Scholar] [CrossRef] [PubMed]
- Achrekar, G.C.; Batra, K.; Urankar, Y.; Batra, R.; Iqbal, N.; Choudhury, S.A.; Hooda, D.; Khan, R.; Arora, S.; Singh, A.; et al. Assessing COVID-19 Booster Hesitancy and Its Correlates: An Early Evidence from India. Vaccines 2022, 10, 1048. [Google Scholar] [CrossRef] [PubMed]
- Ittiwut, C.; Mahasirimongkol, S.; Srisont, S.; Ittiwut, R.; Chockjamsai, M.; Durongkadech, P.; Sawaengdee, W.; Khunphon, A.; Larpadisorn, K.; Wattanapokayakit, S.; et al. Genetic basis of sudden death after COVID-19 vaccination in Thailand. Heart Rhythm 2022, 19, 1874–1879. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Sun, Y.; Dai, H.; Wang, P.; Zhang, X.; Cui, D.; Huang, Y.; Zhang, J.; Xiang, T. Will People Accept a Third Booster Dose of the COVID-19 Vaccine? A Cross-Sectional Study in China. Front. Public Health 2022, 10, 914950. [Google Scholar] [CrossRef]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Aboualkasem, S.; Ebraiek, S.; Elwash, M.; Altarhouni, F.; Alzarrouk, F. Evaluation of COVID-19 Vaccines Side Effects among Staff and Students of Misurata University in Libya. J. Biota 2022, 8, 59–65. [Google Scholar] [CrossRef]
- McKee, C.; Bohannon, K. Exploring the Reasons Behind Parental Refusal of Vaccines. J. Pediatr. Pharm. 2016, 21, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Fredrickson, D.D.; Davis, T.C.; Arnould, C.L.; Kennen, E.M.; Hurniston, S.G.; Cross, J.T.; Bocchini, J. Childhood immunization refusal: Provider and parent perceptions. Fam. Med. 2004, 36, 431–439. [Google Scholar] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccin. Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saada, A.; Lieu, T.A.; Morain, S.R.; Zikmund-Fisher, B.J.; Wittenberg, E. Parents’ Choices and Rationales for Alternative Vaccination Schedules: A Qualitative Study. Clin. Pediatr. 2014, 54, 236–243. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E.F. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.; Teh, H.S.; Suah, J.L.; Husin, M.; Hwong, W.Y. SARS-CoV-2 in Malaysia: A surge of reinfection during the predominantly Omicron period. Lancet Reg. Health-West. Pac. 2022, 26, 100572. [Google Scholar] [CrossRef] [PubMed]
- Rani, M.D.M.; Mohamed, N.A.; Solehan, H.M.; Ithnin, M.; Ariffien, A.R.; Isahak, I. Assessment of acceptability of the COVID-19 vaccine based on the health belief model among Malaysians-A qualitative approach. PLoS ONE 2022, 17, e0269059. [Google Scholar] [CrossRef]
- Sarnoto, A.Z.; Hayatina, L. Polarization of the Muslim community towards government policies in overcoming the COVID-19 pandemic in Indonesia. Linguist. Cult. Rev. 2021, 5, 642–652. [Google Scholar] [CrossRef]
- Sauch Valmaña, G.; Fuster-Casanovas, A.; Ramírez-Morros, A.; Rodoreda Pallàs, B.; Vidal-Alaball, J.; Ruiz-Comellas, A.; Miró Catalina, Q. Motivation for Vaccination against COVID-19 in Persons Aged between 18 and 60 Years at a Population-Based Vaccination Site in Manresa (Spain). Vaccines 2022, 10, 597. [Google Scholar] [CrossRef]
- Abuhammad, S.; Khabour, O.F.; Alzoubi, K.H.; Hamaideh, S.; Alzoubi, B.A.; Telfah, W.S.; El-Zubi, F.K. The public’s attitude to and acceptance of periodic doses of the COVID-19 vaccine: A survey from Jordan. PLoS ONE 2022, 17, e0271625. [Google Scholar] [CrossRef]
- Oganesyan, N. Positive COVID-19 Messaging on TV Can Persuade Resistant Viewers, The Protector Coalition Says. 2021. Available online: https://variety.com/2021/tv/news/positive-tv-messaging-coronavirus-the-protector-coali-tion-1234885193 (accessed on 23 September 2022).
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Kemetrian Komunikasi dan Informasi Indonesia. Penggunaan Internet di Indonesia. Kemetrian Komunikasi dan Informasi Indonesia 2019. Available online: https://aptika.kominfo.go.id/2019/08/penggunaan-internet-di-indonesia/ (accessed on 23 September 2022).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number | Percentage |
|---|---|---|
| Gender | ||
| Male | 942 | 32.1 |
| Female | 1993 | 67.9 |
| Age (year) | ||
| ≤20 | 391 | 13.3 |
| 21–30 | 1406 | 47.9 |
| 31–40 | 758 | 25.8 |
| 41–50 | 226 | 7.7 |
| 51–60 | 118 | 4.0 |
| >60 | 36 | 1.2 |
| Marital status | ||
| Single | 1556 | 53.0 |
| Married | 1326 | 45.2 |
| Widow | 53 | 1.8 |
| Educational attainment | ||
| Elementary–Senior High School | 625 | 21.3 |
| Diploma | 1973 | 67.2 |
| Undergraduate/graduated | 337 | 11.5 |
| Religion | ||
| Islam | 2376 | 81.0 |
| Christian (Protestant) | 224 | 7.6 |
| Catholic | 162 | 5.5 |
| Other (Hindu/Buddha/Atheist or Agnostic/Confucian) | 173 | 5.9 |
| Occupation | ||
| Self-employed | 36 | 1.2 |
| Employed for wages | 1539 | 52.4 |
| Homemaker | 105 | 3.6 |
| Student or retired/unable to work/others | 1255 | 42.8 |
| Monthly household income (Indonesian Rupiah) | ||
| <3 million | 1638 | 55.8 |
| 3–5 million | 456 | 15.5 |
| 5–10 million | 530 | 18.1 |
| >10 million | 311 | 10.6 |
| Item | Number | Percentage |
|---|---|---|
| Had a family member seriously ill or who died from COVID-19? | ||
| Yes | 740 | 25.2 |
| No | 2195 | 74.8 |
| Had an influenza vaccine in the past 5 years? | ||
| Yes | 489 | 16.7 |
| No | 2446 | 83.3 |
| Have you ever been infected with COVID-19? | ||
| Yes | 1387 | 47.3 |
| No | 1548 | 52.7 |
| Type of COVID-19 vaccine received for the 1st dose | ||
| Sinovac | 2498 | 85.1 |
| AstraZeneca | 224 | 7.6 |
| Moderna | 90 | 3.1 |
| Pfizer | 77 | 2.6 |
| Sinopharm | 46 | 1.6 |
| Type of COVID-19 vaccine received for the 2nd dose | ||
| Sinovac | 2368 | 80.7 |
| AstraZeneca | 234 | 8.0 |
| Moderna | 165 | 5.6 |
| Pfizer | 113 | 3.9 |
| Sinopharm | 55 | 1.9 |
| Have you ever been infected with COVID-19 after getting vaccinated? | ||
| Yes | 849 | 28.9 |
| No | 1634 | 55.7 |
| Do not know | 452 | 15.4 |
| A booster dose can provide better immune than a second dose | ||
| Yes | 2389 | 81.4 |
| No | 57 | 1.9 |
| Not sure | 489 | 16.7 |
| A booster dose can stimulate antibody production to fight COVID-19 infection | ||
| Yes | 2546 | 86.7 |
| No | 42 | 1.4 |
| Not sure | 347 | 11.8 |
| A booster dose can lower hospitalization rate if infected by COVID-19 | ||
| Yes | 2481 | 84.5 |
| No | 80 | 2.7 |
| Not sure | 374 | 12.7 |
| A booster dose can protect the unvaccinated people | ||
| Yes | 2053 | 69.9 |
| No | 295 | 10.1 |
| Not sure | 587 | 20.0 |
| The COVID-19 pandemic has greatly affected my source of income | ||
| Agree or strongly agree | 2161 | 73.6 |
| Neither agree nor disagree | 663 | 22.6 |
| Disagree or strongly disagree | 111 | 3.8 |
| The COVID-19 pandemic has greatly affected my social life | ||
| Agree or strongly agree | 2591 | 88.3 |
| Neither agree nor disagree | 301 | 10.3 |
| Disagree or strongly disagree | 43 | 1.5 |
| My decision to be vaccinated with a booster dose was greatly influenced by the workplace during the pandemic | ||
| Agree or strongly agree | 2032 | 69.2 |
| Neither agree nor disagree | 632 | 21.5 |
| Disagree or strongly disagree | 271 | 9.2 |
| The booster dose is important to protect the public from COVID-19 | ||
| Yes | 2599 | 88.6 |
| No | 77 | 2.6 |
| Do not know | 259 | 8.8 |
| Pharmaceutical companies have developed a safe and effective booster dose COVID-19 vaccine | ||
| Yes | 2214 | 75.4 |
| No | 51 | 1.7 |
| Do not know | 670 | 22.8 |
| The government provides free booster vaccines for everyone | ||
| Yes | 2786 | 94.9 |
| No | 33 | 1.1 |
| Do not know | 116 | 4.0 |
| I believe that natural immunity is sufficient and I do not need to be vaccinated | ||
| Agree or strongly agree | 453 | 15.4 |
| Neither agree nor disagree | 558 | 19.0 |
| Disagree or strongly disagree | 1924 | 65.6 |
| COVID-19 infection is harmless, so I do not have to be vaccinated | ||
| Agree or strongly agree | 274 | 9.3 |
| Neither agree nor disagree | 302 | 10.3 |
| Disagree or strongly disagree | 2359 | 80.4 |
| My decision to be vaccinated with a booster dose was greatly influenced by the workplace during the pandemic | ||
| Agree or strongly agree | 1689 | 57.5 |
| Neither agree nor disagree | 761 | 25.9 |
| Disagree or strongly disagree | 485 | 16.5 |
| My decision to be vaccinated with a booster dose is strongly influenced by someone or family who lives with me at home | ||
| Agree or strongly agree | 1699 | 57.9 |
| Neither agree nor disagree | 694 | 23.6 |
| Disagree or strongly disagree | 542 | 18.5 |
| I am not sure vaccination is effective against COVID-19 | ||
| Agree or strongly agree | 482 | 16.4 |
| Neither agree nor disagree | 581 | 19.8 |
| Disagree or strongly disagree | 1872 | 63.8 |
| I am worried about any adverse side effects or allergic reactions when vaccinated with booster doses | ||
| Agree or strongly agree | 1675 | 57.1 |
| Neither agree nor disagree | 887 | 30.2 |
| Disagree or strongly disagree | 373 | 12.7 |
| I believe a booster dose of COVID-19 vaccine is very important | ||
| Agree or strongly agree | 2250 | 76.7 |
| Neither agree nor disagree | 608 | 20.7 |
| Disagree or strongly disagree | 77 | 2.6 |
| I believe optional vaccines and boosters, as a condition of travel, are necessary and useful | ||
| Agree or strongly agree | 2166 | 73.8 |
| Neither agree nor disagree | 525 | 17.9 |
| Disagree or strongly disagree | 244 | 8.3 |
| A booster dose is useful for protecting people from COVID-19 | ||
| Agree or strongly agree | 2390 | 81.4 |
| Neither agree nor disagree | 472 | 16.1 |
| Disagree or strongly disagree | 73 | 2.5 |
| A booster dose is safe | ||
| Agree or strongly agree | 2248 | 76.6 |
| Neither agree nor disagree | 627 | 21.4 |
| Disagree or strongly disagree | 60 | 2.0 |
| Complications may arise after receiving the booster dose | ||
| Agree or strongly agree | 424 | 14.4 |
| Neither agree nor disagree | 1170 | 39.9 |
| Disagree or strongly disagree | 1341 | 45.7 |
| I am worried about the unexpected side effect of booster dose in the future | ||
| Agree or strongly agree | 1189 | 40.5 |
| Neither agree nor disagree | 1057 | 36.0 |
| Disagree or strongly disagree | 689 | 23.5 |
| I believe the booster dose has good effectiveness | ||
| Agree or strongly agree | 2242 | 76.4 |
| Neither agree nor disagree | 641 | 21.8 |
| Disagree or strongly disagree | 52 | 1.8 |
| I believe the booster dose will be useful in protecting me from COVID-19 infection | ||
| Agree or strongly agree | 2318 | 79.0 |
| Neither agree nor disagree | 563 | 19.2 |
| Disagree or strongly disagree | 54 | 1.8 |
| I believe the benefits of the COVID-19 vaccine outweigh the risks | ||
| Agree or strongly agree | 2279 | 77.6 |
| Neither agree nor disagree | 601 | 20.5 |
| Disagree or strongly disagree | 55 | 1.9 |
| I believe if I get vaccinated, the risk of contracting COVID-19 or infecting others will be reduced | ||
| Agree or strongly agree | 2401 | 81.8 |
| Neither agree nor disagree | 463 | 15.8 |
| Disagree or strongly disagree | 71 | 2.4 |
| I am worried about the halal status of the new booster dose of COVID-19 vaccine | ||
| Agree or strongly agree | 1010 | 34.4 |
| Neither agree nor disagree | 1102 | 37.5 |
| Disagree or strongly disagree | 823 | 28.0 |
| Getting a booster dose vaccinated takes a lot of time and effort | ||
| Agree or strongly agree | 983 | 33.5 |
| Neither agree nor disagree | 1128 | 38.4 |
| Disagree or strongly disagree | 824 | 28.1 |
| Profile of the Vaccine | Number | Percentage |
|---|---|---|
| Acceptance of a booster dose of COVID-19 vaccine if it were provided freely by the government (without stating the efficacy or the safety) | ||
| Yes | 2758 | 93.9 |
| No | 117 | 6.1 |
| Acceptance of a booster dose of COVID-19 vaccine if it was 50% effective, with a 5% chance of side effects such as fever. | ||
| Yes | 1976 | 67.3 |
| No | 959 | 32.7 |
| Acceptance of a booster dose of COVID-19 vaccine if it was 95% effective, with a 20% chance of side effects such as fever. | ||
| Yes | 2032 | 69.2 |
| No | 903 | 30.8 |
| Acceptance of a booster dose of COVID-19 vaccine if it was 75% effective, with a 5% chance of side effects such as fever. | ||
| Yes | 2461 | 83.9 |
| No | 474 | 16.1 |
| Acceptance of a booster dose of COVID-19 vaccine if it was 75% effective, with a 20% chance of side effects such as fever. | ||
| Yes | 1477 | 50.3 |
| No | 1458 | 49.7 |
| Item | Number | Percentage | Acceptance Yes | Univariate | Multivariate | ||
|---|---|---|---|---|---|---|---|
| n (%) | OR 95%CI | p Value | OR 95%CI | p Value | |||
| Gender | |||||||
| Male | 942 | 32.1 | 880 (93.4) | 1 | |||
| Female | 1993 | 67.9 | 1878 (94.2) | 1.15 (0.84–1.58) | 0.389 | ||
| Age | |||||||
| ≤20 | 391 | 13.3 | 380 (97.2) | 3.30 (1.72–6.31) | <0.001 | 3.51 (1.30–9.46) | 0.013 |
| 21–30 | 1406 | 47.9 | 1327 (94.4) | 1.60 (1.14–2.25) | 0.007 | 1.96 (1.10–3.50) | 0.022 |
| 31–40 | 758 | 25.8 | 692 (91.3) | 1 | 1 | ||
| 41–50 | 226 | 7.7 | 211 (93.4) | 1.34 (0.75–2.40) | 0.322 | 1.76 (0.71–4.35) | 0.220 |
| 51–60 | 118 | 4.0 | 113 (95.8) | 2.16 (0.85–5.47) | 0.106 | 1.59 (0.40–6.31) | 0.508 |
| >60 | 36 | 1.2 | 35 (97.2) | 3.34 (0.45–24.76) | 0.238 | 1.79 (0.12–25.98) | 0.671 |
| Marital status | |||||||
| Single | 1556 | 53.0 | 1475 (94.8) | 1 | 1 | ||
| Married | 1326 | 45.2 | 1232 (92.9) | 0.72 (0.53–0.98) | 0.036 | 1.21 (0.69–2.13) | 0.514 |
| Widow | 53 | 1.8 | 51 (96.2) | 1.40 (0.34–5.85) | 0.645 | 1.55 (0.17–14.56) | 0.702 |
| Educational attainment | |||||||
| Elementary–Senior High School | 625 | 21.3 | 596 (95.4) | 1 | |||
| Diploma | 1973 | 67.2 | 1847 (93.6) | 0.71 (0.47–1.08) | 0.110 | ||
| Undergraduate/graduated | 337 | 11.5 | 315 (93.5) | 0.70 (0.39–1.23) | 0.215 | ||
| Religion | |||||||
| Islam | 2376 | 81.0 | 2208 (92.9) | 1 | 1 | ||
| Christian (Protestant) | 224 | 7.6 | 219 (97.8) | 3.33 (1.36–8.20) | 0.009 | 2.67 (0.86–8.31) | 0.091 |
| Catholic | 162 | 5.5 | 158 (97.5) | 3.01 (1.10–8.21) | 0.032 | 2.13 (0.57–7.99) | 0.262 |
| Other (Hindu/Buddha/Atheist or Agnostic/Confucian) | 173 | 5.9 | 173 (100.0) | 1 × 108 (0.00–NA) | 0.995 | 3 × 107 (0.00–NA) | 0.995 |
| Occupation | 2.51 (0.43–14.75) | 0.309 | |||||
| Self-employed | 36 | 1.2 | 33 (91.7) | 1.83 (0.50–6.74) | 0.362 | 2.57 (1.07–6.18) | 0.035 |
| Employed for wages | 1539 | 52.4 | 1450 (94.2) | 2.72 (1.51–4.88) | 0.001 | 1 | |
| Homemaker | 105 | 3.6 | 90 (85.7) | 1 | 1.89 (0.74–4.82) | 0.181 | |
| Student or retired/unable to work/others | 1255 | 42.8 | 1185 (94.4) | 12.82 (1.55–5.13) | 0.001 | ||
| Monthly household income (Indonesian Rupiah) | |||||||
| <3 million | 1638 | 55.8 | 1536 (93.8) | 1 | |||
| 3–5 million | 456 | 15.5 | 418 (91.7) | 0.73 (0.50–1.08) | 0.113 | ||
| 5–10 million | 530 | 18.1 | 507 (95.7) | 1.46 (0.92–2.33) | 0.107 | ||
| >10 million | 311 | 10.6 | 297 (95.5) | 1.41 (0.80–2.50) | 0.240 | ||
| Had a family member seriously ill or who died from COVID-19? | |||||||
| Yes | 740 | 25.2 | 706 (95.4) | 1.45 (0.99–2.12) | 0.059 | ||
| No (R) | 2195 | 74.8 | 2052 (93.5) | 1 | |||
| Had an influenza vaccine in the past 5 years? | |||||||
| Yes | 489 | 16.7 | 460 (94.1) | 1.02 (0.68–1.54) | 0.919 | ||
| No (R) | 2446 | 83.3 | 2298 (93.9) | 1 | |||
| Have ever been infected with COVID-19? | |||||||
| Yes | 1387 | 47.3 | 1322 (95.3) | 1.59 (1.16–2.17) | 0.004 | 1.25 (0.74–2.10) | 0.403 |
| No (R) | 1548 | 52.7 | 1436 (92.8) | 1 | 1 | ||
| Type of COVID-19 vaccine you received for the 1st dose | |||||||
| Sinovac (R) | 2498 | 85.1 | 2362 (94.6) | 1 | 1 | ||
| AstraZeneca | 224 | 7.6 | 209 (93.3) | 0.81 (0.46–1.39) | 0.434 | 0.30 (0.08–1.05) | 0.059 |
| Moderna | 90 | 3.1 | 83 (92.2) | 0.68 (0.31–1.51) | 0.344 | 2.58 (0.64–10.40) | 0.183 |
| Pfizer | 77 | 2.6 | 62 (80.5) | 0.24 (0.13–0.43) | <0.001 | 0.43 (0.09–2.10) | 0.296 |
| Sinopharm | 46 | 1.6 | 42 (91.3) | 0.61 (0.21–1.71) | 0.343 | 0.08 (0.01–0.68) | 0.020 |
| Type of COVID-19 vaccine you received for the 2nd dose | |||||||
| Sinovac (R) | 2368 | 80.7 | 2240 (94.6) | 1 | 1 | ||
| AstraZeneca | 234 | 8.0 | 226 (96.6) | 1.61 (0.78–3.34) | 0.197 | 7.72 (1.84–32.42) | 0.005 |
| Moderna | 165 | 5.6 | 146 (88.5) | 0.44 (0.26–0.73) | 0.002 | 0.40 (0.15–1.06) | 0.067 |
| Pfizer | 113 | 3.9 | 95 (84.1) | 0.30 (0.18–0.52) | <0.001 | 1.44 (0.35–5.95) | 0.617 |
| Sinopharm | 55 | 1.9 | 51 (92.7) | 0.73 (0.26–2.05) | 0.548 | 7.38 (0.81–67.30) | 0.076 |
| Have you ever been infected with COVID-19 after getting vaccinated? | |||||||
| Yes (R) | 849 | 28.9 | 821 (96.7) | 1 | 1 | ||
| No | 1634 | 55.7 | 1560 (95.5) | 0.72 (0.46–1.12) | 0.144 | 0.82 (0.41–1.63) | 0.563 |
| Do not know | 452 | 15.4 | 377 (83.4) | 0.17 (0.11–0.27) | <0.001 | 0.42 (0.21–0.86) | 0.018 |
| A booster dose can provide better immune than a second dose | |||||||
| Yes (R) | 2389 | 81.4 | 2329 (97.5) | 1 | 1 | ||
| No | 57 | 1.9 | 37 (64.9) | 0.05 (0.03–0.09) | <0.001 | 0.91 (0.28–2.97) | 0.877 |
| Not sure | 489 | 16.7 | 392 (80.2) | 0.10 (0.07–0.15) | <0.001 | 0.74 (0.38–1.47) | 0.393 |
| A booster dose can stimulate antibody production to fight COVID-19 | |||||||
| Yes (R) | 2546 | 86.7 | 2476 (97.3) | 1 | 1 | ||
| No | 42 | 1.4 | 24 (57.1) | 0.04 (0.02–0.07) | <0.001 | 0.34 (0.09–1.27) | 0.109 |
| Not sure | 347 | 11.8 | 258 (74.4) | 0.08 (0.06–0.12) | <0.001 | 0.77 (0.37–1.58) | 0.469 |
| A booster dose can lower hospitalization rate if infected by COVID-19 | |||||||
| Yes (R) | 2481 | 84.5 | 2415 (97.3) | 1 | 1 | ||
| No | 80 | 2.7 | 64 (80.0) | 0.11 (0.06–0.20) | <0.001 | 0.88 (0.29–2.62) | 0.816 |
| Not sure | 374 | 12.7 | 279 (74.6) | 0.08 (0.06–0.11) | <0.001 | 0.69 (0.35–1.34) | 0.268 |
| A booster dose can protect the unvaccinated people | |||||||
| Yes (R) | 2053 | 69.9 | 1994 (97.1) | 1 | 1 | ||
| No | 295 | 10.1 | 267 (90.5) | 0.28 (0.18–0.45) | <0.001 | 0.81 (0.39–1.69) | 0.579 |
| Not sure | 587 | 20.0 | 497 (84.7) | 0.16 (0.12–0.23) | <0.001 | 1.33 (0.72–2.46) | 0.371 |
| The COVID-19 pandemic has greatly affected my source of income | |||||||
| Agree or strongly agree | 2161 | 73.6 | 2042 (94.5) | 2.08 (1.11–3.89) | 0.022 | 1.21 (0.41–3.57) | 0.731 |
| Neither agree nor disagree | 663 | 22.6 | 617 (93.1) | 1.63 (0.83–3.18) | 0.155 | 1.28 (0.42–3.92) | 0.665 |
| Disagree or strongly disagree (R) | 111 | 3.8 | 99 (89.2) | 1 | 1 | ||
| The COVID-19 pandemic has greatly affected my social life | |||||||
| Agree or strongly agree | 2591 | 88.3 | 2454 (94.7) | 5.43 (2.62–11.24) | <0.001 | 2.04 (0.47–8.84) | 0.340 |
| Neither agree nor disagree | 301 | 10.3 | 271 (90.0) | 2.74 (1.23–6.10) | 0.014 | 1.12 (0.24–5.16) | 0.889 |
| Disagree or strongly disagree (R) | 43 | 1.5 | 33 (76.7) | 1 | 1 | ||
| My decision to be vaccinated with a booster dose was greatly influenced by the workplace during the pandemic | |||||||
| Agree or strongly agree | 2032 | 69.2 | 1926 (94.8) | 1.53 (0.94–2.48) | 0.088 | ||
| Neither agree nor disagree | 632 | 21.5 | 582 (92.1) | 0.98 (0.58–1.66) | 0.934 | ||
| Disagree or strongly disagree (R) | 271 | 9.2 | 250 (92.3) | 1 | |||
| The booster dose is important to protect the public from COVID-19 | |||||||
| Yes | 2599 | 88.6 | 2531 (97.4) | 38.20 (23.00–63.46) | <0.001 | 3.17 (1.34–7.50) | 0.009 |
| No (R) | 77 | 2.6 | 38 (49.4) | 1 | 1 | ||
| Do not know | 259 | 8.8 | 189 (73.0) | 2.77 (1.64–4.68) | <0.001 | 3.02 (1.28–7.16) | 0.012 |
| Pharmaceutical companies have developed a safe and effective booster dose of COVID-19 vaccine | |||||||
| Yes | 2214 | 75.4 | 2166 (97.8) | 26.79 (14.19–50.59) | <0.001 | 0.79 (0.25–2.54) | 0.691 |
| No (R) | 51 | 1.7 | 32 (62.7) | 1 | 1 | ||
| Do not know | 670 | 22.8 | 560 (83.6) | 3.02 (1.65–5.53) | <0.001 | 0.55 (0.18–1.66) | 0.285 |
| I believe that natural immunity is sufficient and I do not need to be vaccinated | |||||||
| Agree or strongly agree | 453 | 15.4 | 367 (81.0) | 0.08 (0.05–0.12) | <0.001 | 0.43 (0.23–0.83) | 0.011 |
| Neither agree nor disagree | 558 | 19.0 | 502 (90.0) | 0.17 (0.11–0.26) | <0.001 | 0.95 (0.51–1.77) | 0.872 |
| Disagree or strongly disagree (R) | 1924 | 65.6 | 1889 (98.2) | 1 | 1 | ||
| COVID-19 infection is harmless, so I do not have to be vaccinated | |||||||
| Agree or strongly agree | 274 | 9.3 | 225 (82.1) | 0.13 (0.09–0.19) | <0.001 | 0.62 (0.30–1.28) | 0.195 |
| Neither agree nor disagree | 302 | 10.3 | 239 (79.1) | 0.11 (0.07–0.16) | <0.001 | 0.65 (0.36–1.15) | 0.137 |
| Disagree or strongly disagree (R) | 2359 | 80.4 | 2294 (97.2) | 1 | 1 | ||
| My decision to be vaccinated with a booster dose was greatly influenced by the workplace during the pandemic | |||||||
| Agree or strongly agree | 1689 | 57.5 | 1586 (93.9) | 0.80 (0.51–1.27) | 0.342 | ||
| Neither agree nor disagree | 761 | 25.9 | 711 (93.4) | 0.74 (0.45–1.22) | 0.239 | ||
| Disagree or strongly disagree (R) | 485 | 16.5 | 461 (95.1) | 1 | |||
| My decision to be vaccinated with a booster dose is strongly influenced by someone or family who lives with me at home | |||||||
| Agree or strongly agree | 1699 | 57.9 | 1637 (96.4) | 2.39 (1.61–3.56) | <0.001 | 1.80 (0.99–3.28) | 0.055 |
| Neither agree nor disagree | 694 | 23.6 | 624 (89.9) | 0.81 (0.54–1.20) | 0.285 | 1.51 (0.82–2.77) | 0.188 |
| Disagree or strongly disagree (R) | 542 | 18.5 | 497 (91.7) | 1 | 1 | ||
| I’m not sure vaccination is effective against COVID-19 | |||||||
| Agree or strongly agree | 482 | 16.4 | 400 (83.0) | 0.08 (0.05–0.12) | <0.001 | 0.42 (0.21–0.83) | 0.012 |
| Neither agree nor disagree | 581 | 19.8 | 515 (88.6) | 0.12 (0.08–0.19) | <0.001 | 0.46 (0.24–0.87) | 0.017 |
| Disagree or strongly disagree (R) | 1872 | 63.8 | 1843 (98.5) | 1 | 1 | ||
| I am worried about any adverse side effects or allergic reactions when vaccinated with booster doses | |||||||
| Agree or strongly agree | 1675 | 57.1 | 1534 (91.6) | 0.30 (0.16–0.58) | <0.001 | 1.19 (0.40–3.57) | 0.754 |
| Neither agree nor disagree | 887 | 30.2 | 861 (97.1) | 0.91 (0.44–1.91) | 0.808 | 1.63 (0.52–5.09) | 0.401 |
| Disagree or strongly disagree (R) | 373 | 12.7 | 363 (97.3) | 1 | 1 | ||
| I believe a booster dose of COVID-19 vaccine is very important | |||||||
| Agree or strongly agree | 2250 | 76.7 | 2215 (98.4) | 93.91 (53.39–165.18) | <0.001 | 5.54 (1.90–16.15) | 0.002 |
| Neither agree nor disagree | 608 | 20.7 | 512 (84.2) | 7.91 (4.78–13.11) | <0.001 | 2.46 (0.97–6.20) | 0.057 |
| Disagree or strongly disagree (R) | 77 | 2.6 | 31 (40.3) | 1 | 1 | ||
| I believe optional vaccines and boosters as a condition of travel, are necessary and useful | |||||||
| Agree or strongly agree | 2166 | 73.8 | 2102 (97.0) | 10.47 (7.13–15.38) | <0.001 | 0.76 (0.39–1.48) | 0.413 |
| Neither agree nor disagree | 525 | 17.9 | 471 (89.7) | 2.78 (1.85–4.18) | <0.001 | 1.14 (0.61–2.15) | 0.680 |
| Disagree or strongly disagree (R) | 244 | 8.3 | 185 (75.8) | 1 | 1 | ||
| A booster vaccines are useful for protecting people from COVID-19 | |||||||
| Agree or strongly agree | 2390 | 81.4 | 2342 (98.0) | 55.97 (32.57–96.18) | <0.001 | 0.78 (0.24–2.59) | 0.685 |
| Neither agree nor disagree | 472 | 16.1 | 382 (80.9) | 4.87 (2.91–8.14) | <0.001 | 0.86 (0.29–2.57) | 0.791 |
| Disagree or strongly disagree (R) | 73 | 2.5 | 34 (46.6) | 1 | 1 | ||
| A booster vaccine is safe | |||||||
| Agree or strongly agree | 2248 | 76.6 | 2207 (98.2) | 57.54 (31.80–104.13) | <0.001 | 2.74 (0.97–7.76) | 0.057 |
| Neither agree nor disagree | 627 | 21.4 | 522 (83.3) | 5.31 (3.07–9.19) | <0.001 | 1.79 (0.69–4.61) | 0.231 |
| Disagree or strongly disagree (R) | 60 | 2.0 | 29 (48.3) | 1 | 1 | ||
| Serious complications will arise after getting the COVID-19 booster vaccine | |||||||
| Agree or strongly agree | 424 | 14.4 | 379 (89.4) | 0.19 (0.12–0.31) | <0.001 | 1.32 (0.61–2.84) | 0.479 |
| Neither agree nor disagree | 1170 | 39.9 | 1068 (91.3) | 0.24 (0.16–0.36) | <0.001 | 1.07 (0.57–2.04) | 0.830 |
| Disagree or strongly disagree (R) | 1341 | 45.7 | 1311 (97.8) | 1 | 1 | ||
| I am worried about the unexpected effect of the booster dose in the future | |||||||
| Agree or strongly agree | 1189 | 40.5 | 1071 (90.1) | 0.12 (0.06–0.24) | <0.001 | 0.67 (0.23–1.93) | 0.456 |
| Neither agree nor disagree | 1057 | 36.0 | 1007 (95.3) | 0.27 (0.13–0.55) | <0.001 | 0.61 (0.21–1.75) | 0.360 |
| Disagree or strongly disagree (R) | 689 | 23.5 | 680 (98.7) | 1 | 1 | ||
| I believe the booster dose will have good effectiveness | |||||||
| Agree or strongly agree | 2242 | 76.4 | 2205 (98.3) | 69.53 (36.86–131.16) | <0.001 | 0.39 (0.06–2.40) | 0.310 |
| Neither agree nor disagree | 641 | 21.8 | 529 (82.5) | 5.51 (3.08–9.86) | <0.001 | 0.31 (0.06–1.60) | 0.162 |
| Disagree or strongly disagree (R) | 52 | 1.8 | 24 (46.2) | 1 | 1 | ||
| I believe the COVID-19 booster dose vaccine will be useful in protecting me from COVID-19 infection | |||||||
| Agree or strongly agree | 2318 | 79.0 | 2272 (98.0) | 98.78 (52.26–186.71) | <0.001 | 3.29 (0.53–20.45) | 0.201 |
| Neither agree nor disagree | 563 | 19.2 | 468 (83.1) | 9.85 (5.37–18.08) | <0.001 | 4.52 (0.83–24.66) | 0.081 |
| Disagree or strongly disagree (R) | 54 | 1.8 | 18 (33.3) | 1 | 1 | ||
| I believe the benefits of COVID-19 vaccine outweigh the risks | |||||||
| Agree or strongly agree | 2279 | 77.6 | 2239 (98.2) | 90.63 (48.39–169.72) | <0.001 | 2.45 (0.67–8.89) | 0.173 |
| Neither agree nor disagree | 601 | 20.5 | 498 (82.9) | 7.83 (4.37–14.04) | <0.001 | 1.20 (0.36–4.00) | 0.766 |
| Disagree or strongly disagree (R) | 55 | 1.9 | 21 (38.2) | 1 | 1 | ||
| I believe that if I get vaccinated, the risk of contracting COVID-19 or infecting others will be reduced | |||||||
| Agree or strongly agree | 2401 | 81.8 | 2348 (97.8) | 34.33 (19.96–59.05) | <0.001 | 0.87 (0.26–2.94) | 0.820 |
| Neither agree nor disagree | 463 | 15.8 | 370 (79.9) | 3.08 (1.83–5.19) | <0.001 | 0.87 (0.27–2.75) | 0.809 |
| Disagree or strongly disagree (R) | 71 | 2.4 | 40 (56.3) | 1 | 1 | ||
| I am worried about the halal status of the new booster dose of the COVID-19 vaccine | |||||||
| Agree or strongly agree | 1010 | 34.4 | 910 (90.1) | 0.20 (0.12–0.34) | <0.001 | 1.56 (0.71–3.45) | 0.270 |
| Neither agree nor disagree | 1102 | 37.5 | 1043 (94.6) | 0.40 (0.23–0.68) | 0.001 | 1.75 (0.79–3.88) | 0.171 |
| Disagree or strongly disagree (R) | 823 | 28.0 | 805 (97.8) | 1 | 1 | ||
| Having a booster dose takes a lot of time and effort | |||||||
| Agree or strongly agree | 983 | 33.5 | 922 (93.8) | 0.57 (0.37–0.89) | 0.014 | 0.98 (0.50–1.93) | 0.958 |
| Neither agree nor disagree | 1128 | 38.4 | 1042 (92.4) | 0.46 (0.30–0.70) | <0.001 | 1.12 (0.57–2.19) | 0.739 |
| Disagree or strongly disagree (R) | 824 | 28.1 | 794 (96.4) | 1 | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harapan, H.; Fathima, R.; Kusuma, H.I.; Anwar, S.; Nalapraya, W.Y.; Wibowo, A.; Wati, K.D.K.; Medina, A.; Defrita, A.H.; Astri, Y.; et al. Drivers of and Barriers to COVID-19 Vaccine Booster Dose Acceptance in Indonesia. Vaccines 2022, 10, 1981. https://doi.org/10.3390/vaccines10121981
Harapan H, Fathima R, Kusuma HI, Anwar S, Nalapraya WY, Wibowo A, Wati KDK, Medina A, Defrita AH, Astri Y, et al. Drivers of and Barriers to COVID-19 Vaccine Booster Dose Acceptance in Indonesia. Vaccines. 2022; 10(12):1981. https://doi.org/10.3390/vaccines10121981
Chicago/Turabian StyleHarapan, Harapan, Raisha Fathima, Hendrix Indra Kusuma, Samsul Anwar, Widhy Yudistira Nalapraya, Adityo Wibowo, Ketut Dewi Kumara Wati, Ayunda Medina, Anna Hanifa Defrita, Yesi Astri, and et al. 2022. "Drivers of and Barriers to COVID-19 Vaccine Booster Dose Acceptance in Indonesia" Vaccines 10, no. 12: 1981. https://doi.org/10.3390/vaccines10121981
APA StyleHarapan, H., Fathima, R., Kusuma, H. I., Anwar, S., Nalapraya, W. Y., Wibowo, A., Wati, K. D. K., Medina, A., Defrita, A. H., Astri, Y., Prasetyowati, A., Nurfarahin, N., Khusna, A., Oktariana, S., Anwar, S., Yussar, M. O., Khotimah, S., Nainggolan, B. W. M., Badri, P. R. A., ... Mudatsir, M. (2022). Drivers of and Barriers to COVID-19 Vaccine Booster Dose Acceptance in Indonesia. Vaccines, 10(12), 1981. https://doi.org/10.3390/vaccines10121981