

Written Briefing and Oral Counseling Increase the Willingness to Receive the SARS-CoV-2 Vaccination among Women in Puerperium: A Qualitative Prospective Cohort Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics (Table 1, Figure 1)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluation Group (n = 69) | Study Group A (n = 68) | Study Group B (n = 80) | Standardized Difference 1 | |||
|---|---|---|---|---|---|---|
| Evaluation Group vs. A | Evaluation Group vs. B | A vs. B | ||||
| Age, years (IQR) | 31.5 (28.1–36.4) | 32.6 (28.9–36.0) | 32.5 (28.8–35.7) | −0.03 | −0.02 | −0.01 |
| Migration background, n (%) | 37 (53.6%) | 40 (58.8%) | 49 (61.3%) | 0.11 | 0.15 | −0.05 |
| Primipara, n (%) | 44 (63.8%) | 30 (44.1%) | 30 (37.5%) | −0.39 | −0.49 | 0.11 |
| Mode of delivery | 0.03 | 0.03 | −0.00 | |||
| Vaginal delivery, n (%) | 36 (52.2%) | 34 (50.7%) | 41 (51.2%) | |||
| Cesarean section, n (%) | 31 (44.9%) | 31 (46.3%) | 36 (45.0%) | |||
| Instrumental delivery, n (%) | 2 (2.9%) | 2 (3.0%) | 3 (3.8%) | |||
| Preterm delivery, n (%) | 18 (26.1%) | 9 (13.2%) | 15 (18.8%) | −0.32 | −0,19 | −0.14 |
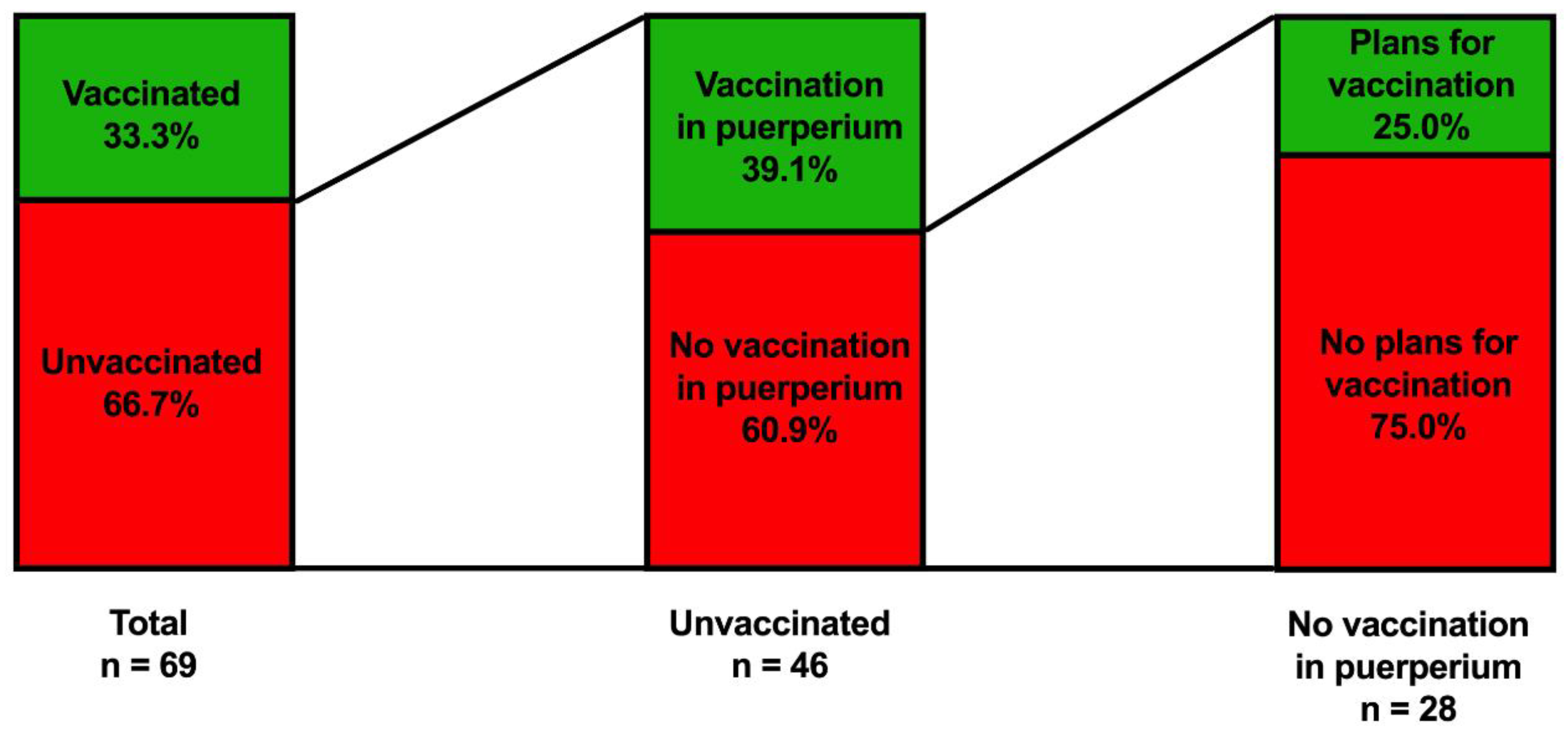
3.2. Women’s Assessment on Their SARS-CoV-2 Vaccination Status (Table 2, Figure 2)
| Yes | No | |
|---|---|---|
| Received at least one shot of the SARS-CoV-2 vaccination | 23 (33.3%) | 46 (66.7%) |
| Received two shots of the SARS-CoV-2 vaccination | 22 (31.9%) | 47 (68.1%) |
| Unvaccinated and want to receive the SARS-CoV-2 vaccination during puerperium/total number of unvaccinated women | 18/46 (39.1%) | 28/46 (60.9%) |
| Did not receive the SARS-CoV-2 vaccination, but plan to receive the vaccination/total number of unvaccinated women declining the vaccination in puerperium | 7/28 (25.0%) | 21/28 (75.0%) |
| One-time vaccinated * and want to receive a second shot after hospital dismissal/total number of one-time vaccinated women in puerperium | 14/19 (73.7%) | 5/19 (26.3%) |

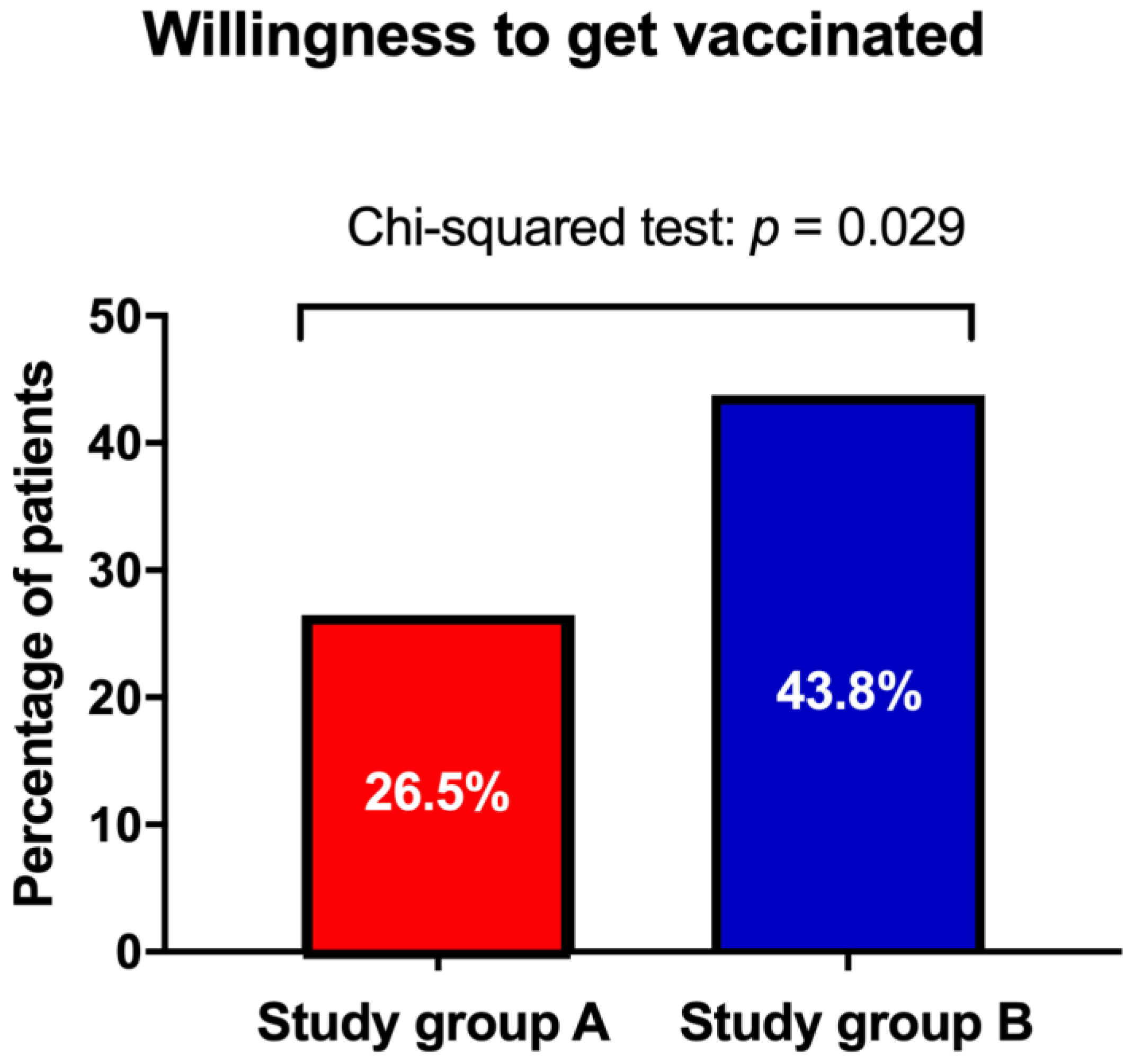
3.3. Effect of Physician’s Counseling on SARS-CoV-2 Vaccination (Figure 3)

3.4. Willingness to Receive the Vaccination in Different Age Strata of Women in Puerperium (Table 3, Figure 4)
| Age Groups(years) | Overall (n = 194) | Study Group A (n = 68) | Study Group B (n = 80) | Unvaccinated Women in the Evaluation Group (n = 46) | ||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | Yes | No | Yes | No | |
| 18–29 | 29 (40.8%) | 42 (59.2%) | 4 (17.4%) | 19 (82.6%) | 12 (44.4%) | 15 (55.6%) | 13 (61.9%) | 8 (38.1%) |
| 30–39 | 43 (39.8%) | 65 (60.2%) | 14 (34.1%) | 27 (65.9%) | 20 (43.5%) | 26 (56.5%) | 9 (42.9%) | 12 (57.1%) |
| 40–49 | 6 (40.0%) | 9 (60.0%) | 0 (0%) | 4 (100%) | 3 (42.9%) | 4 (57.1%) | 3 (75.0%) | 1 (25.0%) |

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Salyer, S.J.; Maeda, J.; Sembuche, S.; Kebede, Y.; Tshangela, A.; Moussif, M.; Ihekweazu, C.; Mayet, N.; Abate, E.; Ouma, A.O.; et al. The first and second waves of the COVID-19 pandemic in Africa: A cross-sectional study. Lancet 2021, 397, 1265–1275. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Narang, K.; Enninga, E.A.L.; Gunaratne, M.; Ibirogba, E.R.; Trad, A.T.A.; Elrefaei, A.; Theiler, R.N.; Ruano, R.; Szymanski, L.M.; Chakraborty, R.; et al. SARS-CoV-2 Infection and COVID-19 during Pregnancy: A Multidisciplinary Review. Mayo Clin. Proc. 2020, 95, 1750–1765. [Google Scholar] [CrossRef]
- Male, V. Are COVID-19 vaccines safe in pregnancy? Nat. Rev. Immunol. 2021, 21, 200–201. [Google Scholar] [CrossRef]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., 3rd; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, 22 January–3 October 2020. Mmwr. Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef]
- Male, V. SARS-CoV-2 infection and COVID-19 vaccination in pregnancy. Nat. Rev. Immunol. 2022, 22, 277–282. [Google Scholar] [CrossRef]
- Khalil, A.; Kalafat, E.; Benlioglu, C.; O′Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Heath, P.; Ladhani, S.; et al. SARS-CoV-2 infection in pregnancy: A systematic review and meta-analysis of clinical features and pregnancy outcomes. EClin. Med. 2020, 25, 100446. [Google Scholar] [CrossRef]
- Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz. Corona-Schutzimpfung: Fachinformationen. 2021. Available online: https://www.sozialministerium.at/Corona-Schutzimpfung/Corona-Schutzimpfung—Fachinformationen.html (accessed on 3 July 2022).
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Pollard, A.J. ChAdOx1 nCoV-19 vaccine: Asymptomatic efficacy estimates—Authors′ reply. Lancet 2021, 397, 2248. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]
- Goldshtein, I.; Nevo, D.; Steinberg, D.M.; Rotem, R.S.; Gorfine, M.; Chodick, G.; Segal, Y. Association between BNT162b2 Vaccination and Incidence of SARS-CoV-2 Infection in Pregnant Women. JAMA 2021, 326, 728–735. [Google Scholar] [CrossRef]
- Kachikis, A.; Englund, J.A.; Singleton, M.; Covelli, I.; Drake, A.L.; Eckert, L.O. Short-term Reactions among Pregnant and Lactating Individuals in the First Wave of the COVID-19 Vaccine Rollout. JAMA Netw. Open 2021, 4, e2121310. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Gorman, J.R.; Chambers, C.D. Pregnant women′s attitudes toward influenza vaccination while breastfeeding. Prev. Med. Rep. 2015, 2, 333–336. [Google Scholar] [CrossRef] [Green Version]
- Stuckelberger, S.; Favre, G.; Ceulemans, M.; Nordeng, H.; Gerbier, E.; Lambelet, V.; Stojanov, M.; Winterfeld, U.; Baud, D.; Panchaud, A.; et al. SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses 2021, 13, 1199. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, S.L.; Weiss, T.W.; Zimet, G.D.; Ma, L.; Good, M.B.; Vichnin, M.D. Predictors of HPV vaccine uptake among women aged 19–26: Importance of a physician′s recommendation. Vaccine 2011, 29, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Biringer, A.; Ofner-Agostini, M.; Upshur, R.; McGeer, A. A cross-sectional study of maternity care providers′ and women′s knowledge, attitudes, and behaviours towards influenza vaccination during pregnancy. J. Obs. Gynaecol. Can. 2008, 30, 404–410. [Google Scholar] [CrossRef]
- Pateisky, P.K.H. Stellungnahme der OEGGG Zum Thema COVID-19 Impfung für Frauen Mit Kinderwunsch, Schwangere und Stillende Frauen; Österreichische Ges. Für Gynäkologie und Geburtshilfe: Vienna, Austria, 2021. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Publishers: Hillsdale, NY, USA, 1988. [Google Scholar]
- Stamm, T.A.; Partheymüller, J.; Mosor, E.; Ritschl, V.; Kritzinger, S.; Eberl, J.M. Coronavirus vaccine hesitancy among unvaccinated Austrians: Assessing underlying motivations and the effectiveness of interventions based on a cross-sectional survey with two embedded conjoint experiments. Lancet Reg. Health Eur. 2022, 17, 100389. [Google Scholar] [CrossRef]
- Oluklu, D.; Goncu Ayhan, S.; Menekse Beser, D.; Uyan Hendem, D.; Ozden Tokalioglu, E.; Turgut, E.; Sahin, D. Factors affecting the acceptability of COVID-19 vaccine in the postpartum period. Hum. Vaccin Immunother 2021, 17, 4043–4047. [Google Scholar] [CrossRef]
- Goncu Ayhan, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynaecol. Obstet. Off. Organ. Int. Fed. Gynaecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef]
- Adhikari, E.H.; Spong, C.Y. COVID-19 Vaccination in Pregnant and Lactating Women. JAMA 2021, 325, 1039–1040. [Google Scholar] [CrossRef]
- Taylor, M.M.; Kobeissi, L.; Kim, C.; Amin, A.; Thorson, A.E.; Bellare, N.B.; Brizuela, V.; Bonet, M.; Kara, E.; Thwin, S.S.; et al. Inclusion of pregnant women in COVID-19 treatment trials: A review and global call to action. Lancet Glob. Health 2021, 9, e366–e371. [Google Scholar] [CrossRef]
- Nooney, J.; Thor, S.; de Vries, C.; Clements, J.; Sahin, L.; Hua, W.; Everett, D.; Zaccaria, C.; Ball, R.; Saint-Raymond, A.; et al. Assuring Access to Safe Medicines in Pregnancy and Breastfeeding. Clin. Pharm. Ther. 2021, 110, 941–945. [Google Scholar] [CrossRef]
- Levy, A.T.; Singh, S.; Riley, L.E.; Prabhu, M. Acceptance of COVID-19 vaccination in pregnancy: A survey study. Am. J. Obs. Gynecol. MFM 2021, 3, 100399. [Google Scholar] [CrossRef]
- Gilkey, M.B.; McRee, A.L. Provider communication about HPV vaccination: A systematic review. Hum. Vaccines Immunother. 2016, 12, 1454–1468. [Google Scholar] [CrossRef] [PubMed]
- McElfish, P.A.; Willis, D.E.; Shah, S.K.; Bryant-Moore, K.; Rojo, M.O.; Selig, J.P. Sociodemographic Determinants of COVID-19 Vaccine Hesitancy, Fear of Infection, and Protection Self-Efficacy. J. Prim. Care Community Health 2021, 12, 21501327211040746. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Prabhu, M.; Murphy, E.A.; Sukhu, A.C.; Yee, J.; Singh, S.; Eng, D.; Zhao, Z.; Riley, L.E.; Yang, Y.J. Antibody Response to Coronavirus Disease 2019 (COVID-19) Messenger RNA Vaccination in Pregnant Women and Transplacental Passage into Cord Blood. Obstet. Gynecol. 2021, 138, 278–280. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk after COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. COVID-19 vaccine response in pregnant and lactating women: A cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Baird, J.K.; Jensen, S.M.; Urba, W.J.; Fox, B.A.; Baird, J.R. SARS-CoV-2 Antibodies Detected in Mother′s Milk Post-Vaccination. J. Hum. Lact. 2021, 37, 492–498. [Google Scholar] [CrossRef]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef]
- Buchy, P.; Ascioglu, S.; Buisson, Y.; Datta, S.; Nissen, M.; Tambyah, P.A.; Vong, S. Impact of vaccines on antimicrobial resistance. Int. J. Infect. Dis. 2020, 90, 188–196. [Google Scholar] [CrossRef]
- Brady, R.C.; Jackson, L.A.; Frey, S.E.; Shane, A.L.; Walter, E.B.; Swamy, G.K.; Schlaudecker, E.P.; Szefer, E.; Wolff, M.; McNeal, M.M.; et al. Randomized trial comparing the safety and antibody responses to live attenuated versus inactivated influenza vaccine when administered to breastfeeding women. Vaccine 2018, 36, 4663–4671. [Google Scholar] [CrossRef]
- DGGG. Empfehlung der COVID-19-Impfung für Schwangere und Stillende Frauen. 2021. Available online: https://www.dggg.de/stellungnahmen/empfehlung-der-covid-19-impfung-fuer-schwangere-und-stillende-frauen (accessed on 3 July 2022).
- ACOG. COVID-19 Vaccination during Pregnancy Is Key to Saving Lives, Medical Experts Urge. 2021. Available online: https://www.acog.org/news/news-releases/2021/12/covid-19-vaccination-during-pregnancy-is-key-to-saving-lives-statement (accessed on 3 July 2022).
- RCOG. Coronavirus (COVID-19), Pregnancy and Women’s Health. 2021. Available online: https://www.rcog.org.uk/guidance/coronavirus-covid-19-pregnancy-and-women-s-health/ (accessed on 3 July 2022).
- Costantino, C.; Mazzucco, W.; Bonaccorso, N.; Cimino, L.; Conforto, A.; Sciortino, M.; Catalano, G.; D′Anna, M.R.; Maiorana, A.; Venezia, R.; et al. Educational Interventions on Pregnancy Vaccinations during Childbirth Classes Improves Vaccine Coverages among Pregnant Women in Palermo′s Province. Vaccines 2021, 9, 1455. [Google Scholar] [CrossRef] [PubMed]
- Sebghati, M.; Khalil, A. Uptake of vaccination in pregnancy. Best Pract. Res. Clin. Obs. Gynaecol. 2021, 76, 53–65. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schirwani, N.; Pateisky, P.; Koren, T.; Farr, A.; Kiss, H.; Bancher-Todesca, D. Written Briefing and Oral Counseling Increase the Willingness to Receive the SARS-CoV-2 Vaccination among Women in Puerperium: A Qualitative Prospective Cohort Study. Vaccines 2022, 10, 1505. https://doi.org/10.3390/vaccines10091505
Schirwani N, Pateisky P, Koren T, Farr A, Kiss H, Bancher-Todesca D. Written Briefing and Oral Counseling Increase the Willingness to Receive the SARS-CoV-2 Vaccination among Women in Puerperium: A Qualitative Prospective Cohort Study. Vaccines. 2022; 10(9):1505. https://doi.org/10.3390/vaccines10091505
Chicago/Turabian StyleSchirwani, Nawa, Petra Pateisky, Tamina Koren, Alex Farr, Herbert Kiss, and Dagmar Bancher-Todesca. 2022. "Written Briefing and Oral Counseling Increase the Willingness to Receive the SARS-CoV-2 Vaccination among Women in Puerperium: A Qualitative Prospective Cohort Study" Vaccines 10, no. 9: 1505. https://doi.org/10.3390/vaccines10091505
APA StyleSchirwani, N., Pateisky, P., Koren, T., Farr, A., Kiss, H., & Bancher-Todesca, D. (2022). Written Briefing and Oral Counseling Increase the Willingness to Receive the SARS-CoV-2 Vaccination among Women in Puerperium: A Qualitative Prospective Cohort Study. Vaccines, 10(9), 1505. https://doi.org/10.3390/vaccines10091505