
The Use of Adaptive Sampling to Reach Disadvantaged Populations for Immunization Programs and Assessments: A Systematic Review

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
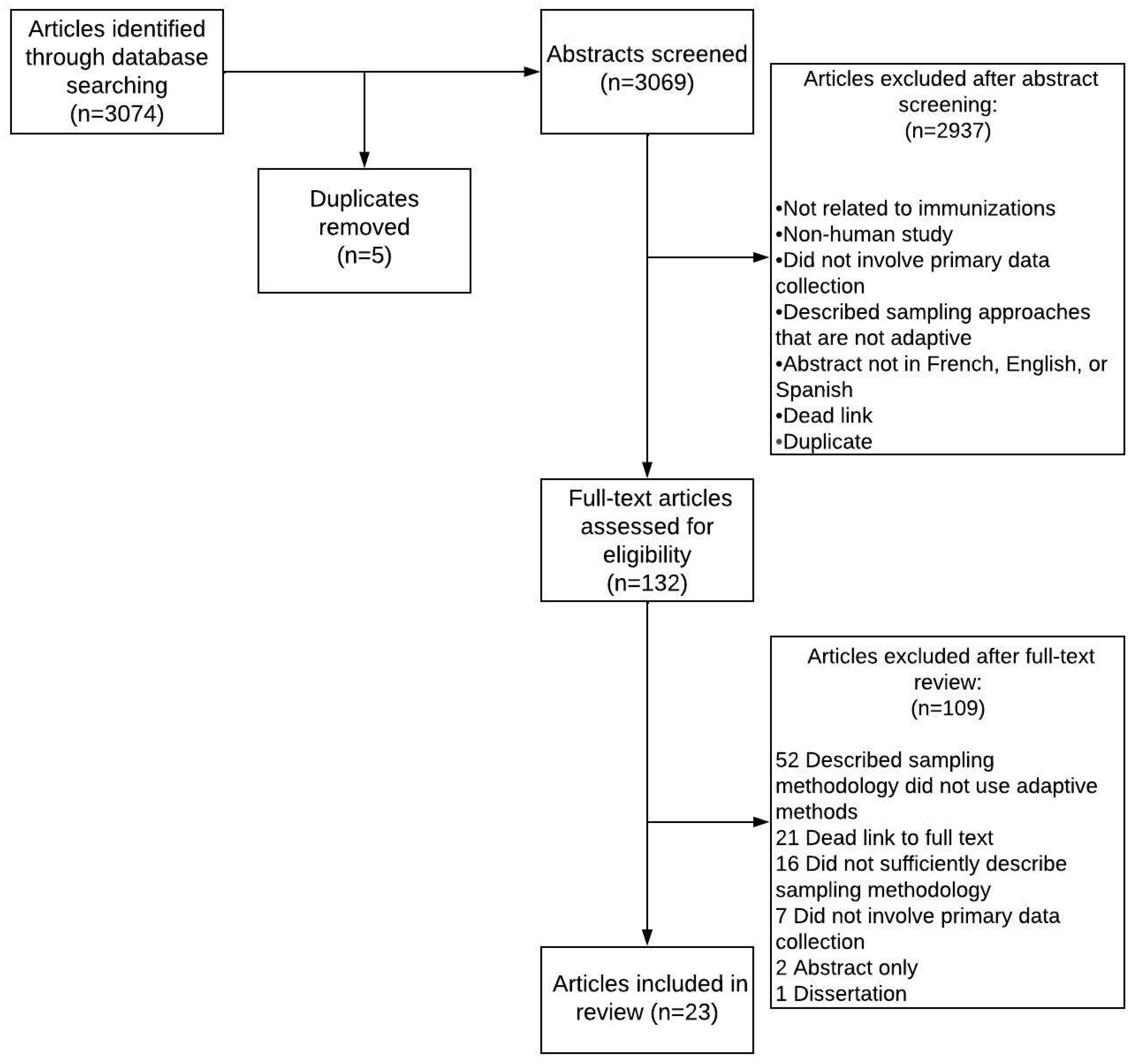
2.2. Study Selection
2.3. Data Extraction
2.4. Data Analysis
3. Results
3.1. Sampling Methods
3.2. Types of Data Collected
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Literature search terms: |
| Five journal databases (PubMed, EMBASE, Medline, PsycInfo, CINAHL) were searched based on the following search terms: |
| Sampling stud* OR (Adaptive ADJ2 sampling) OR (modif* ADJ2 sampling) OR (Snowball ADJ2 sampling) OR (Respondent driven ADJ2 sampling) OR (Indigenous field worker ADJ2 sampling) OR (Targeted ADJ2 sampling) OR (Time location ADJ2 sampling) OR (Capture recapture ADJ2 sampling) OR Rapid assessment response OR (Spatial ADJ2 sampling) OR (Geospatial ADJ2 sampling) OR Satellite imagery OR (compact segment ADJ2 sampling) OR grid sampling OR sampling grid OR (second stage ADJ2 sampling) OR (two cluster ADJ2 sampling) |
| AND |
| Vaccin* OR immuni* OR virus* OR disease* |
| AND |
| subpopulation* OR sub-population* OR vulnerable* OR homeless* OR marginalized OR under-represented OR hard-to-reach OR hidden population* OR at-risk OR high risk OR displaced OR migrant* OR migrating OR nomad* OR transient* OR settlement* OR refugee* OR inaccessible OR infant* OR children OR preschool* OR pre-school* OR target population* OR rural population* OR rural area* |
References
- Rodrigues, C.M.C.; Plotkin, S.A. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mukandavire, C.; Cucunubá, Z.M.; Londono, S.E.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: A modelling study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef]
- Immunization Coverage: Are We Losing Ground? [Internet]. UNICEF DATA. 2020. Available online: https://data.unicef.org/resources/immunization-coverage-are-we-losing-ground/ (accessed on 4 January 2021).
- Hacker, K.; Anies, M.; Folb, B.L.; Zallman, L. Barriers to health care for undocumented immigrants: A literature review. Risk Manag Health Policy 2015, 8, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Claquin, P.; Danovaro-Holliday, M.C.; Rhoda, D.A. Monitoring vaccination coverage: Defining the role of surveys. Vaccine 2016, 34, 4103–4109. [Google Scholar] [CrossRef] [PubMed]
- Watters, J.K.; Biernacki, P. Targeted Sampling: Options for the Study of Hidden Populations. Soc. Probl. 1989, 36, 416–430. [Google Scholar] [CrossRef]
- Zucker, J.R.; Rosen, J.B.; Iwamoto, M.; Arciuolo, R.J.; Langdon-Embry, M.; Vora, N.M.; Rakeman, J.L.; Isaac, B.M.; Jean, A.; Asfaw, M.; et al. Consequences of Undervaccination—Measles Outbreak, New York City, 2018–2019. N. Engl. J. Med. 2020, 382, 1009–1017. [Google Scholar] [CrossRef]
- Gidado, S.O.; Ohuabunwo, C.; Nguku, P.M.; Ogbuanu, I.U.; Waziri, N.E.; Biya, O.; Wiesen, E.S.; Mba-Jonas, A.; Vertefeuille, J.; Oyemakinde, A.; et al. Outreach to underserved communities in northern Nigeria, 2012–2013. J. Infect. Dis. 2014, 210 (Suppl. 1), S118–S124. [Google Scholar] [CrossRef]
- Thompson, K.M.; Duintjer Tebbens, R.J. Lessons From the Polio Endgame: Overcoming the Failure to Vaccinate and the Role of Subpopulations in Maintaining Transmission. J. Infect. Dis 2017, 216, S176–S182. [Google Scholar] [CrossRef]
- Chard, A.N.; Gacic-Dobo, M.; Diallo, M.S.; Sodha, S.V.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1706–1710. [Google Scholar] [CrossRef]
- Vaccination Coverage Cluster Surveys: Reference Manual; Report No.: (WHO/IVB/18.09); World Health Organization: Geneva, Switzerland, 2018.
- Ozawa, S.; Yemeke, T.T.; Evans, D.R.; Pallas, S.E.; Wallace, A.S.; Lee, B.Y. Defining hard-to-reach populations for vaccination. Vaccine 2019, 37, 5525–5534. [Google Scholar] [CrossRef]
- Thompson, S.K.; Collins, L.M. Adaptive sampling in research on risk-related behaviors. Drug Alcohol Depend. 2002, 68 (Suppl. 1), S57–S67. [Google Scholar] [CrossRef]
- Magnani, R.; Sabin, K.; Saidel, T.; Heckathorn, D. Review of sampling hard-to-reach and hidden populations for HIV surveillance. AIDS 2005, 19, S67. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Seizing the Moment: Tackling Entrenched Inequalities to End Epidemics. Global AIDS Update; UNAIDS: Geneva, Switzerland, 2020. [Google Scholar]
- Abdul-Quader, A.S.; Baughman, A.L.; Hladik, W. Estimating the size of key populations: Current status and future possibilities. Curr. Opin. HIV AIDS 2014, 9, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.; Saidel, T.; Magnani, R.; Brown, T. Surveillance and modelling of HIV, STI, and risk behaviours in concentrated HIV epidemics. Sex. Transm. Infect. 2004, 80, ii57–ii62. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Weekly Epidemiological Record. Report No.: No 20, 2022, 97. May 2022; pp. 209–224. Available online: https://apps.who.int/iris/bitstream/handle/10665/354458/WER9720-eng-fre.pdf (accessed on 2 July 2022).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind. April 2020. Available online: https://cdn.who.int/media/docs/default-source/immunization/strategy/ia2030/ia2030-draft-4-wha_b8850379-1fce-4847-bfd1-5d2c9d9e32f8.pdf?sfvrsn=5389656e_66&download=true (accessed on 14 December 2022).
- Higgins, J.; Adamu, U.; Adewara, K.; Aladeshawe, A.; Aregay, A.; Barau, I.; Berens, A.; Bolu, O.; Dutton, N.; Iduma, N.; et al. Finding inhabited settlements and tracking vaccination progress: The application of satellite imagery analysis to guide the immunization response to confirmation of previously-undetected, ongoing endemic wild poliovirus transmission in Borno State, Nigeria. Int. J. Health Geogr. 2019, 18, 11. [Google Scholar] [CrossRef]
- Rosencrans, L.C.; Sume, G.E.; Kouontchou, J.-C.; Voorman, A.; Anokwa, Y.; Fezeu, M.; Seaman, V.Y. Mapping for Health in Cameroon: Polio Legacy and Beyond. J. Infect. Dis. 2017, 216, S337–S342. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.G.; Magnani, R.J.; Shuaib, M. A Not Quite as Quick but Much Cleaner Alternative to the Expanded Programme on Immunization (EPI) Cluster Survey Design. Int J. Epidemiol 1996, 25, 198–203. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- The World Bank. World Bank Country and Lending Groups. 2021. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 10 November 2022).
- Ben Natan, M.; El Kravchenko, B.; Sakashidlo, K.; Mor, S. What drives pregnant women’s decisions to accept the pertussis vaccine? Appl. Nurs. Res. 2017, 38, 60–63. [Google Scholar] [CrossRef]
- Baars, J.E.; Boon, B.J.; Garretsen, H.F.; van de Mheen, D. Vaccination uptake and awareness of a free hepatitis B vaccination program among female commercial sex workers. Womens Health Issues 2009, 19, 61–69. [Google Scholar] [CrossRef]
- Coreil, J.; Augustin, A.; Holt, E.; Halsey, N.A. Use of ethnographic research for instrument development in a case-control study of immunization use in Haiti. Int. J. Epidemiol. 1989, 18, S33–S37. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Sutton, J.; Reid, G.J.; Beynon, C.; Cohen, I.; Huffman, D. Universal influenza immunization. Were Ontario family physicians prepared? Can. Fam. Physician 2003, 49, 1315–1321. [Google Scholar] [PubMed]
- Baars, J.E.; Boon, B.J.; Garretsen, H.F.; van de Mheen, D. The reach of a hepatitis B vaccination programme among men who have sex with men. Eur. J. Public Health 2011, 21, 333–337. [Google Scholar] [CrossRef]
- Pearce, C.; Leask, J.; Ritchie, J. Tapping midwives’ views about the neonatal hepatitis B vaccine: How welcome is a move towards a health promoting orientation? Health Promot. J. Aust. 2008, 19, 161–163. [Google Scholar] [CrossRef]
- Brito Magalhães, R.d.L.; Moura Carvalho, V.; Ibiapina Brito, G.M.; Braz de Oliveira, L.; Gimeniz Galvão, M.T.; Gir, E. Risk practices and immunization against hepatitis B among female sex workers. Rev. Rene 2016, 17, 636–642. [Google Scholar] [CrossRef]
- Jama, A.; Ali, M.; Lindstrand, A.; Butler, R.; Kulane, A. Perspectives on the Measles, Mumps and Rubella Vaccination among Somali Mothers in Stockholm. Int. J. Environ. Res. Public Health 2018, 15, 2428. [Google Scholar] [CrossRef]
- Parker, L.A.; Rumunu, J.; Jamet, C.; Kenyi, Y.; Lino, R.L.; Wamala, J.F.; Mpairwe, A.M.; Muller, V.; Llosa, A.E.; Uzzeni, F.; et al. Neighborhood-targeted and case-triggered use of a single dose of oral cholera vaccine in an urban setting: Feasibility and vaccine coverage. PLoS Negl. Trop. Dis. 2017, 11, e0005652. [Google Scholar] [CrossRef]
- Shand, L.; Burney, S.; Fletcher, J. Knowledge of cervical cancer, pap testing and the human papillomavirus among young Australian women. Health Promot. J. Aust. 2010, 21, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, X.; Qiu, P.; Ma, X.; Chou, C.P. Integrating spatial technology into studying the generational differences of migrants’ health protection status in urban China. Int. J. Equity Health 2015, 14, 27. [Google Scholar] [CrossRef]
- Barau, I.; Zubairu, M.; Mwanza, M.N.; Seaman, V.Y. Improving polio vaccination coverage in Nigeria through the use of geographic information system technology. J. Infect. Dis. 2014, 210 (Suppl. 1), S102–S110. [Google Scholar] [CrossRef] [Green Version]
- Koehlmoos, T.P.; Uddin, J.; Sarma, H. Impact of measles eradication activities on routine immunization services and health systems in Bangladesh. J. Infect. Dis. 2011, 204 (Suppl. 1), S90–S97. [Google Scholar] [CrossRef]
- Massing, L.A.; Aboubakar, S.; Blake, A.; Page, A.L.; Cohuet, S.; Ngandwe, A.; Mukomena Sompwe, E.; Ramazani, R.; Allheimen, M.; Levaillant, P.; et al. Highly targeted cholera vaccination campaigns in urban setting are feasible: The experience in Kalemie, Democratic Republic of Congo. PLoS Negl. Trop. Dis. 2018, 12, e0006369. [Google Scholar] [CrossRef] [PubMed]
- Puga, M.A.M.; Bandeira, L.M.; Weis, S.; Fernandes, F.R.P.; Castro, L.S.; Tanaka, T.S.O.; Rezende, G.R.; Teles, S.A.; Castro, V.O.L.; Murat, P.G.; et al. High-risk behaviors for hepatitis B and C infections among female sex workers. Rev. Da Soc. Bras. De Med. Trop. 2018, 51, 198–202. [Google Scholar] [CrossRef]
- McDonald, P.; Limaye, R.J.; Omer, S.B.; Buttenheim, A.M.; Mohanty, S.; Klein, N.P.; Salmon, D.A. Exploring California’s new law eliminating personal belief exemptions to childhood vaccines and vaccine decision-making among homeschooling mothers in California. Vaccine 2019, 37, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Peel, R.; Ren, S.; Hure, A.; Levi, C.R.; Sturm, J.; Durrheim, D.; McEvoy, M.; Newby, D.A.; Hansbro, P.M.; Attia, J.R.; et al. Evaluating recruitment strategies for AUSPICE, a large Australian community-based randomised controlled trial. Med. J. Aust. 2019, 210, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Grais, R.F.; Rose, A.M.; Guthmann, J.P. Don’t spin the pen: Two alternative methods for second-stage sampling in urban cluster surveys. Emerg. Themes Epidemiol. 2007, 4, 8. [Google Scholar] [CrossRef]
- Ferreras, E.; Matapo, B.; Chizema-Kawesha, E.; Chewe, O.; Mzyece, H.; Blake, A.; Moonde, L.; Zulu, G.; Poncin, M.; Sinyange, N.; et al. Delayed second dose of oral cholera vaccine administered before high-risk period for cholera transmission: Cholera control strategy in Lusaka, 2016. PLoS ONE 2019, 14, e0219040. [Google Scholar] [CrossRef] [PubMed]
- Gullion, J.S.; Henry, L.; Gullion, G. Deciding to opt out of childhood vaccination mandates. Public Health Nurs. 2008, 25, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Milligan, P.; Njie, A.; Bennett, S. Comparison of two cluster sampling methods for health surveys in developing countries. Int. J. Epidemiol. 2004, 33, 469–476. [Google Scholar] [CrossRef]
- Gong, W.; Taighoon Shah, M.; Firdous, S.; Jarrett, B.A.; Moulton, L.H.; Moss, W.J.; Hayford, K.; O’Brien, K.L.; Chandir, S. Comparison of three rapid household survey sampling methods for vaccination coverage assessment in a peri-urban setting in Pakistan. Int. J. Epidemiol. 2019, 48, 583–595. [Google Scholar] [CrossRef]
- Roberton, T.; Weiss, W.; Jordan Health Access Study, T.; Lebanon Health Access Study, T.; Doocy, S. Challenges in Estimating Vaccine Coverage in Refugee and Displaced Populations: Results From Household Surveys in Jordan and Lebanon. Vaccines 2017, 5, 22. [Google Scholar] [CrossRef]
- WHO, CDC, UNAIDS, FHI 360. Biobehavioral Survey Guidelines for Populations at Risk for HIV; World Health Organization: Geneva, Switzerland, 2017.
- Sodha, S.V.; Dietz, V. Strengthening routine immunization systems to improve global vaccination coverage. Br. Med. Bull. 2015, 113, 5–14. [Google Scholar] [CrossRef]
- Oyo-Ita, A.; Wiysonge, C.S.; Oringanje, C.; Nwachukwu, C.E.; Oduwole, O.; Meremikwu, M.M. Interventions for Improving Coverage of Childhood Immunisation in Low- and Middle-Income Countries. Cochrane Effective Practice and Organisation of Care Group, Editor. Cochrane Database of Systematic Reviews [Internet]. 10 July 2016. Available online: https://doi.wiley.com/10.1002/14651858.CD008145.pub3 (accessed on 7 January 2023).
- Cutts, F.T. Strategies to improve immunization services in urban Africa. Bull World Health Organ 1991, 69, 407–414. [Google Scholar] [PubMed]
- Behavioural and Social Drivers of Vaccination: Tools and Practical Guidance for Achieving High Uptake; World Health Organization: Geneva, Switzerland, 2022.
- Editorial the Guardian View on Global Vaccine Inequality: Unwise as Well as Unethical. The Guardian [Internet]. 25 August 2021. Available online: https://www.theguardian.com/commentisfree/2021/aug/25/the-guardian-view-on-global-vaccine-inequality-unwise-as-well-as-unethical (accessed on 8 October 2021).
- Badowski, G.; Somera, L.P.; Simsiman, B.; Lee, H.-R.; Cassel, K.; Yamanaka, A.; Ren, J. The efficacy of respondent-driven sampling for the health assessment of minority populations. Cancer Epidemiol. 2017, 50, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Garcini, L.M.; Galvan, T.; Peña, J.M.; Chen, N.; Klonoff, E. Effectiveness of Respondent-Driven Sampling for Conducting Health Studies Among Undocumented Immigrants at a Time of Heightened Immigration Enforcement. J. Immigr. Minor. Health 2022, 24, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Jauffret-Roustide, M.; Le Strat, Y. Design, Sampling, Organising the Field for a TLS Survey and New Developments: Coquelicot, a Survey of Drug Users. Methodol. Innov. Online 2010, 5, 26–37. [Google Scholar] [CrossRef]


{kind=link}
| Study | Year | Country | Sampling Type | Target Population | Age Eligibility | Vaccines A | Study Objectives |
|---|---|---|---|---|---|---|---|
| Milligan, P. et al. [45] | 2000 | GMB | Compact segment | Mothers and caregivers of children | Mothers and caregivers of children aged 12–23 months | Routine immunizations; yellow fever | Measure coverage; Compare sampling methods |
| Baars, J. E. et al. [29] | 2004 | NLD | Ethnographic mapping; Venue-based | Men who have sex with men | Not specified | Hepatitis B | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Baars, J. E. et al. [26] | 2004 | NLD | Ethnographic mapping; Venue-based | Sex workers | Not specified | Hepatitis B | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Grais, R. F. et al. [42] | 2006 | NER | Geospatial | General population | Not specified | Meningitis | Measure coverage; Compare sampling methods |
| Massing, L. A. et al. [38] | 2014 | DRC | Geospatial | General population | ≥1 year | Oral cholera | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Ferreras, E. et al. [43] | 2016 | ZMB | Geospatial | General population | >1 year | Oral cholera | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Parker, L. A. et al. [33] | 2015 | SSD | Geospatial | General population; internally displaced persons; slum residents; healthcare providers; prisoners/inmates | >1 year | Oral cholera | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Barau, I. et al. [36] | 2012 | NGA | Geospatial | Mothers and caregivers of children | Not specified | Oral polio | Enhance microplanning; Deliver vaccines; Compare sampling methods |
| Gong, W. et al. [46] | 2016 | PAK | Geospatial; Compact segment | Mothers and caregivers of children | Mothers and caregivers of children aged 12–23 months | Routine immunizations | Measure coverage; Compare sampling methods |
| Shand, L. et al. [34] | 2008 | AUS | Peer-driven | General population | 18–26 years | Human papillomavirus | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Peel, R. et al. [41] | 2016 | AUS | Peer-driven | General population | 55–60 years | Pneumococcal polysaccharide | Compare sampling methods |
| Pearce, C. et al. [30] | 2003 | AUS | Peer-driven | Healthcare providers | Not specified | Hepatitis B; All immunizations generally | Measure attitudes, behaviors and vaccine uptake barriers |
| Russell, G. et al. [28] | 2001 | CAN | Peer-driven | Healthcare providers | Not specified | Influenza | Measure attitudes, behaviors and vaccine uptake barriers |
| Koehlmoos, T. P. et al. [37] | Unknown | BGD | Peer-driven | Healthcare providers; government staff; health systems staff that do not directly provide care | Not specified | All immunizations generally; Routine immunizations | Health systems improvement |
| Jama, A. et al. [32] | 2013 | SWE | Peer-driven | Mothers and caregivers of children; immigrants/ethnic minority | Mothers and caregivers of children aged 18 months to 5 years | Routine immunizations | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Ben Natan, M. et al. [25] | 2016 | ISR | Peer-driven | Mothers and caregivers of children | Not specified | Pertussis | Measure attitudes, behaviors and vaccine uptake barriers |
| McDonald, P. et al. [40] | 2017 | USA | Peer-driven | Mothers and caregivers of children | Mothers and caregivers of children in kindergarten (~5 years) through 12th grade (~17–18 years) | All immunizations generally | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Puga, M. A. M. et al. [39] | 2009 | BRA | Peer-driven and fully compliant with RDS | Sex workers | Not specified | Hepatitis B | Measure coverage; Deliver vaccines; Measure attitudes, behaviors and vaccine uptake barriers |
| Yang, Y. et al. [35] | 2008 | CHN | Peer-driven and partially compliant with RDS | Migrants | Not specified | Hepatitis B | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Magalhaes, R.L.B et al. [31] | 2014 | BRA | Peer-driven and partially compliant with RDS | Sex workers | ≥18 years | Hepatitis B | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers; Deliver services |
| Roberton, T. et al. [47] | 2014 | JOR; LBN | Peer-driven; Geospatial | Mothers and caregivers of children; Refugees | Mothers and caregivers of children aged 12–23 months | All immunizations generally; Routine immunizations | Measure coverage; Measure attitudes, behaviors and vaccine uptake barriers |
| Gullion, J. S. et al. [44] | Unknown | USA | Peer-driven; Venue-based | Mothers and caregivers of children | Not specified | All immunizations generally | Measure attitudes, behaviors and vaccine uptake barriers |
| Coreil, J. et al. [27] | 1987 | HTI | Venue-based | Mothers and caregivers of children | Mothers and caregivers of children aged 12–23 months | All immunizations generally | Measure attitudes, behaviors and vaccine uptake barriers |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koyuncu, A.; Ishizumi, A.; Daniels, D.; Jalloh, M.F.; Wallace, A.S.; Prybylski, D. The Use of Adaptive Sampling to Reach Disadvantaged Populations for Immunization Programs and Assessments: A Systematic Review. Vaccines 2023, 11, 424. https://doi.org/10.3390/vaccines11020424
Koyuncu A, Ishizumi A, Daniels D, Jalloh MF, Wallace AS, Prybylski D. The Use of Adaptive Sampling to Reach Disadvantaged Populations for Immunization Programs and Assessments: A Systematic Review. Vaccines. 2023; 11(2):424. https://doi.org/10.3390/vaccines11020424
Chicago/Turabian StyleKoyuncu, Aybüke, Atsuyoshi Ishizumi, Danni Daniels, Mohamed F. Jalloh, Aaron S. Wallace, and Dimitri Prybylski. 2023. "The Use of Adaptive Sampling to Reach Disadvantaged Populations for Immunization Programs and Assessments: A Systematic Review" Vaccines 11, no. 2: 424. https://doi.org/10.3390/vaccines11020424
APA StyleKoyuncu, A., Ishizumi, A., Daniels, D., Jalloh, M. F., Wallace, A. S., & Prybylski, D. (2023). The Use of Adaptive Sampling to Reach Disadvantaged Populations for Immunization Programs and Assessments: A Systematic Review. Vaccines, 11(2), 424. https://doi.org/10.3390/vaccines11020424