
Neutralizing Antibody Response, Safety, and Efficacy of mRNA COVID-19 Vaccines in Pediatric Patients with Inflammatory Bowel Disease: A Prospective Multicenter Case—Control Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Neutralizing Antibody Response Assessment
2.3. Assessment of Safety and Breakthrough Infection
2.4. Statistical Analysis
3. Results
3.1. Study Population
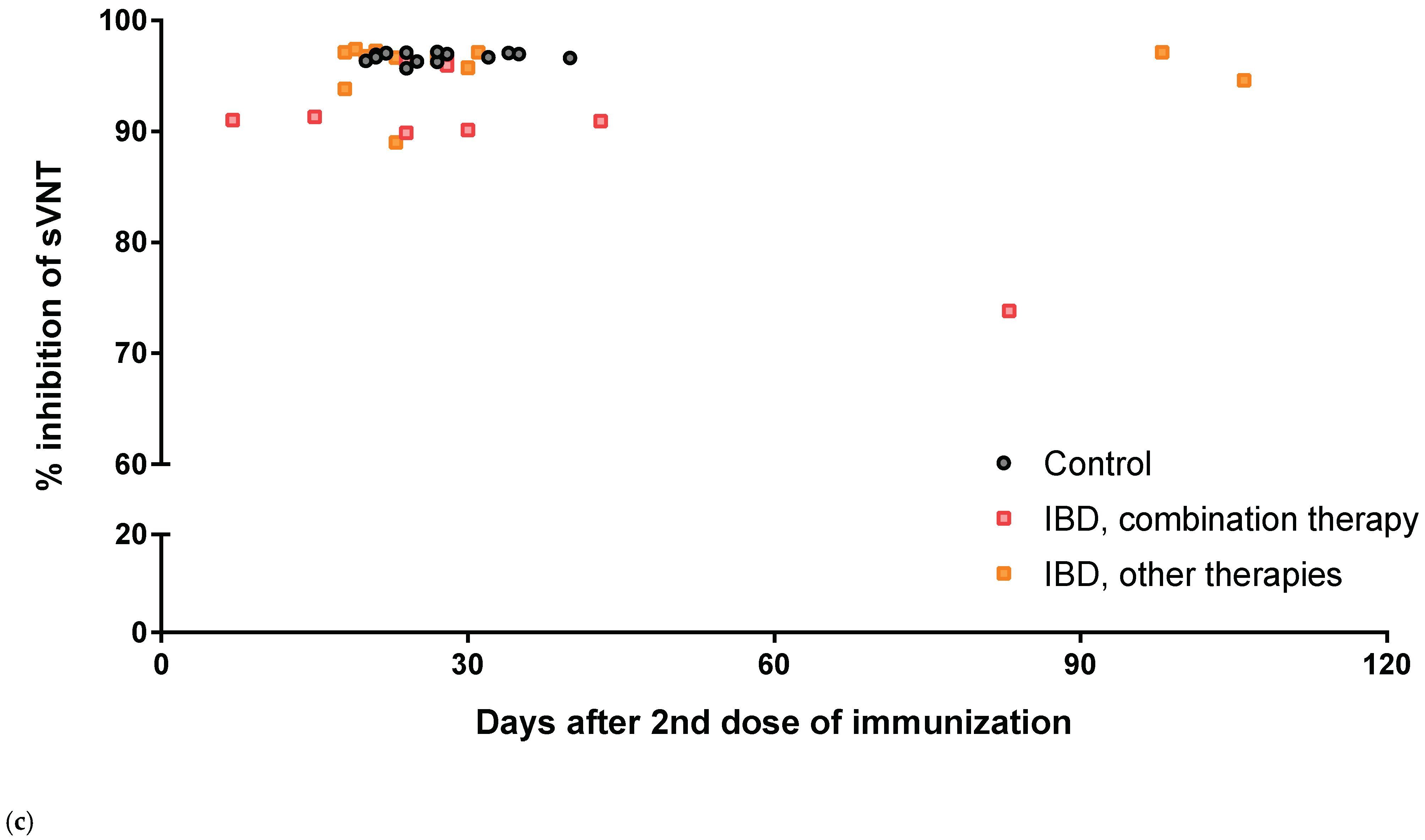
3.2. sVNT Inhibition Levels of Anti-SARS-CoV-2 Antibody Level after Two Doses of BNT162b2
3.3. Safety Profiles
3.4. Efficacy and Breakthrough Infection during the Omicron Variant Outbreak
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- JCVI Statement on Vaccination of Children Aged 5 to 11 Years Old. GOV.UK. Available online: https://www.gov.uk/government/publications/jcvi-update-on-advice-for-covid-19-vaccination-of-children-aged-5-to-11/jcvi-statement-on-vaccination-of-children-aged-5-to-11-years-old (accessed on 2 August 2022).
- Committee on Infectious Diseases. COVID-19 vaccines in children and adolescents. Pediatrics 2021, 149, e2021054332. [Google Scholar]
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/publications-data/interim-public-health-considerations-covid-19-vaccination-children-aged-5-11 (accessed on 8 July 2022).
- Kim, B.J.; Song, S.M.; Kim, K.M.; Lee, Y.J.; Rhee, K.W.; Jang, J.Y.; Park, S.J.; Yoon, C.H. Characteristics and trends in the incidence of inflammatory bowel disease in Korean children: A single-center experience. Dig. Dis. Sci. 2010, 55, 1989–1995. [Google Scholar] [CrossRef]
- Ng, W.K.; Wong, S.H.; Ng, S.C. Changing epidemiological trends of inflammatory bowel disease in Asia. Intest. Res. 2016, 14, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory bowel disease in children and adolescents. JAMA Pediatr. 2015, 169, 1053–1060. [Google Scholar] [CrossRef] [Green Version]
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; de Carpi, J.M.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of paediatric ulcerative colitis, Part 1: Ambulatory care-an evidence-based guideline from European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, hepatology and nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 257–291. [Google Scholar] [CrossRef]
- Van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The medical management of paediatric Crohn’s disease: An ECCO-ESPGHAN guideline update. J. Crohn’s Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef] [PubMed]
- Beaugerie, L.; Kirchgesner, J. Balancing benefit vs. risk of immunosuppressive therapy for individual patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2019, 7, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Bononi, I.; Puozzo, A.; Govoni, M.; Foschi, V.; Lanza, G.; Gafà, R.; Gaboriaud, P.; Touzé, F.A.; Selvatici, R.; et al. Merkel cell carcinomas arising in autoimmune disease affected patients treated with biologic drugs, including anti-TNF. Clin. Cancer Res. 2017, 23, 3929–3934. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.L.; Moran, G.W.; Gaya, D.R.; Raine, T.; Hart, A.; Kennedy, N.A.; Lindsay, J.O.; MacDonald, J.; Segal, J.P.; Sebastian, S.; et al. SARS-CoV-2 vaccination for patients with inflammatory bowel disease: A British Society of Gastroenterology inflammatory bowel Disease section and IBD Clinical Research Group position statement. Lancet Gastroenterol. Hepatol. 2021, 6, 218–224. [Google Scholar] [CrossRef]
- Doherty, J.; Fennessy, S.; Stack, R.; O’Morain, N.; Cullen, G.; Ryan, E.J.; De Gascun, C.; Doherty, G.A. Review Article: Vaccination for patients with inflammatory bowel disease during the COVID-19 pandemic. Aliment. Pharmacol. Ther. 2021, 54, 1110–1123. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based COVID-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Hadi, Y.B.; Thakkar, S.; Shah-Khan, S.M.; Hutson, W.; Sarwari, A.; Singh, S. COVID-19 vaccination is safe and effective in patients with inflammatory bowel disease: Analysis of a Large Multi-institutional Research Network in The United States. Gastroenterology 2021, 161, 1336–1339.e3. [Google Scholar] [CrossRef]
- Widdifield, J.; Kwong, J.C.; Chen, S.; Eder, L.; Benchimol, E.I.; Kaplan, G.G.; Hitchon, C.; Aviña-Zubieta, J.A.; Lacaille, D.; Chung, H.; et al. Vaccine effectiveness against SARS-CoV-2 infection and severe outcomes among individuals with immune-mediated inflammatory diseases tested between March 1 and Nov 22, 2021, in Ontario, Canada: A population-based analysis. Lancet Rheumatol. 2022, 4, e430–e440. [Google Scholar] [CrossRef]
- Ben-Tov, A.; Banon, T.; Chodick, G.; Kariv, R.; Assa, A.; Gazit, S.; Collaborators of the Maccabi Institute for Research & Innovation COVID-19 Task Force. BNT162b2 messenger RNA COVID-19 vaccine effectiveness in patients with inflammatory bowel disease: Preliminary real-world data during mass vaccination campaign. Gastroenterology 2021, 161, 1715–1717.e1. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.A.; Lin, S.; Goodhand, J.R.; Chanchlani, N.; Hamilton, B.; Bewshea, C.; Nice, R.; Chee, D.; Cummings, J.F.; Fraser, A.; et al. Infliximab is associated with attenuated immunogenicity to BNT162b2 and ChAdOx1 nCoV-19 SARS-CoV-2 vaccines in patients with IBD. Gut 2021, 70, 1884–1893. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news/item/26-11-2021-classification-of-Omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 8 July 2022).
- Turner, D.; Otley, A.R.; Mack, D.; Hyams, J.; de Bruijne, J.; Uusoue, K.; Walters, T.D.; Zachos, M.; Mamula, P.; Beaton, D.E.; et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: A prospective multicenter study. Gastroenterology 2007, 133, 423–432. [Google Scholar] [CrossRef]
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef]
- Hyams, J.; Markowitz, J.; Otley, A.; Rosh, J.; Mack, D.; Bousvaros, A.; Kugathasan, S.; Pfefferkorn, M.; Tolia, V.; Evans, J.; et al. Evaluation of the pediatric Crohn disease activity index: A prospective multicenter experience. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 416–421. [Google Scholar] [CrossRef] [PubMed]
- von Rhein, C.; Scholz, T.; Henss, L.; Kronstein-Wiedemann, R.; Schwarz, T.; Rodionov, R.N.; Corman, V.M.; Tonn, T.; Schnierle, B.S. Comparison of potency assays to assess SARS-CoV-2 neutralizing antibody capacity in COVID-19 convalescent plasma. J. Virol. Methods 2021, 288, 114031. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.; Tiu, C.; Hu, Z.; Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/toxicity-grading-scale-healthy-adult-and-adolescent-volunteers-enrolled-preventive-vaccine-clinical (accessed on 2 August 2022).
- Calabuig, J.M.; García-Raffi, L.M.; García-Valiente, A.; Sánchez-Pérez, E.A. Kaplan-Meier type survival curves for COVID-19: A health data based decision-making tool. Front. Public Health 2021, 9, 646863. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; Schiavetti, I.; Inglese, M.; Carmisciano, L.; Laroni, A.; Lapucci, C.; Visconti, V.; Serrati, C.; Gandoglia, I.; Tassinari, T.; et al. Breakthrough SARS-CoV-2 infections after COVID-19 mRNA vaccination in MS patients on disease modifying therapies during the Delta and the Omicron waves in Italy. EBioMedicine 2022, 80, 104042. [Google Scholar] [CrossRef]
- Abu Jabal, K.; Ben-Amram, H.; Beiruti, K.; Batheesh, Y.; Sussan, C.; Zarka, S.; Edelstein, M. Impact of age, ethnicity, sex and prior infection status on immunogenicity following a single dose of the BNT162b2 mRNA COVID-19 vaccine: Real-world evidence from healthcare workers, Israel, December 2020 to January 2021. EuroSurveill. 2021, 26, 2100096. [Google Scholar] [CrossRef]
- Falahi, S.; Kenarkoohi, A. Hosts. Host factors and vaccine efficacy: Implications for COVID-19 vaccines. J. Med. Virol. 2022, 94, 1330–1335. [Google Scholar] [CrossRef]
- Gicchino, M.F.; Abbate, F.G.; Amodio, A.; Miraglia del Giudice, E.; Olivieri, A.N. Preliminary observations on the immunogenicity and safety of vaccines to prevent COVID-19 in patients with juvenile idiopathic arthritis. Acta Paediatr. 2022, 00, 1–3. [Google Scholar] [CrossRef]
- Papp, K.A.; Haraoui, B.; Kumar, D.; Marshall, J.K.; Bissonnette, R.; Bitton, A.; Bressler, B.; Gooderham, M.; Ho, V.; Jamal, S.; et al. Vaccination guidelines for patients with immune-mediated disorders on immunosuppressive therapies. J. Cutan. Med. Surg. 2019, 23, 50–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, P.; Santos-Antunes, J.; Rodrigues, S.; Lopes, S.; Macedo, G. Treatment with infliximab or azathioprine negatively impact the efficacy of hepatitis B vaccine in inflammatory bowel disease patients. J. Gastroenterol. Hepatol. 2015, 30, 1591–1595. [Google Scholar] [CrossRef]
- Hagihara, Y.; Ohfuji, S.; Watanabe, K.; Yamagami, H.; Fukushima, W.; Maeda, K.; Kamata, N.; Sogawa, M.; Shiba, M.; Tanigawa, T.; et al. Infliximab and/or immunomodulators inhibit immune responses to trivalent influenza vaccination in adults with inflammatory bowel disease. J. Crohn’s Colitis 2014, 8, 223–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorino, G.; Peyrin-Biroulet, L.; Naccarato, P.; Szabò, H.; Sociale, O.R.; Vetrano, S.; Fries, W.; Montanelli, A.; Repici, A.; Malesci, A.; et al. Effects of immunosuppression on immune response to pneumococcal vaccine in inflammatory bowel disease: A prospective study. Inflam. Bowel Dis. 2012, 18, 1042–1047. [Google Scholar] [CrossRef]
- Alexander, J.L.; Kennedy, N.A.; Ibraheim, H.; Anandabaskaran, S.; Saifuddin, A.; Castro Seoane, R.; Liu, Z.; Nice, R.; Bewshea, C.; D’Mello, A.; et al. COVID-19 vaccine-induced antibody responses in immunosuppressed patients with inflammatory bowel disease (VIP): A multicentre, prospective, case-control study. Lancet Gastroenterol. Hepatol. 2022, 7, 342–352. [Google Scholar] [CrossRef]
- Dailey, J.; Kozhaya, L.; Dogan, M.; Hopkins, D.; Lapin, B.; Herbst, K.; Brimacombe, M.; Grandonico, K.; Karabacak, F.; Schreiber, J.; et al. Antibody responses to SARS-CoV-2 after infection or vaccination in children and young adults with inflammatory bowel disease. Inflam. Bowel Dis. 2022, 28, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Shehab, M.; Alrashed, F.; Alfadhli, A.; Alotaibi, K.; Alsahli, A.; Mohammad, H.; Cherian, P.; Al-Khairi, I.; Alphonse Thanaraj, T.; Channanath, A.; et al. Serological response to BNT162b2 and ChAdOx1 nCoV-19 vaccines in patients with inflammatory bowel disease on biologic therapies. Vaccines 2021, 9, 1471. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.A.; Goodhand, J.R.; Bewshea, C.; Nice, R.; Chee, D.; Lin, S.; Chanchlani, N.; Butterworth, J.; Cooney, R.; Croft, N.M.; et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut 2021, 70, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Lev-Tzion, R.; Focht, G.; Lujan, R.; Mendelovici, A.; Friss, C.; Greenfeld, S.; Kariv, R.; Ben-Tov, A.; Matz, E.; Nevo, D.; et al. COVID-19 vaccine is effective in inflammatory bowel disease patients and is not associated with disease exacerbation. Clin. Gastroenterol. Hepatol. 2022, 20, e1263–e1282. [Google Scholar] [CrossRef]
- Khan, N.; Mahmud, N. Effectiveness of SARS-CoV-2 vaccination in a Veterans Affairs cohort of patients with inflammatory bowel disease with diverse exposure to immunosuppressive medications. Gastroenterology 2021, 161, 827–836. [Google Scholar] [CrossRef]
- Bhurwal, A.; Mutneja, H.; Bansal, V.; Goel, A.; Arora, S.; Attar, B.; Minacapelli, C.D.; Kochhar, G.; Chen, L.A.; Brant, S.; et al. Effectiveness and safety of SARS-CoV-2 vaccine in inflammatory bowel Disease patients: A systematic review, meta-analysis and meta-regression. Aliment. Pharmacol. Ther. 2022, 55, 1244–1264. [Google Scholar] [CrossRef] [PubMed]
- Ricciuto, A.; Lamb, C.A.; Benchimol, E.I.; Walker, G.J.; Kennedy, N.A.; Kuenzig, M.E.; Kaplan, G.G.; Kappelman, M.D.; Ungaro, R.C.; Colombel, J.F.; et al. Inflammatory bowel disease clinical activity is associated with COVID-19 severity especially in younger patients. J. Crohn’s Colitis 2022, 16, 591–600. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Controls (n = 15) | Patients with IBD (n = 23) |
|---|---|---|
| Age, mean ± SD (year) | 14.7 ± 1.7 | 15.2 ± 1.3 |
| Male sex, n (%) | 11 (73.3) | 16 (69.6) |
| Female, n (%) | 4 (26.7) | 7 (30.4) |
| History of COVID-19 before vaccination | 0 (0.0) | 1 (4.3) |
| Clinical characteristics of the IBD group | ||
| Duration of IBD (months), mean ± SD | 20.6 ± 15.9 | |
| CD, n (%) | 16 (69.6%) | |
| UC, n (%) | 7 (30.4%) | |
| Active disease *, CD, n (%) | 6 (37.5%) | |
| Active disease *, UC, n (%) | 2 (28.6%) | |
| Treatment, n (%) | ||
| 5-ASA monotherapy, n (%) | 1 (4.3%) | |
| Immunomodulator monotherapy, n (%) | 13 (56.5%) AZP 10/MTX 3 | |
| Anti-TNF + immunomodulator, n (%) | 9 (39.1%) AZP 7/MTX 2 | |
| Laboratory findings | ||
| Hemoglobin (g/dL), mean ± SD | 13.5 ± 1.5 | |
| Hematocrit (%), mean ± SD | 40.1 ± 3.7 | |
| ESR (mm/h), median ± IQR | 8 (3–11) | |
| Albumin (g/dL), mean ± SD | 4.7 ± 0.3 | |
| Calprotectin (ug/g), median ± IQR | 801.0 (113.7–1131.3) |
| Control | IBD | |||
|---|---|---|---|---|
| Dose 1 (n = 10) | Dose 2 (n = 10) | Dose 1 (n = 17) | Dose 2 (n = 17) | |
| Adverse events | 8 (80.0) | 8 (80.0) | 9 (52.9) | 6 (47.1) * |
| Local adverse events | ||||
| Pain on injection site | 8 (80.0) | 7 (70.0) | 8 (47.1) | 6 (47.1) |
| Swelling | 2 (20.0) | 4 (40.0) | 1 (5.9) | 2 (11.8) |
| Redness | 0 (0.0) | 2 (20.0) | 0 (0.0) | 1 (5.9) |
| Nodularity | 3 (30.0) | 3 (30.0) | 1 (5.9) | 1 (5.9) |
| Systemic adverse events | ||||
| Fever | 1 (10.0) | 6 (60.0) | 1 (5.9) | 1 (5.9) * |
| Myalgia | 2 (20.0) | 4 (40.0) | 3 (17.6) | 4 (23.5) |
| Fatigue | 4 (40.0) | 6 (60.0) | 5 (29.4) | 5 (29.4) |
| Headache | 0 (0.0) | 7 (70.0) | 2 (11.8) | 3 (17.6) * |
| Skin rash | 0 (0.0) | 1 (10.0) | 1 (5.9) | 1 (5.9) |
| Other | Cervical lymphadenopathy | Chest pain | Chest pain | Chest pain |
| Serious adverse events | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.J.; Choi, S.Y.; Lee, Y.M.; Kim, H.W. Neutralizing Antibody Response, Safety, and Efficacy of mRNA COVID-19 Vaccines in Pediatric Patients with Inflammatory Bowel Disease: A Prospective Multicenter Case—Control Study. Vaccines 2022, 10, 1265. https://doi.org/10.3390/vaccines10081265
Lee KJ, Choi SY, Lee YM, Kim HW. Neutralizing Antibody Response, Safety, and Efficacy of mRNA COVID-19 Vaccines in Pediatric Patients with Inflammatory Bowel Disease: A Prospective Multicenter Case—Control Study. Vaccines. 2022; 10(8):1265. https://doi.org/10.3390/vaccines10081265
Chicago/Turabian StyleLee, Kyung Jae, So Yoon Choi, Yoo Min Lee, and Han Wool Kim. 2022. "Neutralizing Antibody Response, Safety, and Efficacy of mRNA COVID-19 Vaccines in Pediatric Patients with Inflammatory Bowel Disease: A Prospective Multicenter Case—Control Study" Vaccines 10, no. 8: 1265. https://doi.org/10.3390/vaccines10081265
APA StyleLee, K. J., Choi, S. Y., Lee, Y. M., & Kim, H. W. (2022). Neutralizing Antibody Response, Safety, and Efficacy of mRNA COVID-19 Vaccines in Pediatric Patients with Inflammatory Bowel Disease: A Prospective Multicenter Case—Control Study. Vaccines, 10(8), 1265. https://doi.org/10.3390/vaccines10081265