
Cardiac Adverse Events after Vaccination—A Systematic Review

 ,
,
Abstract
:1. Introduction
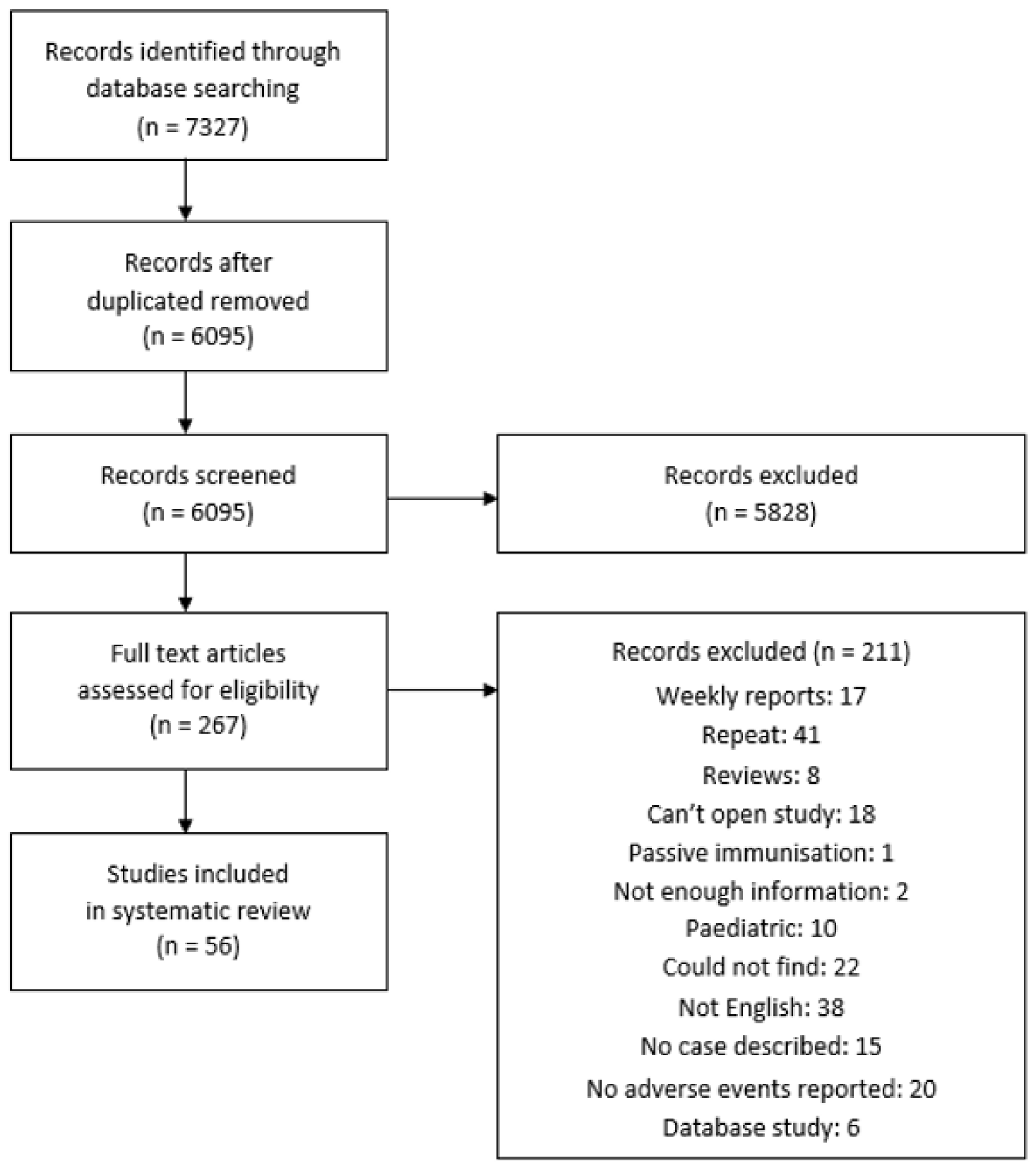
2. Methods
2.1. Design
2.2. Study Selection
2.3. Data Extraction
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- VAERS. Vaccine Adverse Event Reporting System. Available online: https://vaers.hhs.gov/about.html (accessed on 15 January 2022).
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, J.R.; McNeil, M.M.; Welsh, K.J.; Marquez, P.L.; Ng, C.; Yan, M.; Cano, M.V. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990–2018. Vaccine 2021, 39, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Singh, R.; Kaur, J.; Pandey, S.; Sharma, V.; Thakur, L.; Sati, S.; Mani, S.; Asthana, S.; Sharma, T.K.; et al. Wuhan to World: The COVID-19 Pandemic. Front. Cell. Infect. Microbiol. 2021, 11, 596201. [Google Scholar] [CrossRef] [PubMed]
- Team MCVT. Available online: https://covid19.trackvaccines.org/agency/who/ (accessed on 24 November 2021).
- Rosner, C.M.; Genovese, L.; Tehrani, B.N.; Atkins, M.; Bakhshi, H.; Chaudhri, S.; Damluji, A.A.; de Lemos, J.A.; Desai, S.S.; Emaminia, A.; et al. Myocarditis Temporally Associated With COVID-19 Vaccination. Circulation 2021, 144, 502–505. [Google Scholar] [CrossRef]
- Kim, H.W.; Jenista, E.R.; Wendell, D.C.; Azevedo, C.F.; Campbell, M.J.; Darty, S.N.; Parker, M.A.; Kim, R.J. Patients with Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021, 6, 1196. [Google Scholar] [CrossRef]
- Larson, K.F.; Ammirati, E.; Adler, E.D.; Cooper, L.T., Jr.; Hong, K.N.; Saponara, G.; Couri, D.; Cereda, A.; Procopio, A.; Cavalotti, C.; et al. Myocarditis After BNT162b2 and mRNA-1273 Vaccination. Circulation 2021, 144, 506–508. [Google Scholar] [CrossRef]
- Mansour, J.; Short, R.G.; Bhalla, S.; Woodard, P.K.; Verma, A.; Robinson, X.; Raptis, D.A. Acute myocarditis after a second dose of the mRNA COVID-19 vaccine: A report of two cases. Clin. Imaging 2021, 78, 247–249. [Google Scholar] [CrossRef]
- Kao, C.-D.; Chen, J.-T.; Lin, K.-P.; Shan, D.-E.; Wu, Z.-A.; Liao, K.-K. Guillain-Barré syndrome coexisting with pericarditis or nephrotic syndrome after influenza vaccination. Clin. Neurol. Neurosurg. 2004, 106, 136–138. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bae, J.I.; Ryoo, S.M.; Kim, W.Y. Acute Fulminant Myocarditis Following Influenza Vaccination Requiring Extracorporeal Membrane Oxygenation. Acute Crit. Care 2019, 34, 165–169. [Google Scholar] [CrossRef]
- Mei, R.; Raschi, E.; Poluzzi, E.; Diemberger, I.; De Ponti, F. Recurrence of pericarditis after influenza vaccination: A case report and review of the literature. BMC Pharmacol. Toxicol. 2018, 19, 20. [Google Scholar] [CrossRef] [Green Version]
- De Meester, A.; Luwaert, R.; Chaudron, J.M. Symptomatic pericarditis after influenza vaccination: Report of two cases. Chest 2000, 117, 1803–1805. [Google Scholar] [CrossRef] [Green Version]
- Santoro, F.; Ieva, R.; Ferraretti, A.; Carpagnano, G.; Pappalardo, I.; De Gennaro, L.; Di Biase, M.; Brunetti, N.D. Tako-Tsubo cardiomyopathy after influenza vaccination. Int. J. Cardiol. 2013, 167, e51–e52. [Google Scholar] [CrossRef]
- Singh, K.; Marinelli, T.; Horowitz, J.D. Takotsubo cardiomyopathy after anti-influenza vaccination: Catecholaminergic effects of immune system. Am. J. Emerg. Med. 2013, 31, e1–e4. [Google Scholar] [CrossRef]
- Streifler, J.J.; Dux, S.; Garty, M.; Rosenfeld, J.B. Recurrent pericarditis: A rare complication of influenza vaccination. Br. Med. J. 1981, 283, 526–527. [Google Scholar] [CrossRef] [Green Version]
- Cheng, M.P.; Kozoriz, M.G.; Ahmadi, A.A.; Kelsall, J.; Paquette, K.; Onrot, J.M. Post-vaccination myositis and myocarditis in a previously healthy male. Allergy Asthma Clin. Immunol. 2016, 12, 6. [Google Scholar] [CrossRef] [Green Version]
- Zanettini, M.T.; Zanettini, J.O.; Zanettini, J.P. Pericarditis. Series of 84 consecutive cases. Arq. Bras. Cardiol. 2004, 82, 360–369. [Google Scholar] [CrossRef] [Green Version]
- Godreuil, S.; Delhaume, O.; Besset-Prat, L.; Blayac, J.P.; Peyriere, H.; Bonnet, P. Acute haemorrhagic pericarditis following influenza vaccination. Presse Med. 2003, 32, 258–259. [Google Scholar]
- Wiley. Available online: https://onlinelibrary.wiley.com/doi/pdf/10.1111/all.12252 (accessed on 24 November 2021).
- Lee, E.; Chew, N.W.S.; Ng, P.; Yeo, T.J. Reply to “Letter to the editor: Myocarditis should be considered in those with a troponin rise and unobstructed coronary arteries following PfizerBioNTech COVID-19 vaccination”. QJM 2021, 114, hcab231. [Google Scholar] [CrossRef]
- Montgomery, J.; Ryan, M.; Engler, R.; Hoffman, D.; McClenathan, B.; Collins, L.; Loran, D.; Hrncir, D.; Herring, K.; Platzer, M.; et al. Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021, 6, 1202. [Google Scholar] [CrossRef]
- Lee, E.; Chew, N.W.S.; Ng, P.; Yeo, T.J. A spectrum of cardiac manifestations post Pfizer-BioNTech COVID-19 vaccination. QJM 2021, 114, 661–662. [Google Scholar] [CrossRef]
- Habib, M.B.; Hamamyh, T.; Elyas, A.; Altermanini, M.; Elhassan, M. Acute myocarditis following administration of BNT162b2 vaccine. IDCases 2021, 25, e01197. [Google Scholar] [CrossRef]
- Mouch, S.A.; Roguin, A.; Hellou, E.; Ishai, A.; Shoshan, U.; Mahamid, L.; Zoabi, M.; Aisman, M.; Goldschmid, N.; Yanay, N.B. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021, 39, 3790–3793. [Google Scholar] [CrossRef]
- Chatterjee, S.; Ojha, U.K.; Vardhan, B.; Tiwari, A. Myocardial infarction after COVID-19 vaccination-casual or causal? Diabetes Metab. Syndr. 2021, 15, 1055–1056. [Google Scholar] [CrossRef]
- Deb, A.; Abdelmalek, J.; Iwuji, K.; Nugent, K. Acute Myocardial Injury Following COVID-19 Vaccination: A Case Report and Review of Current Evidence from Vaccine Adverse Events Reporting System Database. J. Prim. Care Community Health 2021, 12, 21501327211029230. [Google Scholar] [CrossRef]
- Albert, E.; Aurigemma, G.; Saucedo, J.; Gerson, D.S. Myocarditis following COVID-19 vaccination. Radiol. Case Rep. 2021, 16, 2142–2145. [Google Scholar] [CrossRef]
- D’Angelo, T.; Cattafi, A.; Carerj, M.L.; Booz, C.; Ascenti, G.; Cicero, G.; Blandino, A.; Mazziotti, S. Myocarditis After SARS-CoV-2 Vaccination: A Vaccine-Induced Reaction? Can. J. Cardiol. 2021, 37, 1665–1667. [Google Scholar] [CrossRef]
- Watkins, K.; Griffin, G.; Septaric, K.; Simon, E.L. Myocarditis after BNT162b2 vaccination in a healthy male. Am. J. Emerg. Med. 2021, 50, 815.e1–815.e2. [Google Scholar] [CrossRef]
- Ammirati, E.; Cavalotti, C.; Milazzo, A.; Pedrotti, P.; Soriano, F.; Schroeder, J.W.; Morici, N.; Giannattasio, C.; Frigerio, M.; Metra, M.; et al. Temporal Relation Between Second Dose BNT162b2 mRNA Covid-19 Vaccine and Cardiac involvement in a Patient with Previous SARS-COV-2 Infection. Int. J. Cardiol. Heart Vasc. 2021, vol.34, 100774. [Google Scholar]
- Tajstra, M.; Jaroszewicz, J.; Gąsior, M. Acute Coronary Tree Thrombosis After Vaccination for COVID-19. JACC Cardiovasc. Interv. 2021, 14, e103–e104. [Google Scholar] [CrossRef]
- Srinivasan, K.N.; Sathyamurthy, I.; Neelagandan, M. Relation between COVID-19 vaccination and myocardial infarction—Casual or coincidental? IHJ Cardiovasc. Case Rep. 2021, 5, 71–74. [Google Scholar] [CrossRef]
- Özdemir, İ.H.; Özlek, B.; Özen, M.B.; Gündüz, R.; Bayturan, Ö. Type 1 Kounis Syndrome Induced by Inactivated SARS-COV-2 Vaccine. J. Emerg. Med. 2021, 61, e71–e76. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef] [PubMed]
- Timothy, J.; Whitman, M.; Ferguson, A.; Catherine, F.; Decker, A. Cardiac Dysrhythmia following Smallpox Vaccination. Clin. Infect. Dis. 2003, 37, 1579–1580. [Google Scholar] [CrossRef] [Green Version]
- Engler, R.J.; Nelson, M.R.; Collins, L.C., Jr.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; Atwood, J.E.; Howard, R.S.; Chang, A.S.; Cruser, D.L.; et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS ONE. 2015, 10, e0118283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckart, R.E.; Love, S.S.; Atwood, J.E.; Arness, M.K.; Cassimatis, D.C.; Campbell, C.L.; Boyd, S.Y.; Murphy, J.G.; Swerdlow, D.L.; Collins, L.C.; et al. Incidence and follow-up of inflammatory cardiac complications after smallpox vaccination. J. Am. Coll. Cardiol. 2004, 44, 201–205. [Google Scholar] [CrossRef] [Green Version]
- Sarkisian, S.A.; Hand, G.; Rivera, V.M.; Smith, M.; Miller, J.A. A Case Series of Smallpox Vaccination-Associated Myopericarditis: Effects on Safety and Readiness of the Active Duty Soldier. Mil. Med. 2019, 184, e280–e283. [Google Scholar] [CrossRef] [Green Version]
- Saurina, G.; Shirazi, S.; Lane, J.M.; Daniel, B.; Di Eugenia, L. Myocarditis after Smallpox Vaccination: A Case Report. Clin. Infect. Dis. 2003, 37, 145–146. [Google Scholar] [CrossRef] [Green Version]
- Sharma, U.; Tak, T. A report of 2 cases of myopericarditis after Vaccinia virus (smallpox) immunization. WMJ 2011, 110, 291–294. [Google Scholar]
- Sniadack, M.M.; Neff, L.J.; Swerdlow, D.L.; Schieber, R.A.; McCauley, M.M.; Mootrey, G.T. Follow-Up of Cardiovascular Adverse Events after Smallpox Vaccination among Civilians in the United States, 2003. Clin. Infect. Dis. 2008, 46, S251–S257. [Google Scholar] [CrossRef] [Green Version]
- Keinath, K.; Church, T.; Kurth, B.; Hulten, E. Myocarditis secondary to smallpox vaccination. BMJ Case Rep. 2018, 2018, bcr–2017–223523. [Google Scholar] [CrossRef]
- Halsell, J.S.; Riddle, J.R.; Atwood, J.E.; Gardner, P.; Shope, R.; Poland, G.A.; Gray, G.C.; Ostroff, S.; Eckart, R.E.; Hospenthal, D.R.; et al. Myopericarditis following smallpox vaccination among vaccinia-naive US military personnel. JAMA 2003, 289, 3283–3289. [Google Scholar] [CrossRef]
- Matthews, A.W.; Griffiths, I.D. Post-vaccinial pericarditis and myocarditis. Br. Heart J. 1974, 36, 1043–1045. [Google Scholar] [CrossRef] [Green Version]
- Eckart, R.E.; Shry, E.A.; Jones SOt Atwood, J.E.; Grabenstein, J.D. Comparison of clinical presentation of acute myocarditis following smallpox vaccination to acute coronary syndromes in patients <40 years of age. Am. J. Cardiol. 2005, 95, 1252–1255. [Google Scholar]
- Cangemi, V.F. Acute pericarditis after smallpox vaccination. N. Engl. J. Med. 1958, 258, 1257–1259. [Google Scholar] [CrossRef]
- Taylor, C.L.; Eckart, R.E. Chest pain, ST elevation, and positive cardiac enzymes in an austere environment: Differentiating smallpox vaccination-mediated myocarditis and acute coronary syndrome in Operation Iraqi Freedom. J. Emerg. Med. 2012, 42, 267–270. [Google Scholar] [CrossRef]
- Murphy, J.G.; Wright, R.S.; Bruce, G.K.; Baddour, L.M.; Farrell, A.M.; Edwards, W.D.; Kita, H.; Cooper, L.T. Eosinophilic-lymphocytic myocarditis after smallpox vaccination. Lancet 2003, 362, 1378–1380. [Google Scholar] [CrossRef]
- Guerdan, B.R.; Shumway, G.J. Case Report: A Presumptive Case of Vaccinia Myocarditis. Mil. Med. 2004, 169, 866–867. [Google Scholar] [CrossRef] [Green Version]
- Docekal, J.W.; Francisco, G.; Lee, J.C. Recurrent epicardial ventricular tachycardia following smallpox vaccination. Heart Rhythm Case Rep. 2018, 5, 6–9. [Google Scholar] [CrossRef]
- Finlay-Jones, L.R. Fatal myocarditis after vaccination against smallpox—Report of a case. N. Engl. J. Med. 1964, 270, 41–42. [Google Scholar] [CrossRef]
- Dalgaard, J.B. Fatal myocarditis following smallpox vaccination. Am. Heart J. 1957, 54, 156–157. [Google Scholar] [CrossRef]
- Bruner, D.I.; Butler, B.S. Smallpox vaccination-associated myopericarditis is more common with the newest smallpox vaccine. J. Emerg. Med. 2014, 46, e85–e87. [Google Scholar] [CrossRef]
- Lin, A.H.; Phan, H.A.; Barthel, R.V.; Maisel, A.S.; Crum-Cianflone, N.F.; Maves, R.C.; Nayak, K.R. Myopericarditis and pericarditis in the deployed military member: A retrospective series. Mil. Med. 2013, 178, 18–20. [Google Scholar] [CrossRef] [Green Version]
- Makaryus, A.N.; Revere, D.J.; Steinberg, B. Recurrent reversible dilated cardiomyopathy secondary to viral and streptococcal pneumonia vaccine-associated myocarditis. Cardiol. Rev. 2006, 14, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, P.; Gertner, E.; McEvoy, C.E. Severe polyserositis induced by the 13-valent pneumococcal conjugate vaccine: A case report. J. Med. Case Rep. 2017, 11, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccara, F.; Benhaiem-Sigaux, N.; Cohen, A. Acute myopericarditis after diphtheria, tetanus, and polio vaccination. Chest 2001, 120, 671–672. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Hashimoto, T.; Ohta-Ogo, K.; Ishibashi-Ueda, H.; Imanaka-Yoshida, K.; Hiroe, M.; Yokochi, T. A case of biopsy-proven eosinophilic myocarditis related to tetanus toxoid immunization. Cardiovasc. Pathol. 2018, 37, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.L.; Boroujerdi-Rad, L. Acute myopericarditis after tetanus, diptheria, and pertussis vaccination in a healthy adult. J. Gen. Intern. Med. 2014, 29, S298. [Google Scholar]
- Koutsaimanis, K.G.; Rée, G.H. Possible association of myocardial infarction and active immunization. N. Engl. J. Med. 1978, 299, 153–154. [Google Scholar]
- Karger. Available online: https://wwwkargercom/Article/Pdf/167026 (accessed on 15 December 2021).
- Seferović, P.M.; Tsutsui, H.; McNamara, D.M.; Ristić, A.D.; Basso, C.; Bozkurt, B.; Jr, L.T.C.; Filippatos, G.; Ide, T.; Inomata, T.; et al. Heart Failure Association of the ESC, Heart Failure Society of America and Japanese Heart Failure Society Position statement on endomyocardial biopsy. Eur. J. Hear. Fail. 2021, 23, 854–871. [Google Scholar] [CrossRef]
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; Heidecker, B.; Heymans, S.; Hübner, N.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef]
- Olejniczak, M.; Schwartz, M.; Webber, E.; Shaffer, A.; Perry, T.E. Viral Myocarditis-Incidence, Diagnosis and Management. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1591–1601. [Google Scholar] [CrossRef]
- Cassimatis, D.C.; Atwood, J.E.; Engler, R.M.; Linz, P.E.; Grabenstein, J.D.; Vernalis, M.N. Smallpox vaccination and myopericarditis: A clinical review. J. Am. Coll. Cardiol. 2004, 43, 1503–1510. [Google Scholar] [CrossRef] [Green Version]
- Reif, D.M.; Motsinger-Reif, A.A.; McKinney, B.A.; Rock, M.T.; Crowe, J.E.; Moore, J.H. Integrated analysis of genetic and proteomic data identifies biomarkers associated with adverse events following smallpox vaccination. Genes Immun. 2009, 10, 112–119. [Google Scholar] [CrossRef]
- Rodrigues, B.S.; Alves, M.; Duarte, G.S.; Costa, J.; Pinto, F.J.; Caldeira, D. The impact of influenza vaccination in patients with cardiovascular disease: An overview of systematic reviews. Trends Cardiovasc. Med. 2021, 31, 315–320. [Google Scholar] [CrossRef]
- Reuters. Israel Examining Heart Inflammation Cases in People Who Received Pfizer COVID Shot. Available online: https://www.reuters.com/world/middle-east/israel-examining-heart-inflammation-cases-people-who-received-pfizer-covid-shot-2021-04-25/ (accessed on 15 January 2022).
- Hannah, G.; Rosenblum, M. Use of COVID-19 Vaccines After Reports of Adverse Events Among Adult Recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 Vaccines (Pfizer-BioNTech and Moderna): Update from the Advisory Committee on Immunization Practices—United States, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1094. [Google Scholar]
- Witberg, G.; Barda, N.; Hoss, S.; Richter, I.; Wiessman, M.; Aviv, Y.; Grinberg, T.; Auster, O.; Dagan, N.; Balicer, R.D.; et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N. Engl. J. Med. 2021, 385, 2132–2139. [Google Scholar] [CrossRef]
- Wise, J. Covid-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- Jabagi, M.J.; Botton, J.; Bertrand, M.; Weill, A.; Farrington, P.; Zureik, M.; Dray-Spira, R. Myocardial Infarction, Stroke, and Pulmonary Embolism After BNT162b2 mRNA COVID-19 Vaccine in People Aged 75 Years or Older. JAMA 2022, 327, 80–82. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. [Google Scholar] [CrossRef]
- Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K.; Tropsha, A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines 2021, 9, 1186. [Google Scholar] [CrossRef]
- Lazaros, G.; Klein, A.L.; Hatziantoniou, S.; Tsioufis, C.; Tsakris, A.; Anastassopoulou, C. The Novel Platform of mRNA COVID-19 Vaccines and Myocarditis: Clues into the Potential Underlying Mechanism. Vaccine 2021, 39, 4925–4927. [Google Scholar] [CrossRef]
- Huber, S.A.; Pfaeffle, B. Differential Th1 and Th2 cell responses in male and female BALB/c mice infected with coxsackievirus group B type 3. J. Virol. 1994, 68, 5126–5132. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]


{kind=link}
| Vaccine Type | No. of Studies | No. of Patients | Average Time of Symptom Onset from Vaccination (Days) | Mean Age (±SD) | Gender | Types of Events | Outcome |
|---|---|---|---|---|---|---|---|
| Influenza vaccine | 11 | 34 | 4.77 | 68.55 ± 18.23 | Males: 15 Females: 19 | Myocarditis: 2 Pericarditis: 27 Pericardial effusion: 2 Takotsubo: 2 Kounis syndrome: 1 | Recovery in all patients |
| COVID-19 vaccines. Subtype: J&J: 1 Pfizer: 35 Moderna: 26 Covishield: 4 CoronaVac: 1 | 18 | 67 | 2.34 | 42.733 ± 19.6 | Males: 59 Females: 8 | Myocarditis: 55 MI: 6 Acute myocardial injury: 1 Type 1 Kounis syndrome: 1 MINOCA: 1 Pericarditis: 2 | 1 death. Recovery in all other patients. |
| Smallpox vaccine | 20 | 232 | 16.68 | 29.48 ± 8.97 | Males: 192 Females: 29 NR: 11 | Myocarditis: 75 Pericarditis: 7 Myopericarditis: 121 Ischemic events: 26 DCM: 2 Trigeminy: 1 Ventricular tachycardia: 1 | 1 death. Recovery in all other patients. |
| Pneumococcal Vaccine | 2 | 2 | 18 | 73.00 ± 2.8 | Females: 2 | Myocarditis: 1, Pericardial effusion: 1 | Recovery in all patients |
| Tetanus toxoid | 3 | 3 | 3 | 25.66 ± 6.8 | Males: 3 | Myocarditis: 2 Myopericarditis: 1 | Recovery in all patients |
| Cholera | 1 | 1 | 6 | 40 | Male: 1 | Myocardial infarction: 1 | Recovery |
| Rabies | 1 | 1 | NR | 58 | Male: 1 | Myocarditis: 1 | NR |
| Author, Year | Country | Type of Study | Number of Cases | Median Age | Gender | Patient Comorbidities | Event | Dose after Which Event Happened | Days after Vaccination Symptoms | Treatment | Outcome | Was EMB Done? If Yes, Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chuen-Der Kao et al., 2003 [10] | Taiwan | Case report | 1 | 68 | F | NR | Pericarditis | 1 | 14 | Plasmapheresis | R | N |
| Y J Kim et al., 2017 [11] | Korea | Case report | 1 | 27 | F | NR | Myocarditis | 1 | 3 | ECMO | R | N |
| De Meester et al., 2000 [13] | Belgium | Case Report | 2 | 75, 40 | M | 1: CKD, DM, smoker, 2: smoker, hyperlipidemia | 1: pericardial effusion on echo, 2: pericarditis | 1 | 4 | NSAIDs | R | N |
| Santoro et al., 2013 [14] | Italy | Case report | 1 | 78 | M | NR | TTC | 1 | 3 | Furosemide, ramipril, and bisoprolol | R | N |
| Singh et al., 2013 [15] | Australia | Case report | 1 | 86 | F | NR | TTC | 1 | 1 | NA | R | N |
| Streifler et al., 1981 [16] | Israel | Case report | 1 | 61 | M | NR | Pericarditis | 1 | 7 | NSAIDs | R | N |
| Cheng et al., 2016 [17] | Canada | Case report | 1 | 65 | M | None | Myocarditis | 1 | 5 | NA | R | N |
| Mei et al.,2018 [12] | Italy | Case report | 1 | 87 | M | COPD, thyroidectomy, MI, total AV block with SSS | Pericardial effusion | 2 | 1st event: 5–7 days; 2nd event: few days; 3rd event: relapse: 8 months later | Prednisone pericardiocentesis | R | N |
| Garcia et al., 2013 [20] | Spain | Case report | 1 | 69 | M | IHD | Kounis syndrome | 1 | 15 min | Nitroglycerin | R | N |
| Zanettini et al., 2003 [18] | Brazil | Case series | 23 | <40: 1; 40–59: 3; ≥60: 19 | 16 F, 7 M | Obesity: 10, smokers: 10, HTN: 3, IHD: 2, HLD: 6, mitral valvopathy: 13, HTN cardiomyopathy: 8, arrythmias: 7, COPD: 3. MI: 1, hypothyroidism: 1 | Pericarditis | 1 | NA | 19 patients: NSAIDs | R | N |
| Godreuil et al., 1983 [19] | France | Case report | 1 | 87 | M | NR | Hemorrhagic pericarditis | 1 | NA | Surgical pericardiectomy, colchicine | R | N |
| Author, Year | Country | Type of Study | Type of Vaccine | Number of Cases | Median Age | Gender | Patient Comorbidities | Event | Dose after Which Event Happened | Days after Vaccination Symptoms | Treatment | Outcome | Was EMB Done? If Yes, Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rosner et al., 2021 [6] | USA | Case series | J&J: 1, Pfizer: 5, Moderna: 1 | 7 | 28, 39, 39, 24, 19, 20, 23 | 7 M | NR | Myocarditis | 1: 2 pts, 2: 5 pts | 3 to 7 days | NA | R | 1/7: One patient underwent endomyocardial biopsy without pathological evidence of myocarditis |
| Kim et al., 2021 [7] | USA | Retrospective | Pfizer: 2, Moderna: 2 | 4 | 36, 23, 70, 24 | 3 M, 1 F | Pt 3: HTN, HLD, cigarette smoking; Others: None | Myocarditis | 2: 4 pts | 3, 5, 1, 2 | 1: Colchicine, NSAIDs; 2: Colchicine, corticosteriods; 3: Nothing; 4: Colchicine, NSAIDs | R | N |
| Larson et al., 2021 [8] | Case series | Moderna: 3, Pfizer: 5 | 8 | 22, 31, 40, 56, 26, 35, 21, 22 | 8 M | NR | Myocarditis | 1: 7 pts, 2: 1 pts | 2–4 days | 5 pts were treated with NSAIDs, colchicine, and prednisone | R | N | |
| Mansour et al., 2021 [9] | USA | Case series | Moderna: 2 | 2 | 25, 21 | 1 M, 1 F | NR | Myocarditis | 2: 2 pts | 1: same day; 2: the next day | Pt. 2 metoprolol | R | N |
| Lee et al., 2021 [23] | Singapore | Case Series | Pfizer: 3 | 3 | 70, 44, 73 | 3 F | 1: Type 2 DM, HTN, HLD, prior CVA; 2: Mitral valve prolapse and mild mitral regurgitation; 3: HTN | 1: STEMI with 100% LCX occlusion; 2: Stress-induced cardiomyopathy; 3: MINOCA | 1: 3 pts | 1: same day; 2: same day; 3: same day | Pt. 1: PCI | R | N |
| Habib et al., 2021 [24] | Qatar | Case report | Pfizer: 1 | 1 | 37 | M | HTN | Myocarditis | 2: 1 | 3 days | LHC | R | N |
| Abu Mouch et al., 2021 [25] | Israel | Case series | Pfizer: 6 | 6 | 1: 24, 2: 20, 3: 29, 4: 45, 5: 16, 6: 17 | 6 M | NR | Myocarditis | 1: 1 pt, 2: 5 pts | 1: 72 h, 2: 24 h, 3: 48 h, 4: 16 days, 5: 24 h, 6: 72 h | NSAIDs and colchicine; | R | N |
| Chatterjee et al., 2021 [26] | India | Case report | Covishield: 1 | 1 | 63 | M | NR | Myocardial infarction | 2 | 48 h | Thrombolysis | R | N |
| Deb et al., 2021 [27] | USA | Case report | Moderna: 1 | 1 | 67 | M | HTN, DM 2, HLD, CAD s/p stents and CABG | Acute myocardial injury | 2 | 6 h | Diuretics | R | N |
| Albert et al., 2021 [28] | USA | Case report | Moderna: 1 | 1 | 24 | M | NR | Myocarditis | 2 | 24 h | Beta-blocker | R | N |
| Ammirati et al., 2021 [31] | USA | Case report | Pfizer: 1 | 1 | 56 | M | NR | Acute myocarditis | 2 | 3 days | NA | R | N |
| Özdemir et al., 2021 [34] | Turkey | Case report | CoronaVac: 1 | 1 | 41 | F | NR | Type 1 Kounis syndrome | 1 | 15 min | N | ||
| D’Angelo et al., 2021 [29] | Italy | Case report | Pfizer: 1 | 1 | 30 | M | NR | Myocarditis | 2 | 72 h | N | ||
| Tajstra et al., 2021 [32] | Poland | Case report | Pfizer: 1 | 1 | 86 | M | Prostate cancer, Paroxysmal A.fib. | Acute MI | 1 | 30 min | N | ||
| Montgomery et al., 2021 [22] | USA | Case series | Pfizer: 7, Moderna:16 | 23 | Median age: 25 | 23 M | NR | Myocarditis | 1: 3 pt; 2: 20 pts | 4 days | N | ||
| Watad et al., 2021 [35] | Israel | Case series | Pfizer: 2 | 2 | 48, 66 | 1 M, 1 F | Pt 1: HTN, HLD, HCM; Pt 2: Idiopathic pericarditis, anemia, DVT, spontaneous abortion in 1st trimester | 1: pericarditis; 2: pericarditis | 1: 2 pts; 1 pt had relapse after 2nd dose | 1: after 4 days for both events; 2: 2 days | N | ||
| Watkins et al., 2021 [30] | USA | Case report | Pfizer: 1 | 1 | 20 | M | NR | Myocarditis | 2 | 2 days | N | ||
| Srinivasan et al., 2021 [33] | India | Case series | Covishield: 3 | 3 | 46, 48, 75 | 2 M, 1 F | 1: DM, HTN; 2: DM, HTN, CAD; 3: NA | 1: TVD, MI RCA occlusion, 2: LAD occlusion MI; 3: TVD, occlusion of postero-lateral branch of RCA | 2: 2 pts, 1: 1 pt | 1: 12 days; 2: 6 days; 3: 1 day | N |
| Author, Year | Country | Type of Study | Number of Cases | Mean Age (Years) | Gender | Patient Comorbidities | Event | Dose after Which Event Happened | Days after Vaccination Symptoms | Treatment | Outcome | EMB(Y/N). If Y, findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Whitman et al., 2003 [36] | USA | Case Report | 1 | 29 | F | NR | Frequent episodes of trigeminy associated with symptoms of palpitations | 1 | 10 | Beta blocker | R | N |
| Lin et al., 2013 [55] | USA | Retrospective | 11 | NA | NA | NR | 4 pericarditis, 7 myopericarditis | 1 | 21 | Supportive | R | N |
| Engler et al., 2015 [37] | USA | Prospective Cohort | 5 | NA | 4 M, 1 F | NR | 4 pts myocarditis; 1 pt pericarditis | 1 | NA | Supportive | R | N |
| NR | All pts: subclinical myocarditis | 1 | NA | Supportive | R | N | ||||||
| Eckart et al., 2004 [38] | USA | Systematic surveillance | 67 | 26.6 | 66 M, 1 F | NR | 67 myocarditis | 1 | 10.4 | Supportive | 1 fatality: 33 days after multiple vaccinations | Y,1 fatality. Autopsy: eosinophilic epicardial inflammation; |
| Sarkisian et al., 2019 [39] | USA | Case Series | 6 | 23 | 6 M | NR | 2 cases: myocarditis; 4 cases: myopericarditis | 1 | 10.5 | Pt1. colchicine, Pt2. NSAIDs, colchicine, Pt.3. NSAIDs, Pt4. NA, Pt5. NSAIDs, colcichine, Pt6. NSAIDs | R | N |
| Saurina et al., 2003 [40] | USA | Case series | 1 | 20 | M | NR | Myocarditis | 1 | 8 | NSAIDs | R | N |
| Sharma et al., 2011 [41] | USA | Case Series | 2 | 34 | 2 M | NR | 1 case myocarditis, 1 case myopericarditis | 1 | 12 | NSAIDs | R | N |
| Sniadack et al., 2008 [42] | USA | Cohort prospective | 33 | 13 M, 20 F | NR | 10 cases: ischemic event, 2 cases: DCM and 21 cases: myopericarditis | 1: 4 pts; Revaccinee: 29 pts; | 11 | Supportive | R | N | |
| Keinath et al., 2018 [43] | USA | Case study | 1 | 36 | M | NR | 1 myocarditis | 1 | 70 | Cardioversion, ICD placement, GDMT for HF | R | N |
| Halsell et al., 2003 [44] | USA | Case series | 18 | 26.5 | 18 M | NR | 18 cases of myopericarditis | 1 | 10.5 | Supportive | R | Y, eosinophilic infiltration |
| Mathews et al., 1974 [45] | England | Case report | 1 | 25 | M | NR | 1 myopericarditis | 1 | 14 | Hydrocortisone, Prednisone Digoxin and furosemide | R | N |
| Eckart et al., 2005 [46] | USA | Retrospective | 62 | 30.2 | 61 M, 1 F | 19% smokers | 62 cases of myocarditis | 1 | Supportive | R | Y,Pt1: no clear cellular infiltrate, Pt2: mild lymphocytic infiltrate; Pt3: eosinophilic infiltrate | |
| 16 | 11 M, 5 F | NR | ACS:16 | 1 | Supportive | R | ||||||
| Cangemi et al., 1958 [47] | USA | Case report | 1 | 56 | M | NR | 1 pericarditis | 1 | 16 | Supportive | R | |
| Taylor et al., 2012 [48] | USA | Case report | 1 | 32 | M | Smoker | 1 myopericarditis | 1 | 14 | Aspirin, morphine, nitroglycerin | R | N |
| Murphy et al., 2003 [49] | USA | Case report | 1 | 29 | M | NR | 1 myocarditis | 1 | 21 | GDMT for HF; prednisone | R | Y,mixed eosinophilic-lymphocytic |
| Guerdan et al., 2004 [50] | USA | Case report | 1 | 26 | M | NR | 1 myocarditis | 1 | 11 | NSAIDS, and pain control | R | N |
| Docekal et al., 2019 [51] | USA | Case report | 1 | 20 | M | NR | Recurrent epicardial V. tach | 1 | 28 | EP ablations were attempted. | R | N |
| Jones et al., 1964 [52] | USA | Case report | 1 | 39 | M | NR | 1 myocarditis | 1 | 11 | Supportive | D | Y,mixed infiltrate of mononuclear cells and edematous IV septum and ventricles; necrotic foci containing eosinphils |
| Dalgaard et al., 1954 [53] | Norway | Case report | 1 | 22 | M | NR | 1 myocarditis | Revaccine | 8 | Supportive | D | Y,Autopsy: Numerous foci of acute degeneration with loss of transverse striation, granular necrosis of myofibrils, and pronounced infiltration with granulocytes and lymphocytes. Between these areas normal myofibrils were found. |
| Bruner et al., 2014 [54] | USA | Case report | 1 | 27 | M | NR | 1 myopericarditis | 1 | 14 | Thrombolysis | R | N |
| Author, Year | Country | Type of Study | Number of Cases | Median Age | Gender | Patient Comorbidities | Event | Dose after Which Event Happened | Days after Vaccination Symptoms | Treatment | Outcome | EMB |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pneumococcal vaccination | ||||||||||||
| Makaryus et al., 2006 [56] | USA | Case report | 1 | 71 | F | NR | Myocarditis | NA | Supportive: GDMT for HF | R | No | NA |
| Tawfik et al., 2017 [57] | USA | Case report | 1 | 75 | F | NR | Pericardial effusion | 18 | Prednisone for 2 weeks tapered over 3 months | R | Yes; organized effusion containing hemorrhage, acute inflammation with reactive changes and mesothelial hyperplasia | NA |
| Tdap vaccination | ||||||||||||
| Boccara et al., 2001 [58] | USA | Case report | 1 | 31 | M | NR | Myopericarditis | Re vaccine | NA | Aspirin | R | Y; arteriolar smooth muscle contraction was prominent with increased permeability demonstrated by interstitial edema and diapedesis of erythrocytes. |
| Clark et al., 2014 [60] | USA | Case Report | 1 | 28 | M | Smoker | Myopericarditis | Re vaccine | 3 days | Colchicine and DAPT | R | N |
| Tetanus Toxoid | ||||||||||||
| Yamamoto et al., 2018 [59] | Japan | Case report | 1 | 18 | M | NR | Myocarditis | Re-vaccine | NA | Steroids | R | Yes: perivascular eosinophilic infiltrates with myocyte necrosis and abundant interstitial lymphocytic infiltrates with myocyte necrosis, separately. Numerous eosinophilic infiltrations with degranulating eosinophils were observed in the perivascular regions. Perivascular interstitial fibrosis was also observed Immunostaining for eosinophilic cationic protein showed extensive staining in the myocardial interstitium. |
| Cholera vaccine | ||||||||||||
| Koutsaimanis et al., 1978 [61] | England | Case Report | 1 | 40 | M | NR | Anterior wall MI | 1 | 6 days | NA | R | N |
| Rabies vaccine | ||||||||||||
| Lyon et al., 1948 [62] | Jerusalem | Case Report | 1 | 58 | M | NR | Myocarditis | 1 | Few weeks after 14 injections | VItamin B complex and sedrena extract | R | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmar, K.; Subramanyam, S.; Del Rio-Pertuz, G.; Sethi, P.; Argueta-Sosa, E. Cardiac Adverse Events after Vaccination—A Systematic Review. Vaccines 2022, 10, 700. https://doi.org/10.3390/vaccines10050700
Parmar K, Subramanyam S, Del Rio-Pertuz G, Sethi P, Argueta-Sosa E. Cardiac Adverse Events after Vaccination—A Systematic Review. Vaccines. 2022; 10(5):700. https://doi.org/10.3390/vaccines10050700
Chicago/Turabian StyleParmar, Kanak, Sai Subramanyam, Gaspar Del Rio-Pertuz, Pooja Sethi, and Erwin Argueta-Sosa. 2022. "Cardiac Adverse Events after Vaccination—A Systematic Review" Vaccines 10, no. 5: 700. https://doi.org/10.3390/vaccines10050700
APA StyleParmar, K., Subramanyam, S., Del Rio-Pertuz, G., Sethi, P., & Argueta-Sosa, E. (2022). Cardiac Adverse Events after Vaccination—A Systematic Review. Vaccines, 10(5), 700. https://doi.org/10.3390/vaccines10050700