1. Introduction
Metastatic malignant melanoma (MMM) is a severe and life-threatening disease, often leading to a fatal outcome. Its frequency is decreasing; however, during the last decade, the disease-free survival and the overall survival of patients suffering MMM have increased due to new effective treatments that include immunotherapy and targeted therapy [
1,
2].
Immunotherapy involves inhibitory receptors or checkpoint inhibitors. These regimens include cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed death-1 (PD-1) protein.
Checkpoint immunotherapy often leads to disease remission of metastatic disease in every visceral organ, including the central nervous system. Combination checkpoint immunotherapy has shown remarkable success, and it is of note that a small number of MMM patients receiving such therapy have been considered cured [
1,
2]. On the other hand, molecular studies have revealed that melanoma is a tumor with a high mutational burden, and it was understood that mutations could be targeted by drugs. Currently, several agents target the MAPK pathway, while mutations are routinely assessed in these tumors, and, if present, treatment with these agents leads to satisfactory results with long remissions of the disease [
1,
2,
3]. Hence, satisfactory responses of metastatic disease in all visceral organs, including the brain, with the use of BRAF-targeted therapy in cases of melanomas expressing a BRAF V600E mutation, have been observed; while in resistant tumors, targeted therapy with the combination of BRAF and MEK inhibitors resulted in tumor remissions [
1,
2,
3]. BRAF is serine-thionine kinase in the RAS-RAF-MEK-ERK pathway [
1,
2,
3].
While immunotherapy and targeted therapy have revolutionized MMM treatment, efforts have been made to develop melanoma vaccines, since vaccination is a type of immunotherapy [
4]. Up to now, several vaccines, including those using the mRNA technique, have been used for the treatment of melanoma. These vaccines induce immune responses, although with minimal clinical benefits of limited duration. However, this research is ongoing towards personalized anti-melanoma mRNA vaccines [
1,
4,
5].
The COVID-19 infection that often causes severe acute respiratory syndrome due to coronavirus-2 (SARS-CoV-2) is an ongoing pandemic that has taken millions of lives worldwide and represents a major threat to public health [
4,
6]. COVID-19 symptoms may differ substantially from patient to patient and may range from undetectable to fatal. The disease represents a special threat for immunocompromised hosts, such as those suffering malignant diseases. Hence, the need for effective treatment, especially for protective vaccines, became urgent [
4,
7].
The COVID-19 pandemic and the urgent need for a SARS-CoV-2 effective vaccine have led investigators to reassess the value of the mRNA vaccines, and the effort has been proven successful. Hence, the mRNA technology used for vaccines against tumors was ready and shifted rapidly to address the SARS-CoV-2 with success [
4,
6,
7].
The approval of these vaccines was fast, and they have been distributed to many countries since December 2020, aiming to elevate immune response to the COVID-19 virus antigen in humans at risk of developing the infection [
6,
7].
The mRNA SARS-CoV-2 vaccine contains messenger RNA, which causes cells to express the virus spike protein. When the vaccine enters the human body, it helps the immune system identify and destroy the pathogen [
4,
6,
7].
A unique case of metastatic melanoma skin nodules regression, after mRNA Pfizer-BioNTech SARS-CoV-2 vaccination, in a heavily pretreated 72-year-old Caucasian female is presented.
2. Case Presentation
We present a patient suffering MMM, with long survival due to several successful treatments.
The patient’s melanoma was firstly diagnosed 10 years ago, when a nevoid malignant melanoma (BRAF mutated), with maxillary lymph node involvement, was removed from her left arm. Consequently, she received adjuvantly interferon for almost a year.
However, three years later, the disease recurred with several skin metastatic nodules all over her body. For the following seven years, she has been on several treatments sequentially, receiving practically all existing types of available anti-melanoma therapies (chemotherapy, checkpoint inhibitors, and targeted therapies) [
1,
2,
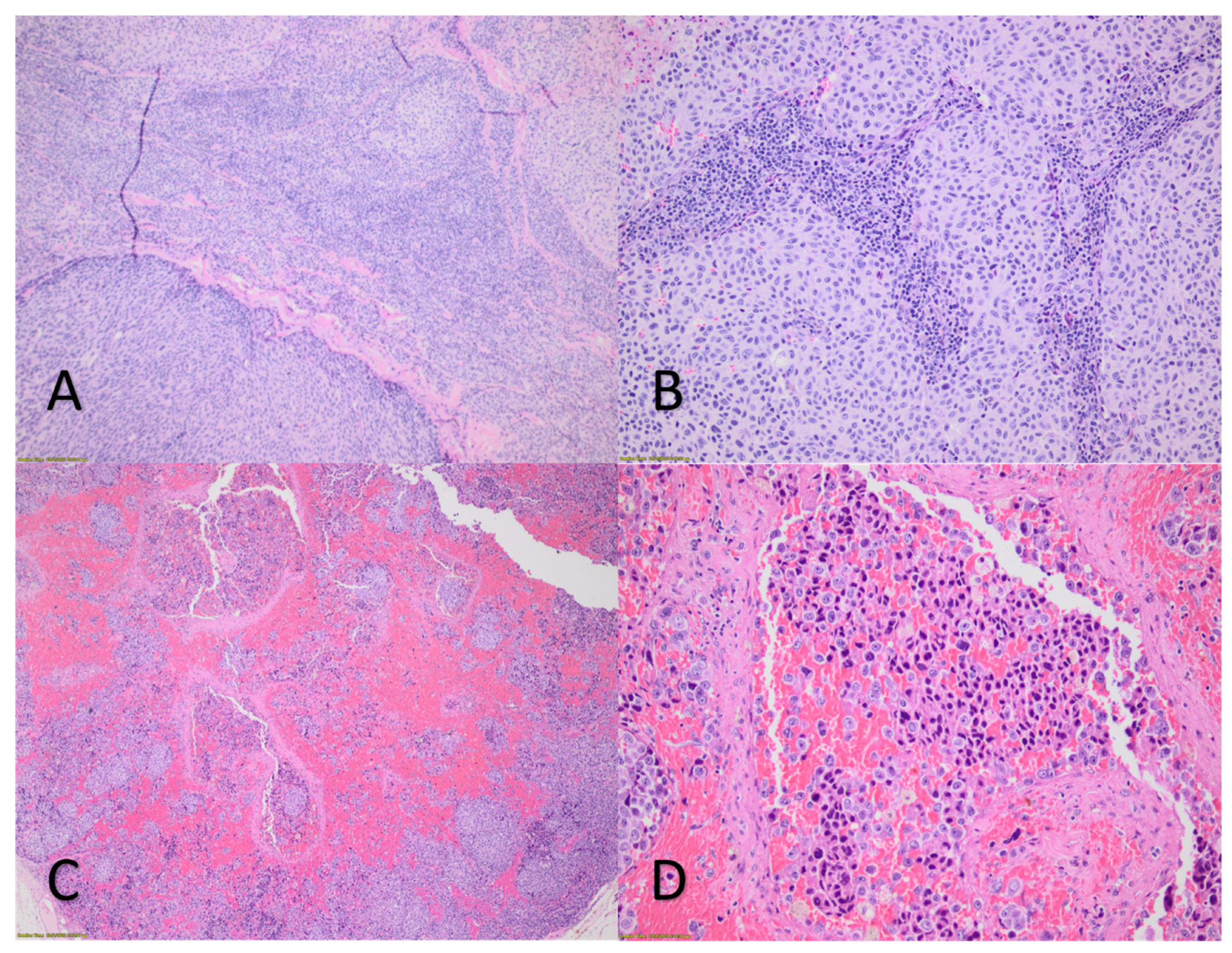
3]. She started with the dacarbazine and vindesine combination with no response. Then she received ipilimumab with also poor results. Hence, the treatment changed to dabrafenib and, due to intolerance, she was put on pembrolizumab, which kept her disease stable for 18 months. When the disease progressed, she received nivolumab, which also kept her melanoma under control for 15 months (
Figure 1A,B).
However, at this point, she developed liver metastasis, and “salvage” treatment was decided using chemotherapy (cis platinum and temozolomide) with poor results. Consequently, because of the BRAF mutated tumor status, she was treated with the encorafenib-binimetinib combination, which led to partial response and stabilization of her melanoma lesions for 18 months. Nevertheless, due to further progression of the skin melanoma nodules, the disease was re-challenged with pembrolizumab with satisfactory results lasting 14 months, up to the present. During these seven years, she never complained of pain.
At this point, 15 days after the last dose of pembrolizumab, she had the first dose of the mRNA-CoV-2 Pfizer-BioNTech vaccine uneventfully. Three weeks later, she received the second vaccine dose. No other medication had been given to her between the two vaccine doses.
Ten hours after the second vaccine dose, all her metastatic skin nodules became progressively painful, and gradually the pain became unbearable, forcing her to seek medical attention. She was hospitalized and treated with analgesics. Two days later, the pain was reduced and finally disappeared. The same day she felt that all her palpable skin melanoma nodules had reduced in size. Physical examination confirmed her observation, since all her skin nodules were significantly smaller by at least 50%. Ultrasound examination of several such nodules confirmed the significant reduction of their size compared to previous recent ultrasound imaging of the same nodules. However, an MRI revealed that the liver metastasis did not show any change.
One week after the skin nodules had been reduced and remained unchanged, one of them was surgically removed and histologically examined. At the same time, the current histopathology was compared to that of a previously removed melanoma nodule (
Figure 1C,D).
Notable differences between the previous and the current histopathology were observed. The previous one showed melanoma with high mitotic activity, epithelial and spindle neoplastic cells, and moderate lymphocytic infiltration. The current histopathology confirmed the diagnosis of melanoma, also with high mitotic activity, with neoplastic epithelial cells characterized by pronounced cellular atypia and polymorphism. There were hemorrhagic deposits and areas of necrosis, while lymphocytic infiltration was not observed.
Four months later, when the patient received the third vaccine dose, the metastatic melanoma skin nodules became slightly painful and were reduced a little further in size. However, her visceral disease remained unchanged as previously.
3. Discussion
The COVID-19 epidemic became a major risk for patients with neoplastic diseases that are immunocompromised due to their disease and/ or the treatment they receive. Hence, in most developed countries, this patient population has been vaccinated with three doses of the mRNA SARS-CoV-2 vaccine without severe side effects [
6,
7]. This vaccine is a type of immunotherapy since its administration enhances immunogenicity. This activity is of special interest for patients suffering MMM, for whom immunotherapy represents a major therapeutic tool [
4,
6,
7].
The present patient has been suffering MMM for seven years, and she has received most available treatments, some resulting in partial response and stabilization of her disease [
1,
2]. For all these years, her performance status was excellent. She had been fully functioning and never complained of pain.
After receiving the second dose of the SARS-CoV-2 mRNA vaccine, her skin metastases became painful and reduced in size within 48 h. The shrinkage of all the melanoma skin nodules had been confirmed by thorough clinical examination and ultrasound imaging.
Considering the existing literature, this is a unique case of special interest, revealing an unexpected activity of this vaccine, indicating that it may exert antitumor activity [
5,
6,
7].
No definite explanation of the vaccine’s antitumor activity can be given. However, some possible mechanisms involved may be speculated upon, based on existing relevant information. It is of interest, however, that initially the mRNA vaccines had been developed as antineoplastic agents [
5,
6,
7].
The lack of lymphocytic infiltration of the reduced metastatic melanoma skin nodule was an unexpected finding. Therefore, it is unlikely that the vaccine triggered an “anamnestic” expansion of preexisting tumor-targeting lymphocytes induced by the previous immunotherapy. High infiltration of the tumor by lymphocytes (TILs) is beneficial in melanoma cases, and the composition of TILs is important [
1,
2,
3]. However, the reduced melanoma nodule of the present patient did not have any TILs. Hence, another possible mechanism may be operative: the exogenous mRNA could have exerted antitumor activity and apoptosis via stimulation of Tol Like Receptor 3 (TLR3), TLR7, and TLR8, and downstream the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway of non-lymphocytic immune effector cells, since TRL7 and TRL8 agonists have been extensively studied as adjunct anti-melanoma drugs [
4,
8]. The possibility that the observed effects are, perhaps, a delayed response to pembrolizumab treatment cannot be excluded. However, the acute symptoms following the vaccination make this possibility remote.
The possible salutary effect of the second and third vaccine doses was sustained. Five months after the third vaccination, all skin nodules remained reduced in size, and new skin lesions did not appear.
Irrespectively of the possible immunological mechanism(s) involved, the effect of the SARS-CoV-2 mRNA vaccine on the melanoma metastatic skin nodules, if validated on a larger scale, could have important clinical implications. It is of note that mRNA vaccines directed against patient-specific neoantigens have been used already as melanoma treatment [
9,
10].
Finally, the lack of response of the liver metastasis is also of interest, as it might reflect differences in tissue-specific response patterns to immune-mediated (presumed catalyzed by the mRNA SARS-CoV-19 vaccine) control of the MMM, as it has been shown in patients with MMM treated with ipilimumab combined with anti-PD-1 therapy [
11]. Such individually tailored mRNA cancer vaccine is a topic of active investigation in cancer immunotherapy [
12].
Although the mRNA SARS-CoV-2 vaccine has already been given to millions of at-risk patients, new data continue to emerge, and recommendations are updated periodically. There are still immunological results that need to be studied. It must be kept in mind that the urgency to create the vaccine has shortened its development timeline, and though the side-effects are studied extensively, scientific issues regarding the range of the vaccine’s activities are open and require further experience, observation, and analyses of new emerging data.
4. Conclusions
This present, signal case, is reported to increase the index of suspicion of oncologists who treat melanoma patients also receiving the SARS-CoV-2 mRNA vaccine, and may present similar effects. Additionally, this report should stimulate further research into the possibility of using the mRNA technology to devise personalized vaccines against each patient’s melanoma, following genetic analysis of each melanoma from a tissue sample of the patient’s tumor.
Author Contributions
Conceptualization, D.B. and G.S.; methodology, A.B., E.C.; investigation, K.P., I.P.; data curation, I.P., K.P., A.B., E.C.; writing—original draft preparation, C.K., G.S.; writing—review and editing, D.B., G.S.; visualization, C.K.; supervision, G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This is a case report.
Informed Consent Statement
Informed consent has been received.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Dimitrios Kontoyiannis of M.D. Anderson Cancer Center, Houston, TX, USA, for his valuable advice and consultation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Curti, B.D.; Faries, M.B. Recent Advances in the Treatment of Melanoma. N. Engl. J. Med. 2021, 384, 2229–2240. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current state of melanoma diagnosis and treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, H.; Yacoub, N.; Mishra, R.; White, A.; Long, Y.; Alanazi, S.; Garrett, J.T. Current Advances in the Treatment of BRAF-Mutant Melanoma. Cancers 2020, 12, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heine, A.; Juranek, S.; Brossart, P. Clinical and immunological effects of mRNA vaccines in malignant diseases. Mol. Cancer 2021, 20, 52. [Google Scholar] [CrossRef] [PubMed]
- Miao, L.; Zhang, Y.; Huang, L. mRNA vaccine for cancer immunotherapy. Mol. Cancer 2021, 20, 41. [Google Scholar] [CrossRef] [PubMed]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Amanpour, S. The Rapid Development and Early Success of Covid 19 Vaccines Have Raised Hopes for Accelerating the Cancer Treatment Mechanism. Arch. Razi. Inst. 2021, 76, 1–6. [Google Scholar] [PubMed]
- Chi, H.; Li, C.; Zhao, F.S.; Zhang, L.; Ng, T.B.; Jin, G.; Sha, O. Anti-tumor Activity of Toll-Like Receptor 7 Agonists. Front Pharmacol. 2017, 8, 304. [Google Scholar] [CrossRef] [PubMed]
- Kyte, J.A.; Aamdal, S.; Dueland, S.; Sæbøe-Larsen, S.; Inderberg, E.M.; Madsbu, U.E.; Skovlund, E.; Gaudernack, G.; Kvalheim, G. Immune response and long-term clinical outcome in advanced melanoma patients vaccinated with tumor-mRNA-transfected dendritic cells. Oncoimmunology 2016, 5, e1232237. [Google Scholar] [CrossRef] [PubMed]
- Kyte, J.A.; Gaudernack, G.; Faane, A.; Lislerud, K.; Inderberg, E.M.; Brunsvig, P.; Aamdal, S.; Kvalheim, G.; Wälchli, S.; Pule, M. T-helper cell receptors from long-term survivors after telomerase cancer vaccination for use in adoptive cell therapy. Oncoimmunology 2016, 5, e1249090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires da Silva, I.; Lo, S.; Quek, C.; Gonzalez, M.; Carlino, M.S.; Long, G.V.; Menzies, A.M. Site-specific response patterns, pseudoprogression, and acquired resistance in patients with melanoma treated with ipilimumab combined with anti-PD-1 therapy. Cancer 2020, 126, 86–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, J.D.; Reidenbach, D.; Salomon, N.; Sahin, U.; Türeci, Ö.; Vormehr, M.; Kranz, L.M. mRNA therapeutics in cancer immunotherapy. Mol. Cancer 2021, 20, 69. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, {kind=link}
