
Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
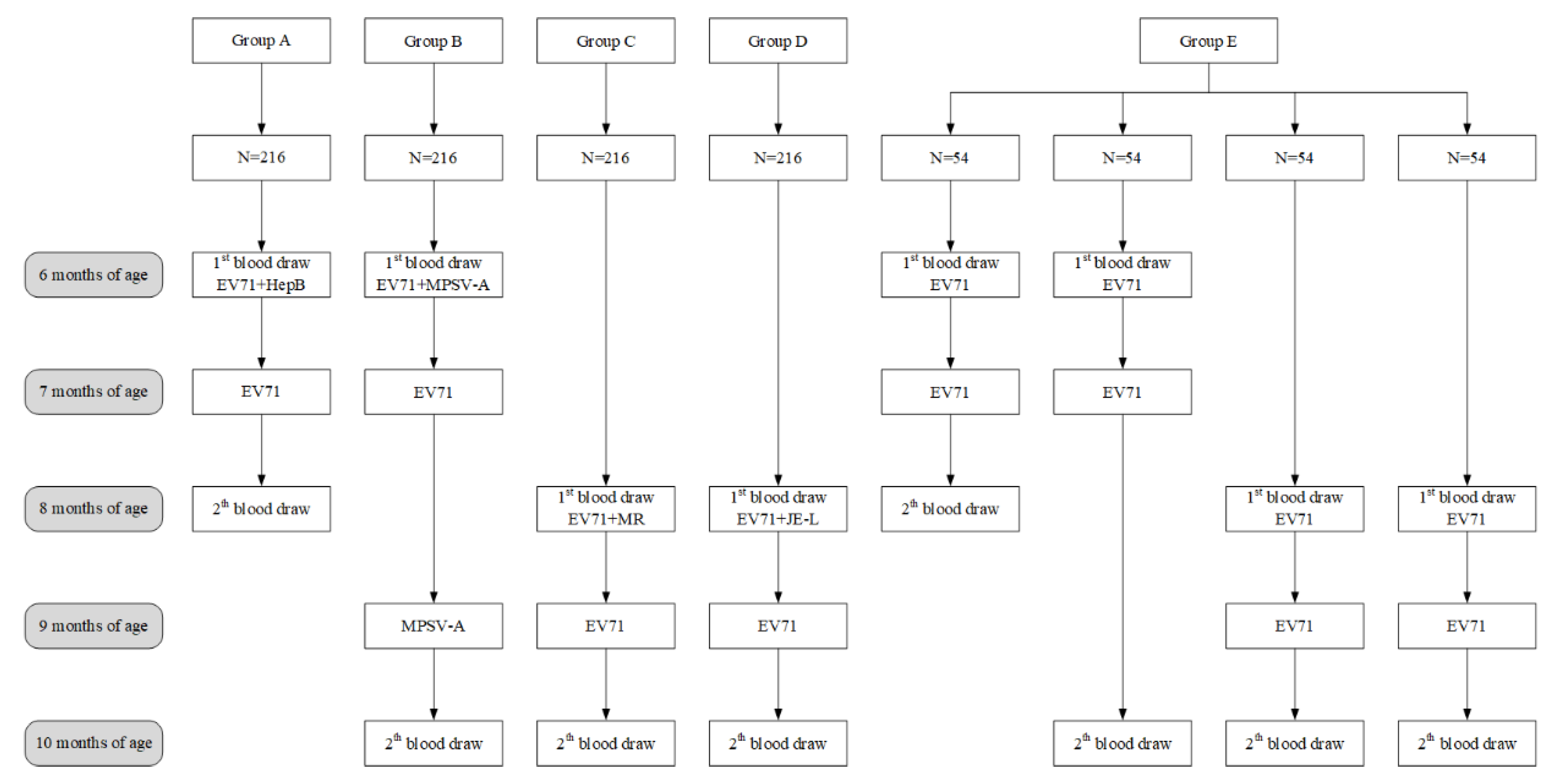
2.1. Study Design
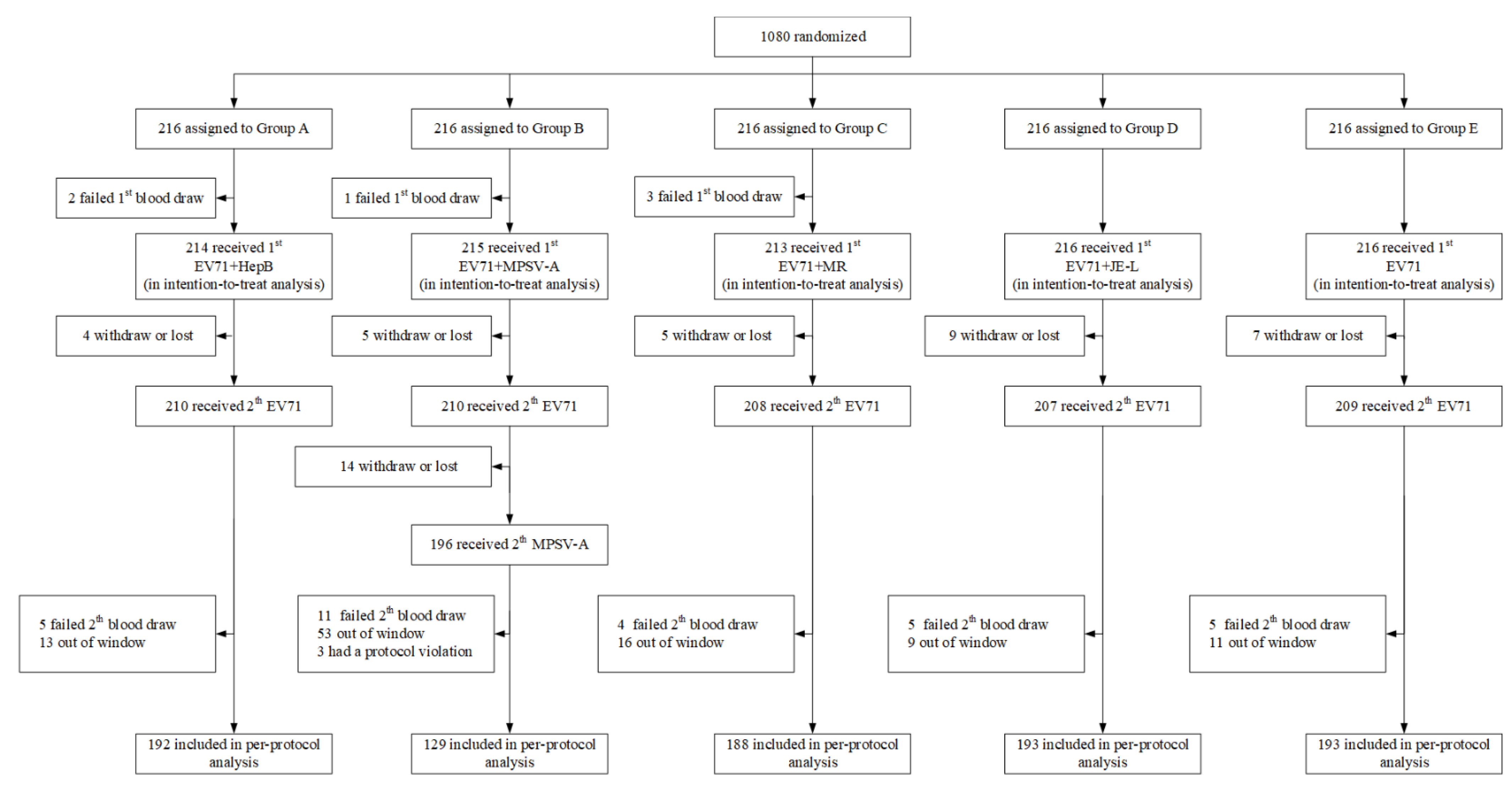
2.2. Participants
2.3. Vaccine
2.4. Randomization and Masking
2.5. Procedures
2.6. Outcomes
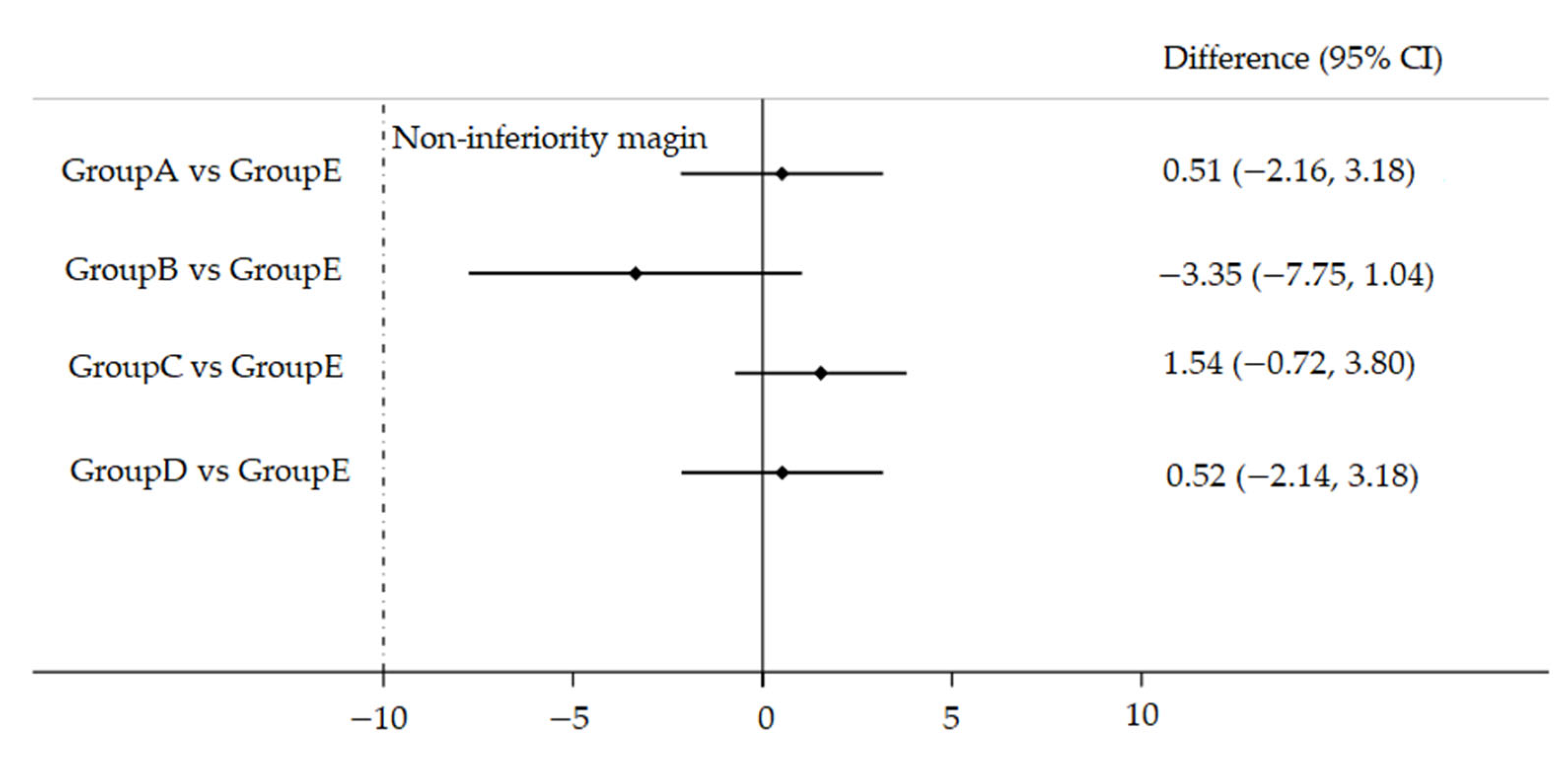
2.7. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, C.R.; Doane, F.W.; Rhodes, A.J. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; Isolation of group A Coxsackie virus. Can. Med. Assoc. J. 1958, 79, 615–621. [Google Scholar] [PubMed]
- Hagiwara, A.; Tagaya, I.; Yoneyama, T. Epidemic of hand, foot and mouth disease associated with enterovirus 71 infection. Intervirology 1978, 9, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Liu, C.C.; Chang, Y.C.; Chen, C.Y.; Wang, S.T.; Yeh, T.F. Neurologic complications in children with enterovirus 71 infection. N. Engl. J. Med. 1999, 341, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Liu, C.C.; Tseng, H.W.; Wang, J.R.; Huang, C.C.; Chen, Y.J.; Yang, Y.J.; Lin, S.J.; Yeh, T.F. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurological complications. Clin. Infect. Dis. 1999, 29, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Ren, L.; Xiong, Z.; Li, J.; Xiao, Y.; Zhao, R.; He, Y.; Bu, G.; Zhou, S.; Wang, J.; et al. Enterovirus 71 outbreak in the People’s Republic of China in 2008. J. Clin. Microbiol. 2009, 47, 2351–2352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Yeo, A.; Phoon, M.C.; Tan, E.L.; Poh, C.L.; Quak, S.H.; Chow, V.T. The largest outbreak of hand; foot and mouth disease in Singapore in 2008: The role of enterovirus 71 and coxsackievirus A strains. Int. J. Infect. Dis. 2010, 14, e1076–e1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuang, Z.C.; Kou, Z.Q.; Bai, Y.J.; Cong, X.; Wang, L.H.; Li, C.; Zhao, L.; Yu, X.J.; Wang, Z.Y.; Wen, H.L. Epidemiological Research on Hand, Foot, and Mouth Disease in Mainland China. Viruses 2015, 7, 6400–6411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.Y.; Wateska, A.R.; Bailey, R.R.; Tai, J.H.; Bacon, K.M.; Smith, K.J. Forecasting the economic value of an Enterovirus 71 (EV71) vaccine. Vaccine 2010, 28, 7731–7736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, F.C.; Meng, F.Y.; Li, J.X.; Li, X.L.; Mao, Q.Y.; Tao, H.; Zhang, Y.T.; Yao, X.; Chu, K.; Chen, Q.H.; et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2013, 381, 2024–2032. [Google Scholar] [CrossRef]
- Zhu, F.; Xu, W.; Xia, J.; Liang, Z.; Liu, Y.; Zhang, X.; Tan, X.; Wang, L.; Mao, Q.; Wu, J.; et al. Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China. N. Engl. J. Med. 2014, 370, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Meng, F.; Wang, S.; Li, J.; Zhang, Y.; Mao, Q.; Hu, Y.; Liu, P.; Shi, N.; Tao, H.; et al. 2-Year Efficacy, Immunogenicity, and Safety of Vigoo Enterovirus 71 Vaccine in Healthy Chinese Children: A Randomized Open-Label Study. J. Infect. Dis. 2017, 215, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zeng, G.; Chu, K.; Zhang, J.; Han, W.; Zhang, Y.; Li, J.; Zhu, F. Five-year immunity persistence following immunization with inactivated enterovirus 71 type (EV71) vaccine in healthy children: A further observation. Hum. Vaccines Immunother. 2018, 14, 1517–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, X.; Che, Y.; Wei, S.; Li, S.; Zhao, Z.; Tong, Y.; Wang, L.; Gong, W.; Zhang, Y.; Zhao, Y.; et al. Effectiveness and safety of an inactivated enterovirus 71 vaccine in children aged 6–71 months in a phase IV study. Clin. Infect. Dis. 2019, 71, 2421–2427. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.P.; Liang, Z.L.; Xia, J.L.; Wu, J.Y.; Wang, L.; Song, L.F.; Mao, Q.Y.; Wen, S.Q.; Huang, R.G.; Hu, Y.S.; et al. Immunogenicity, safety, and immune persistence of a novel inactivated human enterovirus 71 vaccine: A phase II, Randomized, double-blind, placebo-controlled Trial. J. Infect. Dis. 2014, 209, 46–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Head, J.R.; Collender, P.A.; Lewnard, J.A.; Skaff, N.K.; Li, L.; Cheng, Q.; Baker, J.M.; Li, C.; Chen, D.; Ohringer, A.; et al. Early evidence of inactivated enterovirus 71 vaccine impact against hand, foot, and mouth disease in a major center of ongoing transmission in China, 2011-2018: A longitudinal surveillance study. Clin. Infect. Dis. 2019, 71, 3088–3095. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.C.; Liang, Z.L.; Li, X.L.; Ge, H.M.; Meng, F.Y.; Mao, Q.Y.; Zhang, Y.T.; Hu, Y.M.; Zhang, Z.Y.; Li, J.X.; et al. Immunogenicity and safety of an enterovirus 71 vaccine in healthy Chinese children and infants: A randomised, double-blind, placebo-controlled phase 2 clinical trial. Lancet 2013, 381, 1037–1045. [Google Scholar] [CrossRef]
- Zhang, Z.; Liang, Z.; Zeng, J.; Zhang, J.; He, P.; Su, J.; Zeng, Y.; Fan, R.; Zhao, D.; Ma, W.; et al. Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously With Hepatitis B Vaccine and Group A Meningococcal Polysaccharide Vaccine: A Phase 4, Open-Label, Single-Center, Randomized, Noninferiority Trial. J. Infect. Dis. 2019, 220, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Cao, Q.; Yang, W.; Liu, X.; Liu, H.; Tian, X.; Li, J.; Fang, X.; Jia, N.; Zeng, G.; et al. Interchangeability of two Enterovirus 71 inactivated vaccines in Chinese children: A phase IV, open-label, and randomized controlled trial. Vaccine 2020, 38, 2671–2677. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Wu, P.; Wu, J.T.; Lau, E.H.; Leung, G.M.; Yu, H.; Cowling, B.J. Seroprevalence of Enterovirus 71 Antibody Among Children in China: A Systematic Review and Meta-analysis. Pediatric Infect. Dis. J. 2015, 34, 1399–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | Group C | Group D | Group E | |
|---|---|---|---|---|---|
| Total Populations | |||||
| No. of participant | 216 | 216 | 216 | 216 | 216 |
| Age, mean ± SD (months) | 6.52 ± 0.02 | 6.54 ± 0.02 | 8.56 ± 0.02 | 8.57 ± 0.02 | 7.55 ± 0.07 |
| Male sex, n (%) | 103 (47.69) | 103 (47.69) | 115 (53.24) | 104 (48.15) | 110 (50.93) |
| Per-Protocol Populations | |||||
| No. of participant | 192 | 129 | 188 | 193 | 193 |
| Age, mean ± SD (months) | 6.53 ± 0.02 | 6.57 ± 0.03 | 8.56 ± 0.02 | 8.56 ± 0.02 | 7.56 ± 0.08 |
| Male sex, n (%) | 93 (48.44) | 59 (45.74) | 96 (51.06) | 89 (46.11) | 100 (51.81) |
| Group A (n = 192) | Group B (n = 129) | Group C (n = 188) | Group D (n = 193) | Group E (n = 193) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Five Group | Group A vs. E * | Group B vs. E * | Group C vs. E * | Group D vs. E * | ||||||
| Pre-Vaccination | ||||||||||
| SPR, n (%) | 38 (19.79) | 24 (18.60) | 11 (5.85) | 16 (8.29) | 26 (13.47) | 0.000 | 0.096 | 0.213 | 0.012 | 0.102 |
| (95% CI) | (14.73–26.06) | (12.77–26.31) | (3.26–10.28) | (5.13–13.13) | (9.32–19.08) | |||||
| GMT | 5.06 | 5.17 | 4.30 | 4.61 | 4.85 | 0.052 | ||||
| (95% CI) | (4.55–5.62) | (4.61–5.79) | (4.10–4.51) | (4.16–5.11) | (4.43–5.30) | |||||
| Post-Vaccination | ||||||||||
| SPR, n (%) | 191 (99.48) | 124 (96.12) | 187 (99.47) | 192 (99.48) | 189 (97.93) | 0.055 | ||||
| (95% CI) | (97.13–99.99) | (91.19–98.73) | (97.07–99.99) | (97.15–99.99) | (94.78–99.43) | |||||
| SCR, n (%) | 189 (98.44) | 122 (94.57) | 187 (99.47) | 190 (98.45) | 189 (97.93) | 0.068 | ||||
| (95% CI) | (95.50–99.68) | (89.14–97.79) | (97.07–99.99) | (95.52–99.68) | (94.78–99.43) | |||||
| GMT | 792.51 | 287.93 | 680.91 | 677.13 | 562.47 | 0.000 | 0.007 | 0.000 | 0.134 | 0.166 |
| (95% CI) | (671.95–934.69) | (228.66–362.56) | (576.44–804.30) | (562.35–815.35) | (466.59–678.05) | |||||
| Group E1 (n = 51) | Group E2 (n = 45) | Group E3 (n = 48) | Group E4 (n = 49) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Four Group | Group E1 vs. E2 * | Group E3 vs. E2 * | Group E4 vs. E2 * | |||||
| Post-vaccination | ||||||||
| SPR, n (%) | 51 (100.00) | 43 (95.56) | 47 (97.92) | 48 (97.96) | 0.507 | |||
| (95% CI) | (93.02–100.00) | (84.85–99.46) | (88.93–99.95) | (89.15–99.95) | ||||
| SCR, n (%) | 51 (100.00) | 43 (95.56) | 47 (97.92) | 48 (97.96) | 0.507 | |||
| (95% CI) | (93.02–100.00) | (84.85–99.46) | (88.93–99.95) | (89.15–99.95) | ||||
| GMT | 1004.00 | 341.06 | 553.35 | 495.08 | 0.001 | 0.000 | 0.087 | 0.177 |
| (95% CI) | (738.13–1365.65) | 225.06–516.85) | (377.46–811.22) | (343.39–713.77) | ||||
| Event | Group A (n = 215) n, (%) | Group B (n = 216) n, (%) | Group C (n = 213) n, (%) | Group D (n = 215) n, (%) | Group E (n = 216) n, (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Five Group | Group A vs. E * | Group B vs. E * | Group C vs. E * | Group D vs. E * | ||||||
| Total adverse events | 76 (35.35) | 83 (38.43) | 89 (41.78) | 104 (48.37) | 82 (37.96) | 0.061 | ||||
| Solicited adverse events | 55 (25.58) | 64 (29.63) | 70 (32.86) | 87 (40.47) | 70 (32.41) | 0.019 | 0.118 | 0.533 | 0.920 | 0.082 |
| Local adverse events | 14 (6.51) | 9 (4.17) | 2 (0.94) | 11 (5.12) | 12 (5.56) | 0.057 | ||||
| Redness | 8 (3.72) | 6 (2.78) | 1 (0.47) | 7 (3.26) | 10 (4.63) | 0.127 | ||||
| Induration | 8 (3.72) | 6 (2.78) | 1 (0.47) | 5 (2.33) | 5 (2.31) | 0.261 | ||||
| Swelling | 3 (1.40) | 0 (0) | 0 (0) | 1 (0.47) | 0 (0) | 0.074 | ||||
| Systemic adverse events | 45 (20.93) | 58 (26.85) | 69 (32.39) | 78 (36.28) | 62 (28.70) | 0.007 | 0.062 | 0.667 | 0.407 | 0.093 |
| Fever | 37 (17.21) | 44 (20.37) | 58 (27.23) | 69 (32.09) | 53 (24.54) | 0.003 | 0.061 | 0.299 | 0.524 | 0.082 |
| Diarrhea | 5 (2.33) | 6 (2.78) | 5 (2.5) | 6 (2.79) | 6 (2.78) | 0.995 | ||||
| Vomiting | 1 (0.47) | 1 (0.46) | 0 (0) | 0 (0) | 1 (0.46) | 0.738 | ||||
| Irritability | 0 (0) | 1(0.46) | 1(0.47) | 1 (0.47) | 0 (0) | 0.733 | ||||
| Anorexia | 1 (0.47) | 0 (0) | 2 (0.94) | 1 (0.47) | 0 (0) | 0.469 | ||||
| Allergy | 0 (0) | 0 (0) | 1 (0.47) | 1 (0.47) | 1 (0.46) | 0.733 | ||||
| Unsolicited adverse events | 35 (16.28) | 34 (15.74) | 38 (17.84) | 49 (22.79) | 28 (12.96) | 0.092 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Chang, S.; Wang, R.; Xiao, Y.; Li, F.; Xu, Q.; Zhang, S.; Chen, X.; Zhang, S.; Zhang, M.; et al. Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China. Vaccines 2022, 10, 895. https://doi.org/10.3390/vaccines10060895
Liu X, Chang S, Wang R, Xiao Y, Li F, Xu Q, Zhang S, Chen X, Zhang S, Zhang M, et al. Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China. Vaccines. 2022; 10(6):895. https://doi.org/10.3390/vaccines10060895
Chicago/Turabian StyleLiu, Xiaodong, Shaoying Chang, Ruize Wang, Yanhui Xiao, Fangjun Li, Qing Xu, Shaobai Zhang, Xiao Chen, Shangxiao Zhang, Min Zhang, and et al. 2022. "Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China" Vaccines 10, no. 6: 895. https://doi.org/10.3390/vaccines10060895
APA StyleLiu, X., Chang, S., Wang, R., Xiao, Y., Li, F., Xu, Q., Zhang, S., Chen, X., Zhang, S., Zhang, M., Chen, X., Cao, Q., Liu, X., Wang, H., Zhan, D., Chen, H., Chen, W., Jiang, J., Zhang, C., ... Xu, A. (2022). Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China. Vaccines, 10(6), 895. https://doi.org/10.3390/vaccines10060895