
Parent Acceptance toward Inactivated COVID-19 Vaccination in Children with Acute Lymphoblastic Leukemia: The Power of Oncologist and Alliance

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Enrollment
2.2. Patient Follow-Up and Instrument Evaluation
2.3. Statistical Analysis
3. Results
3.1. Demographic and Oncological Information
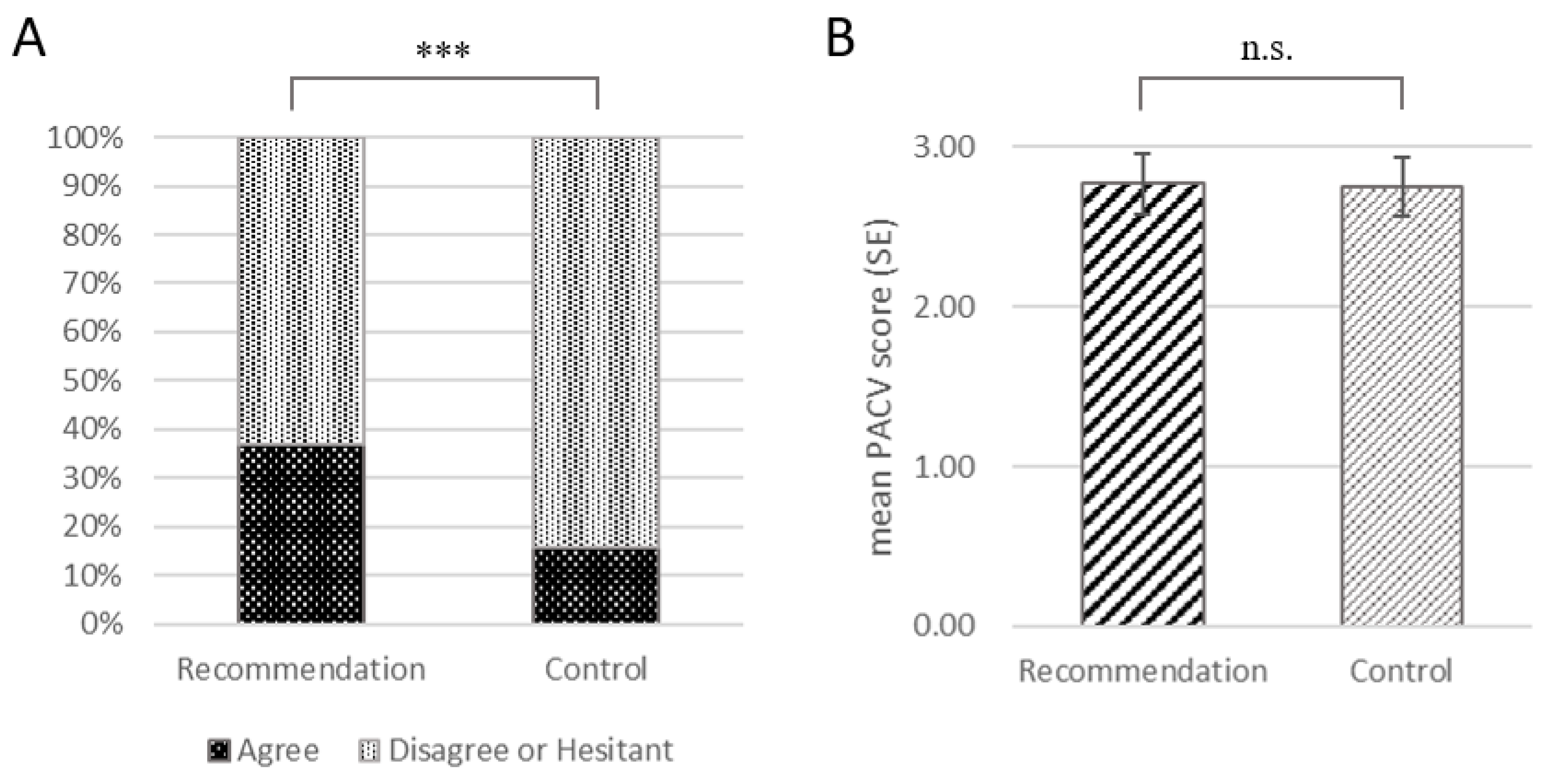
3.2. Oncologist Recommendation Increases COVID-19 Vaccination Willingness
3.3. Parent–Oncologist Alliance Affects Recommendation Strength
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; He, J. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Wanga, V.; Gerdes, M.E.; Shi, D.S.; Choudhary, R.; Dulski, T.M.; Hsu, S.; Idubor, O.I.; Webber, B.J.; Wendel, A.M.; Agathis, N.T.; et al. Characteristics and Clinical Outcomes of Children and Adolescents Aged <18 Years Hospitalized with COVID-19—Six Hospitals, United States, July-August 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1766–1772. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Song, Y.; Li, C.; Yang, W.; Ma, Q.; Jiang, Z.; Li, M.; Lian, X.; Jiao, W.; Wang, L.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: A double-blind, randomised, controlled, phase 1/2 clinical trial. Lancet. Infect. Dis. 2021, 21, 1645–1653. [Google Scholar] [CrossRef]
- Mohseni Afshar, Z.; Babazadeh, A.; Janbakhsh, A.; Mansouri, F.; Sio, T.T.; Sullman, M.J.M.; Carson-Chahhoud, K.; Hosseinzadeh, R.; Barary, M.; Ebrahimpour, S. Coronavirus disease 2019 (Covid-19) vaccination recommendations in special populations and patients with existing comorbidities. Rev. Med. Virol. 2021, 32, e2309. [Google Scholar] [CrossRef]
- Ryan, A.L.; Wadia, U.D.; Jacoby, P.; Cheung, L.C.; Kerr, F.; Fraser, C.; Tapp, H.; Mechinaud, F.; Carolan, L.A.; Laurie, K.L.; et al. Immunogenicity of the inactivated influenza vaccine in children who have undergone allogeneic haematopoietic stem cell transplant. Bone Marrow Transpl. 2020, 55, 773–779. [Google Scholar] [CrossRef]
- Kotecha, R.S. COVID-19 vaccination for children with cancer. Pediatr. Blood Cancer 2022, 69, e29340. [Google Scholar] [CrossRef]
- Mark, C.; Gupta, S.; Punnett, A.; Upton, J.; Orkin, J.; Atkinson, A.; Clarke, L.; Heisey, A.; McGovern, C.; Alexander, S. Safety of administration of BNT162b2 mRNA (Pfizer-BioNTech) COVID-19 vaccine in youths and young adults with a history of acute lymphoblastic leukemia and allergy to PEG-asparaginase. Pediatr. Blood Cancer 2021, 68, e29295. [Google Scholar] [CrossRef]
- Choi, D.K.; Strzepka, J.T.; Hunt, S.R.; Tannenbaum, V.L.; Jang, I.E. Vaccination in pediatric cancer survivors: Vaccination rates, immune status, and knowledge regarding compliance. Pediatr. Blood Cancer 2020, 67, e28565. [Google Scholar] [CrossRef]
- Peng, X.; Gao, P.; Wang, Q.; Wu, H.G.; Yan, Y.L.; Xia, Y.; Wang, J.Y.; Lu, F.; Pan, H.; Yang, Y.; et al. Prevalence and Impact Factors of COVID-19 Vaccination Hesitancy Among Breast Cancer Survivors: A Multicenter Cross-Sectional Study in China. Front. Med. 2021, 8, 741204. [Google Scholar] [CrossRef]
- Chirico, I.; Andrei, F.; Salvatori, P.; Malaguti, I.; Trombini, E. The Focal Play Therapy: An Empirical Study on the Parent-Therapist Alliance, Parent-Child Interactions and Parenting Stress in a Clinical Sample of Children and Their Parents. Int. J. Environ. Res. Public Health 2020, 17, 8379. [Google Scholar] [CrossRef] [PubMed]
- Sønsterud, H.; Kirmess, M.; Howells, K.; Ward, D.; Feragen, K.B.; Halvorsen, M.S. The working alliance in stuttering treatment: A neglected variable? Int. J. Lang. Commun. Disord. 2019, 54, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Peng, H.; Song, X.; Xu, C.; Zhang, M. Using AI chatbots to provide self-help depression interventions for university students: A randomized trial of effectiveness. Internet Interv. 2022, 27, 100495. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.L.; Huang, Z.; Ren, J.; Laffoon, M.; Ji, M.; Pinckney, L.C.; Sun, X.; Prosser, L.A.; Boulton, M.L.; Zikmund-Fisher, B.J. Vaccine Hesitancy and Concerns About Vaccine Safety and Effectiveness in Shanghai, China. Am. J. Prev. Med. 2021, 60, S77–S86. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Pan, F.; Zhao, H.; Nicholas, S.; Maitland, E.; Liu, R.; Hou, Q. Parents’ Decisions to Vaccinate Children against COVID-19: A Scoping Review. Vaccines 2021, 9, 1476. [Google Scholar] [CrossRef]
- Luxi, N.; Giovanazzi, A.; Capuano, A.; Crisafulli, S.; Cutroneo, P.M.; Fantini, M.P.; Ferrajolo, C.; Moretti, U.; Poluzzi, E.; Raschi, E.; et al. COVID-19 Vaccination in Pregnancy, Paediatrics, Immunocompromised Patients, and Persons with History of Allergy or Prior SARS-CoV-2 Infection: Overview of Current Recommendations and Pre- and Post-Marketing Evidence for Vaccine Efficacy and Safety. Drug Saf. 2021, 44, 1247–1269. [Google Scholar] [CrossRef]
- Suran, M. Why Parents Still Hesitate to Vaccinate Their Children Against COVID-19. Jama 2022, 327, 23–25. [Google Scholar] [CrossRef]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; Shah, N.; Gerhardt, C.A. Factors affecting COVID-19 vaccine hesitancy in parents of children with cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef]
- Wimberly, C.E.; Towry, L.; Davis, E.; Johnston, E.E.; Walsh, K.M. SARS-CoV-2 vaccine acceptability among caregivers of childhood cancer survivors. Pediatr. Blood Cancer 2021, 69, e29443. [Google Scholar] [CrossRef]
- Esposito, S.; Cecinati, V.; Brescia, L.; Principi, N. Vaccinations in children with cancer. Vaccine 2010, 28, 3278–3284. [Google Scholar] [CrossRef] [PubMed]
- Wimberly, C.E.; Towry, L.; Caudill, C.; Johnston, E.E.; Walsh, K.M. Impacts of COVID-19 on caregivers of childhood cancer survivors. Pediatr. Blood Cancer 2021, 68, e28943. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Xu, W.; Liang, Z.; Li, Y.; Yu, H.; Yang, C.; Li, J.; Liang, S.; Liu, T.; Xiao, J. Patient-oncologist alliance and psychosocial well-being in Chinese society strongly affect cancer management adherence with cancer of unknown primary. Psycho. Oncol. 2017, 26, 991–998. [Google Scholar] [CrossRef]
- Trevino, K.M.; Maciejewski, P.K.; Epstein, A.S.; Prigerson, H.G. The lasting impact of the therapeutic alliance: Patient-oncologist alliance as a predictor of caregiver bereavement adjustment. Cancer 2015, 121, 3534–3542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temsah, M.H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- WHO. Weekly Epidemiological COVID-19. 6 July 2021 Edition 47. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19%2D%2D-6-july-2021 (accessed on 11 July 2021).
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Williamson, E.J.; I McDonald, H.; Bhaskaran, K.; Walker, A.J.; Bacon, S.; Davy, S.; Schultze, A.; Tomlinson, L.; Bates, C.; Ramsay, M.; et al. Risks of covid-19 hospital admission and death for people with learning disability: Population based cohort study using the OpenSAFELY platform. BMJ 2021, 374, n1592. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Tizazu, A.M.; Mengist, H.M.; Demeke, G. Aging, inflammaging and immunosenescence as risk factors of severe COVID-19. Immun. Ageing 2022, 19, 53. [Google Scholar] [CrossRef] [PubMed]
- Cook, L.B.; O’Dell, G.; Vourvou, E.; Palanicawandar, R.; Marks, S.; Milojkovic, D.; Apperley, J.F.; Loaiza, S.; Claudiani, S.; Bua, M.; et al. Third primary SARS-CoV-2 mRNA vaccines enhance antibody responses in most patients with haematological malignancies. Nat. Commun. 2022, 13, 6922. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. The race for coronavirus vaccines: A graphical guide. Nature 2020, 580, 576–577. [Google Scholar] [CrossRef]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Pui, C.H. Childhood leukemias. N. Engl. J. Med. 1995, 332, 1618–1630. [Google Scholar] [CrossRef]
- Roberts, K.G.; Mullighan, C.G. The Biology of B-Progenitor Acute Lymphoblastic Leukemia. Cold Spring Harb. Perspect. Med. 2020, 10, a034835. [Google Scholar] [CrossRef]
- Sehrawat, S.; Kumar, D.; Rouse, B.T. Herpesviruses: Harmonious Pathogens but Relevant Cofactors in Other Diseases? Front. Cell Infect Microbiol. 2018, 8, 177. [Google Scholar] [CrossRef]
- Rouger-Gaudichon, J.; Bertrand, Y.; Boissel, N.; Brethon, B.; Ducassou, S.; Gandemer, V.; Halfon-Domenech, C.; Leblanc, T.; Leverger, G.; Michel, G.; et al. COVID19 and acute lymphoblastic leukemias of children and adolescents: Updated recommendations (Version 2) of the Leukemia Committee of the French Society for the fight against Cancers and leukemias in children and adolescents (SFCE). Bull. Cancer 2021, 108, 490–500. [Google Scholar] [CrossRef]
- Jaskula, E.; Dlubek, D.; Sedzimirska, M.; Duda, D.; Tarnowska, A.; Lange, A. Reactivations of cytomegalovirus, human herpes virus 6, and Epstein-Barr virus differ with respect to risk factors and clinical outcome after hematopoietic stem cell transplantation. Transpl. Proc. 2010, 42, 3273–3276. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factor | All CALLS Families | Agree N = 91 (21.4%) | Disagree N = 165 (38.9%) | Hesitant N = 168 (39.6%) | |
|---|---|---|---|---|---|
| Child Characteristics | |||||
| Sex | Female | 194 (45.8%) | 34 (37.4%) | 84 (50.9%) | 76 (45.2%) |
| Male | 230 (54.2%) | 57 (62.6%) | 81 (49.1%) | 92 (54.8%) | |
| Age at Remission | Mean ± SD | 5.99 ± 3.40 | 6.31 ± 3.94 | 6.05 ± 2.83 | 5.76 ± 3.60 |
| Age at Remission (Category) | <6 | 220 (51.9%) | 50 (54.9%) | 75 (45.5%) | 95 (56.5%) |
| ≥6 | 204 (48.1%) | 41 (45.1%) | 90 (54.5%) | 73 (43.5%) | |
| Remission Time (Year) | <1 | 92 (21.7%) | 20 (22.0%) | 34 (20.6%) | 38 (22.6%) |
| 1–2 | 78 (18.4%) | 15 (16.5%) | 32 (19.4%) | 31 (18.5%) | |
| 2–3 | 108 (25.5%) | 30 (33.0%) | 42 (25.5%) | 36 (21.4%) | |
| ≥3 | 146 (34.4%) | 26 (28.6%) | 57 (34.5%) | 63 (37.5%) | |
| School Preparation | Yes | 191 (45.0%) | 46 (50.5%) | 73 (44.2%) | 72 (42.9%) |
| Not yet | 233 (55.0%) | 45 (49.5%) | 92 (55.8%) | 96 (57.1%) | |
| Relapse History | Ever | 165 (38.9%) | 30 (33.0%) | 68 (41.2%) | 67 (39.9%) |
| Never | 259 (61.1%) | 61 (67.0%) | 97 (58.8%) | 101 (60.1%) | |
| Family Characteristics | |||||
| Age of Mother at Remission | Mean ± SD | 32.50 ± 3.87 | 32.81 ± 4.04 | 32.58 ± 3.81 | 32.26 ± 3.84 |
| Age of Mother at Remission (Category) | <33 | 227 (53.5%) | 43 (47.3%) | 89 (53.9%) | 95 (56.5%) |
| ≥33 | 197 (46.5%) | 48 (52.7%) | 76 (46.1%) | 73 (43.5%) | |
| Education Level † | High school or below | 224 (52.8%) | 45 (49.5%) | 83 (50.3%) | 96 (57.1%) |
| Junior college | 149 (35.1%) | 37 (40.7%) | 53 (32.1%) | 59 (35.1%) | |
| Bachelors or above | 51 (12.0%) | 9 (9.9%) | 29 (17.6%) | 13 (7.7%) | |
| Annual Family Income, CNY ‡ | <20,000 | 33 (7.8%) | 7 (7.7%) | 14 (8.5%) | 12 (7.1%) |
| 20,000 to 100,000 | 168 (39.6%) | 39 (42.9%) | 64 (38.8%) | 65 (38.7%) | |
| 100,000 to 200,000 | 60 (14.2%) | 16 (17.6%) | 17 (10.3%) | 27 (16.1%) | |
| >200,000 | 163 (38.4%) | 29 (31.9%) | 70 (42.4%) | 64 (38.1%) | |
| Marital Status | Married | 363 (85.6%) | 77 (84.6%) | 142 (86.1%) | 144 (85.7%) |
| Divorced | 61 (14.4%) | 14 (15.4%) | 23 (13.9%) | 24 (14.3%) | |
| Oncologist Recommendation | Yes | 118 (27.8%) | 44 (48.4%) | 13 (7.9%) | 61 (36.3%) |
| No | 306 (72.2%) | 47 (51.6%) | 152 (92.1%) | 107 (63.7%) | |
| Swayed by Nonhealthcare Information | Yes | 175 (41.3%) | 36 (39.6%) | 78 (47.3%) | 61 (36.3%) |
| No | 249 (58.7%) | 55 (60.4%) | 87 (52.7%) | 107 (63.7%) | |
| Variables (Reference) | β | Standard Error | Wald | p | OR | 95% CI |
|---|---|---|---|---|---|---|
| Sex (Female) | 0.36 | 0.26 | 1.97 | 0.16 | 1.43 | 0.87–2.36 |
| Age at Remission (Continuous) | 0.02 | 0.04 | 0.16 | 0.69 | 1.02 | 0.94–1.09 |
| Remission Time (Continuous) | −0.03 | 0.11 | 0.10 | 0.76 | 0.97 | 0.78–1.19 |
| School Preparation (Not yet) | 0.17 | 0.25 | 0.46 | 0.50 | 1.18 | 0.73–1.93 |
| Relapse History (Never) | −0.36 | 0.26 | 1.87 | 0.17 | 0.70 | 0.42–1.17 |
| Mother’s Gestating Age (Continuous) a | 0.00 | 0.05 | 0.00 | 0.97 | 1.00 | 0.90–1.11 |
| Education Level (High school or below) b | 0.15 | 0.25 | 0.34 | 0.56 | 1.16 | 0.71–1.88 |
| Family Income (Poverty) c | 0.07 | 0.46 | 0.03 | 0.87 | 1.08 | 0.43–2.68 |
| Marital Status (Divorced) | 0.00 | 0.35 | 0.00 | 1.00 | 1.00 | 0.51–1.98 |
| Swayed by Nonhealthcare Information (No) | −0.06 | 0.25 | 0.05 | 0.82 | 0.94 | 0.58–1.55 |
| Recommendation (No) | 1.15 | 0.25 | 20.94 | <0.001 | 3.17 | 1.93–5.20 |
| Constant | −2.05 | 1.55 | 1.76 | 0.19 | 0.13 |
| Variables (Reference) | β | Standard Error | Wald | p | OR | 95% CI |
|---|---|---|---|---|---|---|
| Sex (Female) | 0.59 | 0.55 | 1.14 | 0.29 | 1.80 | 0.61–5.32 |
| Age at Remission (Continuous) | 0.12 | 0.08 | 2.32 | 0.13 | 1.13 | 0.97–1.32 |
| Remission Time (Continuous) | −0.04 | 0.22 | 0.03 | 0.85 | 0.96 | 0.62–1.48 |
| School Preparation (Not yet) | 0.43 | 0.54 | 0.61 | 0.43 | 1.53 | 0.53–4.45 |
| Relapse History (Never) | 0.38 | 0.56 | 0.46 | 0.50 | 1.46 | 0.48–4.43 |
| Mother’s Gestating Age (Continuous) a | 0.02 | 0.11 | 0.05 | 0.82 | 1.03 | 0.83–1.27 |
| Education Level (High school or below) b | −0.31 | 0.53 | 0.35 | 0.55 | 0.73 | 0.26–2.06 |
| Family Income (Poverty) c | −0.44 | 1.14 | 0.15 | 0.70 | 0.65 | 0.07–6.03 |
| Marital Status (Divorced) | −0.12 | 0.72 | 0.03 | 0.86 | 0.88 | 0.21–3.65 |
| Swayed by Nonhealthcare Information (No) | −0.62 | 0.56 | 1.21 | 0.27 | 0.54 | 0.18–1.62 |
| WAI-SR (Continuous) | 0.14 | 0.03 | 26.34 | <0.001 | 1.15 | 1.09–1.21 |
| Constant | −7.87 | 3.61 | 4.75 | 0.03 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Liu, N.; Zhong, G.; Wang, D.; Cao, L.; Bai, S.; Zhu, P.; Zhang, A.; Wang, X. Parent Acceptance toward Inactivated COVID-19 Vaccination in Children with Acute Lymphoblastic Leukemia: The Power of Oncologist and Alliance. Vaccines 2022, 10, 2016. https://doi.org/10.3390/vaccines10122016
Ma Y, Liu N, Zhong G, Wang D, Cao L, Bai S, Zhu P, Zhang A, Wang X. Parent Acceptance toward Inactivated COVID-19 Vaccination in Children with Acute Lymphoblastic Leukemia: The Power of Oncologist and Alliance. Vaccines. 2022; 10(12):2016. https://doi.org/10.3390/vaccines10122016
Chicago/Turabian StyleMa, Yifei, Nianqi Liu, Guanqing Zhong, Dao Wang, Lu Cao, Shenrui Bai, Pengfei Zhu, Ao Zhang, and Xinjia Wang. 2022. "Parent Acceptance toward Inactivated COVID-19 Vaccination in Children with Acute Lymphoblastic Leukemia: The Power of Oncologist and Alliance" Vaccines 10, no. 12: 2016. https://doi.org/10.3390/vaccines10122016
APA StyleMa, Y., Liu, N., Zhong, G., Wang, D., Cao, L., Bai, S., Zhu, P., Zhang, A., & Wang, X. (2022). Parent Acceptance toward Inactivated COVID-19 Vaccination in Children with Acute Lymphoblastic Leukemia: The Power of Oncologist and Alliance. Vaccines, 10(12), 2016. https://doi.org/10.3390/vaccines10122016