
CVAPPS: A Cross-Sectional Study of SARS-CoV-2 Vaccine Acceptance, Perceptions, and Post-Vaccination Side Effects among Rheumatic Disease Patients in Kuwait

Abstract
:1. Introduction
2. Methods
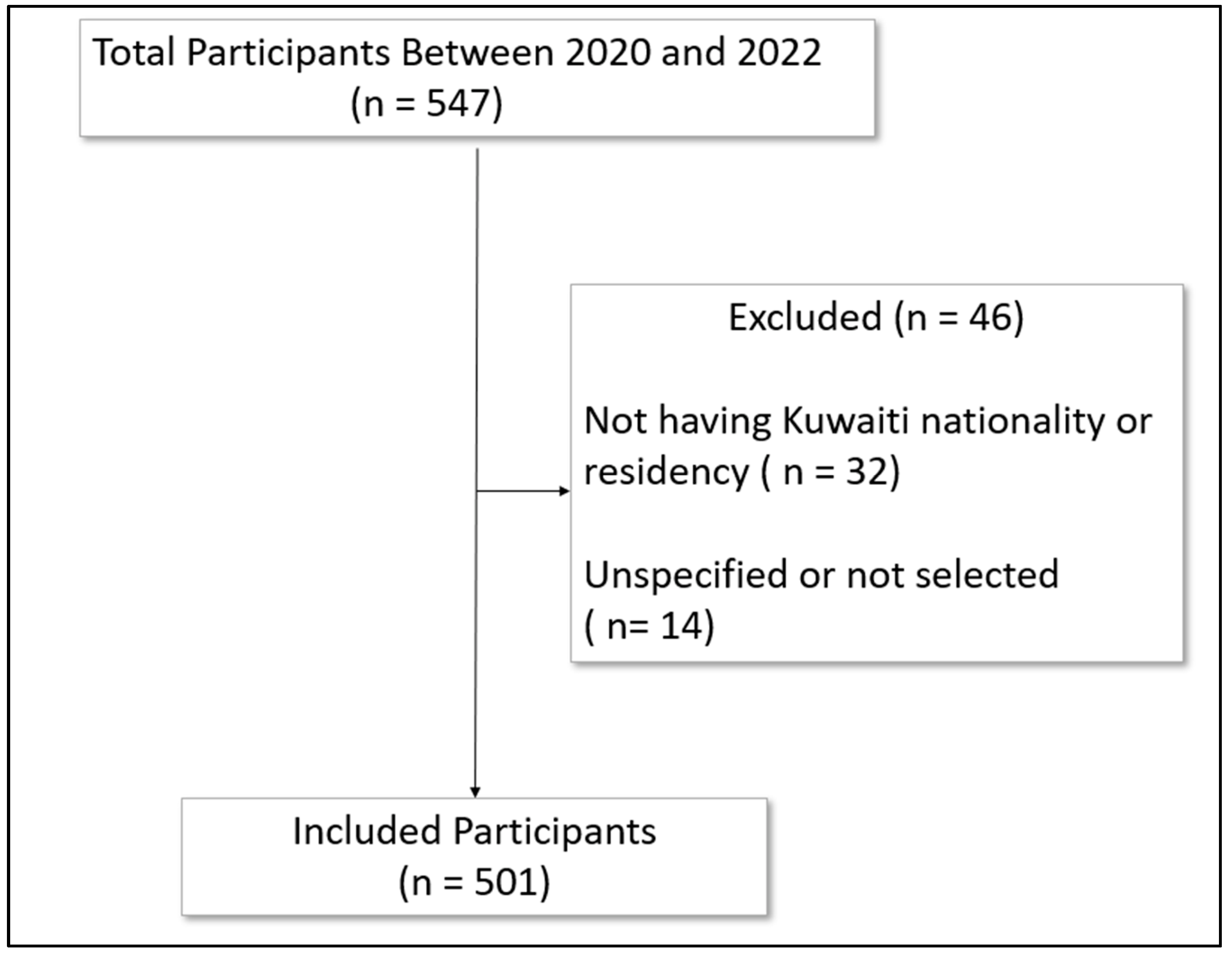
2.1. Study Population and Data Source
2.2. Data Sources/Measurement
2.3. Study Size
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Included Participants
3.2. SARS-CoV-2 Vaccine Status among the Included Participants
3.3. Vaccination Status Based on Demographic Characteristics
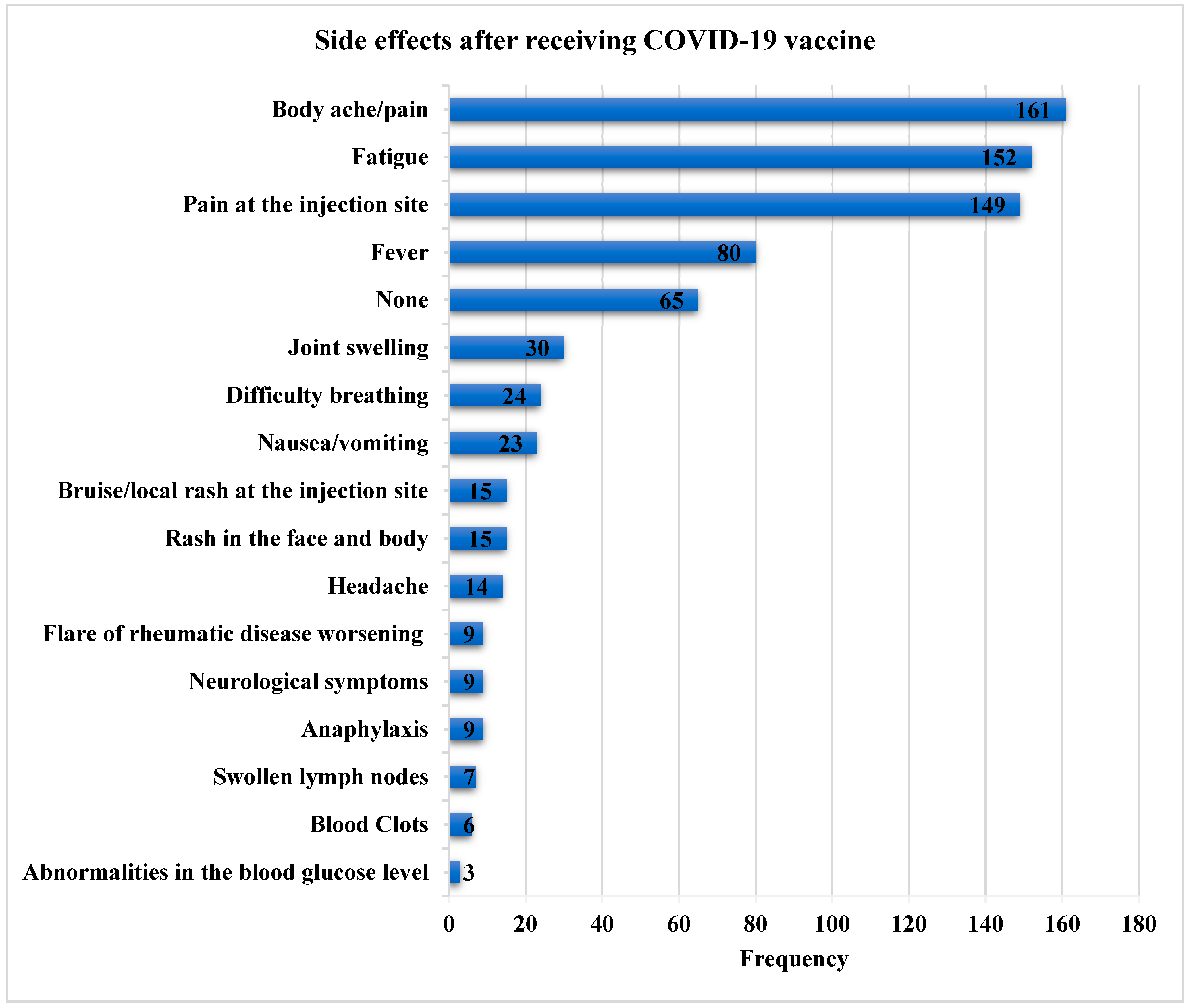
3.4. Side Effects
3.5. Flares Post-SARS-CoV-2 Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ebada, M.A.; Wadaa-Allah, A.; Bahbah, E.; Negida, A. An Updated Review on COVID-19. Infect. Disord. Drug Targets 2021, 21, e160921189190. [Google Scholar] [CrossRef]
- Abdelgawad, H.A.H.; Sayed, A.; Munir, M.; Elberry, M.H.; Sayed, I.M.; Kamal, M.A.; Negida, A.; Ebada, M.A.; Bahbah, E.I. Clinical Review of COVID-19; Pathogenesis, Diagnosis, and Management. Curr. Pharm. Des. 2021, 27, 4232–4244. [Google Scholar] [CrossRef] [PubMed]
- Gabra, M.D.; Ghaith, H.S.; Ebada, M.A. Nipah Virus: An Updated Review and Emerging Challenges. Infect. Disord. Drug Targets 2022, 22, e170122200296. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.-T.; Hsu, B.-C.; Chen, D.-Y. Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines in Rheumatic Patients: An Updated Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 834. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Rutherford, M.A.; Scott, J.; Karabayas, M.; Antonelou, M.; Gopaluni, S.; Gray, D.; Barrett, J.; Brix, S.R.; Dhaun, N.; McAdoo, S.P.; et al. Risk Factors for Severe Outcomes in Patients With Systemic Vasculitis and COVID-19: A Binational, Registry-Based Cohort Study. Arthritis Rheumatol. 2021, 73, 1713–1719. [Google Scholar] [CrossRef]
- Ahmed, S.; Gasparyan, A.Y.; Zimba, O. Comorbidities in rheumatic diseases need special consideration during the COVID-19 pandemic. Rheumatol. Int. 2021, 41, 243–256. [Google Scholar] [CrossRef]
- Hyrich, K.L.; Machado, P.M. Rheumatic disease and COVID-19: Epidemiology and outcomes. Nat. Rev. Rheumatol. 2021, 17, 71–72. [Google Scholar] [CrossRef]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef]
- Arnold, J.; Winthrop, K.; Emery, P. COVID-19 vaccination and antirheumatic therapy. Rheumatology 2021, 60, 3496–3502. [Google Scholar] [CrossRef]
- Prendecki, M.; Clarke, C.; Edwards, H.; McIntyre, S.; Mortimer, P.; Gleeson, S.; Martin, P.; Thomson, T.; Randell, P.; Shah, A.; et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann. Rheum. Dis. 2021, 80, 1322–1329. [Google Scholar] [CrossRef]
- Malipiero, G.; Moratto, A.; Infantino, M.; D’Agaro, P.; Piscianz, E.; Manfredi, M.; Grossi, V.; Benvenuti, E.; Bulgaresi, M.; Benucci, M.; et al. Assessment of humoral and cellular immunity induced by the BNT162b2 SARS-CoV-2 vaccine in healthcare workers, elderly people, and immunosuppressed patients with autoimmune disease. Immunol. Res. 2021, 69, 576–583. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.; Betschel, S.D.; Cheung, M.; Hicks, L.K. Vaccine response following anti-CD20 therapy: A systematic review and meta-analysis of 905 patients. Blood Adv. 2021, 5, 2624–2643. [Google Scholar] [CrossRef]
- Geisen, U.M.; Berner, D.K.; Tran, F.; Sümbül, M.; Vullriede, L.; Ciripoi, M.; Reid, H.M.; Schaffarzyk, A.; Longardt, A.C.; Franzenburg, J.; et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann. Rheum. Dis. 2021, 80, 1306–1311. [Google Scholar] [CrossRef]
- Avouac, J.; Drumez, E.; Hachulla, E.; Seror, R.; Georgin-Lavialle, S.; El Mahou, S.; Pertuiset, E.; Pham, T.; Marotte, H.; Servettaz, A.; et al. COVID-19 outcomes in patients with inflammatory rheumatic and musculoskeletal diseases treated with rituximab: A cohort study. Lancet Rheumatol. 2021, 3, e419–e426. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. Declaration of Helsinki, Ethical principles for medical research involving human subjects. In Proceedings of the 64th WMA General Assembly, Fortaleza, Brazil, 16–19 October 2013; Volume 107. [Google Scholar]
- Khaled Fahim, N.; Negida, A. Sample Size Calculation Guide—Part 1: How to Calculate the Sample Size Based on the Prevalence Rate. Adv. J. Emerg. Med. 2018, 2, e50. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069. [Google Scholar] [CrossRef]
- Hasseli, R.; Ladner, U.M. COVID-19 and inflammatory rheumatic diseases. Dtsch. Med. Wochenschr. 2021, 146, 1564–1568. [Google Scholar] [CrossRef]
- McKeigue, P.; Porter, D.; Hollick, R.; Ralston, S.; McAllister, D.; Colhoun, H. Risk of severe COVID-19 in patients with inflammatory rheumatic diseases treated with immunosuppressive therapy in Scotland. Scand. J. Rheumatol. 2022, 1–6. [Google Scholar] [CrossRef]
- Day, A.L.; Winthrop, K.L.; Curtis, J.R. The effect of disease-modifying antirheumatic drugs on vaccine immunogenicity in adults. Cleve Clin. J. Med. 2020, 87, 695. [Google Scholar] [CrossRef] [PubMed]
- Boekel, L.; Hooijberg, F.; Besten, Y.R.; Vogelzang, E.H.; Steenhuis, M.; Leeuw, M.; Atiqi, S.; van Vollenhoven, R.; Lems, W.F.; Bos, W.H.; et al. COVID-19 vaccine acceptance over time in patients with immune-mediated inflammatory rheumatic diseases. Lancet Rheumatol. 2022, 4, e310. [Google Scholar] [CrossRef] [PubMed]
- Barbhaiya, M.; Levine, J.M.; Bykerk, V.P.; Jannat-Khah, D.; Mandl, L.A. Systemic rheumatic disease flares after SARS-CoV-2 vaccination among rheumatology outpatients in New York City. Ann. Rheum. Dis. 2021, 80, 1352–1354. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Geng, Y.; Wang, Y.; Deng, X.; Li, G.; Zhao, J.; Ji, L.; Zhang, X.; Song, Z.; Zhang, H.; et al. Safety and disease flare of autoimmune inflammatory rheumatic diseases: A large real-world survey on inactivated COVID-19 vaccines. Ann. Rheum. Dis. 2022, 81, 443. [Google Scholar] [CrossRef]
- Park, J.K.; Lee, E.B.; Shin, K.; Sung, Y.K.; Kim, T.H.; Kwon, S.R.; Lee, M.S.; Hong, S.J.; Choi, B.Y.; Lee, S.S.; et al. COVID-19 Vaccination in Patients with Autoimmune Inflammatory Rheumatic Diseases: Clinical Guidance of the Korean College of Rheumatology. J. Korean Med. Sci. 2021, 36, e95. [Google Scholar] [CrossRef]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; Liebeskind, M.J.; et al. Glucocorticoids and B Cell Depleting Agents Substantially Impair Immunogenicity of mRNA Vaccines to SARS-CoV-2. MedRxiv 2021. [Google Scholar] [CrossRef]
- Gaur, P.; Agrawat, H.; Shukla, A. COVID-19 vaccine hesitancy in patients with systemic autoimmune rheumatic disease: An interview-based survey. Rheumatol. Int. 2021, 41, 1601–1605. [Google Scholar] [CrossRef]
- Ko, T.; Dendle, C.; Woolley, I.; Morand, E.; Antony, A. SARS-CoV-2 vaccine acceptance in patients with rheumatic diseases: A cross-sectional study. Hum. Vaccin. Immunother. 2021, 17, 4048–4056. [Google Scholar] [CrossRef]
- El Kibbi, L.; Metawee, M.; Hmamouchi, I.; Abdulateef, N.; Halabi, H.; Eissa, M.; El Rakawi, M.; Masri, B.; Abutiban, F.; Hamdi, W.; et al. Acceptability of the COVID-19 vaccine among patients with chronic rheumatic diseases and healthcare professionals: A cross-sectional study in 19 Arab countries. Lancet Rheumatol. 2022, 4, e160–e163. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Priori, R.; Pellegrino, G.; Colafrancesco, S.; Alessandri, C.; Ceccarelli, F.; Di Franco, M.; Riccieri, V.; Scrivo, R.; Scavalli, A.S.; Spinelli, F.R.; et al. SARS-CoV-2 vaccine hesitancy among patients with rheumatic and musculoskeletal diseases: A message for rheumatologists. Ann. Rheum. Dis. 2021, 80, 953–954. [Google Scholar] [CrossRef]
- Felten, R.; Dubois, M.; Ugarte-Gil, M.F.; Chaudier, A.; Kawka, L.; Bergier, H.; Costecalde, C.; Pijnenburg, L.; Fort, J.; Chatelus, E.; et al. Vaccination against COVID-19: Expectations and concerns of patients with autoimmune and rheumatic diseases. Lancet Rheumatol. 2021, 3, e243–e245. [Google Scholar] [CrossRef]
- Yurttas, B.; Poyraz, B.C.; Sut, N.; Ozdede, A.; Oztas, M.; Uğurlu, S.; Tabak, F.; Hamuryudan, V.; Seyahi, E. Willingness to get the COVID-19 vaccine among patients with rheumatic diseases, healthcare workers and general population in Turkey: A web-based survey. Rheumatol. Int. 2021, 41, 1105–1114. [Google Scholar] [CrossRef]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Avery, R.K.; Werbel, W.A.; Segev, D.L.; Garonzik-Wang, J.; Paik, J.J. Safety of the first dose of mRNA SARS-CoV-2 vaccines in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1100–1101. [Google Scholar] [CrossRef]
- Esquivel-Valerio, J.A.; Skinner-Taylor, C.M.; Moreno-Arquieta, I.A.; Cardenas-de la Garza, J.A.; Garcia-Arellano, G.; Gonzalez-Garcia, P.L.; Almaraz-Juarez, F.D.R.; Galarza-Delgado, D.A. Adverse events of six COVID-19 vaccines in patients with autoimmune rheumatic diseases: A cross-sectional study. Rheumatol. Int. 2021, 41, 2105–2108. [Google Scholar] [CrossRef]
- Machado, P.M.; Lawson-Tovey, S.; Strangfeld, A.; Mateus, E.F.; Hyrich, K.L.; Gossec, L.; Carmona, L.; Rodrigues, A.; Raffeiner, B.; Duarte, C.; et al. Safety of vaccination against SARS-CoV-2 in people with rheumatic and musculoskeletal diseases: Results from the EULAR Coronavirus Vaccine (COVAX) physician-reported registry. Ann. Rheum. Dis. 2022, 81, 695–709. [Google Scholar] [CrossRef]
- Raheel, S.; Matteson, E.L.; Crowson, C.S.; Myasoedova, E. Improved flare and remission pattern in rheumatoid arthritis over recent decades: A population-based study. Rheumatology 2017, 56, 2154–2161. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total = 501 | ||
|---|---|---|
| Age, years | Mean ± SD | 43.38 ± 11.15 |
| Range | 22.00–78.00 | |
| Gender, N (%) | Female | 400 (79.8%) |
| Male | 100 (20.0%) | |
| Educational level, N (%) | ≤high school | 236 (47.1%) |
| >high school | 264 (52.7%) | |
| Healthcare workers, N (%) | 149(29.7%) | |
| Smoking, N (%) | 70 (14.0%) | |
| Rheumatological disease, N (%) | Rheumatoid arthritis | 213 (42.5%) |
| Spondylarthritis | 97 (19.4%) | |
| Systemic lupus erythematous | 95 (19.0%) | |
| Connective tissue disease | 5 (1.0%) | |
| Rheumatism | 1 (0.2%) | |
| Juvenile arthritis | 2 (0.4%) | |
| Other | 88 (17.6%) | |
| Medication, N (%) | Steroid alone | 0 (0.00%) |
| c DMARD | 187 (37.3%) | |
| b DMARD | 90 (18.0%) | |
| s DMARD | 19 (3.8%) | |
| IVIG | 1 (0.2%) | |
| Anti-TNF | 5 (1.0%) | |
| IL-6 | 13 (2.6%) | |
| B-cell depleting therapy | 7 (1.4%) | |
| Combination therapy of DMARD | 45 (9.0%) | |
| Combination of steroid and DMARD therapy | 6 (1.2%) | |
| Combination of DMARD + B-cell depleting therapy | 5 (1.0%) | |
| Other | 15 (3.0%) | |
| Disease duration, years | Mean ± SD | 10.46 ± 8.54 |
| Range | 1.00–44.00 | |
| COVID-19 infection | COVID PCR positive swab result | 105 (21.0%) |
| Patients reported outcomes from the infection, n (%) (How things have turned out?) | I was not hospitalized | 86 (17.2%) |
| I was hospitalized with supplemental oxygen | 6 (1.2%) | |
| I was hospitalized, but I was not given supplemental oxygen | 10 (2.0%) | |
| I was hospitalized with the ICU admission | 1 (0.2%) | |
| Have quarantined during the period from 2019 to 2021, N (%) | 49 (9.8%) | |
| Number of vaccinated participants, N (%) | 351 (70.1%) | |
| Type of vaccine, N (%) | Pfizer/BioNTech | 205 (40.9%) |
| AstraZeneca/Oxford | 144 (28.7%) | |
| Vaccinated (n = 351) | Non-Vaccinated (n = 133) | p-Value | ||
|---|---|---|---|---|
| Age, years | Mean ± SD | 43.47 ± 11.53 | 42.84 ± 10.19 | 0.621 a |
| Gender, N (%) | Female | 273 (77.8%) | 114 (85.7%) | 0.052 b |
| Male | 78 (22.2%) | 19 (14.3%) | ||
| Educational level, N (%) | >high school | 203 (57.8%) | 57 (42.9%) | 0.003 b,* |
| Rheumatological disease, N (%) | Rheumatoid arthritis | 154 (43.9%) | 53 (39.6%) | 0.042 b,* |
| Spondylarthritis | 69 (19.7%) | 28 (20.9%) | ||
| Systemic lupus erythematous | 57 (16.2%) | 33 (24.6%) | ||
| Connective tissue disease | 2 (0.6%) | 3 (2.2%) | ||
| Rheumatism | 0 (0.0%) | 1 (0.7%) | ||
| Juvenile arthritis | 2 (0.6%) | 0 (0.0%) | ||
| Other | 67 (19.1%) | 16 (11.9%) | ||
| Disease duration, years | Median (Range) | 7.00 (1.00–42.00) | 7.00 (1.00–44.00) | 0.577 c |
| Patient assessment for the disease, N (describe rheumatic disease) | Inactive | 91 (26.0%) | 29 (21.8%) | 0.059 b |
| Mild to moderately active | 213 (60.9%) | 75 (56.4%) | ||
| Severely active | 46 (13.1%) | 29 (21.8%) | ||
| Prior SARS-CoV-2 infection, N (PCR positive swab result) | Yes | 73 (20.9%) | 32 (24.2%) | 0.422 b |
| No | 277 (79.1%) | 100 (75.8%) | ||
| Patient concerns about getting COVID-19, N (%) | Not concerned | 4 (10.8%) | 7 (41.2%) | 0.039 b,* |
| Mildly concerned | 6 (16.2%) | 4 (23.5%) | ||
| Deeply concerned | 15 (40.5%) | 3 (17.6%) | ||
| Moderately concerned | 12 (32.4%) | 3 (17.6%) | ||
| Prior influenza 2019/2020 combined Prior pneumonia vaccine, N (%) | Yes | 152 (43.3%) | 32 (23.9%) | <0.001 b,* |
| No | 199 (56.7%) | 102 (76.1%) | ||
| Consulting their doctor, N (%) | 288 (82.5%) | 76 (57.6%) | <0.001 b,* | |
| Reading KAR online info, N (%) | 156 (44.6%) | 39 (29.3%) | 0.005 b,* | |
| Family member receiving vaccine, N (%) | 0 (0.0%) | 51 (78.5%) | - | |
| Variables | Disease Flare Post-Vaccination (n = 9) | No Flare (n = 342) | p-Value | |
|---|---|---|---|---|
| Age | Mean ± SD | 42.71 ± 10.44 | 43.49 ± 11.57 | 0.861 a |
| Type of vaccine, N (%) | Pfizer/BioNTech | 4 (44.4%) | 200 (58.5%) | 0.837 b |
| AstraZeneca/Oxford | 5 (55.6%) | 139 (40.6%) | ||
| Gender, N (%) | Female | 7 (77.8%) | 266 (77.8%) | 0.1000 b |
| Male | 2 (22.2%) | 76 (22.2%) | ||
| Smoking, N (%) | 1 (11.1%) | 54 (15.8%) | 0.703 b | |
| Rheumatological disease, N (%) | Rheumatoid arthritis | 5 (55.6%) | 149 (43.6%) | 0.648 b |
| Spondylarthritis | 0 (0.0%) | 69 (20.2%) | ||
| Systemic lupus erythematous | 1 (11.1%) | 56 (16.4%) | ||
| Connective tissue disease | 0 (0.0%) | 2 (0.6%) | ||
| Polymyalgia Rheumatica | 0 (0.0%) | 2 (0.6%) | ||
| Juvenile arthritis | 0 (0.0%) | 0 (0.0%) | ||
| Other | 3 (33.3%) | 64 (18.7%) | ||
| Patient assessment of the disease, N (%) (Describe rheumatic disease) | Inactive | 0 (0.0%) | 91 (26.7%) | <0.001 b,* |
| Mild to moderately active | 4 (44.4%) | 209 (61.3%) | ||
| Severely active | 5 (55.6%) | 41 (12.0%) | ||
| Patient stopping their medication when taking the vaccine, N (%) | 7 (77.8%) | 134 (39.2%) | 0.141 b | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baroun, F.; Albasri, A.; Abutiban, F.; Alhajeri, H. CVAPPS: A Cross-Sectional Study of SARS-CoV-2 Vaccine Acceptance, Perceptions, and Post-Vaccination Side Effects among Rheumatic Disease Patients in Kuwait. Vaccines 2023, 11, 666. https://doi.org/10.3390/vaccines11030666
Baroun F, Albasri A, Abutiban F, Alhajeri H. CVAPPS: A Cross-Sectional Study of SARS-CoV-2 Vaccine Acceptance, Perceptions, and Post-Vaccination Side Effects among Rheumatic Disease Patients in Kuwait. Vaccines. 2023; 11(3):666. https://doi.org/10.3390/vaccines11030666
Chicago/Turabian StyleBaroun, Fatemah, Anwar Albasri, Fatemah Abutiban, and Heba Alhajeri. 2023. "CVAPPS: A Cross-Sectional Study of SARS-CoV-2 Vaccine Acceptance, Perceptions, and Post-Vaccination Side Effects among Rheumatic Disease Patients in Kuwait" Vaccines 11, no. 3: 666. https://doi.org/10.3390/vaccines11030666
APA StyleBaroun, F., Albasri, A., Abutiban, F., & Alhajeri, H. (2023). CVAPPS: A Cross-Sectional Study of SARS-CoV-2 Vaccine Acceptance, Perceptions, and Post-Vaccination Side Effects among Rheumatic Disease Patients in Kuwait. Vaccines, 11(3), 666. https://doi.org/10.3390/vaccines11030666