
Short-Term Drop in Antibody Titer after the Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Adults

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anti-SARS-CoV-2-IgG Antibodies
2.3. Surrogate Virus Neutralization Test
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Saciuk, Y.; Kertes, J.; Shamir Stein, N.; Ekka Zohar, A. Effectiveness of a third dose of BNT162b2 mRNA vaccine. J. Infect. Dis. 2021, 225, 30–33. [Google Scholar] [CrossRef]
- Eliakim-Raz, N.; Leibovici-Weisman, Y.; Stemmer, A.; Ness, A.; Awwad, M.; Ghantous, N.; Stemmer, S.M. Antibody Titers Before and After a Third Dose of the SARS-CoV-2 BNT162b2 Vaccine in Adults Aged ≥60 Years. JAMA 2021, 326, 2203. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; Olagne, J.; Cognard, N.; Fafi-Kremer, S.; Caillard, S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326, 1063. [Google Scholar] [CrossRef] [PubMed]
- Ducloux, D.; Colladant, M.; Chabannes, M.; Yannaraki, M.; Courivaud, C. Humoral response after 3 doses of the BNT162b2 mRNA COVID-19 vaccine in patients on hemodialysis. Kidney Int. 2021, 100, 702–704. [Google Scholar] [CrossRef]
- Stumpf, J.; Tonnus, W.; Paliege, A.; Rettig, R.; Steglich, A.; Gembardt, F.; Kessel, F.; Kröger, H.; Arndt, P.; Sradnick, J.; et al. Cellular and Humoral Immune Responses After 3 Doses of BNT162b2 mRNA SARS-CoV-2 Vaccine in Kidney Transplant. Transplantation 2021, 105, e267–e269. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, J.; Vollmer, T.; Fischer, B.; Becher, H.; Becker, A.-K.; Sahly, H.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. A Prospective Sero-epidemiological Evaluation of SARS-CoV-2 among Health Care Workers in a German Secondary Care Hospital. Int. J. Infect. Dis. 2020, 102, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Fischer, B.; Lichtenberg, C.; Müller, L.; Timm, J.; Fischer, J.; Knabbe, C. A combined strategy to detect plasma samples reliably with high anti-SARS-CoV-2 neutralizing antibody titers in routine laboratories. J. Clin. Virol. 2021, 144, 104984. [Google Scholar] [CrossRef] [PubMed]
- Infantino, M.; Manfredi, M.; Stacchini, L.; Cosma, C.; Grossi, V.; Lari, B.; Russo, E.; Amedei, A.; Benucci, M.; Veneziani, F.; et al. The role of neutralizing antibodies by sVNT after two doses of BNT162b2 mRNA vaccine in a cohort of Italian healthcare workers. Clin. Chem. Lab. Med. 2022, 60. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, J.; Fischer, B.; Lindenkamp, C.; Becher, H.; Becker, A.-K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Persistence of Immune Response in Health Care Workers After Two Doses BNT162b2 in a Longitudinal Observational Study. Front. Immunol. 2022, 13, 701. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Adamson, A.; Haljasm, L.; Pauliina Rumm, A.; Maruste, R.; Gerhold, J.M.; Planken, A.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Davidov, Y.; Indenbaum, V.; Tsaraf, K.; Cohen-Ezra, O.; Likhter, M.; Ben Yakov, G.; Halperin, R.; Levy, I.; Mor, O.; Agmon-Levin, N.; et al. A third dose of the BNT162b2 mRNA vaccine significantly improves immune responses among liver transplant recipients. J. Hepatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Munro, A.P.S.; Feng, S.; Janani, L.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; et al. Persistence of immunogenicity after seven COVID-19 vaccines given as third dose boosters following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK: Three month analyses of the COV-BOOST trial. J. Infect. 2022. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, E.; Günal, Ö.; Başbulut, E.; Şen, A. SARS-CoV-2 specific antibody responses in healthcare workers after a third booster dose of CoronaVac or BNT162b2 vaccine. J. Med. Virol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Standing Committee on Vaccination Press Release STIKO. Available online: https://www.rki.de/DE/Content/Kommissionen/STIKO/Empfehlungen/PM_2022-02-03.html (accessed on 4 February 2022).
- Burki, T.K. Fourth dose of COVID-19 vaccines in Israel. Lancet. Respir. Med. 2022, 10, e19. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Stubblefield, W.B.; Talbot, H.K.; Feldstein, L.; Tenforde, M.W.; Rasheed, M.A.U.; Mills, L.; Lester, S.N.; Freeman, B.; Thornburg, N.J.; Jones, I.D.; et al. Seroprevalence of SARS-CoV-2 Among Frontline Healthcare Personnel During the First Month of Caring for COVID-19 Patients—Nashville, Tennessee. Clin. Infect. Dis. 2020, 72, 1645–1648. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Mean ± SD | Median | IQR |
|---|---|---|---|
| Age (M ± SD; years) | 48.03 ± 9.45 | 48.00 | 15 |
| BMI (M ± SD; kg/m2) | 25.61 ± 4.71 | 24.69 | 6.16 |
| Sex | n (%) | ||
| Women (%) | 73 (75.3) | ||
| Men (%) | 24 (24.7) | ||
| Comorbidities | n (%) | ||
| Cardiac (%) | 20 (20.62) | ||
| Pulmonary (%) | 9 (9.28) | ||
| Metabolic (%) | 18 (18.56) | ||
| Immunologic (%) | 1 (1.03) | ||
| Other (%) | 18 (18.56) | ||
| Smoking (%) | 25 (25.77) | ||
| Mean ± SD | Median | IQR | |
|---|---|---|---|
| Immunoglobulin G | |||
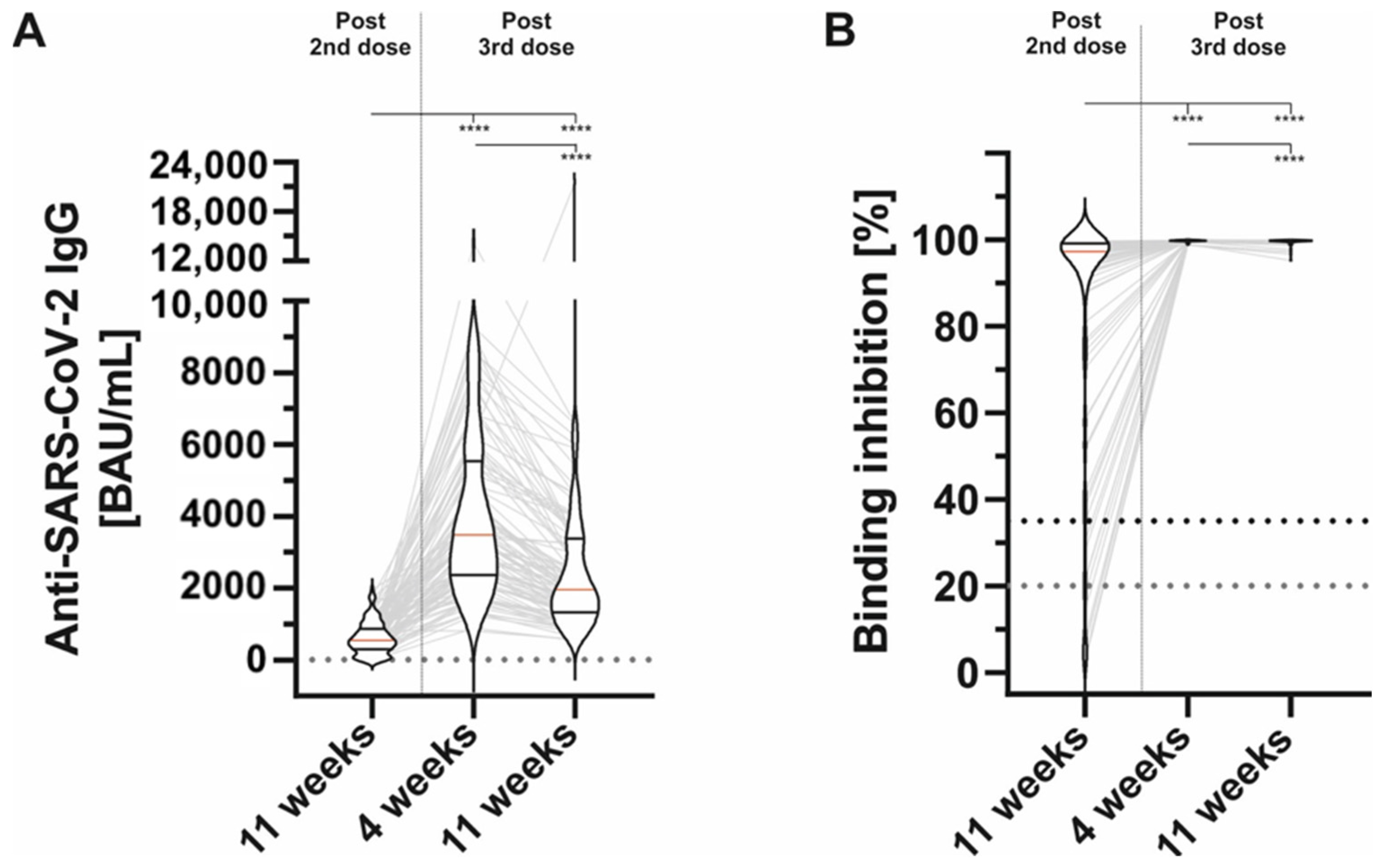
| A1:11 weeks after second dose (BAU/mL) | 611.92 ± 450.31 | 543.60 | 599.90 |
| B1: 4 weeks after third dose (BAU/mL) | 4155.59 ± 2373.65 | 3482.70 | 3200.80 |
| C1: 11 weeks after third dose (BAU/mL) | 2389.10 ± 1433.90 | 1949.90 | 1921.40 |
| Difference C1-A1 | 1777.18 ± 1470.51 | 1466.80 | 2075.00 |
| Difference C1-B1 | −1766.49 ± 1329.81 | −1574.60 | 1440.05 |
| Binding inhibition | |||
| A2: 11 weeks after second dose (%) | 83.26 ± 27.79 | 97.23 | 14.80 |
| B2: 4 weeks after third dose (%) | 99.73 ± 0.18 | 99.76 | 0.10 |
| C2: 11 weeks after third dose (%) | 99.51 ± 0.64 | 99.69 | 0.23 |
| Difference C2-A2 | 16.25 ± 27.61 | 2.29 | 14.95 |
| Difference C2-B2 | −0.22 ± 0.51 | −0.10 | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herzberg, J.; Fischer, B.; Becher, H.; Becker, A.-K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Short-Term Drop in Antibody Titer after the Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Adults. Vaccines 2022, 10, 805. https://doi.org/10.3390/vaccines10050805
Herzberg J, Fischer B, Becher H, Becker A-K, Honarpisheh H, Guraya SY, Strate T, Knabbe C. Short-Term Drop in Antibody Titer after the Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Adults. Vaccines. 2022; 10(5):805. https://doi.org/10.3390/vaccines10050805
Chicago/Turabian StyleHerzberg, Jonas, Bastian Fischer, Heiko Becher, Ann-Kristin Becker, Human Honarpisheh, Salman Yousuf Guraya, Tim Strate, and Cornelius Knabbe. 2022. "Short-Term Drop in Antibody Titer after the Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Adults" Vaccines 10, no. 5: 805. https://doi.org/10.3390/vaccines10050805
APA StyleHerzberg, J., Fischer, B., Becher, H., Becker, A. -K., Honarpisheh, H., Guraya, S. Y., Strate, T., & Knabbe, C. (2022). Short-Term Drop in Antibody Titer after the Third Dose of SARS-CoV-2 BNT162b2 Vaccine in Adults. Vaccines, 10(5), 805. https://doi.org/10.3390/vaccines10050805