
COVID-19 Vaccine Hesitancy among Adolescents: Cross-Sectional School Survey in Four Chinese Cities Prior to Vaccine Availability

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
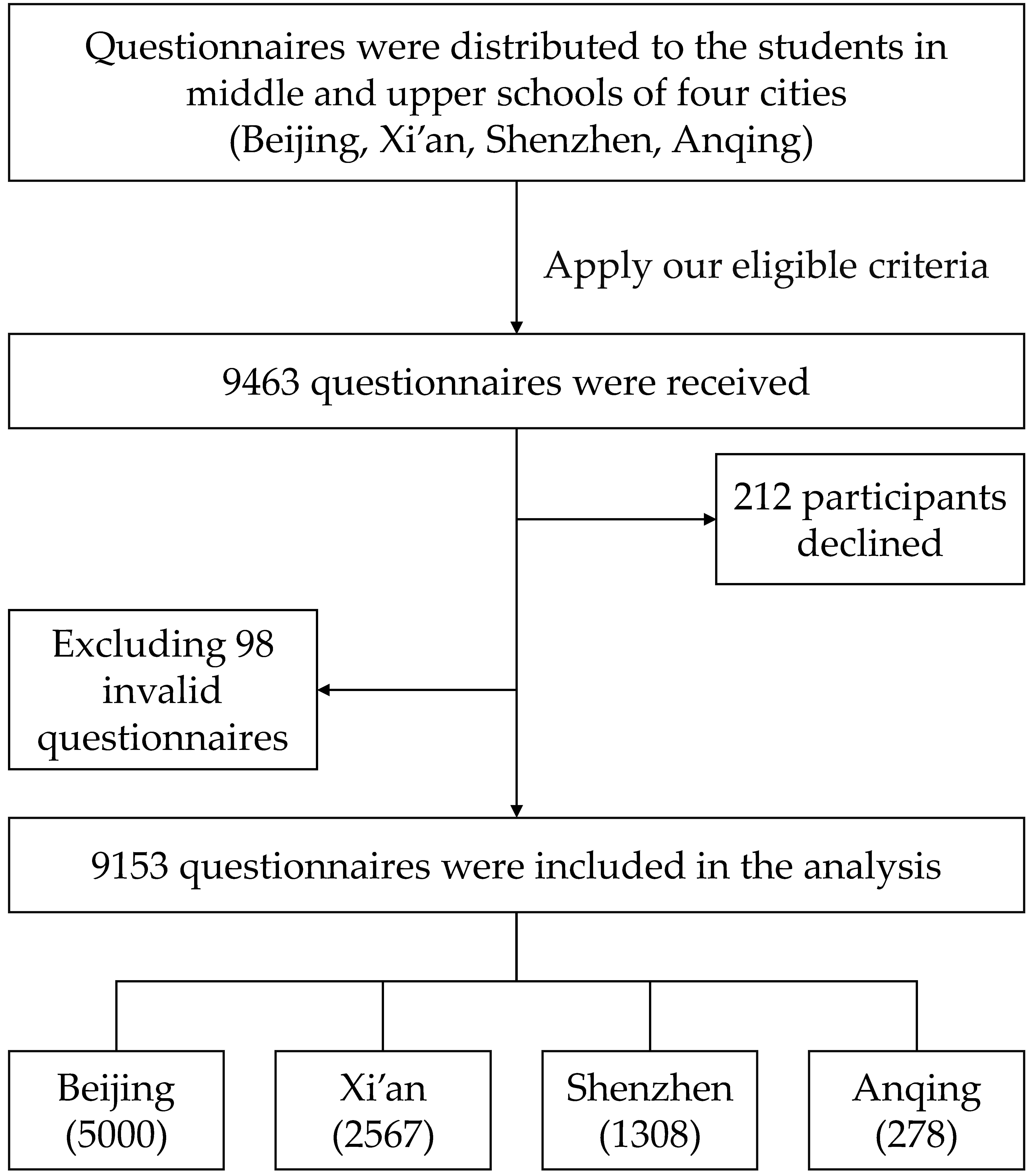
2.1. Study Design
2.2. Measurement
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Participants
3.2. Comparison of Vaccination Willingness
3.3. Factors Influencing Vaccine Resistance
3.4. Factors Influencing Vaccine Hesitancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y. Shaping Hong Kong cinema’s new icon: Milkyway Image at international film festivals. Transnatl. Cine. 2015, 6, 67–83. [Google Scholar] [CrossRef]
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, diagnostics and drug development. J. Hepatol. 2021, 74, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Song, Y.; Li, C.; Yang, W.; Ma, Q.; Jiang, Z.; Li, M.; Lian, X.; Jiao, W.; Wang, L.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy children and adolescents: A double-blind, randomised, controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 1645–1653. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated COVID-19 vaccine, BBIBP-CorV, in people younger than 18 years: A randomised, double-blind, controlled, phase 1/2 trial. Lancet Infect. Dis. 2022, 22, 196–208. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 COVID-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Trent, M.J.; Salmon, D.A.; MacIntyre, C.R. Using the health belief model to identify barriers to seasonal influenza vaccination among Australian adults in 2019. Influenza Other Respir Viruses 2021, 15, 678–687. [Google Scholar] [CrossRef]
- Coe, A.B.; Gatewood, S.B.; Moczygemba, L.R.; Goode, J.V.; Beckner, J.O. The use of the health belief model to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Innov. Pharm. 2012, 3, 1–11. [Google Scholar] [CrossRef]
- Kang, G.J.; Culp, R.K.; Abbas, K.M. Facilitators and barriers of parental attitudes and beliefs toward school-located influenza vaccination in the United States: Systematic review. Vaccine 2017, 35, 1987–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 5th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- Olson, O.; Berry, C.; Kumar, N. Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies. Vaccines 2020, 8, 590. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Elliott, L.; Yang, K. Vaccine Acceptance and Hesitancy among College Students in Nevada: A State-Wide Cross-Sectional Study. Vaccines 2022, 10, 105. [Google Scholar] [CrossRef] [PubMed]
- Mant, M.; Aslemand, A.; Prine, A.; Jaagumägi Holland, A. University students’ perspectives, planned uptake, and hesitancy regarding the COVID-19 vaccine: A multi-methods study. PLoS ONE 2021, 16, e0255447. [Google Scholar] [CrossRef] [PubMed]
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; De Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef] [PubMed]
- Middleman, A.B.; Klein, J.; Quinn, J. Vaccine Hesitancy in the Time of COVID-19: Attitudes and Intentions of Teens and Parents Regarding the COVID-19 Vaccine. Vaccines 2021, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Brandt, E.J.; Rosenberg, J.; Waselewski, M.E.; Amaro, X.; Wasag, J.; Chang, T. National Study of Youth Opinions on Vaccination for COVID-19 in the U.S. J. Adolesc. Health 2021, 68, 869–872. [Google Scholar] [CrossRef]
- Wong, W.H.S.; Leung, D.; Chua, G.T.; Duque, J.S.R.; Peare, S.; So, H.K.; Chan, S.M.; Kwan, M.Y.W.; Ip, P.; Lau, Y.L. Adolescents’ attitudes to the COVID-19 vaccination. Vaccine 2022, 40, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Xu, D.; Luo, L.; Ma, F.; Wang, P.; Li, H.; Li, Q.; Wei, L.; Diao, J.; Liu, Y.; et al. A Cross-Sectional Survey on COVID-19 Vaccine Hesitancy among Parents from Shandong vs. Zhejiang. Front. Public Health 2021, 9, 779720. [Google Scholar] [CrossRef] [PubMed]
- Shackman, G. Sample Size and Design Effect. Available online: https://www.alnap.org/help-library/sample-size-and-design-effect (accessed on 24 March 2001).
- Zhang, M.; Peng, Z.; Zheng, J.; Tan, Y.; Wang, X.; Qin, Y.; Feng, L. Disease burden of influenza in children and current status of vaccine usage in China. Chin. J. Appl. Clin. Pediatr. 2019, 34, 91–97. [Google Scholar] [CrossRef]
- Vallée-Tourangeau, G.; Promberger, M.; Moon, K.; Wheelock, A.; Sirota, M.; Norton, C.; Sevdalis, N. Motors of influenza vaccination uptake and vaccination advocacy in healthcare workers: Development and validation of two short scales. Vaccine 2018, 36, 6540–6545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhalaseh, L.; Fayoumi, H.; Khalil, B. The Health Belief Model in predicting healthcare workers’ intention for influenza vaccine uptake in Jordan. Vaccine 2020, 38, 7372–7378. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Q.; Huang, B.; Zhang, J.; Zhang, J.; Chen, X.; Zhang, H.; Hao, Y.; Li, Z.; Chen, X.; Dong, X. Development, reliability, and validity assessment of a Chinese version of the Parent Attitudes about Childhood Vaccines scale. Chin. J. Vaccines Immun. 2020, 26, 568–573. [Google Scholar]
- Shahnazi, H.; Ahmadi-Livani, M.; Pahlavanzadeh, B.; Rajabi, A.; Hamrah, M.S.; Charkazi, A. Assessing preventive health behaviors from COVID-19: A cross sectional study with health belief model in Golestan Province, Northern of Iran. Infect. Dis. Poverty 2020, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Puntis, S.; White, S.R.; Townsend, A.; Mansfield, K.L.; Viner, R.; Herring, J.; Pollard, A.J.; Freeman, D. Willingness of children and adolescents to have a COVID-19 vaccination: Results of a large whole schools survey in England. EClinicalMedicine 2021, 40, 101144. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, S.; Mattson, J.; Berghammer, M.; Brorsson, A.; Forsner, M.; Jenholt Nolbris, M.; Kull, I.; Lindholm Olinder, A.; Ragnarsson, S.; Rullander, A.; et al. To be or not to be vaccinated against COVID-19—The adolescents’ perspective—A mixed-methods study in Sweden. Vaccine X 2021, 9, 100117. [Google Scholar] [CrossRef] [PubMed]
- Afifi, T.O.; Salmon, S.; Taillieu, T.; Stewart-Tufescu, A.; Fortier, J.; Driedger, S.M. Older adolescents and young adults willingness to receive the COVID-19 vaccine: Implications for informing public health strategies. Vaccine 2021, 39, 3473–3479. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, N.; Singleton, J.A. COVID-19 Vaccination Intent, Perceptions, and Reasons for Not Vaccinating Among Groups Prioritized for Early Vaccination—United States, September and December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Olusanya, O.A.; Bednarczyk, R.A.; Davis, R.L.; Shaban-Nejad, A. Addressing Parental Vaccine Hesitancy and Other Barriers to Childhood/Adolescent Vaccination Uptake during the Coronavirus (COVID-19) Pandemic. Front. Immunol. 2021, 12, 663074. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.; Shi, J.; Zhang, G.; Liu, B. Willingness and associated factors of novel coronavirus vaccination among parents of primary and middle school students in Tongzhou District of Beijing. Chin. J. Sch. Health 2021, 42, 371–374. [Google Scholar] [CrossRef]
- Wang, Z.W.; Li, Z.; Huang, H.M.; Yang, Z.C.; Lv, J.C. Investigation on residents’ awareness of COVID-19 vaccines and vaccination willingness in Guangzhou. Mod. Prev. Med. 2021, 48, 732–737. [Google Scholar]
- Behrouzi, B.; Araujo Campoverde, M.V.; Liang, K.; Talbot, H.K.; Bogoch, I.I.; McGeer, A.; Fröbert, O.; Loeb, M.; Vardeny, O.; Solomon, S.D.; et al. Influenza Vaccination to Reduce Cardiovascular Morbidity and Mortality in Patients with COVID-19: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1777–1794. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.H.; Li, C.P.; Liu, Z.S.; Liu, S.J.; Zhang, D.W.; Ning, X.M.; Xie, D.J. Breeding and planting techniques of the high-quality and high-yield new variety Xinluzao 50. China Cotton 2011, 38, 37. [Google Scholar]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015-2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Diekema, D.S.; Ross, L.F. Should We Mandate a COVID-19 Vaccine for Children? JAMA Pediatr. 2021, 175, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, e2021726118. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Salmon, D.A. The Dual Epidemics of COVID-19 and Influenza: Vaccine Acceptance, Coverage, and Mandates. JAMA 2020, 324, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Chen, Z.; Xiang, Y.; Deng, C.; Zhang, H.; Wang, J. Simultaneous influence of sympathetic autonomic stress on Schlemm’s canal, intraocular pressure and ocular circulation. Sci. Rep. 2019, 9, 20060. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Lin, E.Z.; Brault, M.A.; Paquette, J.; Vermund, S.H.; Godri Pollitt, K.J. Reopening Schools after a Novel Coronavirus Surge. Adv. Exp. Med. Biol. 2021, 1318, 785–813. [Google Scholar] [CrossRef] [PubMed]
- Vermund, S.H.; Pitzer, V.E. Asymptomatic Transmission and the Infection Fatality Risk for COVID-19: Implications for School Reopening. Clin. Infect. Dis. 2021, 72, 1493–1496. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristics | n (%) |
|---|---|
| Sex | |
| Boy | 4575 (50.0) |
| Girl | 4578 (50.0) |
| Daily living | |
| Boarding at school | 1822 (19.9) |
| Not boarding | 7331 (80.1) |
| Ethnicity | |
| Han | 8618 (94.2) |
| Minorities | 535 (5.8) |
| Stage of schooling | |
| Junior high (middle) school grades 7–9 | 5708 (62.4) |
| Senior high (upper) school grades 10–12 | 3445 (37.6) |
| Region | |
| Beijing | 5000 (54.6) |
| Anqing, Anhui province | 278 (3.0) |
| Shenzhen, Guangdong province | 1308 (14.3) |
| Xi’an, Shaanxi province | 2567 (28.1) |
| COVID-19 concerns | |
| I am afraid of SARS-CoV-2 transmission | |
| Agree | 7248 (79.2) |
| Not sure | 852 (9.3) |
| Disagree | 1053 (11.5) |
| I have a potential risk of being infected with SARS-CoV-2 | |
| Agree | 3550 (38.8) |
| Not sure | 2536 (27.7) |
| Disagree | 3067 (33.5) |
| The COVID-19 has made me pay more attention to the influence of infectious diseases in my life, influencing me to get/want an influenza vaccine | |
| Agree | 6412 (70.0) |
| Not sure | 2059 (22.5) |
| Disagree | 682 (7.5) |
| COVID-19 vaccination concerns | |
| I will get the COVID-19 vaccine | |
| Agree | 5497 (60.0) |
| Not sure | 2891 (31.6) |
| Disagree | 765 (8.4) |
| Major concerns that affect my COVID-19 vaccination decision | |
| Safety | 8516 (93.0) |
| Effectiveness | 7587 (82.9) |
| Price | 3520 (38.5) |
| Convenience | 3448 (37.7) |
| Doctors’ recommendation | 3116 (34.0) |
| Influenza vaccination | |
| Did you get influenza vaccination in 2020 | |
| Yes | 3494 (38.2) |
| No | 5659 (61.8) |
| I have experience with a prior influenza vaccination | |
| Agree | 5240 (57.2) |
| Not sure | 1992 (21.8) |
| Disagree | 1921 (21.0) |
| Characteristics | Resist to Be Vaccinated (N = 765), n (%) | Hesitate to Be Vaccinated (N = 2891), n (%) | Willing to Be Vaccinated (N = 5497), n (%) | p |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Sex | <0.001 | |||
| Boy | 392 (8.6) | 1356 (29.6) | 2827 (61.8) | |
| Girl | 373 (8.1) | 1535 (33.5) | 2670 (58.3) | |
| Daily living | 0.015 | |||
| Boarding at school | 137 (7.5) | 537 (29.5) | 1148 (63.0) | |
| Not boarding | 628 (8.6) | 2354 (32.1) | 4349 (59.3) | |
| Ethnicity | 0.836 | |||
| Han | 722 (8.4) | 2716 (31.5) | 5180 (60.1) | |
| Minorities | 43 (8.0) | 175 (32.7) | 317 (59.3) | |
| Stage of schooling | 0.012 | |||
| Junior high (middle) school grades 7–9 | 512 (9.0) | 1766 (30.9) | 3430 (60.1) | |
| Senior high (upper) school grades 10–12 | 253 (7.3) | 1125 (32.7) | 2067 (60.0) | |
| Region | <0.001 | |||
| Beijing | 481 (9.6) | 1680 (33.6) | 2839 (56.8) | |
| Anqing, Anhui province | 14 (5.0) | 105 (37.8) | 159 (57.2) | |
| Shenzhen, Guangdong province | 63 (4.8) | 356 (27.2) | 889 (68.0) | |
| Xi’an, Shaanxi province | 207 (8.1) | 750 (29.2) | 1610 (62.7) | |
| COVID-19 concerns | ||||
| I am afraid of SARS-CoV-2 transmission | <0.001 | |||
| Agree | 507 (7.0) | 2010 (27.7) | 4731 (65.3) | |
| Not sure | 39 (4.6) | 595 (69.8) | 218 (25.6) | |
| Disagree | 219 (20.8) | 286 (27.2) | 548 (52.0) | |
| I have a potential risk of being infected with SARS-CoV-2 | <0.001 | |||
| Agree | 166 (4.7) | 731 (20.6) | 2653 (74.7) | |
| Not sure | 117 (4.6) | 1215 (47.9) | 1204 (47.5) | |
| Disagree | 482 (15.7) | 945 (30.8) | 1640 (53.5) | |
| The COVID-19 has made me pay more attention to the influence of infectious diseases in my life, influencing me to get an influenza vaccine | <0.001 | |||
| Agree | 245 (3.8) | 1169 (18.2) | 4998 (77.9) | |
| Not sure | 158 (7.7) | 1570 (76.3) | 331 (16.1) | |
| Disagree | 362 (53.1) | 152 (22.3) | 168 (24.6) | |
| COVID-19 vaccination concerns | ||||
| Major concerns that affect my COVID-19 vaccination decision | <0.001 | |||
| Safety | 680 (8.0) | 2667 (31.3) | 5169 (60.7) | |
| Effectiveness | 571 (7.5) | 2326 (30.7) | 4690 (61.8) | |
| Price | 213 (6.1) | 1100 (31.3) | 2207 (62.7) | |
| Convenience | 208 (6.0) | 999 (29.0) | 2241 (65.0) | |
| Doctors’ recommendation | 209 (6.7) | 908 (29.1) | 1999 (64.2) | |
| Influenza vaccination | ||||
| Did you get influenza vaccination in 2020 | <0.001 | |||
| Yes | 242 (6.9) | 972 (27.8) | 2280 (65.3) | |
| No | 523 (9.2) | 1919 (33.9) | 3217 (56.8) | |
| I have experience with a prior influenza vaccination | <0.001 | |||
| Agree | 353 (6.7) | 1336 (25.5) | 3551 (67.8) | |
| Not sure | 143 (7.2) | 890 (44.7) | 959 (48.1) | |
| Disagree | 269 (14.0) | 665 (34.6) | 987 (51.4) | |
| Factors | Intend to Be Vaccinated: Vaccine Resistance vs. Willing | Intend to Be Vaccinated: Vaccine Hesitancy vs. Willing | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Sex | ||||
| Boy | Ref | Ref | ||
| Girl | 1.04 (0.87–1.24) | 0.692 | 1.21 (1.09–1.36) | <0.001 |
| Daily living | ||||
| Boarding at school | 0.78 (0.61–1.00) | 0.052 | 0.79 (0.68–0.92) | 0.003 |
| Not boarding | Ref | Ref | ||
| Stage of schooling | ||||
| Junior high (middle) school grades 7–9 | 0.99 (0.80–1.22) | 0.913 | 0.98 (0.86–1.11) | 0.725 |
| Senior high (upper) school grades 10–12 | Ref | Ref | ||
| Region | ||||
| Beijing | 1.81 (1.44–2.28) | <0.001 | 1.62 (1.40–1.88) | <0.001 |
| Anqing, Anhui province | 0.65 (0.34–1.25) | 0.200 | 1.23 (0.89–1.71) | 0.213 |
| Shenzhen, Guangdong province | 0.72 (0.51–1.01) | 0.056 | 0.90 (0.75–1.09) | 0.282 |
| Xi’an, Shaanxi province | Ref | Ref | ||
| I am afraid of SARS-CoV-2 transmission | ||||
| Agree | Ref | Ref | ||
| Not sure | 0.87 (0.58–1.29) | 0.487 | 2.09 (1.70–2.57) | <0.001 |
| Disagree | 1.35 (1.07–1.71) | 0.013 | 0.93 (0.78–1.12) | 0.458 |
| I have a potential risk of being infected with SARS-CoV-2 | ||||
| Agree | Ref | Ref | ||
| Not sure | 1.43 (1.08–1.89) | 0.012 | 1.93 (1.67–2.22) | <0.001 |
| Disagree | 3.57 (2.86–4.46) | <0.001 | 1.72 (1.50–1.97) | <0.001 |
| The COVID-19 has made me pay more attention to the influence of infectious diseases in my life, influencing me to get an influenza vaccine | ||||
| Agree | Ref | Ref | ||
| Not sure | 8.03 (6.30–10.22) | <0.001 | 14.15 (12.27–16.31) | <0.001 |
| Disagree | 27.68 (21.81–35.13) | <0.001 | 3.24 (2.56–4.11) | <0.001 |
| Major concerns that affect my vaccination | ||||
| Safety | 0.80 (0.58–1.10) | 0.167 | 1.20 (0.95–1.50) | 0.130 |
| Effectiveness | 0.66 (0.52–0.83) | <0.001 | 0.84 (0.72–0.98) | 0.027 |
| Price | 0.86 (0.69–1.07) | 0.169 | 1.20 (1.05–1.36) | 0.007 |
| Convenience | 0.81 (0.64–1.01) | 0.064 | 0.84 (0.73–0.96) | 0.011 |
| Doctors’ recommendation | 0.93 (0.75–1.15) | 0.496 | 0.86 (0.76–0.98) | 0.025 |
| Did you get influenza vaccination in 2020 | ||||
| Yes | 0.88 (0.72–1.09) | 0.240 | 0.89 (0.78–1.01) | 0.063 |
| No | Ref | Ref | ||
| I have experience with a prior influenza vaccination | ||||
| Agree | Ref | Ref | ||
| Not sure | 1.30 (1.01–1.67) | 0.038 | 1.44 (1.24–1.67) | <0.001 |
| Disagree | 1.57 (1.25–1.98) | <0.001 | 1.33 (1.14–1.55) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehati, P.; Amaerjiang, N.; Yang, L.; Xiao, H.; Li, M.; Zunong, J.; Wang, L.; Vermund, S.H.; Hu, Y. COVID-19 Vaccine Hesitancy among Adolescents: Cross-Sectional School Survey in Four Chinese Cities Prior to Vaccine Availability. Vaccines 2022, 10, 452. https://doi.org/10.3390/vaccines10030452
Rehati P, Amaerjiang N, Yang L, Xiao H, Li M, Zunong J, Wang L, Vermund SH, Hu Y. COVID-19 Vaccine Hesitancy among Adolescents: Cross-Sectional School Survey in Four Chinese Cities Prior to Vaccine Availability. Vaccines. 2022; 10(3):452. https://doi.org/10.3390/vaccines10030452
Chicago/Turabian StyleRehati, Palizhati, Nubiya Amaerjiang, Liping Yang, Huidi Xiao, Menglong Li, Jiawulan Zunong, Long Wang, Sten H. Vermund, and Yifei Hu. 2022. "COVID-19 Vaccine Hesitancy among Adolescents: Cross-Sectional School Survey in Four Chinese Cities Prior to Vaccine Availability" Vaccines 10, no. 3: 452. https://doi.org/10.3390/vaccines10030452
APA StyleRehati, P., Amaerjiang, N., Yang, L., Xiao, H., Li, M., Zunong, J., Wang, L., Vermund, S. H., & Hu, Y. (2022). COVID-19 Vaccine Hesitancy among Adolescents: Cross-Sectional School Survey in Four Chinese Cities Prior to Vaccine Availability. Vaccines, 10(3), 452. https://doi.org/10.3390/vaccines10030452