
COVID-19 Vaccination in Health Care Workers in Italy: A Literature Review and a Report from a Comprehensive Cancer Center

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Review
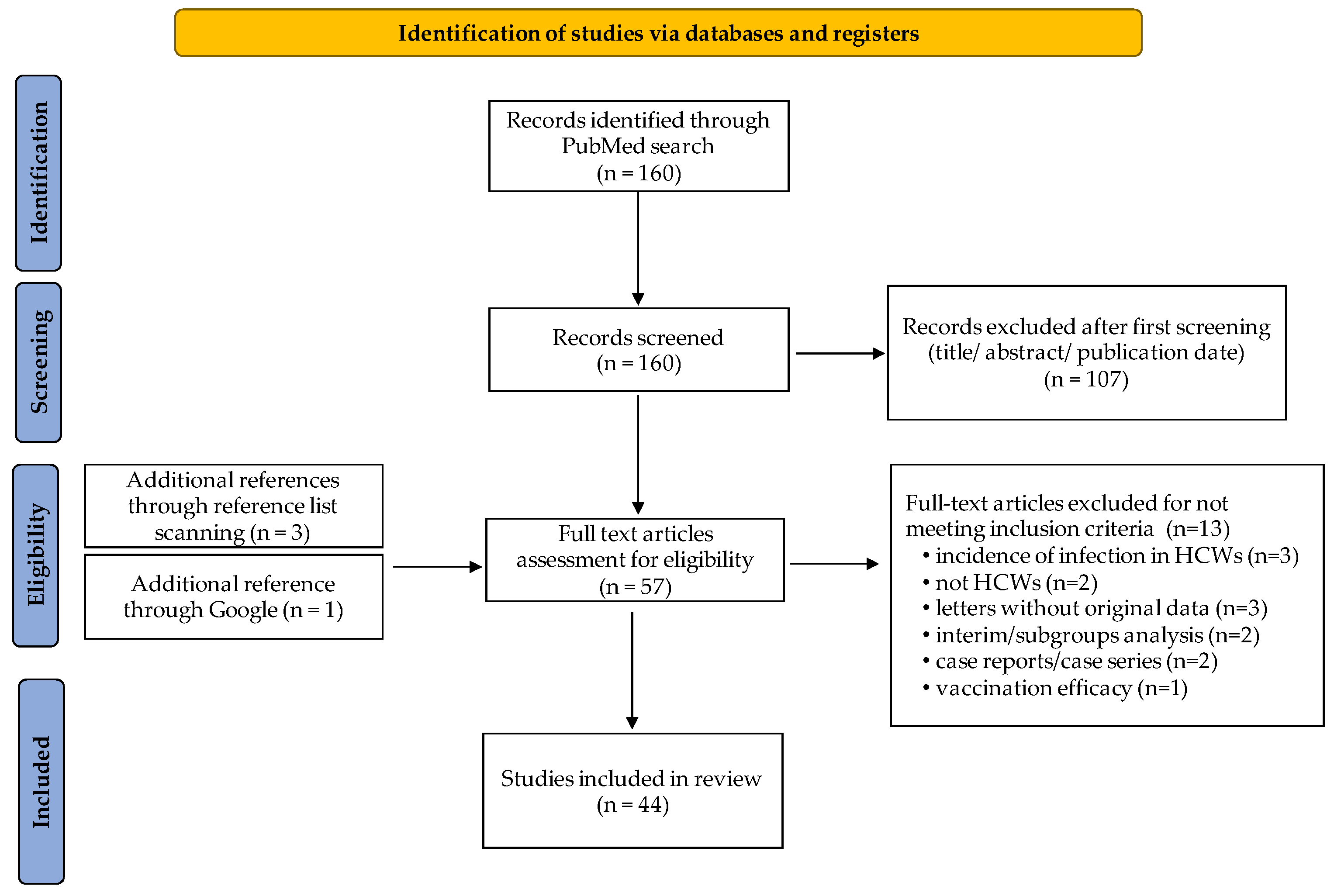
2.1.1. Search Strategy
2.1.2. Study Inclusion and Exclusion Criteria
2.1.3. Data Extraction
2.1.4. Data Synthesis and Analysis
2.2. Antibody Response to BNT162b2 mRNA Vaccine at INT-Milan
2.2.1. Study Design
2.2.2. Evaluation of Anti-SARS-CoV-2-Spike Antibody
2.2.3. Statistical Analysis
3. Results
3.1. Literature Review
Studies Identification and Characteristics
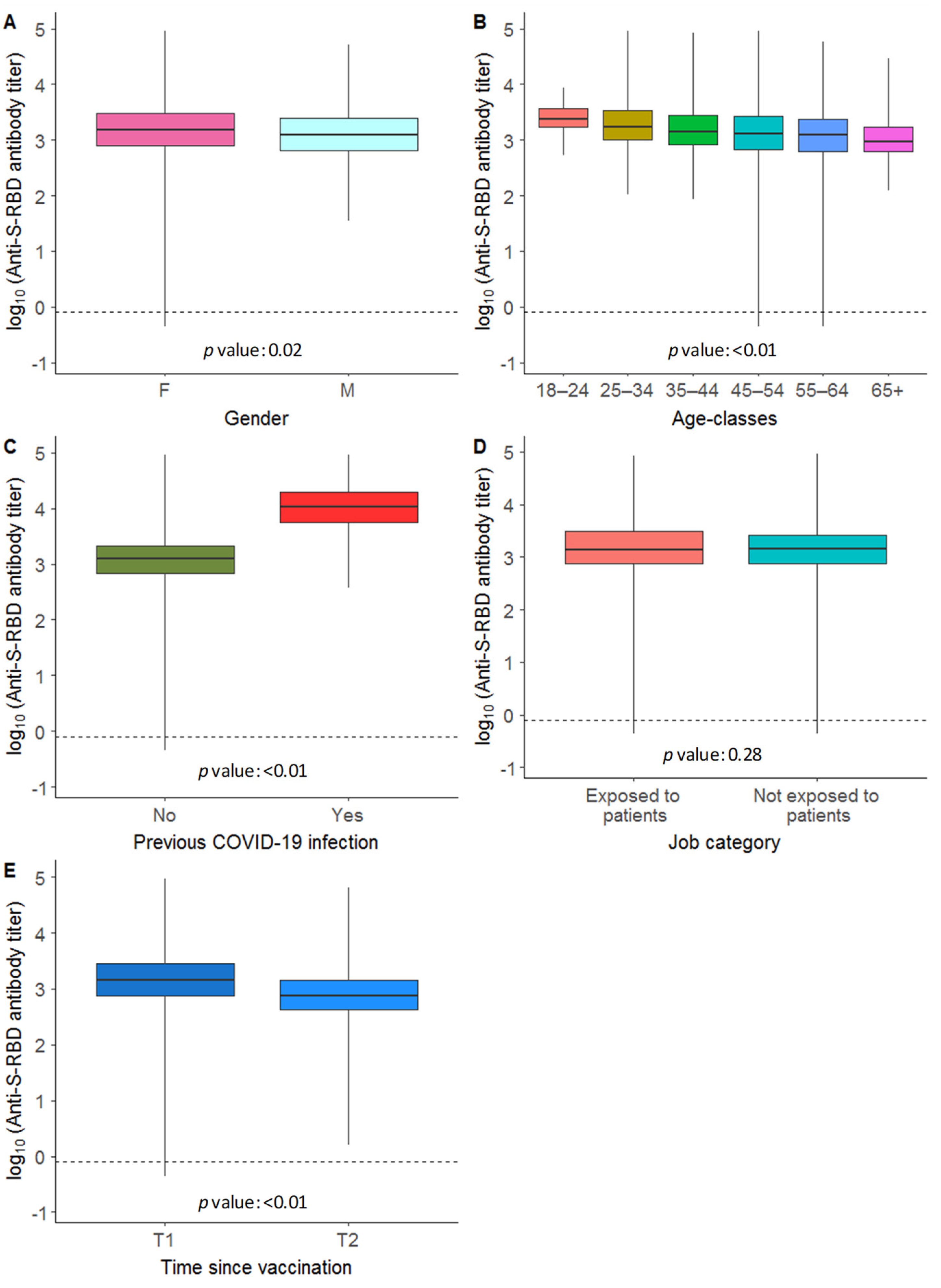
3.2. Antibody Response to BNT162b2 mRNA Vaccine at INT-Milan
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between MRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Della Polla, G.; Pelullo, C.P.; Di Giuseppe, G.; Angelillo, I.F. Changes in Behaviors and Attitudes in Response to COVID-19 Pandemic and Vaccination in Healthcare Workers and University Students in Italy. Vaccines 2021, 9, 1276. [Google Scholar] [CrossRef]
- Circolare 24 Dicembre 2020—Raccomandazioni per L’organizzazione della Campagna Vaccinale contro SARS-CoV-2/COVID-19 e Procedure di Vaccinazione. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto&tab=2 (accessed on 26 January 2022).
- Direzione Generale Della Prevenzione Sanitaria. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2021&codLeg=78398&parte=1%20&serie=null (accessed on 26 January 2022).
- Craxì, L.; Casuccio, A.; Amodio, E.; Restivo, V. Who Should Get COVID-19 Vaccine First? A Survey to Evaluate Hospital Workers’ Opinion. Vaccines 2021, 9, 189. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Primary COVID-19 Vaccine Cycle and Booster Doses Efficacy: Analysis of Italian Nationwide Vaccination Campaign. Eur. J. Public Health 2022, 32, 328–330. [Google Scholar] [CrossRef]
- Coppeta, L.; Ferrari, C.; Somma, G.; Mazza, A.; D’Ancona, U.; Marcuccilli, F.; Grelli, S.; Aurilio, M.T.; Pietroiusti, A.; Magrini, A.; et al. Reduced Titers of Circulating Anti-SARS-CoV-2 Antibodies and Risk of COVID-19 Infection in Healthcare Workers during the Nine Months after Immunization with the BNT162b2 MRNA Vaccine. Vaccines 2022, 10, 141. [Google Scholar] [CrossRef]
- Milazzo, L.; Pezzati, L.; Oreni, L.; Kullmann, C.; Lai, A.; Gabrieli, A.; Bestetti, G.; Beschi, C.; Conti, F.; Ottomano, C.; et al. Impact of Prior Infection Status on Antibody Response to the BNT162b2 MRNA COVID-19 Vaccine in Healthcare Workers at a COVID-19 Referral Hospital in Milan, Italy. Hum. Vaccines Immunother. 2021, 17, 4747–4754. [Google Scholar] [CrossRef]
- Greco, M.; Cucci, F.; Portulano, P.; Lazzari, R.A.; Caldararo, C.; Sicuro, F.; Catanese, C.; Lobreglio, G. Effects of Influenza Vaccination on the Response to BNT162b2 Messenger RNA COVID-19 Vaccine in Healthcare Workers. J. Clin. Med. Res. 2021, 13, 549–555. [Google Scholar] [CrossRef]
- Gianfagna, F.; Veronesi, G.; Baj, A.; Dalla Gasperina, D.; Siclari, S.; Drago Ferrante, F.; Maggi, F.; Iacoviello, L.; Ferrario, M.M. Anti-SARS-CoV-2 Antibody Levels and Kinetics of Vaccine Response: Potential Role for Unresolved Inflammation Following Recovery from SARS-CoV-2 Infection. Sci. Rep. 2022, 12, 385. [Google Scholar] [CrossRef]
- Serraino, C.; Melchio, R.; Badinella Martini, M.; Gerbaudo, L.; Fenoglio, L. Response to BNT162b2 MRNA COVID-19 Vaccine among Healthcare Workers in Italy: A 3-Month Follow-up: Comment. Intern. Emerg. Med. 2022, 17, 311–312. [Google Scholar] [CrossRef]
- Azzi, L.; Dalla Gasperina, D.; Veronesi, G.; Shallak, M.; Ietto, G.; Iovino, D.; Baj, A.; Gianfagna, F.; Maurino, V.; Focosi, D.; et al. Mucosal Immune Response in BNT162b2 COVID-19 Vaccine Recipients. EBioMedicine 2022, 75, 103788. [Google Scholar] [CrossRef]
- Vietri, M.T.; Albanese, L.; Passariello, L.; D’Elia, G.; Caliendo, G.; Molinari, A.M.; Angelillo, I.F. Evaluation of Neutralizing Antibodies after Vaccine BNT162b2: Preliminary Data. J. Clin. Virol. 2022, 146, 105057. [Google Scholar] [CrossRef] [PubMed]
- Padoan, A.; Cosma, C.; Bonfante, F.; Della Rocca, F.; Barbaro, F.; Santarossa, C.; Dall’Olmo, L.; Pagliari, M.; Bortolami, A.; Cattelan, A.; et al. Neutralizing Antibody Titers Six Months after Comirnaty Vaccination: Kinetics and Comparison with SARS-CoV-2 Immunoassays. Clin. Chem. Lab. Med. 2022, 60, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Mueller, T. Time Course of Antibody Concentrations against the Spike Protein of SARS-CoV-2 among Healthy Hospital Workers up to 200 Days after Their First COVID-19 Vaccination. J. Clin. Lab. Anal. 2022, 36, e24175. [Google Scholar] [CrossRef] [PubMed]
- Forgeschi, G.; Cavallo, G.; Lorini, C.; Balboni, F.; Sequi, F.; Bonaccorsi, G. Investigating Adherence to COVID-19 Vaccination and Serum Antibody Concentration among Hospital Workers—The Experience of an Italian Private Hospital. Vaccines 2021, 9, 1332. [Google Scholar] [CrossRef]
- Brisotto, G.; Muraro, E.; Montico, M.; Corso, C.; Evangelista, C.; Casarotto, M.; Caffau, C.; Vettori, R.; Cozzi, M.R.; Zanussi, S.; et al. IgG Antibodies against SARS-CoV-2 Decay but Persist 4 Months after Vaccination in a Cohort of Healthcare Workers. Clin. Chim. Acta 2021, 523, 476–482. [Google Scholar] [CrossRef]
- Padoan, A.; Cosma, C.; Bonfante, F.; Rocca, F.D.; Barbaro, F.; Santarossa, C.; Dall’Olmo, L.; Pagliari, M.; Bortolami, A.; Cattelan, A.; et al. SARS-CoV-2 Neutralizing Antibodies after One or Two Doses of Comirnaty (BNT162b2, BioNTech/Pfizer): Kinetics and Comparison with Chemiluminescent Assays. Clin. Chim. Acta 2021, 523, 446–453. [Google Scholar] [CrossRef]
- Firinu, D.; Perra, A.; Campagna, M.; Littera, R.; Fenu, G.; Meloni, F.; Cipri, S.; Sedda, F.; Conti, M.; Miglianti, M.; et al. Evaluation of Antibody Response to BNT162b2 MRNA COVID-19 Vaccine in Patients Affected by Immune-Mediated Inflammatory Diseases up to 5 Months after Vaccination. Clin. Exp. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Pani, A.; Cento, V.; Vismara, C.; Campisi, D.; Di Ruscio, F.; Romandini, A.; Senatore, M.; Schenardi, P.A.; Gagliardi, O.M.; Giroldi, S.; et al. Results of the RENAISSANCE Study: REsponse to BNT162b2 COVID-19 VacciNe—Short- And Long-Term Immune ReSponSe EvAluatioN in Health Care WorkErs. Mayo Clin. Proc. 2021, 96, 2966–2979. [Google Scholar] [CrossRef]
- Piano Mortari, E.; Russo, C.; Vinci, M.R.; Terreri, S.; Fernandez Salinas, A.; Piccioni, L.; Alteri, C.; Colagrossi, L.; Coltella, L.; Ranno, S.; et al. Highly Specific Memory B Cells Generation after the 2nd Dose of BNT162b2 Vaccine Compensate for the Decline of Serum Antibodies and Absence of Mucosal IgA. Cells 2021, 10, 2541. [Google Scholar] [CrossRef]
- Ponticelli, D.; Madotto, F.; Conti, S.; Antonazzo, I.C.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; et al. Response to BNT162b2 MRNA COVID-19 Vaccine among Healthcare Workers in Italy: A 3-Month Follow-Up. Intern. Emerg. Med. 2021, 17, 481–486. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.M.; di Piazza, G.; Pighi, L.; de Nitto, S.; Bragantini, D.; Gianfilippi, G.L.; Lippi, G. Anti-Spike S1 IgA, Anti-Spike Trimeric IgG, and Anti-Spike RBD IgG Response after BNT162b2 COVID-19 MRNA Vaccination in Healthcare Workers. J. Med. Biochem. 2021, 40, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Mangia, A.; Spanò, M.S.; Zaffarano, L.; Viganò, M.; Di Resta, C.; Locatelli, M.; Ciceri, F.; De Vecchi, E. Quantitative Serological Evaluation as a Valuable Tool in the COVID-19 Vaccination Campaign. Clin. Chem. Lab. Med. 2021, 59, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Cassaniti, I.; Bergami, F.; Percivalle, E.; Gabanti, E.; Sammartino, J.C.; Ferrari, A.; Adzasehoun, K.M.G.; Zavaglio, F.; Zelini, P.; Comolli, G.; et al. Humoral and Cell-Mediated Response against SARS-CoV-2 Variants Elicited by MRNA Vaccine BNT162b2 in Healthcare Workers: A Longitudinal Observational Study. Clin. Microbiol. Infect. 2022, 28, 301.e1–301.e8. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Somma, G.; Ferrari, C.; Mazza, A.; Rizza, S.; Trabucco Aurilio, M.; Perrone, S.; Magrini, A.; Pietroiusti, A. Persistence of Anti-S Titre among Healthcare Workers Vaccinated with BNT162b2 MRNA COVID-19. Vaccines 2021, 9, 947. [Google Scholar] [CrossRef] [PubMed]
- Meschi, S.; Matusali, G.; Colavita, F.; Lapa, D.; Bordi, L.; Puro, V.; Leoni, B.D.; Galli, C.; Capobianchi, M.R.; Castilletti, C. Predicting the Protective Humoral Response to a SARS-CoV-2 MRNA Vaccine. Clin. Chem. Lab. Med. 2021, 59, 2010–2018. [Google Scholar] [CrossRef]
- Vicenti, I.; Basso, M.; Gatti, F.; Scaggiante, R.; Boccuto, A.; Zago, D.; Modolo, E.; Dragoni, F.; Parisi, S.G.; Zazzi, M. Faster Decay of Neutralizing Antibodies in Never Infected than Previously Infected Healthcare Workers Three Months after the Second BNT162b2 MRNA COVID-19 Vaccine Dose. Int. J. Infect. Dis. 2021, 112, 40–44. [Google Scholar] [CrossRef]
- Cocomazzi, G.; Piazzolla, V.; Squillante, M.M.; Antinucci, S.; Giambra, V.; Giuliani, F.; Maiorana, A.; Serra, N.; Mangia, A. Early Serological Response to BNT162b2 MRNA Vaccine in Healthcare Workers. Vaccines 2021, 9, 913. [Google Scholar] [CrossRef]
- Malipiero, G.; Moratto, A.; Infantino, M.; D’Agaro, P.; Piscianz, E.; Manfredi, M.; Grossi, V.; Benvenuti, E.; Bulgaresi, M.; Benucci, M.; et al. Assessment of Humoral and Cellular Immunity Induced by the BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers, Elderly People, and Immunosuppressed Patients with Autoimmune Disease. Immunol. Res. 2021, 69, 576–583. [Google Scholar] [CrossRef]
- Ragone, C.; Meola, S.; Fiorillo, P.C.; Penta, R.; Auriemma, L.; Tornesello, M.L.; Miscio, L.; Cavalcanti, E.; Botti, G.; Buonaguro, F.M.; et al. HLA Does Not Impact on Short-Medium-Term Antibody Response to Preventive Anti-SARS-CoV-2 Vaccine. Front. Immunol. 2021, 12, 734689. [Google Scholar] [CrossRef]
- Buonfrate, D.; Piubelli, C.; Gobbi, F.; Martini, D.; Bertoli, G.; Ursini, T.; Moro, L.; Ronzoni, N.; Angheben, A.; Rodari, P.; et al. Antibody Response Induced by the BNT162b2 MRNA COVID-19 Vaccine in a Cohort of Health-Care Workers, with or without Prior SARS-CoV-2 Infection: A Prospective Study. Clin. Microbiol. Infect. 2021, 27, 1845–1850. [Google Scholar] [CrossRef]
- Lombardi, A.; Consonni, D.; Oggioni, M.; Bono, P.; Uceda Renteria, S.; Piatti, A.; Pesatori, A.C.; Castaldi, S.; Muscatello, A.; Riboldi, L.; et al. SARS-CoV-2 Anti-Spike Antibody Titres after Vaccination with BNT162b2 in Naïve and Previously Infected Individuals. J. Infect. Public Health 2021, 14, 1120–1122. [Google Scholar] [CrossRef]
- Mariani, M.; Acquila, M.; Tripodi, G.; Spiazzi, R.; Castagnola, E. Antibodies against Receptor Binding Domain of SARS-CoV-2 Spike Protein Induced by BNT162b2 Vaccine: Results from a Pragmatic, Real-Life Study. J. Infect. Public Health 2021, 14, 1560–1562. [Google Scholar] [CrossRef] [PubMed]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Early Onset of SARS-CoV-2 Antibodies after First Dose of BNT162b2: Correlation with Age, Gender and BMI. Vaccines 2021, 9, 685. [Google Scholar] [CrossRef]
- Puro, V.; Castilletti, C.; Agrati, C.; Goletti, D.; Leone, S.; Agresta, A.; Cimini, E.; Tartaglia, E.; Casetti, R.; Colavita, F.; et al. Impact of Prior Influenza and Pneumoccocal Vaccines on Humoral and Cellular Response to SARS-CoV-2 BNT162b2 Vaccination. Vaccines 2021, 9, 615. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.M.; Pighi, L.; De Nitto, S.; Gianfilippi, G.L.; Lippi, G. Monitoring of the Immunogenic Response to Pfizer BNT162b2 MRNA COVID-19 Vaccination in Healthcare Workers with Snibe SARS-CoV-2 S-RBD IgG Chemiluminescent Immunoassay. Clin. Chem. Lab. Med. 2021, 59, e377–e379. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Capuano, R.; Donnarumma, G.; Bisecco, A.; Grimaldi, E.; Conte, M.; d’Ambrosio, A.; Coppola, N.; Galdiero, M.; Tedeschi, G. Preliminary Evidence of Blunted Humoral Response to SARS-CoV-2 MRNA Vaccine in Multiple Sclerosis Patients Treated with Ocrelizumab. Neurol. Sci. 2021, 42, 3523–3526. [Google Scholar] [CrossRef] [PubMed]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial Observations on Age, Gender, BMI and Hypertension in Antibody Responses to SARS-CoV-2 BNT162b2 Vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef] [PubMed]
- Di Resta, C.; Ferrari, D.; Viganò, M.; Moro, M.; Sabetta, E.; Minerva, M.; Ambrosio, A.; Locatelli, M.; Tomaiuolo, R. The Gender Impact Assessment among Healthcare Workers in the SARS-CoV-2 Vaccination—An Analysis of Serological Response and Side Effects. Vaccines 2021, 9, 522. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.M.; di Piazza, G.; Pighi, L.; De Nitto, S.; Bragantini, D.; Gianfilippi, G.L.; Lippi, G. Anti-SARS-CoV-2 Receptor-Binding Domain Total Antibodies Response in Seropositive and Seronegative Healthcare Workers Undergoing COVID-19 MRNA BNT162b2 Vaccination. Diagnostics 2021, 11, 832. [Google Scholar] [CrossRef]
- Zaffina, S.; Alteri, C.; Ruggiero, A.; Cotugno, N.; Vinci, M.R.; Camisa, V.; Santoro, A.P.; Brugaletta, R.; Deriu, G.; Piano Mortari, E.; et al. Induction of Immune Response after SARS-CoV-2 MRNA BNT162b2 Vaccination in Healthcare Workers. J. Virus Erad. 2021, 7, 100046. [Google Scholar] [CrossRef]
- Cavalcanti, E.; Isgrò, M.A.; Rea, D.; Di Capua, L.; Trillò, G.; Russo, L.; Botti, G.; Miscio, L.; Buonaguro, F.M.; Bianchi, A.A.M. Vaccination Strategy and Anti-SARS-CoV-2 S Titers in Healthcare Workers of the INT-IRCCS “Fondazione Pascale” Cancer Center (Naples, Italy). Infect. Agents Cancer 2021, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central Obesity, Smoking Habit, and Hypertension Are Associated with Lower Antibody Titres in Response to COVID-19 MRNA Vaccine. Diabetes Metab. Res. Rev. 2022, 38, e3465. [Google Scholar] [CrossRef] [PubMed]
- Padoan, A.; Dall’Olmo, L.; Rocca, F.D.; Barbaro, F.; Cosma, C.; Basso, D.; Cattelan, A.; Cianci, V.; Plebani, M. Antibody Response to First and Second Dose of BNT162b2 in a Cohort of Characterized Healthcare Workers. Clin. Chim. Acta 2021, 519, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 MRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. [Google Scholar] [CrossRef]
- Callegaro, A.; Borleri, D.; Farina, C.; Napolitano, G.; Valenti, D.; Rizzi, M.; Maggiolo, F. Antibody Response to SARS-CoV-2 Vaccination Is Extremely Vivacious in Subjects with Previous SARS-CoV-2 Infection. J. Med. Virol. 2021, 93, 4612–4615. [Google Scholar] [CrossRef]
- Mueller, T. Antibodies against Severe Acute Respiratory Syndrome Coronavirus Type 2 (SARS-CoV-2) in Individuals with and without COVID-19 Vaccination: A Method Comparison of Two Different Commercially Available Serological Assays from the Same Manufacturer. Clin. Chim. Acta 2021, 518, 9–16. [Google Scholar] [CrossRef]
- Agrati, C.; Castilletti, C.; Goletti, D.; Meschi, S.; Sacchi, A.; Matusali, G.; Bordoni, V.; Petrone, L.; Lapa, D.; Notari, S.; et al. Coordinate Induction of Humoral and Spike Specific T-Cell Response in a Cohort of Italian Health Care Workers Receiving BNT162b2 MRNA Vaccine. Microorganisms 2021, 9, 1315. [Google Scholar] [CrossRef]
- Ponticelli, D.; Antonazzo, I.C.; Caci, G.; Vitale, A.; Della Ragione, G.; Romano, M.L.; Borrelli, M.; Schiavone, B.; Polosa, R.; Ferrara, P. Dynamics of Antibody Response to BNT162b2 MRNA COVID-19 Vaccine after 6 Months. J. Travel Med. 2021, 28, taab173. [Google Scholar] [CrossRef]
- Ciniselli, C.M.; Micali, A.; De Cecco, L.; Notti, P.; Sinno, V.; Luison, E.; Melani, C.C.; Daidone, M.G.; Apolone, G.; Verderio, P.; et al. SARS-CoV-2 Serology Monitoring of a Cancer Center Staff in the Pandemic Most Infected Italian Region. Cancers 2021, 13, 1035. [Google Scholar] [CrossRef]
- Riester, E.; Findeisen, P.; Hegel, J.K.; Kabesch, M.; Ambrosch, A.; Rank, C.M.; Pessl, F.; Laengin, T.; Niederhauser, C. Performance Evaluation of the Roche Elecsys Anti-SARS-CoV-2 S Immunoassay. J. Virol. Methods 2021, 297, 114271. [Google Scholar] [CrossRef]
- Apolone, G.; Mosconi, P.; Ware, J.E., Jr. Questionario Sullo Stato di Salute SF-36. Manuale D’uso e Guida All’interpretazione dei Risultati; Guerini e Associati: Milan, Italy, 1997. [Google Scholar]
- Infantino, M.; Pieri, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Calugi, G.; Pancani, S.; Benucci, M.; Casprini, P.; et al. The WHO International Standard for COVID-19 Serological Tests: Towards Harmonization of Anti-Spike Assays. Int. Immunopharmacol. 2021, 100, 108095. [Google Scholar] [CrossRef] [PubMed]
- Bertram, S.; Blazquez-Navarro, A.; Seidel, M.; Hölzer, B.; Seibert, F.S.; Doevelaar, A.; Rohn, B.; Zgoura, P.; Witte-Lack, A.; Skrzypczyk, S.; et al. Predictors of Impaired SARS-CoV-2 Immunity in Healthcare Workers after Vaccination with BNT162b2. Sci. Rep. 2022, 12, 6243. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination with BNT162b2 and MRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Ikezaki, H.; Nomura, H.; Shimono, N. Dynamics of Anti-Spike IgG Antibody Level after the Second BNT162b2 COVID-19 Vaccination in Health Care Workers. J. Infect. Chemother. 2022, 28, 802–805. [Google Scholar] [CrossRef]
- Herzberg, J.; Fischer, B.; Lindenkamp, C.; Becher, H.; Becker, A.-K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Persistence of Immune Response in Health Care Workers After Two Doses BNT162b2 in a Longitudinal Observational Study. Front. Immunol. 2022, 13, 839922. [Google Scholar] [CrossRef]
- Borroni, E.; Consonni, D.; Cugno, M.; Lombardi, A.; Mangioni, D.; Bono, P.; Oggioni, M.; Uceda Renteria, S.; Bordini, L.; Nava, C.D.; et al. Side Effects among Healthcare Workers from a Large Milan University Hospital after Second Dose of BNT162b2 MRNA COVID-19 Vaccine. Med. Lav. 2021, 112, 477–485. [Google Scholar] [CrossRef]
- Ripabelli, G.; Tamburro, M.; Buccieri, N.; Adesso, C.; Caggiano, V.; Cannizzaro, F.; Di Palma, M.A.; Mantuano, G.; Montemitro, V.G.; Natale, A.; et al. Active Surveillance of Adverse Events in Healthcare Workers Recipients After Vaccination with COVID-19 BNT162b2 Vaccine (Pfizer-BioNTech, Comirnaty): A Cross-Sectional Study. J. Community Health 2022, 47, 211–225. [Google Scholar] [CrossRef]
- Skrzat-Klapaczyńska, A.; Bieńkowski, C.; Kowalska, J.; Paciorek, M.; Puła, J.; Krogulec, D.; Stengiel, J.; Pawełczyk, A.; Perlejewski, K.; Osuch, S.; et al. The Beneficial Effect of the COVID-19 Vaccine Booster Dose among Healthcare Workers in an Infectious Diseases Center. Vaccines 2022, 10, 552. [Google Scholar] [CrossRef]
- Hueda-Zavaleta, M.; Gómez de la Torre, J.C.; Cáceres-Del Aguila, J.A.; Muro-Rojo, C.; De La Cruz-Escurra, N.; Arenas Siles, D.; Minchón-Vizconde, D.; Copaja-Corzo, C.; Bardales-Silva, F.; Benites-Zapata, V.A.; et al. Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection. Vaccines 2022, 10, 502. [Google Scholar] [CrossRef]
- Canaday, D.H.; Oyebanji, O.A.; White, E.; Keresztesy, D.; Payne, M.; Wilk, D.; Carias, L.; Aung, H.; Denis, K.S.; Sheehan, M.L.; et al. Significantly Elevated Antibody Levels and Neutralization Titers in Nursing Home Residents after SARS-CoV-2 BNT162b2 MRNA Booster Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| S. No. | First Author | Journal | Institute | Italian Region | Sample Size | Vaccination Campaign Period | Vaccination Protocol |
|---|---|---|---|---|---|---|---|
| 7 | Coppeta L | Vaccines (Basel) | Polyclinic of Roma “Tor Vergata” | Lazio | 793 (173 §) | by 15 March 2021 | BNT162b2 (two doses, three weeks apart) |
| 8 | Milazzo L | Human Vaccines & Immunotheraoeutics | Luigi Sacco University Hospital | Lombardy | 407 | 28 December 2020– | BNT162b2 (two doses) |
| 9 | Greco M | J Clin Med Res | Vito Fazzi Hospital of Lecce | Puglia | 297 | December 2020–April 2021 | BNT162b2 (two doses, three weeks apart) |
| 10 | Gianfagna F | Scientific Reports | ASST Sette Laghi | Lombardy | 175 (137 °) | - | BNT162b2 (two doses, three weeks apart) |
| 11 | Serraino C | Internal and Emergency Medicine | AO Santa Croce & Carle | Piedmont | 2059 | 27 December 2020 and following 3-months | BNT162b2 (ND) |
| 12 | Azzi L | EBioMedicine | ASST dei Sette Laghi | Lombardy | 60 | 30 December 2020–20 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 13 | Vietri MT | J Clin Virol | Clinical Pathology Lab—University of Campania “Luigi Vanvitelli” | Campania | 52 | 7 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 14 | Padoan A | Clin Chem Lab Med | Padua University-Hospital Emergency Department, Infectious Disease and Laboratory Medicine wards | Veneto | 189 | 26 December 2020–10 March 2021 | BNT162b2 (two doses, three weeks apart) [n = 179] single dose for non-naïve SARS-CoV-2 HCWs [n = 10] |
| 15 | Muller T a | J Clin Lab Anal | Hospital of Bolzano Department of Clinical Pathology | Trentino Alto Adige | 34 (24 °) | 29 December 2020–14 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 16 | Forgeschi G | Vaccines (Basel) | Istituto Fiorentino di Cura e Assistenza | Tuscany | 297 (193 °) | January 2021–March 2021 | BNT162b2 (two doses) |
| 17 | Brisotto G | Clin Chim Acta | Centro di Riferimento Oncologico Aviano | Friuli Venezia Giulia | 767 (516 §) | - | BNT162b2 two doses) [n = 722] mRNA-1273 (two doses) [n = 43] unknown [n = 2] |
| 18 | Padoan A | Clin Chim Acta | Padua University-Hospital Emergency Department, Infectious Disease and Laboratory Medicine wards | Veneto | 174 | 26 December 2020–10 March 2021 | BNT162b2 (two doses, three weeks apart) [n = 164] single dose for non-naïve SARS-CoV-2 HCWs [n = 10] |
| 19 | Firinu D | Clin Exp Med | University Hospital of Cagliari | Sardinia | 551 | - | BNT162b2 (two doses, three weeks apart) |
| 20 | Pani A | Mayo Clin Proc | ASST Grande Ospedale Metropolitano Niguarda | Lombardy | 2569 (1886 ^) | - | BNT162b2 (two doses, three weeks apart) * |
| 21 | Piano Mortari E | Cells | Bambino Gesù Children Hospital IRCCS | Lazio | 108 | - | BNT162b2 (two doses, three weeks apart) |
| 22 | Ponticelli D | Intern Emerg Med | Pineta Grande Hospital | Campania | 444 (126 °) | December 2020–January 2021 | BNT162b2 (two doses, three weeks apart) |
| 23 | Salvagno GL | J Med Biochem | Pederzoli Hospital | Veneto | 181 | 4–7 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 24 | Ferrari D | Clin Chem Lab Med | IRCCS San Raffaele Hospital (OSR) IRCCS Orthopedic Institute Galeazzi (IOG) IRCCS Casa Sollievo della Sofferenza Hospital (CSS) | Lombardy Puglia | 4290 [OSR: 3340; IOG: 773; CSS: 177] | 4 January 2021–12 February 2021 | BNT162b2 (two doses, three weeks apart) |
| 25 | Cassaniti I | Clin Microbiol Infect | Fondazione IRCCS Policlinico San Matteo | Lombardy | 145 | 27 December 2020–11 February 2021 | BNT162b2 (two doses) |
| 26 | Coppeta L | Vaccines (Basel) | University hospital “Tor Vergata” * | Lazio | 300 | vaccination cycle completion within 15 March 2021 | BNT162b2 (two doses) |
| 27 | Meschi S | Clin Chem Lab Med | National Institute for Infectious Diseases “L. Spallanzani”—IRCCS | Lazio | 120 | December–February 2021 | BNT162b2 (two doses, three weeks apart) |
| 28 | Vicenti I | Int J Infect Dis | - | - | 62 (36 §§) | - | BNT162b2 (two doses, three weeks apart) |
| 29 | Cocomazzi G | Vaccines (Basel) | IRCCS Casa Sollievo della Sofferenza Hospital | Puglia | 340 | - | BNT162b2 (two doses) |
| 30 | Malipiero G | Immunol Res | - | - | 108 | - | BNT162b2 (two doses, three weeks apart) |
| 31 | Ragone C | Front Immunol | National Cancer Institute “Pascale”—IRCCS | Campania | 56 | - | BNT162b2 (two doses, three weeks apart) single dose for non-naïve SARS-CoV-2 HCWs and titer > 2500 BAU/mL after 1st dose |
| 32 | Buonfrate D | Clin Microbiol Infect | IRCCS Sacro Cuore Don Calabria hospital | Veneto | 1935 | 1 January 2021–30 March 2021 | BNT162b2 (two doses, three weeks apart) |
| 33 | Lombardi A | J Infect Public Health | IRCCS Ospedale Maggiore Policlinico Milan | Lombardy | 3475 | - | BNT162b2 (two doses, three weeks apart) |
| 34 | Mariani M | J Infect Public Health | IRCCS Istituto Giannina Gaslini children’s hospital | Liguria | 1675 | 31 December 2020– | BNT162b2 (two doses, three weeks apart) |
| 35 | Pellini R | Vaccines (Basel) | Istituti Fisioterapici Ospitalieri | Lazio | 252 | - | BNT162b2 (two doses, three weeks apart) * |
| 36 | Puro V | Vaccines (Basel) | National Institute for Infectious Diseases “L. Spallanzani”—IRCCS | Lazio | 710 | 27 December 2020– | BNT162b2 (two doses) |
| 37 | Salvagno GL | Clin Chem Lab Med | Pederzoli Hospital | Veneto | 194 | - | BNT162b2 (two doses, three weeks apart) |
| 38 | Gallo A | Neurol Sci | Neurology Clinic—University of Campania Luigi Vanvitelli * | Campania | 55 | 5 January 2021– | BNT162b2 (two doses, three weeks apart) * |
| 39 | Pellini R | EclincalMedicine | Istituti Fisioterapici Ospitalieri | Lazio | 248 | - | BNT162b2 (two doses, three weeks apart) * |
| 40 | Di Resta C | Vaccines (Basel) | IRCCS San Raffaele Hospital | Lombardy | 3318 | January 2021–15 February 2021 | BNT162b2 (two doses, three weeks apart) |
| 41 | Salvagno GL | Diagnostics | Pederzoli Hospital | Veneto | 925 | 4–15 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 42 | Zaffina S | J Virus Erad | Bambino Gesù Children Hospital IRCCS | Lazio | 965 | 27 December 2020– | BNT162b2 (two doses, three weeks apart) |
| 43 | Cavalcanti E | Infect Agent Cancer | IRCCS Fondazione “Pascale” Cancer Center | Campania | 193 | - | BNT162b2 (two doses, three weeks apart) single dose for non-naïve SARS-CoV-2 HCWs |
| 44 | Watanabe M | Diabetes Metab Res Rev | Policlinico Umberto I of Rome | Lazio | 86 | January/February 2021– | BNT162b2 (two doses, three weeks apart) |
| 45 | Padoan A | Clin Chim Acta | Padua University-Hospital | Veneto | 163 | 26 December 2020–10 March 2021 | BNT162b2 (two doses, three weeks apart) |
| 46 | Gobbi F | J Inf | IRCCS Sacro Cuore Don Calabria hospital * | Veneto | 1958 (158 °) | 1 January 2021–30 March 2021 | BNT162b2 (two doses, three weeks apart) Concomitant infected with the second dose after a median of 75 days [n = 22] |
| 47 | Callegaro A | J Med Virol | ASST Papa Giovanni XXIII * | Lombardy | 184 | - | BNT162b2 (two doses) |
| 48 | Mueller Y | Clin Chim Acta | Hospital of Bolzano Department of Clinical Pathology | Trentino Alto Adige | 34 | 29 December 2020–14 January 2021 | BNT162b2 (two doses, three weeks apart) |
| 49 | Agati C | Microorganisms | National Institute for Infectious Diseases “L. Spallanzani” | Lazio | 35 + 167 | - | BNT162b2 (two doses) |
| 50 | Ponticelli D | Journal of Travel Medicine | Pineta Grande Hospital | Campania | 162 | December 2020–January 2021 | BNT162b2 (two doses, three weeks apart) single dose for non-naïve SARS-CoV-2 HCWs |
| S. No | Age Median | Age Range | Female (%) | Previous Covid19 Infection-Exposure (%) | Assessment of Infection-Exposure | Professional Categories (%) | Comorbidity (≥1) (%) | Side Effect Evaluation |
|---|---|---|---|---|---|---|---|---|
| 7 | 43.9 ^ | 21–77 | 67.50 | 3.15 * | Documented diagnosis of SARS-CoV-2 infection | 33.0% physicians 33.9% nurses 33.0% other | - | - |
| 8 | 45.5 *^ | NE | 74.20 | 17.93 | Questionnaire with information of previous PCR swabs and/or serology tests + anti-N IgG by Abbott chemiluminescent microparticle immunoassay and anti-S IgG SARS-CoV-2 IgG II Quant assay (Abbott, Abbott Park, IL, USA) | 38.8% nurses 30.7% medical doctors 20.9% other 9.6% socio-administrative staff | 4.91% (immunosuppressive medications) | Yes |
| 9 | 42 ^ | 0.8 ^^^ | 63.63 | - | exclusion per protocol | - | none | - |
| 10 | 48.05 ^ | NE | 88.57 | 42.90 | PCR swab result or Serological test’s result | 8.0% physicians 63.4% nurses 15.4% nurse assistants 13.1% administrative [38.86% worked in a COVID-19 unit] | 13.71% autoimmune disease 15.43% chronic disease | - |
| 11 | 43.1 ^ | 11.7 ^^^ | 73.77 | 13.6 | Documented history of infection | - | - | - |
| 12 | 41.2 ^ | 26–62 | 66.70 | 16.67 * | Serological testing or NAAT | - | none (exclusion of glucocorticosteroid and/or immunosuppressant drugs, autoimmune disorders) | Yes |
| 13 | - | 25–70 | 55.77 | 9.62 | PCR swab result and serological test’s result (Abbot Architect SARS-Cov-2) | - | - | - |
| 14 | 42.3 ^ | 24–66 | 69.30 | 8.99 * | Diagnosis of infection by swab results and clinical confirmation | - | 8.9% (cardiovascular diseases, diabetes, respiratory diseases, severe obesity, cancer) | - |
| 15 | 50 | 24–62 | 70.59 | - | exclusion per protocol by documented history of infection and confirmed by T0 serology | - | - | - |
| 16 | - | - | - | 21.4 | Questionnaire | 83.5% health workers * 12.7% administrative * 3.8% naïve workers * | - | - |
| 17 | 46 | 35–55 ^^ | 72.60 | 8.30 | molecular swab analysis | - | - | Yes |
| 18 | 41.8 ^ | 24–65 | 69.00 | 5.75 | At least one positive nasopharyngeal swab test and clinical conformation- | - | 9.7% (cardiovascular disease, diabetes, respiratory disease, severe obesity, cancer) | - |
| 19 | 49.5 * | 35–58 | 64.75 * | 16.76 * | Interview, cross-matching with hospital/laboratory databases, serological test’s result (IgM and IgG Maglumi) | - | 3.55% diabetes * 14.05% current smokers * | Yes |
| 20 | 48 | 36–56 ^^ | 69.60 | 6.3 | Anti-nucleocapsid (N) total Ig seropositivity at day 14 after the second vaccine dose (history of unrecognized contact with SARS-CoV-2) | 32.4% nurses 23.7% medical staff 18.2% other sanitary staff 13.7% administrative 6.5% laboratory staff 3.4% non sanitary staff 2.1% pharmacy and physics staff | 22.7% (cardiovascular disease, hypertension, endocrine disease, autoimmune disease, respiratory disease, diabetes, allergies, hypercholesterolemia, arrhythmia, immunosuppression, multiple sclerosis, coinfection with HIV, coinfection with hepatitis B virus) a 10.8% (obesity) a | Yes |
| 21 | 46.95 ^ | 11.35 ^^^ | 71.30 | 0 | Demonstrated by molecular (Allplex2019-ncov, Seegene, Seoul, South Korea) and antibody assays (Elecsys® Anti-N, Roche, Basel, Switzerland) | - | - | - |
| 22 | 40.7 ^,b | 11.1 ^^^,b | 61.11 b | 5.6 b | interview (history of symptoms compatible with COVID-19, previous laboratory-confirmed SARS-CoV-2 infection) | 12.2% physician 44.4% nurses 6.5% other HCWs 16.7% students 20.3% other c | - | Yes c |
| 23 | 42 | 31–52 ^^ | 59.70 | - | exclusion per protocol by Roche Elecsys AntiSARS-CoV-2 S on Cobas 6000 (Roche Diagnostics, Basel, Switzerland) [cutoff negativity <0.8 U/L] | - | - | - |
| 24 | OSR:44.4 * IOG + CSS: 47.5 * | NE | OSR: 64.07 IOG + CSS: 54.95 | OSR: 9.43 * IOG + CSS: 21.16 * | OSR: by Roche Elecsys AntiSARS-CoV-2 S on Cobas 6000 (Roche Diagnostics, Basel, Switzerland), cross-matching with swab tests and serological test’s result (Liaison SARS-CoV-2- S1/S2 IgG), questionnaire IOG + CSS: by SARS-CoV-2 (COV2, Siemens Healthineers, Erlangen, Germany) | - | - | - |
| 25 | 44 | 21–69 | -- | 12.41 | documented diagnosis | - | - | - |
| 26 | 43 ^ | 21–75 | 61.33 | 0 | interview | 41.7% medical doctors 42.0% nurses 16.3% other HCWs | - | - |
| 27 | 48 | 23–71 | 66.66 | 25.0 | Experienced of previous SARS-CoV-2 infection | - | - | - |
| 28 | 50.5 * | 33–60 * | 69.44 * | 63.89 * | laboratory test’s results by survelliance hospital program | - | - | - |
| 29 | 47.7 ^ | 11.8 ^^^ | 57.30 | 22.1 | Questionnaire, swab and serology test results, clinical data from Regional Registry | - | - | - |
| 30 | 51 ^ | 23–69 | 75.00 | - | exclusion per protocol by PCR swab result | - | NR | - |
| 31 | - | - | - | - | - | - | - | - |
| 32 | 45 | 33–53 ^^ | 63.30 | 16.33 * | confirmed RT-PCR results or any serology positivity at T0 | - | - | Yes |
| 33 | 35–44 § | -- | 71.22 * | 14.59 * | confirmed RT-PCR results or symptoms | - | 7.65% obesity 23.13% current smoking | - |
| 34 | 50 | 36–56 ^^ | 79.30 | 3.52 | confirmed RT-PCR results | - | - | - |
| 35 | 47 ^ | 23–69 | 63.80 * | - | exclusion per protocol by interview, serology or mocrobiological tests by swab | - | 10.31% obesity | - |
| 36 | 43 | 21–75 | 70.00 | - | exclusion per protocol by previous SASR-CoV-2 diagnosis, confirmed RT-PCR result or positive to anti-N and/or anti-S/RBD at T0 or positive to anti-N at T1or T2 | 77.0% direct contact with COVID-19 patients | - | - |
| 37 | 42 | 30–52 ^^ | 59.30 | 15.5 | Snibe IgG anti S-RBD [cutoff > 1 kU/L] | - | - | - |
| 38 | 41.2 | 31.9–55.9 ^^ | 58.00 | 0 | molecular and/or antigenic nasopharyngeal swab and/or (IgM, IgG) antibodies tests) | - | - | - |
| 39 | 47 | 23–69 | 63.70 | - | exclusion per protocol by interview, serology or mocrobiological tests by swab | - | 12.5% hypertension 10.48% obesity | - |
| 40 | NE | NE | 64.40 | 9 | Roche Elecsys Anti-SARS-CoV-2 assay on the Cobas 601 platform [cut-off positivity > 1 COI] | - | - | Yes |
| 41 | 44 ^ | 13 ^^ | 49.40 | 22.3 | total anti-SARS-CoV-2 RBD antibodies positive | - | - | - |
| 42 | 46 | 36–56 ^^ | 69.74 | 0 | by molecular (Allplex2019-nCov, Seegene) and antibody assays (Elecsys® Anti-SARS-CoV-2 Roche) | - | - | - |
| 43 | 48.1 ^ | 31–69 | 51.29 | 18.13 | Seropositive for anti-N immunoglobulins | - | - | - |
| 44 | 29 ^ | 17 ^^^ | 60.50 | - | exclusion per protocol by serology | - | 31.7% current smokers 15.3 hypertensive treat 2.4% diabetic 7.1% dysplipidemic 9.5% obesity | Yes |
| 45 | 42.4 ^ | 11.7 ^^^ | 69.90 | 7.98 * | interview | - | - | |
| 46 | 44.5 ^* | ND | 78.48 | 51.26 * | - | - | - | - |
| 47 | 50 | 24–66 | 67.90 | 28.80 | previous SASR-CoV-2 diagnosis, confirmed RT-PCR result | - | - | - |
| 48 | 50 | 24–62 | 70.59 | - | exclusion per protocol by documented history and confirmed by T0 serology | - | - | - |
| 49 | 42 d | 31–52 ^^,d | 71.00 d | 0 | Anti-nucleprotein IgG (AdviseDx, ARCHITECT® Abbott Diagnostics, Chicago, IL, USA) [cut-off positivity S/CO ≥ 1.4] | 86% direct care of COVID19 patients(d) | - | - |
| 50 | 42.5 ^ | 11.9 ^^^ | 58.00 | 17.28 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciniselli, C.M.; Lecchi, M.; Figini, M.; Melani, C.C.; Daidone, M.G.; Morelli, D.; Zito, E.; Apolone, G.; Verderio, P. COVID-19 Vaccination in Health Care Workers in Italy: A Literature Review and a Report from a Comprehensive Cancer Center. Vaccines 2022, 10, 734. https://doi.org/10.3390/vaccines10050734
Ciniselli CM, Lecchi M, Figini M, Melani CC, Daidone MG, Morelli D, Zito E, Apolone G, Verderio P. COVID-19 Vaccination in Health Care Workers in Italy: A Literature Review and a Report from a Comprehensive Cancer Center. Vaccines. 2022; 10(5):734. https://doi.org/10.3390/vaccines10050734
Chicago/Turabian StyleCiniselli, Chiara Maura, Mara Lecchi, Mariangela Figini, Cecilia C. Melani, Maria Grazia Daidone, Daniele Morelli, Emanuela Zito, Giovanni Apolone, and Paolo Verderio. 2022. "COVID-19 Vaccination in Health Care Workers in Italy: A Literature Review and a Report from a Comprehensive Cancer Center" Vaccines 10, no. 5: 734. https://doi.org/10.3390/vaccines10050734
APA StyleCiniselli, C. M., Lecchi, M., Figini, M., Melani, C. C., Daidone, M. G., Morelli, D., Zito, E., Apolone, G., & Verderio, P. (2022). COVID-19 Vaccination in Health Care Workers in Italy: A Literature Review and a Report from a Comprehensive Cancer Center. Vaccines, 10(5), 734. https://doi.org/10.3390/vaccines10050734